
Abstract
Background
NUT carcinoma, also named NUT midline carcinoma, is a highly aggressive and rare subset of squamous cell carcinoma. Its recognition is very challenging and demanding due to the following reasons: 1. it is rare and most pathologists and oncologists are not familiar with this malignancy, 2. its clinical and laboratory features may mimic other malignancies, 3. morphological and immunohistochemical analysis may be misleading if the diagnosis is not suspected, and 4. it is defined by the presence of a NUTM1 fusion. 1 Most commonly, NUTM1 is fused with either the BRD4 or BRD3 gene, and less commonly with NSD3 or other genes. 1 Since bromodomain and extraterminal domain inhibitor therapies have been developed and are currently used in clinical trials, identification of NUTM1 fusion partner may be essential for the appropriate clinical management. 1
Case Report
The patient was a previously healthy 47-year-old male, non-smoker, with an unremarkable medical history. He came to medical attention because of progressive dry cough lasting for a few weeks, progressive dyspnea, sharp pain under the left coastal margin and weight loss of 10 kg over the one month. He was referred to hospital where laboratory results showed leukocytosis (14 × 109/L) with neutrophilia (84%), increased CRP (112 mg/L) and increased LDH (6.15 U/L; normal range <4 U/L) levels. Massive bilateral serohemorrhagic pleural effusion was found and evacuated (1700 ml from the left and 1800ml from the right pleural space). Computed tomography of the thorax showed a partially necrotic mediastinal/left lung mass, measuring 12 cm in the largest diameter which was radiologically suggestive of primary lung carcinoma. To clarify the diagnosis, bronchoscopy with biopsy was performed. Histologic analysis showed a poorly differentiated neoplasm that was immunohistochemically negative for keratins CK AE1-AE3 and CKMNF116, EMA, TTF-1 and SALL4, but strongly and diffusely positive for LCA. A hematolymphoid neoplasm was suggested as the most likely diagnosis and patient was transferred to our institution for further evaluation and treatment. Additional laboratory work-up showed increased serum AFP (6389 kIU/L, normal <5.8 kIU/L). 18F-FDG PET CT showed increased uptake with SUV 13 in mediastinal/left lung tumor, multiple metastases in mediastinal and peripheral lymph nodes, bones and subcutaneous tissue as well as diffusely increased uptake in pleura on both sides. Radiological and laboratory findings suggested a mediastinal non-seminomatous germ cell tumor (NS-GCT). Since this clinical diagnosis was highly discrepant with the primary pathologic report, the oncologist decided to repeat the biopsy.
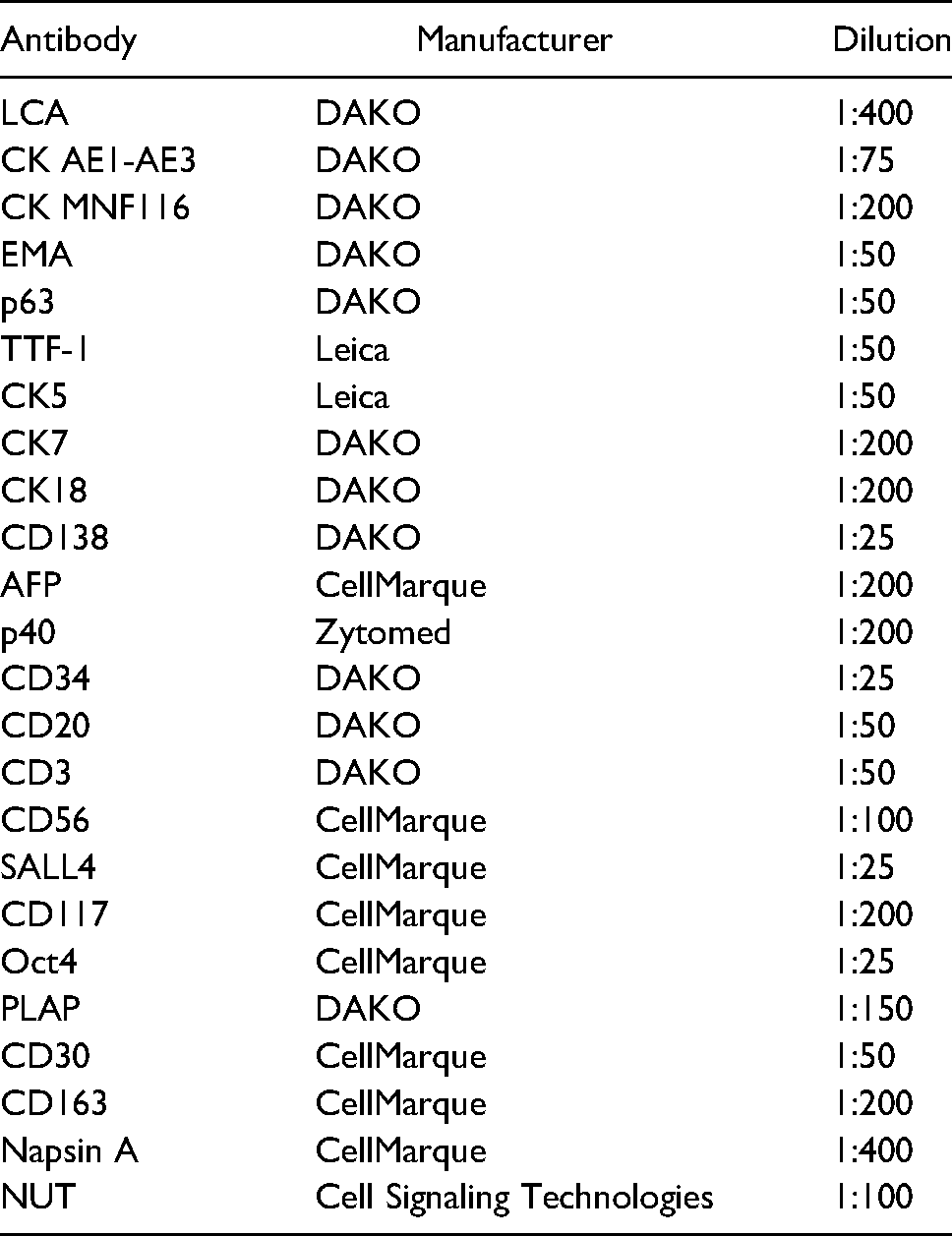
A subcutaneous metastasis from the left shoulder was excised and sent for pathological evaluation. Hematoxylin and eosin-stained sections showed a neoplasm consisting of undifferentiated, large vesicular cells with conspicuous, solitary nucleoli and poorly demarcated cytoplasms (Figure 1a). Foci of abrupt keratinization were present (Figure 1a arrows). A wide immunohistochemical panel was applied (Table 1). Tumor cells were positive for LCA (Figure 1b), CK AE1-AE3, CK MNF116 (Figure 1c), EMA, p63 and TTF-1 (Figure 1d), focally positive for CK5, CK7, CK18, CD138, AFP (Figure 1e), p40 and negative for CD34, CD20, CD3, CD56, SALL4, CD117, Oct4, PLAP, CD30, CD163, Napsin A. Immunohistochemical staining for NUT protein (Figure 1f) showed the characteristic speckled nuclear reaction and, finally, a diagnosis of NUT carcinoma was rendered. For molecular analysis, we performed RNA sequencing using the Oncomine™ Childhood Cancer Research Assay. Interestingly, we detected a BRD4-NUTM1 gene fusion in 82585 reads. On RNA level, exon 14 of BRD4 was fused to exon 2 of NUTM1, resulting in an in-frame fusion transcript containing many of the coding regions of both partner genes, including the BRD and ET domains of BRD4 and AD1 domain of NUTM1. 2 The slides from the bronchoscopic biopsy were reviewed. The morphology of the tumor cells was identical to those in metastatic lesion but there were no morphological signs of squamous differentiation.
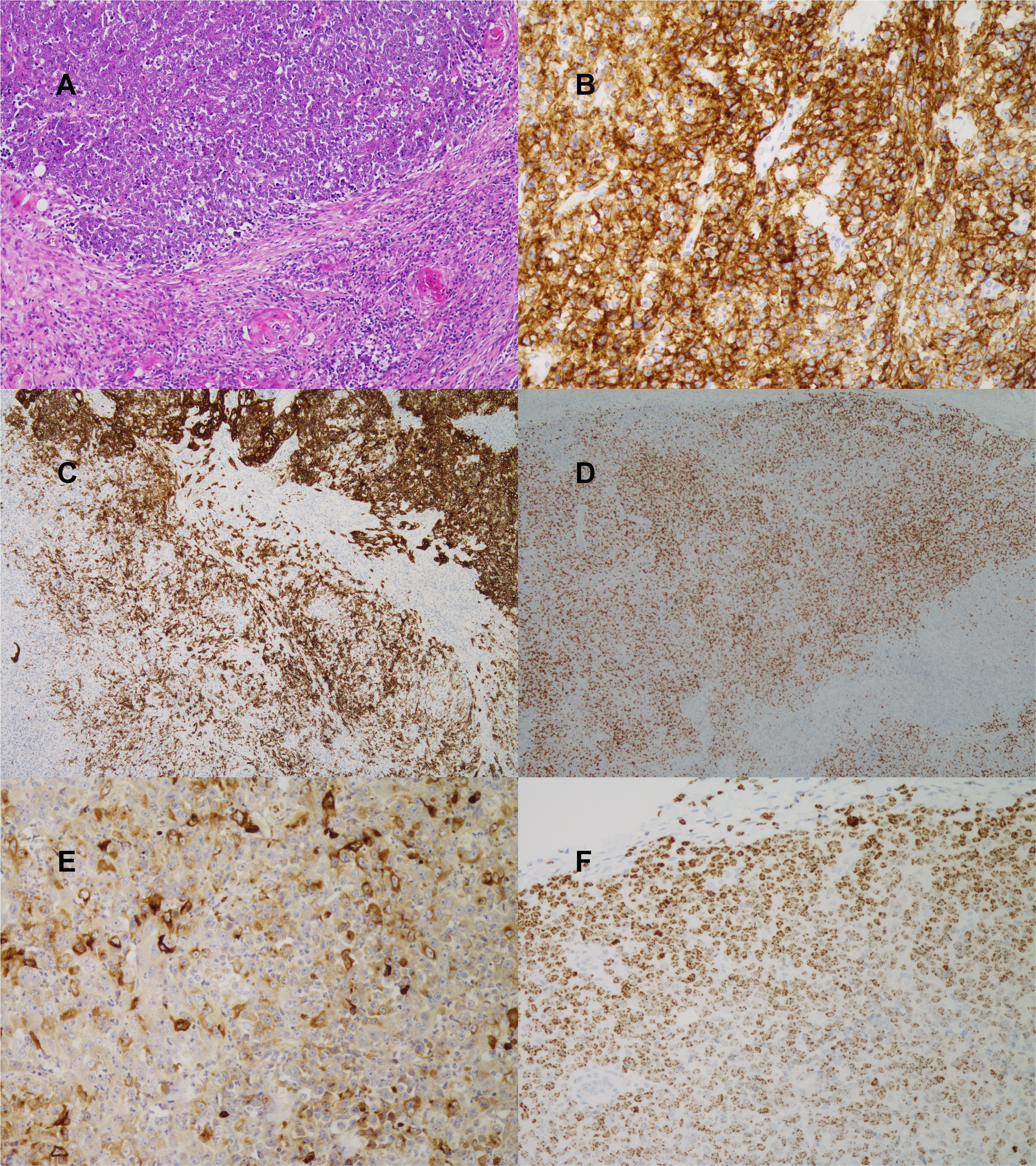
(A) H&E, 10×: poorly differentiated neoplasm with focus of abrupt keratinization (marked by arrows) (B) LCA immunohistochemistry, 20× (C) CK MNF116 immunohistochemistry, 5× (D) TTF-1 immunohistochemistry, 5× (E) AFP immunohistochemistry, 20× (F) NUT immunohistochemistry, 20×: characteristic, speckled pattern of staining.
Immunohistochemistry.
The patient received two cycles of chemotherapy according to the CAP protocol (cyclophosphamide, doxorubicin, platinol) but showed progressive disease and a fast deterioration of the performance status. Unfortunately, he succumbed less than 2 months after the diagnosis.
Discussion
NUT carcinoma is a poorly differentiated subtype of squamous cell carcinoma, commonly associated with a rearrangement of the NUTM1 gene with various partner genes, such as BRD4, BRD3 and NSD3. 1 In our case we detected a BRD4-NUTM1 fusion. Indeed, BRD4-NUTM1 are the most frequent rearrangements in NUT carcinoma and have been shown to be present in up to 80% of NC. 1 The breakpoint seen in our case is common, which frequently involves exon 2 from NUTM1 and exons 11 to 15 from BRD4. 3 Fusion oncoproteins cause upregulation of MYC and hence autonomous tumor growth. NUT carcinoma is an aggressive malignancy, and a recent analysis of a large patient cohort identified three prognostic groups based on tumor location and presence and type of fusion. 4 Interestingly, at least a subset of patients may benefit from the use of BET inhibitors, possibly in combination with other agents. 5 Tumors with NUTM1-BRD4 fusion could be sensitive to BET inhibitors. 5 NUT carcinoma is a relatively under-recognized entity and is usually not suspected by both pathologists and oncologists. It may be misdiagnosed if it is not considered in the differential diagnosis and specifically looked for. For example, in the study by Evans et al 6 , a re-evaluation of 114 cases of undifferentiated mediastinal malignancies with immunohistochemical staining and FISH for NUT lead to the diagnosis of NUT carcinoma in 3.5% of the cases.
The diagnosis of NUT carcinoma can be very challenging for the following reasons:
Clinical presentation may mimic other neoplasms. In our case, a mediastinal tumor with elevation of AFP suggested a mediastinal NS-GCT. Principal tumors that secrete AFP are yolk sac tumor, hepatoblastoma, and hepatocellular carcinoma, and only rarely some other tumors like lung or gastrointestinal carcinomas, Sertoli-Leydig cell tumor or Wilms tumor. It can also be seen in chronic liver disease, such as cirrhosis and in acute hepatitis. Although NUT carcinoma only rarely produces AFP, a few reports have been published in the recent literature
7
describing patients with NUT carcinoma with similar clinical presentation and elevated levels of serum AFP. In some cases, immunohistochemical staining of the tumor tissue for AFP was done and was negative. By morphology it is an undifferentiated neoplasm which may or may not show foci of abrupt keratinization. Abrupt keratinization has been described to be characteristic for NUT carcinoma but is not always present and could very often be missing in small specimens harvested from endoscopic, aspirational or core needle procedures. Immunohistochemical analysis yields frequently also ambiguous results. In our case the primary tumor from the bronchoscopy specimen showed an intense and strong positivity for LCA while there was no keratin expression. Keratin and LCA expression are in general mutually exclusive in practice of diagnostic surgical pathology and differential diagnosis between poorly differentiated/undifferentiated carcinoma and hematolymphoid neoplasm is greatly aided by immunohistochemical staining for the two markers with rare exceptions such as in small subset of otherwise characteristic B- and T-cell lymphomas, but not in acute leukemias.
8
LCA is considered highly specific for hematological neoplasms and is a commonly used marker of hematopoietic cells except erythrocytes and thrombocytes. Reports of aberrant expression of LCA in non-hematological neoplasms are more or less anecdotal consisting of very rare cases of undifferentiated and neuroendocrine carcinoma9–11, one seminoma and one rhabdomyosarcoma.
12
On the basis of the extremely aggressive clinical behavior, tumor location (midline) and microscopic description of such undifferentiated/poorly differentiated neoplasm, we could presume that at least a few of them9,11 may represent NUT carcinoma, an entity non-existent in the time of publication of those reports. Second point regarding immunohistochemistry of note in our case is tumor positivity for AFP. In some of the cases of NUT carcinoma with elevated levels of serum AFP that were immunohistochemically stained for AFP
7
, the tumor tissue itself was immunohistochemically negative for AFP staining. On the basis of that finding, D’Ambrosio et al
7
concluded that negative AFP staining could exclude the diagnosis of mediastinal NS-GCT. Our conclusion is that immunohistochemical positivity for AFP cannot serve as a reliable marker of NS-GCT even if clinical presentation together with laboratory findings suggests that diagnosis, as we have shown in our case. As well, strong and diffuse expression of TTF-1 is highly unusual in NUT carcinoma. So far, it was described only in a few cases.13–15 This may be important potential source of misdiagnosis especially in tumors that on morphology lack squamous differentiation or are immunohistochemically negative for its markers such as p40 or CK 5/6.
15
p40 or CK 5/6 negative tumor with TTF-1 expression could be erroneously diagnosed as lung adenocarcinoma. A definitive diagnosis of NUT carcinoma can basically be made by NUT immunohistochemistry and/or NUTM1 FISH in characteristic clinical context. Immunohistochemical staining has 100% specificity and 87% sensitivity in detection of NUT protein expression and is considered the first line approach to NUT carcinoma diagnosis.
16
However, due to the use of next generation sequencing methods, NUTM1 rearrangement with different fusion partners have been found in diverse array of other neoplasms that could show immunohistochemical positivity for NUT protein. For example, a NUTM1 rearranged acute lymphoblastic leukemia (ALL) shows speckled nuclear positivity for NUT protein and since NUT carcinoma in our case showed diffuse LCA positivity, NUTM1 rearranged ALL should be considered in the differential diagnosis. NUTM1- rearranged ALL is characteristically a disease of infant and pediatric population with many different fusion genes reported, none of them belonging to the BET family.
1
It seems reasonable to perform next generation sequencing for identification NUTM1 fusion partner in order to confirm a diagnosis of NUT carcinoma in malignancy with positive NUT immunohistochemistry/NUTM1 FISH especially if there are discrepant clinical and/or histopathological findings.
3
To the best of our knowledge, this is the first case of NUT carcinoma showing aberrant expression of LCA described in the literature so far. Therefore, we suggest that all poorly differentiated/undifferentiated tumors with aggressive clinical picture, especially those arising in the midline should be tested for NUT protein and/or NUT gene translocation since morphology of NUT carcinoma is non-specific, particularly in small biopsies and its imunohistochemical profile can be very wide and misleading. Since the category of the NUTM1 – rearranged neoplasms is rapidly expanding and new targeted drugs such as BET inhibitors are developing, identification of NUTM1 fusion partner is essential for appropriate diagnosis and adequate clinical management.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
This study was approved by the Ethical board of Institute of Oncology Ljubljana, Slovenia, ERIDNPVO-0032/2020
Informed Consent
Signed consent for publication was obtained from patient's spouse since he passed away.
Trial Registration
Not applicable, because this article does not contain any clinical trials.