
Abstract
Reparative perineural hyperplasia is an incidental and probably underreported reactive histologic finding thus far only reported in the setting of healing wounds or adjacent to a dermatofibroma in cutaneous specimens. It is characterized by a focal concentric proliferation of cytologically bland spindled perineurial cells and is hence considered a benign histologic mimic of neoplastic perineural invasion. Thus, it may present a diagnostic pitfall and we therefore consider it as a valuable entity to be aware of. To the best of our knowledge, this brief case report is the first to convey that reparative perineural hyperplasia may also occur in the gastrointestinal tract. It may therefore be a ubiquitous reactive histological phenomenon relating to previous surgical or traumatic wounds in various sites, that is, outside the thus far established setting of skin reexcision specimens.
Keywords
Background
Reparative perineural hyperplasia (RPH) is a seldom-reported incidental histological finding, which is likely reactive in nature since it characteristically occurs in the setting of healing surgical or traumatic wounds. In the literature, RPH has initially been described by Beer 1 in a series of 10 cutaneous reexcisions of various skin tumors, occurring as a focal concentric proliferation of the perineurial cells in close association to fibrosis and/or chronic inflammatory infiltrate. Subsequently, it has also been reported to occur in association with a dermatofibroma, the implication being that RPH is not restricted to the context of previous surgical procedure and may occur more commonly in various fibrosis- and trauma-related cutaneous conditions. 2 Indeed, many consider dermatofibroma as a trauma-related entity. Outside the setting of skin excision specimens, RPH has not yet been reported.
Clinical Data
A 78-year-old female patient with the unremarkable past medical history presented to the emergency department in hypovolemic shock due to massive hematemesis. Gastroscopy revealed a likely perforated peptic ulcer of the lesser curve, with signs of active arterial bleeding. Surgical management with excision of the ulcer followed by omental patch repair was thus performed. The hemostasis was inadequate, though, and the patient required multiple transfusions in the postoperative period. Due to multiple hemorrhagic episodes with hypotension, she also developed mural ischemic proctosigmoiditis, necessitating segmental bowel resection 1 week after initial presentation. Finally, an emergency gastrectomy was warranted due to incessant diffuse active bleeding from the stomach wall and the resection specimen was sent to our pathology department.
Pathological Findings
Macroscopic examination revealed numerous coagula in the gastric lumen, together with diffusely pale, dull mucosa with multiple erosions and ulcerations. A transmural defect of the lesser curvature, covered by the omental patch corresponding to perforation, was seen. The stomach wall was otherwise regular and of normal thickness.
Light microscopic features were thus those of acute ischemic gastritis with abundant peptic necrosis, small vessel thrombosis, perforation, and resultant acute peritonitis. Sampled lymph nodes displayed nonspecific reactive sinus histiocytosis.
Additionally, a peculiar and at first glance rather worrisome finding was observed in the subserosa adjacent to the omental patch repair site. The perineurium of a single smaller nerve was expanded by a concentric proliferation of bland spindle-shaped cells in a syncitial arrangement and with mildly pleomorphic open nuclei, fine chromatin, and inconspicuous nucleoli (Figure 1A). A single regular mitotic figure was present in 1 lesional cell. There was also a mixed inflammatory infiltrate consisting of neutrophils, lymphocytes, and plasma cells in the surrounding edematous loose connective tissue, in keeping with a reparative process due to both ischemia and recent surgical procedure. Unfortunately, the proliferation could not be completely immunohistochemically characterized since the tissue block had been exhausted at that location. Limited by only the original slide and guided by the perineurial-like morphology, we therefore stained for epithelial membrane antigen (EMA; clone E29; 1:20 dilution; Dako), which was positive in a weak and diffuse granular cytoplasmic pattern (Figure 1B). Overall, the findings were consistent with perineurial differentiation of the proliferation and thus with a diagnosis of postsurgical RPH.
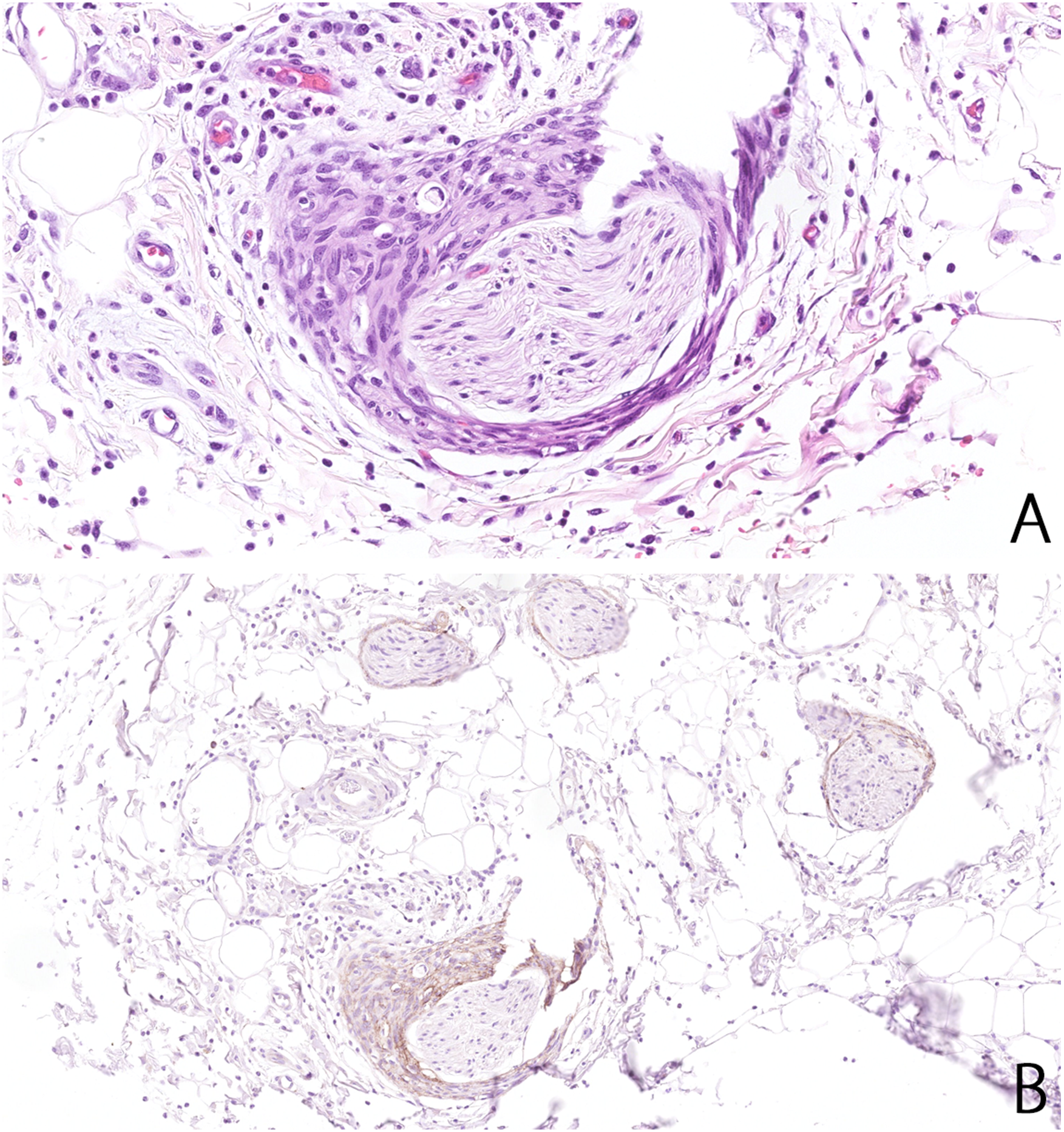
(A) Plump spindle cells with bland nuclei and pinpoint nucleoli surround a smaller subserosal nerve, expanding its perineurium. There is mixed inflammation and edema in the surroundings. (×200). (B) Weak and diffuse epithelial membrane antigen (EMA, ×100) immunoreactivity in the cells expanding the perineurium at the bottom center. The staining character was comparable to that of adjacent uninvolved perineuria.
Discussion
In the context of concurrent or previous malignancy, RPH may well mimic neoplastic perineural invasion (PNI), which is characterized by the presence of cytologically malignant cells in the perineural space and is an important feature to recognize in a wide variety of malignant tumors and resection specimens, due to its negative prognostic significance. 3 However, to prevent unnecessary morbidity, it is probably equally important to be aware of and recognize its potential histologic mimics, such as RPH, epithelial sheath neuroma (ESN), reexcision perineural invasion (RPI), peritumoral fibrosis, and Renaut bodies.1,4,5
Contrary to PNI, however, these are all characterized by cytologically bland benign proliferations confined to the perineural space or mimicking the nerve fibers themselves in cases of peritumoral fibrosis. In addition to PNI, ESN and RPI are also considered as morphological differentials of RPH.
ESN, first described in 2000 by Requena et al 6 , has a characteristic and consistent clinical presentation of papular skin lesions on the upper back of elderly (female) patients arising de novo, that is, without a history of trauma, preexisting lesion, or surgery. This presentation alone contrasts with that of RPH, which is considered as a “histology-only” entity. The histological findings of ESN consist of proliferated enlarged nerves in the superficial dermis surrounded by orthokeratinizing squamous epithelial sheath in the perineural space.
RPI is another “histology-only” benign mimic of both PNI and RPH in the setting of skin reexcision specimens. Stern and Haupt 7 initially described it in 1990 as a benign squamous epithelial proliferation involving the perineuria of cutaneous nerves adjacent to and possibly originating from eccrine ducts. Like RPH, it is considered as a reparative phenomenon related to previous surgery and thus scarring.
To back up the idea of RPH and exclude these differential diagnoses, an immunohistochemical panel consisting of EMA, S100 protein, and pancytokeratin (CK) may be employed and is a useful adjunct to morphology, highlighting the perineurial differentiation (EMA positive/S100 and CK negative). Conversely, the perineural involvement in both ESN and RPI would show positivity for CK and negativity for S100 protein. The latter would also differentiate concentrically proliferated fibrous tissue in peritumoral fibrosis, which might be difficult to distinguish from nerve tissues on morphology alone.
Thus far, only a handful of cases and a single case series discussing RPH have been reported, none outside the setting of skin excision specimens. However, we speculate that this may partly be due to high frequency of reexcisions and thus healing wound sampling in dermatopathology.
Helpful microscopic clues to reach this diagnosis include a focal and localized nature, overall bland and organized appearance with a lack of significant atypia, and features of adjacent reparative process (inflammation and scarring from previous surgical procedure/trauma).
The unremarkable patient medical record, that is, no history of current or past malignancy, also contributed to discarding the initial differential diagnosis of PNI.
In essence, we present a case of RPH in a gastrectomy specimen, primarily to raise awareness of this incidental histologic finding in order to avoid misinterpreting it as incidentally sampled PNI, especially in cases where a (malignant) tumor is adjacent. Additionally, our findings corroborate that RPH is a ubiquitous reactive phenomenon that may be encountered in various pathology specimens in relation to previous surgical procedures and is not limited to skin reexcision specimens alone.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.