
Abstract
A solid and cystic pancreatic lesion was incidentally found in a 62-year-old woman on abdominal computed tomography. The lesion was diagnosed as a solid pseudopapillary neoplasm by using endoscopic ultrasound-guided fine needle aspiration, and the tumor was resected. Histologically, the tumor cells had relatively small, round nuclei and papillary-like architecture in a hemorrhagic background. On immunohistochemical examination, the tumor cells were diffusely positive for nuclear β-catenin and cytoplasmic CD10. In addition, typical histological findings of IgG4-related pancreatitis (obstructive phlebitis, storiform-type fibrosis, and abundant IgG4-positive plasma cell infiltration) were found in the surrounding stroma of the solid pseudopapillary neoplasm. Postoperative workup failed to detect any other sclerotic lesions or serum IgG4 elevation, suggesting that the patient had no evidence of IgG4-related disease. To avoid misdiagnosis of a combined pancreatic neoplasm and fibro-inflammatory lesion, pathologists should consider such situations and make a definitive diagnosis after careful observation of all pancreatic lesions.
Keywords
Introduction
IgG4-related pancreatitis has been recognized as a unique form of autoimmune pancreatitis (also known as type 1 autoimmune pancreatitis), the histology of which consists of lymphocytic and IgG4-positive plasma cell infiltration, storiform fibrosis, and obstructive phlebitis. 1 These fibro-inflammatory lesions are found at multiple, different anatomical sites, together with serum IgG4 elevation, indicating that the condition is regarded not as a local immune response but a systemic disorder (IgG4-related disease; IgG4-RD).
Recent studies revealed that approximately 0.5% to 1.0% of patients with IgG4-related pancreatitis or type 1 autoimmune pancreatitis are diagnosed with pancreatic cancer concurrently or during follow-up after the pancreatitis diagnosis.2,3 On the other hand, approximately 10% of patients with pancreatic cancer have concomitant serum IgG4 elevation or moderate-to-marked IgG4-positive plasma cell infiltration.4,5 Taken together, these data support a close association between pancreatic malignant processes and IgG4-positive plasma cell–associated inflammation. However, any causal relationship between both lesions remains unclear.
Herein, we report the first case, to our knowledge, of combined IgG4-related pancreatitis and solid pseudopapillary neoplasm (SPN), a rare low-grade malignant tumor.
Case Report
A solid and cystic lesion of the pancreatic tail was incidentally found in a 62-year-old woman with no significant past medical history. The lesion appeared as a 3-cm low-density area in the pancreatic tail on abdominal computed tomography (CT). There was no diffuse radiological change in the pancreas or main pancreatic duct, probably owing to the distal location of the pancreatic lesion. Contrast-enhanced CT showed narrowing of the splenic vein and development of collateral circulation, suggesting that this pancreatic lesion was associated with venous invasion. The lesion was diagnosed as an SPN on endoscopic ultrasound-guided fine needle aspiration (EUS-FNA), and distal pancreatectomy was performed.
Histologically, the solid and cystic tumor was surrounded by pancreatic fibro-inflammatory stroma (Figure 1). The tumor cells showed relatively small, round nuclei and papillary-like architecture in a hemorrhagic background (Figure 2A). On immunohistochemical examination, the tumor cells were diffusely positive for nuclear β-catenin (Figure 2B) and cytoplasmic dot-like CD10 (Figure 2C). The tumor cells were focally positive for synaptophysin and CD56, while they were negative for chromogranin A and trypsin. The Ki-67 tumor labeling index was <5%. Consistent with the diagnosis based on EUS-FNA biopsy, we diagnosed the patient with an SPN of the pancreas.
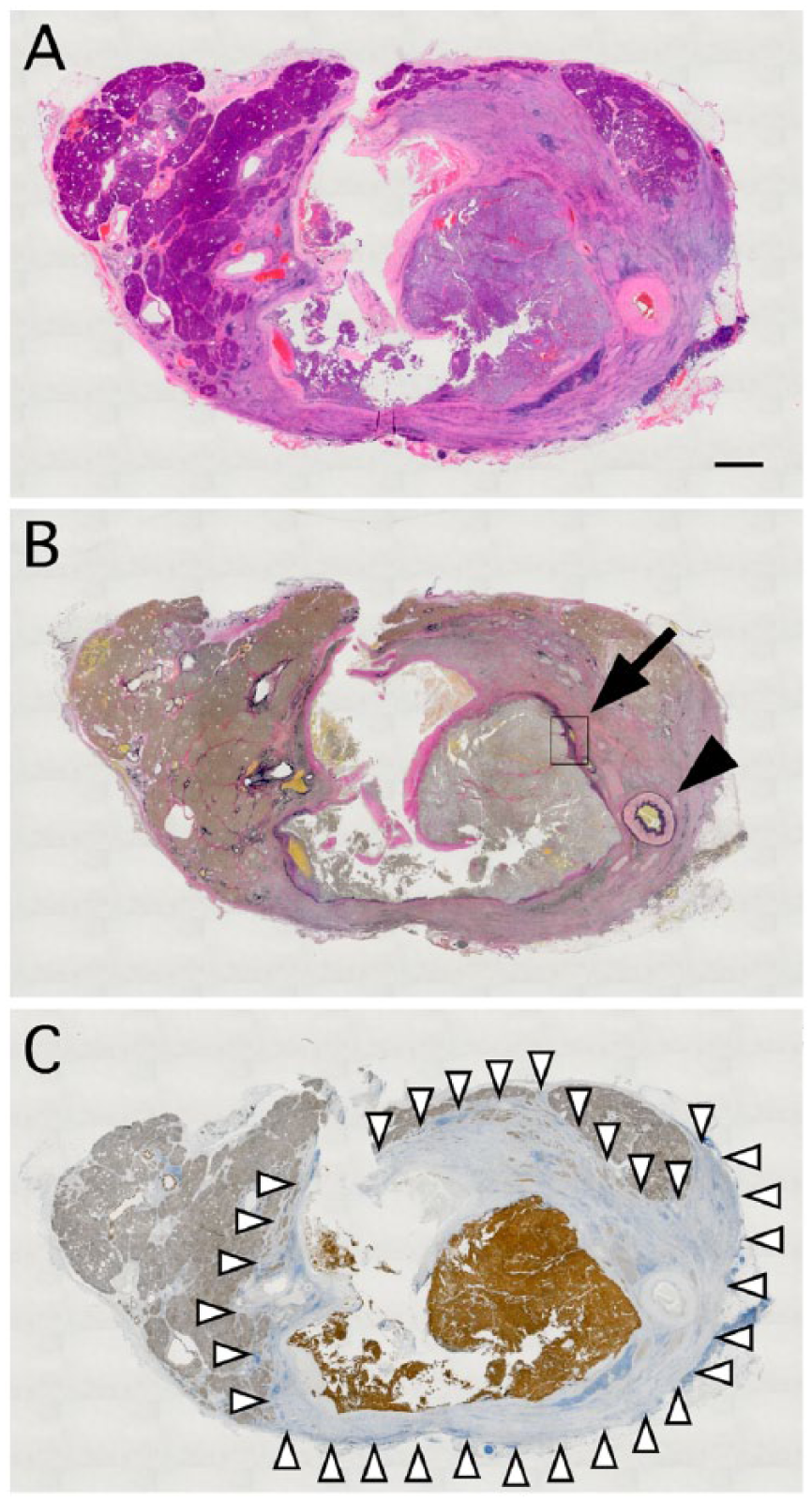
Overview of the pancreatic lesion. (A) Hematoxylin and eosin (HE) staining, (B) Elastica van Gieson (EvG) staining, and (C) β-catenin immunostaining of the cross-section of the pancreatic tail. After HE staining, the lesion appears pale, compared with normal pancreatic tissue. β-catenin immunostaining reveals areas of the tumor cells, normal pancreatic tissue, and IgG4-related pancreatitis that are strongly positive, weakly positive, and negative, respectively. According to β-catenin immunoreactivity, these 3 areas are clearly distinguished. Note that EvG staining reveals a venous-like structure around the tumor nests (see also Figure 2D, black arrow), which is likely the splenic vein. Black arrowhead, the splenic artery. White arrowheads, the border between area of IgG4-related pancreatitis and normal pancreatic tissue. Scale bar = 2 mm.
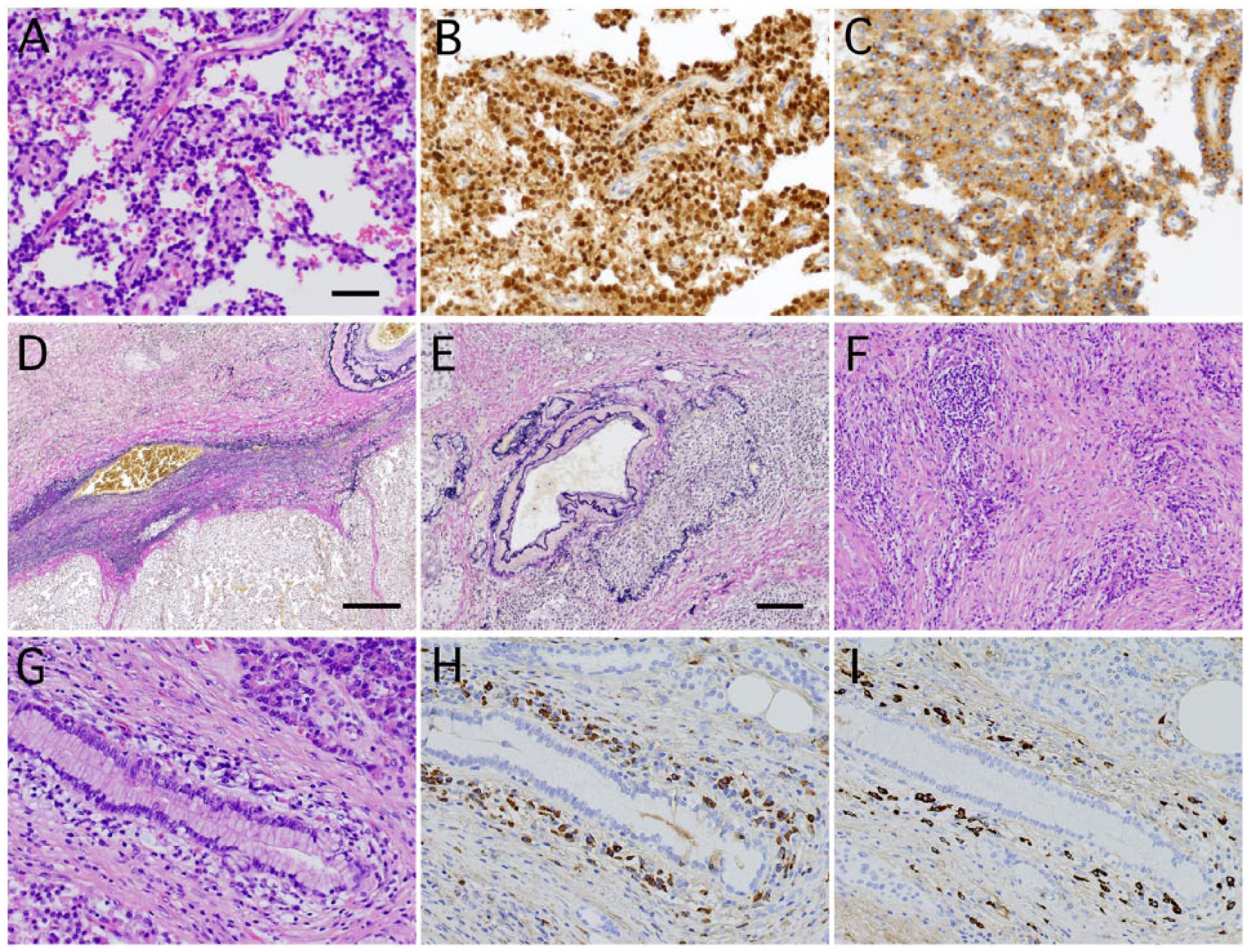
Representative images of a solid pseudopapillary neoplasm (SPN) of the pancreas and IgG4-related pancreatitis. Hematoxylin and eosin (HE) staining (A), β-catenin immunostaining (B), CD10 immunostaining (C), and Elastica van Gieson (EvG) staining (D) of an SPN. EvG staining indicates venous invasion of tumor cells. (E-I) Typical findings of IgG4-related pancreatitis. EvG staining of obstructive phlebitis (E), HE staining of storiform fibrosis (F), and HE staining (G), IgG immunostaining (H), and IgG4 immunostaining (I) of dense lymphoplasmacytic infiltrates. IgG and IgG4-immunostaining reveals that a ratio of IgG4/IgG-positive plasma cells of approximately 45% and >50 IgG4-positive plasma cells/high-power field. Scale bars = 100 µm (A-C and G-I), 200 µm (E and F), or 500 µm (D).
In order to identify the venous invasion observed on radiological examinations, we performed Elastica van Gieson staining. Interestingly, we found not only a venous-like structure around the tumor nest (Figure 2D) but also obstructive phlebitis in the surrounding stroma (Figure 2E). In addition, the surrounding stroma exhibited storiform-type fibrosis (Figure 2F) and was associated with dense lymphoplasmacytic infiltrates (Figure 2G). IgG and IgG4-immunostaining revealed a ratio of IgG4/IgG-positive plasma cells of approximately 45% and >50 IgG4-positive plasma cells/high-power field (Figure 2H and 2I). These findings were compatible with the typical features of IgG4-related pancreatitis. Subsequently, we measured the patient’s postoperative serum IgG4 level, which was within normal limits, and no other sclerotic lesion was found on radiological assessment, suggesting that the patient had no evidence of IgG4-RD. The patient has received no additional therapy and exhibited no disease recurrence for 15 months postoperatively.
Discussion
SPN is a rare pancreatic tumor that does not differentiate along any particular lineage, and almost all SPNs harbor a somatic mutation in exon 3 of β-catenin. 6 SPN is classified as a low-grade malignant tumor, in that direct extension or metastasis is sometimes found in the surrounding organs, for example, stomach and spleen. In the present case, the tumor cells invaded the splenic vein, and collateral circulation subsequently developed. These findings may reflect its malignant behavior.
IgG4-positive plasma cell infiltration associated with pancreatic cancer is sometimes found. Most patients lack the above-mentioned typical histology of IgG4-related pancreatitis,4,5 suggesting that these phenomena should be distinguished from IgG4-related pancreatitis and/or IgG4-RD. However, the pathological significance of these nonspecific IgG4-positive plasma cell infiltrations is unknown, and it is not clear whether a routine search for IgG4-positive plasma cell infiltration should be made in pancreatic cancer. In addition, a clear distinction between the fibrotic phase of IgG4-RD and nonspecific IgG4-positive plasma cell infiltration is difficult, even with a sufficient surgical specimen. In the present case, the observed fibro-inflammatory changes fulfilled the histological criteria of IgG4-related pancreatitis, although the fibro-inflammatory changes were limited to the zone immediately surrounding the tumor. In addition to the histological distribution, clinical and radiological findings favor the diagnosis of a stromal reaction to the tumor over true IgG4-RD. Further investigation of combined pancreatic neoplasia and IgG4-positive plasma cell infiltration with or without histology associated with typical IgG4-related pancreatitis is needed.
Bateman et al described the link between intraductal papillary mucinous neoplasm of the pancreas and IgG4-RD. 7 Of 14 intraductal papillary mucinous neoplasm cases, 2 “index” cases showed most of the key clinical and histological features of IgG4-RD, although data on serum IgG4 concentration were not available. On the other hand, the other 12 cases lacked the findings of obstructive phlebitis and storiform-type fibrosis, and some of them contained a small amount of IgG4-positive plasma cell infiltrates. Taken together, these key clinical findings are essential for the diagnosis of IgG4-RD, and the Boston criteria 1 can be used to distinguish type 1 autoimmune pancreatitis/IgG4-RD from other nonspecific chronic inflammations of the pancreas.
Obstructive phlebitis is one of the histological diagnostic clues of IgG4-related pancreatitis and IgG4-RD. Obstructive phlebitis is frequently found in the various affected organs,8-21 except for the lacrimal glands 22 and lymph nodes. 23 This angiotropic fibro-inflammation may be important for clarifying the detailed mechanism of IgG4-RD. In the present case, obstructive phlebitis in the surrounding stroma supported the presence of IgG4-related pancreatitis, and possibly contributed to the development of collateral circulation through the blockage of minor veins.
EUS-FNA is a relatively new, safe, and less invasive diagnostic technique to obtain a histological specimen that is sufficient to diagnose pancreatic lesions, including pancreatic tumors and IgG4-related pancreatitis. 24 To confirm IgG4-related pancreatitis without histological examination is a diagnostic challenge, because some cases mimic neoplasia to form a pancreatic mass.25-29 This technique allows the choice of an optimal treatment according to the pathological diagnosis of the pancreatic disease. Malignant disease requires surgery and/or chemo-radiation, whereas steroid therapy is appropriate for treating autoimmune pancreatitis. However, a small sample obtained using EUS-FNA may be inadequate to diagnose combined neoplastic and fibro-inflammatory lesions, especially if the distribution of the 2 lesions is distinguished in the pancreatic mass (Figure 1). For diagnosing combined pancreatic disease, surgical resection is probably required to confirm global lesion features.
We report a combined case of IgG4-related pancreatitis and SPN. Similar to pancreatic cancer, this low-grade malignancy is also rarely associated with IgG4-related pancreatitis. To avoid misdiagnosis of a combined pancreatic neoplasm and fibro-inflammatory lesion, pathologists should consider such situations and make a definitive diagnosis after careful observation of all pancreatic lesions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.