
Abstract
Couples facing a serious medical diagnosis of one of the partners face unique challenges. Relationship quality, especially emotional and practical support, impacts the well-being of both partners and, at times, the physical response of the afflicted client to illness and disease. Emotionally focused couples therapy (EFCT) is an effective treatment for increasing couple secure attachment and decreasing conflict and stress in couple relationships. In this systematic review, we screened 450 articles looking for studies about emotionally focused therapy (EFT) in the treatment of couples facing a serious medical diagnosis. Of these articles, 42 full articles were reviewed, and eight met criteria to be included in this systematic review. Outcomes from the studies included showed EFT/EFCT helped couples where one partner has a major health diagnosis reduce psychological distress and improve relationship health factors such as communication, self-disclosure, secure bond, and emotional expression, increasing relationship satisfaction. Quality of life increased after EFT interventions, and in one study, a patient's physical response to their neurodegenerative disease improved poststudy and during EFT sessions.
A serious health diagnosis or illness has an emotional and relationship impact on couples (Bouchard et al., 2023; Chawla & Kafescioglu, 2012; Crangle & Hart, 2017). Disease and chronic illness affect both the individual who is afflicted, as well as that person's intimate partner and their relationship interactions and patterns (Kowal et al., 2003). Exposure to a loved one's “suffering” has a significant impact on their spousal caregiver's wellness, can become a source of stress, and take a multifaceted toll on their caregiver (Monin & Schulz, 2009). Suffering is a holistic construct, involving emotional, spiritual, or physical distress dimensions. Moderators that influence caregiver's emotional responses include gender, closeness, caregiving efficacy, and individual differences in emotion regulation (Monin & Schulz, 2009). The experience of receiving news of a serious health diagnosis can significantly impact a person's life, affecting not just their physical health but also their relationships (Fortin et al., 2021).
Relationship quality and health impact one another in a reciprocal manner, in that health problems both influence and are influenced by relationship quality (Dankoski & Pais, 2007). Greater relationship quality is related to better health, with mean effect sizes from r = .07 to .21, including lower risk of mortality (r = .11) and lower cardiovascular reactivity during conflict (r = .13), encouraging researchers and clinicians to focus on moderating factors that may influence the relationship between marital quality and health (Robles et al., 2014). Regarding physical health outcomes, the quality of close relationships and social support is linked to immune function (Kiecolt-Glaser & Gaser, 2001). According to Kowal et al. (2003), the constructs of relationship status, relationship quality, and specific relationship behaviors interacting with illness are three important areas to examine when looking at the connection between relationship and illness. These authors found that marital quality predicts survival following congestive heart failure and is linked to disease symptoms and negative health outcomes. Relationship behaviors related to an illness of one of the partners, such as hostile interactions, criticism, and contempt, were related to the number of health problems couples face, and a reduced ability to cope with chronic illness collaboratively (Kowal et al., 2003). In summary, though married couples are seen to have high levels of socioemotional support, the marriage/health connection is contingent on the quality of the emotional climate in the relationship (Carr & Springer, 2010).
Adult Attachment
The tenets of attachment theory posit that all human beings are hardwired to establish and maintain meaningful emotional connections to important others throughout the lifespan (Bowlby, 1973). These connections offer a form of protection from physical and emotional harm and, by extension, create an environment conducive to emotional resilience, balance, and optimal functionality (Bowlby, 1979; Greenman & Johnson, 2022). In contrast, those who lack emotional bonds are more susceptible to distress and disease (Pietromonaco et al., 2013). According to Bowlby, lack of availability and responsiveness of “attachment figures” (e.g., important others to whom we rely upon from connection, comfort, and support) due to separation, loss, or inconsistent responding was a major contributing factor leading to the onset of anxiety and depression (Bowlby, 1979; Greenman & Johnson, 2022). Theorists believe that attachment processes might play an important role in the “etiology of and recovery from physical disease” (Greenman & Johnson, 2022; Pietromonaco et al., 2013). Additionally, attachment theory posits that humans form working models-of-self based on recurring experiences with important others, which create an individual attachment style. These working models consist of “expectations about the worthiness of the self in relation to significant others, as well as the availability and responsiveness of attachment figures” (Bowlby, 1973; Pietromonaco et al., 2013). When a person learns their needs are important and consistently responded to, they tend to enjoy attachment security, and when the opposite occurs, insecure attachment styles tend to fall within the dimensions of either attachment anxiety or avoidance, with both styles negatively impacting support-seeking and receiving behaviors (Pietromonaco et al., 2013). Meredith and Strong (2019) concluded that insecurely attached people would be more likely to appraise their pain as threatening, less likely to believe and they could cope with the pain, and less able to obtain and sustain useful support. Additionally, those with an insecure attachment style are more likely to distrust treating professionals, less able to use effective coping responses, more likely to report depression and anxiety, and less able to manage the distress arising from the pain experience. These factors were further expected to contribute to poorer treatment outcomes and poorer general adjustment to persistent pain and discomfort (Meredith & Strong, 2019). In a systematic review of attachment and physical illness, Maunder and Hunter (2001) found supportive evidence for the hypothesis that attachment insecurity contributes to physical illness through the mechanisms of (a) altered stress physiology, (b) increased use of external regulators of affect, and (c) altered use of health-protective behaviors, all of which increase disease risk.
Medical Conditions and Couples
Couples who are facing a serious health diagnosis such as Parkinson's disease (PD) experience drastic role changes in their partnerships, new routines, a reduction in household task functioning for the patient, physical deterioration, caregiver strain, and grief over the loss of health and vitality (Spencer & Haub, 2018). In a qualitative study of both PD patients and their partners, participants expressed relational issues stemming from PD which were grouped into common themes: couples reported (a) experiencing changes in closeness, (b) shifting relational roles, (c) changes in sexual intimacy, (d) facing financial stress, (e) engaging in fewer leisure and social activities together, and (f) experiencing uncertainty about their relationship (Martin, 2016). Other relational themes emerging from studies with couples where one partner has PD highlight the importance of caregiver support and the experience of a couple's emotional co-regulation as they face an uncertain future (Constant et al., 2022). Some PD patients report fears of becoming a burden to their partner or their partner beginning to resent them with the challenges the disease brings (Martin, 2016). Increased couple mutuality (e.g., the quality of interaction or reciprocity of sentiment in a relationship) as reported by the spouse of PD patients, is associated with lower caregiver burden, less depression of both spouse and patient, and less PD symptom severity. In addition, mutuality was inversely correlated with common PD symptoms such as gait impairment (Tanji et al., 2008). Looking at the data around the distressing personal and relational impact of PD on couples, researchers have offered specific recommendations for providing family therapy using narrative, solution-focused, and emotionally focused therapy (Spencer & Haub, 2018). Other researchers have studied the need for couple-specific support for this population. After studying currently available dyadic interventions for couples facing neurodegenerative disease (NDD), Bannon et al. (2022) proposed a framework for early dyadic intervention in the treatment of NDD to include the following: (a) contextual factors (b) illness-related factors (c) individual and dyadic stressors (d) adaptive coping strategies, and (e) the dyads’ resources.
Patients with a recent breast cancer diagnosis report psychologically distressing symptoms, including feelings of shock, denial, anxiety, and symptoms of post traumatic stress disorder (PTSD) (Fortin et al., 2021). After the initial diagnosis period, couple communication is shown to continue to impact psychological distress of cancer patients. In men diagnosed with prostate cancer, three elements of couple communication (mutual constructive communication, mutual avoidance, and patient demand-partner withdraw) were studied and findings indicated that how couples talk about cancer-related concerns and the degree of avoidance in talking about cancer-related concerns can either facilitate or reduce relationship intimacy, thereby creating a path linking couple communication strategies and psychological distress of cancer patients (Manne et al., 2010). For women in relationships facing early-stage breast cancer, those whose partners offered a reciprocal disclosure, showed humor, or did not offer solutions experienced less distress in discussing a cancer-related topic (Manne et al., 2004).
Couples where one partner has a diagnosis of multiple sclerosis (MS) have higher than normal rates of marital distress, separation, and divorce (Crangle & Hart, 2017). However, in couples where one partner has a diagnosis of MS, those who identified a positive couple identity noted that this alleviated the stress associated with caregiving and helped them make sense of their situation by the couple focusing on being “on the journey together” (Boland et al., 2012). In patients with cardiovascular disease (CVD), the appraised quality of couple relationship appears to matter for patients’ and spouses’ quality of life (QoL; Bouchard et al., 2023). Men who report higher levels of self-disclosure to their wives were less likely to be hospitalized or die the year following a heart attack than were men who reported low self-disclosure (Helgeson, 1991). Liu and Waite (2014) found that when evaluating for cardiovascular risk as measured by hypertension, rapid heart rate, C-reactive protein, and general cardiovascular events, for older women (aged 57–85), higher negative marital quality led to higher risks of hypertension. Additionally, negative marital quality tends to increase the risk of high C-reactive protein (which indicates inflammation and increases the risk of getting coronary artery disease), for both men and women ages 57–85. In studying the impact of marital relationship on cardiovascular risk, actor and partner interactions were found in that for individuals who both viewed and were viewed by their partner as ambivalent, coronary–artery calcification scores (a sign of coronary artery disease) were highest (Uchino et al., 2014). In a qualitative study of couples in a rehabilitation program after a hospitalization due to heart disease event, relational themes emerged as couples reported on experiences as a couple with the subsequent changes in lifestyle (Mahrer-Imhof et al., 2007). Mahrer-Imhof et al. (2007) report that for some couples the illness was seen as a “positive, transformative experience in their lives, bringing them closer together,” while others reported the health event as highlighting a sense of being “disenchanted about each other.” Put together, these studies indicate that relationship quality can impact physiological risk factors of disease and the need for emotional support that facilitates healing after an acute illness.
Supporting the Holistic Treatment of Disease
Couples who are facing the stress of a health diagnosis may benefit from additional interventions to increase collaboration and emotional support. The benefits of a felt sense of care and support from friends, family, and broader social networks have impacts on physical health (Woods et al., 2014). Researchers note a physiological mechanism related to immune functioning and inflammation, along with related depression and affect dysregulation that may explain the effects of social support on health outcomes (Kiecolt-Glaser & Newton, 2001). Pietromonaco et al. (2013) proposed a theoretical model that incorporates couple attachment styles, dyadic processes, health behaviors, physiology, and affect interacting in a reciprocal manner with the health outcomes of each partner. This model can serve as a guide for holistic treatment of cardiovascular or other diseases. Research on various illnesses suggests that couple-based interventions can improve relationship quality and increase the availability of individual and couple-based coping strategies (Dankoski & Pais, 2007). For coronary heart disease, a couple-based intervention has the potential to improve both psychological and physical recovery (Rankin-Esquer et al., 2000). Couples therapy as part of the overall care with those facing a serious medical diagnosis (e.g., dementia or PD) can encourage both couple members to understand and process their situation and learn to flexibly adapt to the changes to their roles and view of self (Robinson et al., 2005). Stiell et al. (2007) propose that EFT, which is based on principles of attachment theory, could be used as part of treatment efforts and long-term support programs for couples affected by chronic illness. With this evidence in mind, we next examine the foundations, goals, and interventions of emotionally focused couples therapy (EFCT), an intervention with a growing body of empirical evidence supporting efficacy (see Beasley & Ager, 2019).
Emotionally Focused Couples Therapy
EFCT, sometimes referred to as EFT, is a humanistic, experiential, systemic, attachment theory-based therapy model designed to help clients reduce relational conflict and unhealthy call and respond cycles to create a safe and stable emotional connection, which has been compromised previously by conflict (Beasley & Ager, 2019). EFCT is effective in strengthening relational connections and interpersonal bonds, which every human is hardwired to need as well as to support strong attachment ties, which can emotionally buffer stressors and assuage chronic feelings of loneliness and isolation (Greenman & Johnson, 2022). EFCT is a model containing three stages and nine steps, and although it is generally manualized in terms of these stages, the therapist considers the changes in individual and couple dynamics occurring throughout treatment, addressing general relationship distress or more serious attachment injuries or traumatic events (Adamson, 2013). Grounded in attachment theory, EFT conceptualizes distressed relationships in terms of insecure bonds, where attachment needs for physical or emotional closeness, comfort, and security, particularly during crisis, are not being met (Johnson, 2004). The overarching goal of EFT is to promote a secure bond between partners, which, in turn, facilitates emotional connection and resilience in the face of adversity (Naaman, 2008). EFCT therapists sensitively use knowledge of attachment styles and needs to provide individualized treatment for each couple, helping more avoidant partners to learn and access their emotions and attachment needs, while the angry or critical traits of the more anxiously attached partner are validated and soothed, thus enabling the couple to learn to reach for and connect with each other (Fitzgerald & Thomas, 2012). EFT demonstrates a significant effect size (d = 0.93) from pretest to posttest, indicating a large positive impact on relationship, which is shown to be sustained up to 2 years with “modest decline” (Spengler et al., 2024). Couples treated with EFCT show significant changes in how the brain responds to threats when compared to those not receiving treatment, emphasizing its impact on emotional security and supportive intimate alliances on the ability to regulate threat states (Johnson et al., 2013). Additionally, Johnson et al. (2013) link these findings to the concept of load sharing, looking at how proximity to relational partners decreases the response to threat due to co-regulatory mechanisms. Because a serious medical condition and chronic illness can introduce a feeling a threat into a person's life, it makes sense that increasing the security of relational bonds through EFCT, has the potential to improve QoL and treatment results of those suffering with a difficult medical diagnosis. Stiell et al. (2007) propose that EFT, could be used as part of treatment efforts and long-term support programs for those people affected by illness.
Studies using EFCT with couples experiencing illness show how the intervention helps couples improve the emotional quality of their relationship through the expression of vulnerable emotions such as fear, sadness, and loneliness to each other and working to meet one another's attachment needs (e.g., safety, comfort, and security), despite the new and limiting experiences the illness introduced into the relationship (Chawla & Kafescioglu, 2012). Dansby Olufowote et al. (2022) integrated an interracial couple with medical family therapy using EFCT, suggesting the following as treatment goals: (1) assess the effect of illness on their relationship (2) make explicit the role the illness plays in their interaction cycle (3) help the couple identify the roles race, culture, and faith play in the management of the illness and in their relationship distress; (4) Promote and facilitate agency; and (5) increase emotional connection and intimacy in couple relationship.
EFCT was used to support a couple where one partner was diagnosed with PD (Spencer & Haub, 2018). The couple experienced greater ability to access and share with one another their underlying attachment-related emotions and found support in one another. The couple reported an ability to process their anger, disorientation, fear, and frustration that arose from the progression of the disease and reported an increase in happiness and confidence in their ability to navigate the illness (Spencer & Haub, 2018). These and other case examples and conceptual papers using EFCT motivated us to systematically review the literature for studies about the efficacy and experience of EFCT for couples where one partner has a serious medical diagnosis. The purpose of this paper is to present the findings from our systematic review on this topic.
Method
Eligibility Criteria
We predetermined the inclusion and exclusion criteria. The inclusion criteria were the scope of our review to answer the research question. The research question we are hoping to answer is finding out the effectiveness of a couple-based intervention based on EFT on couples affected by a medical health condition. The exclusion criteria excluded any and all articles that were conceptual articles or literature review articles. We decided to only include academic journals that were either qualitative or quantitative studies. For the intervention aspect, couple interventions that were based on EFT principles were included. For example, Healing Hearts Together (HHT) is a specialized program derived from EFT to help couples who are affected by cardiac disease (Tulloch et al., 2021). Any and all interventions that utilized EFT components were reviewed for inclusion in the final write-up. Furthermore, with the population component, we wanted to look at how a therapeutic model such as EFT has an effect on medical health conditions. Because EFT is often linked with mental health illnesses, we excluded any and all mental health-related concerns and focused only on physical health concerns. The final inclusion and exclusion criteria for this paper include research articles published within approximately 10 years of this systematic review, which was conducted in the fall of 2024.
Search Strategy
MEDLINE/PubMed, PsycArticles, APA PsycINFO, ERIC, EBSCO, and Psychology and Behavioral Sciences were all the databases that were utilized for the search process of this systematic review. The search terms that were utilized were “Emotion* Focus* Therapy,” “Emotion* Focus* Couple* Therapy,” disease, cardiovascular disease, Parkinson's, chronic illness, neurodegenerative, EFT, EFCT, EFFT, EFMedFT, Healing Hearts Together, illness, and disorder. The reason for using search terms like “Emotion*,” “Focus*,” and “Couple*” is to use the asterisk function within the advanced search engine that searches all variations of the word. For example, Emotion* will find articles that include “Emotion” and “Emotionally.” The search terms were paired in a way that matched a condition with an intervention. The advanced search function was used to ensure that the articles that were being pulled up included both the intervention and the condition we were looking for. The search process also included hand-searching, where we looked through the reference lists of different research articles to see if the titles fit with our inclusion/exclusion criteria. See Figure 1 for a detailed description of our search process. Another method of hand-searching that was utilized was looking at resources from the EEFT website that may fit within our search criteria.
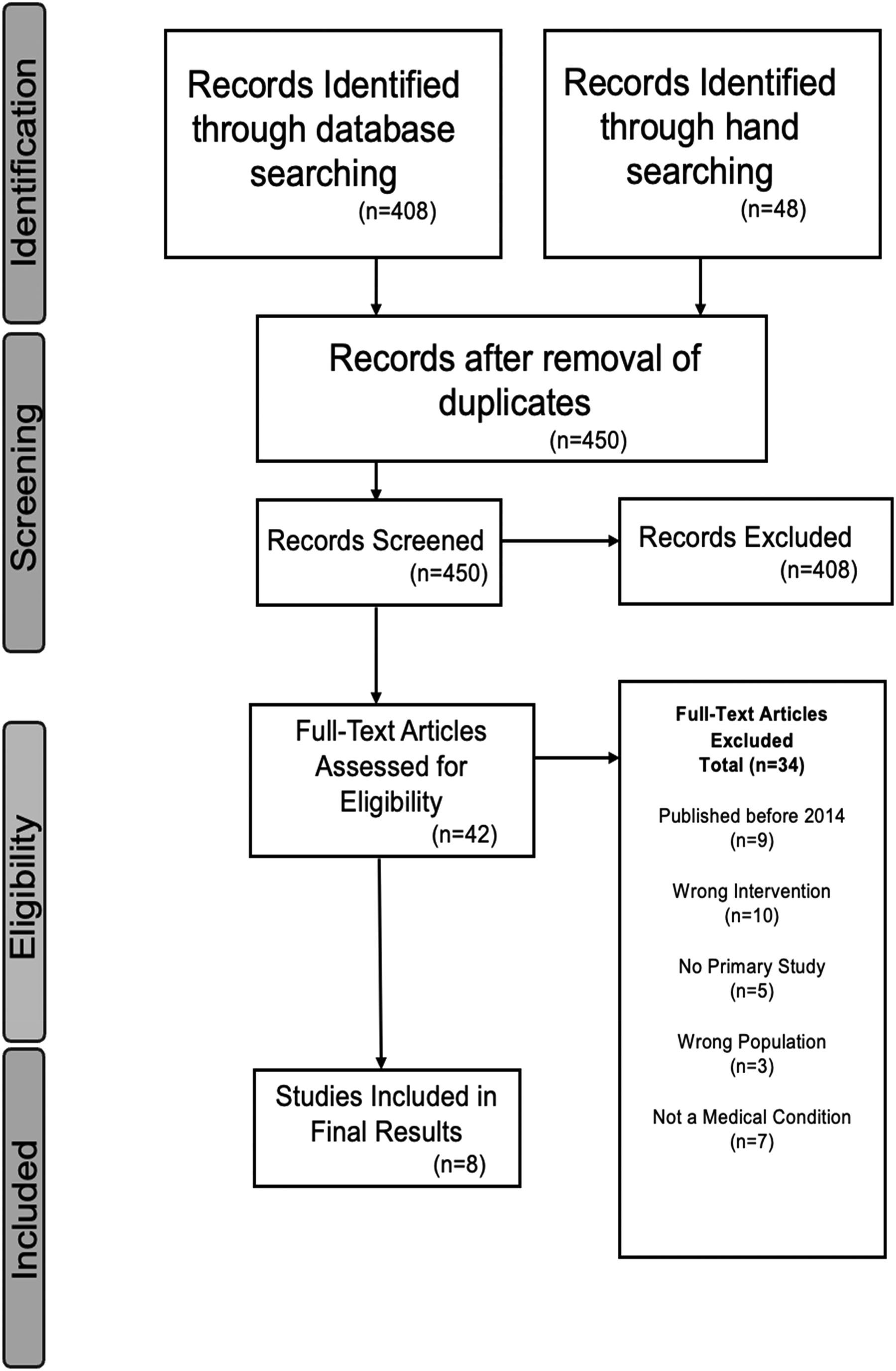
Identification of studies via databases and hand searching.
Results and Discussion
Out of the eight studies that we retained to include in our systematic review, seven followed a quantitative design of some form (Ghedin et al., 2017; McLean et al., 2013; Najafi et al., 2015; Oladi et al., 2024; Petzke et al., 2022; Tulloch et al., 2021; van Diest et al., 2023). The remaining study was a qualitative design, with a pre- and postintervention assessment (Mendelson, 2024). That same study had a single couple case design (Mendelson, 2024); the remaining studies all had double-digit participants (N). Each study was different in applying quantitative design (see Table 1 for a detailed snapshot of study characteristics). Three studies included in our findings had a control group in their design (McLean et al., 2013; Najafi et al., 2015; Oladi et al., 2024). The studies had a myriad of settings they took place at, such as hospitals (Ghedin et al., 2017; McLean et al., 2013; van Diest et al., 2023), care centers (Tulloch et al., 2021), at-home (McLean et al., 2013), and even virtually (Mendelson, 2024). Participants were included from across the world, from places such as Italy (Ghedin et al., 2017), Iran (Oladi et al., 2024), Canada (Tulloch et al., 2021), and the Netherlands (Petzke et al., 2022; van Diest et al., 2023), showing the diversity of practice and application across different populations and the inclusivity of the research.
Study Characteristics: Design, Control, Participants, and Setting.
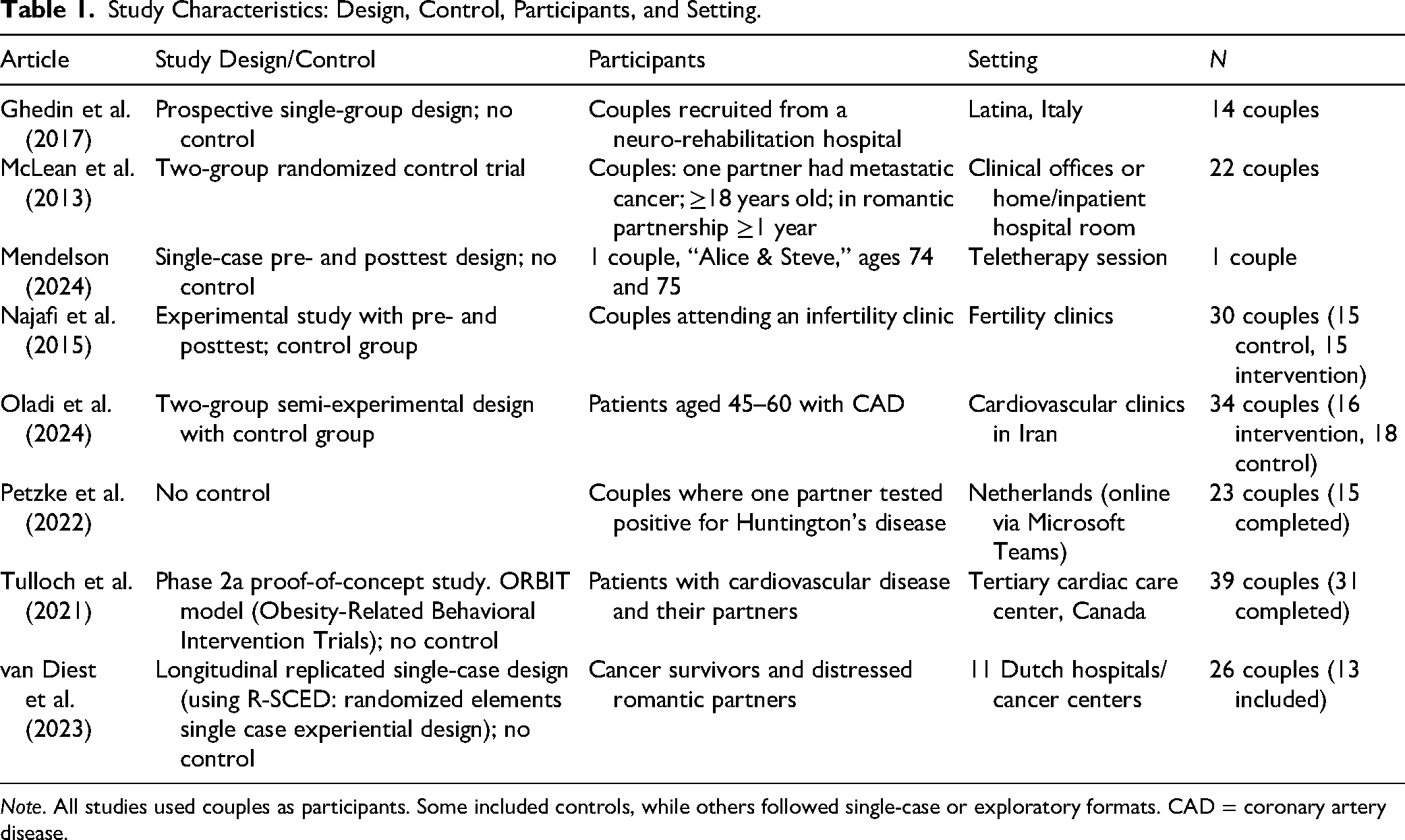
Note. All studies used couples as participants. Some included controls, while others followed single-case or exploratory formats. CAD = coronary artery disease.
There was some variability in the intervention time frame across studies. The majority of studies followed a time frame between 8 and 12 weeks with weekly sessions. However, some studies deviated. Outlier studies were those of Petzke et al. (2022), which implemented a condensed approach of only four sessions, and Mendelson (2024), which extended the intervention to a comprehensive 20-session model. These outliers highlight the range of methodological approaches within the research, potentially influencing the comparability of outcomes.
The primary base intervention for all studies was EFT. Most of our included studies focused on the utilization of EFCT (Mendelson, 2024; Najafi et al., 2015; Oladi et al., 2024; Petzke et al., 2022; Tulloch et al., 2021; van Diest et al., 2023). Two studies used the HHT program, a collaborative effort created by Heather Tulloch in partnership with the University of Ottawa Heart Institute (Tulloch et al., 2021), as their intervention components (Oladi et al., 2024; Tulloch et al., 2021).
Study Outcomes
Many of our study outcomes were significant and positive. Most reported that EFT/EFCT significantly affected the distress levels of couples in which at least one partner had a physical health complication. Participants in the studies often experienced psychological issues stemming from health concerns, which were alleviated using EFT/EFCT intervention. Studies showed overall improvement in many aspects of relational health, such as emotional expression (Ghedin et al., 2017), marital function (McLean et al., 2013; Mendelson, 2024), and irritability (Oladi et al., 2024). There were statistically significant increases in QoL (Tulloch et al., 2021), couples’ relationship satisfaction increased (Petzke et al., 2022), and their secure bond was strengthened (Najafi et al., 2015). Research shows there was even an increase in partner responsiveness towards intimacy (van Diest et al., 2023).
Several studies showed that improvement had a lasting effect on the participants physically and emotionally. Ghedin et al. (2017) found that the patient's physical response to their NDD improved poststudy and during EFT sessions. At follow-up in studies by McLean et al. (2013) and Najafi et al. (2015), participants did not show a decline in marital function or positive affectional expression but maintained clinical improvement. In Petzke et al. (2022), the use of the Hold me Tight (HmT) program significantly increased the mean score of hyperthymic temperament (positive); however, the changes observed at follow-up were less pronounced than initially observed. Overall, research indicates that most participants benefited from EFT/EFCT interventions. See Table 2 for a complete reference of study results.
Intervention Details and Results.
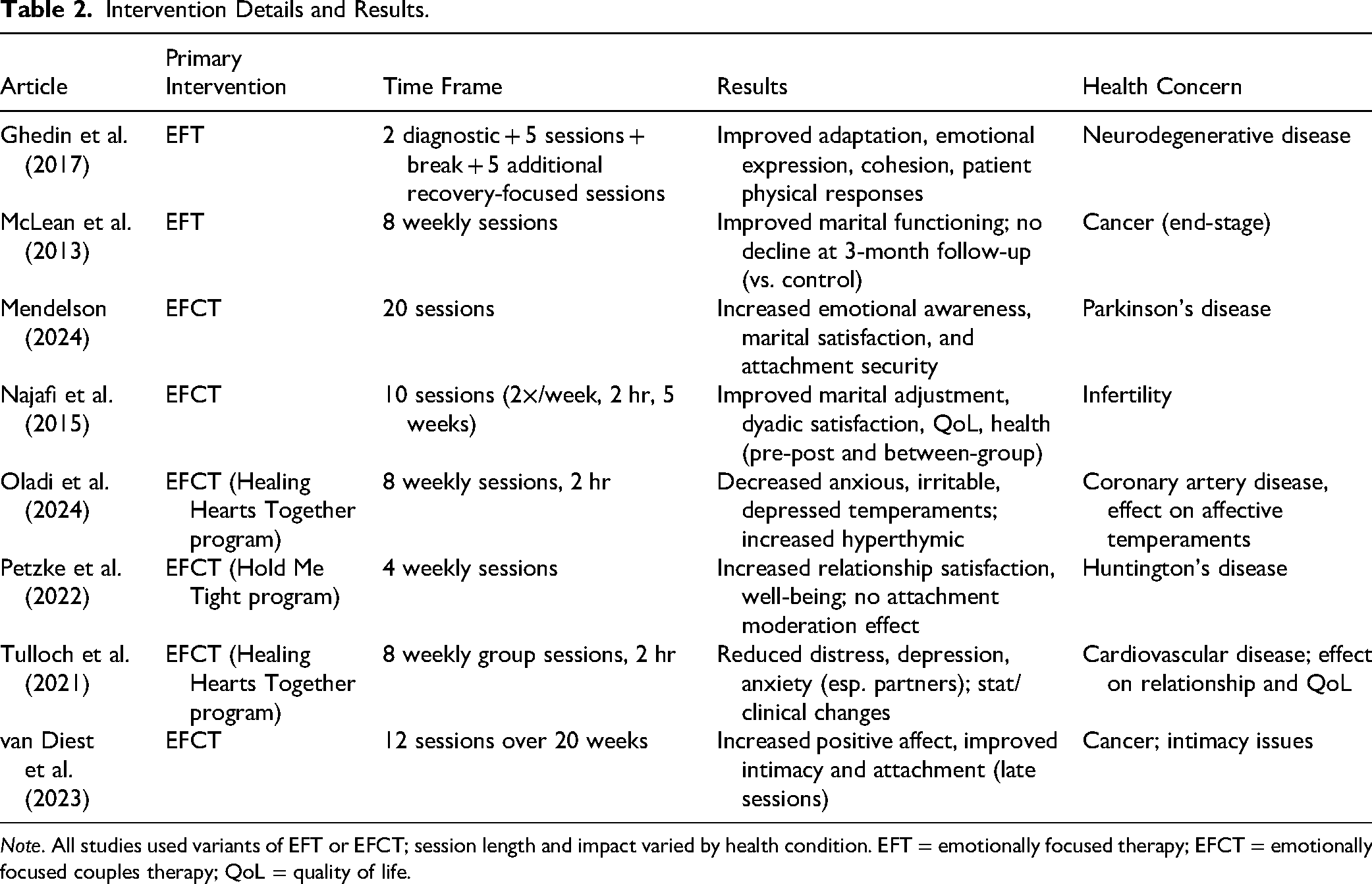
Note. All studies used variants of EFT or EFCT; session length and impact varied by health condition. EFT = emotionally focused therapy; EFCT = emotionally focused couples therapy; QoL = quality of life.
Strengths and Limitations
A strength of this systematic review is how the studies covered a diversity of medical conditions. Cancer, coronary artery disease, PD, CVD, NDD, Huntington's disease, and infertility were all mentioned. In fact, all our included studies had different health concerns, with the exception of cancer as a diagnosis, which had two (McLean et al., 2013; van Diest et al., 2023), showing the contributions that EFT can have on couples, with a breadth of medical diagnoses. Another strength of this systematic review is that in our search process, the studies were thoroughly examined because of the vernacular changes that have been made to EFT. As the search process progressed, we began to notice how there were multiple name variations of the same intervention. EFT was often referred to as EFCT, EFT-C EFT, and Emotionally Focused MedFT (Dansby Olufowote et al., 2022; Ghedin et al., 2017; Mendelson, 2024; Petzke et al., 2022). Furthermore, there were different types of intervention that were birthed out of EFT/EFCT, such as the HmT and the HHT programs. Lastly, there is a completely different technique that uses the same acronym, EFT, called Emotional Freedom Technique, which further complicates the search process. Because of these varying names of the interventions that we are looking for, it added to the rigors of the search process, resulting in the final review only including studies using EFT with couples. Lastly, most of the studies that were covered in the final write-up of this review are rigorous quantitative studies. Although there are not many studies to pull from, seven of eight studies present concrete results as a quantitative study showing measurable findings poststudy. As far as reviewing the effectiveness of EFT/EFCT, these studies generally show a strong, rigorous design with promising findings. See Table 2 for a detailed description of interventions and results.
Due to our inclusion and exclusion criteria being specific, the scope of our review became narrow, which only allowed us to include a total of eight studies in our final write-up of results and discussion. Although there were many studies with EFT or EFCT as an intervention that deals with mental health issues, most of them were excluded in order to focus on medical/physical conditions. There simply were not many recent studies examining EFT as an intervention for couples with medical conditions such as cancer, NDD, and infertility (see Figure 1). Although the results of this review seem promising, there are not enough interdisciplinary efforts marrying mental health and medical studies on this topic. Another limitation of this review is the cohesion in the name of the interventions. With EFT, there are a few iterations of the EFT model (Dansby Olufowote et al., 2022; Ghedin et al., 2017; Mendelson, 2024; Petzke et al., 2022). Although the search process was thorough, there is no guarantee that all forms of EFT were included for this review. There is a need for a coordinated effort in the mental health field to synchronize the name of the intervention so that the search process can be easier for further interdisciplinary efforts.
Implications for Practice and Research
Despite an increase in research in recent years supporting the link between attachment and medical conditions (see Maunder & Hunter, 2001; Pietromonaco et al., 2013) and the research showing the efficacy of attachment-based EFCT (see Spengler et al., 2024) on helping couples achieve attachment security, there were limited studies found on the efficacy of EFCT in the treatment of couples and physical health conditions. Future research should focus on the outcomes of EFCT on attachment security, relationship satisfaction, and the impact of these changes on the mechanisms of altered stress physiology, increased use of external regulators of affect, and altered use of health-protective behaviors that all increase disease risk (Maunder & Hunter, 2001). Additionally, findings should be presented at conferences and in journals that couple's counselors and therapists frequent to clearly disseminate findings that can be used in practical clinical settings.
Recommendations from the studies suggest that similar research and larger randomized control trials be conducted with different populations and presenting concerns (McLean et al., 2013; Najafi et al., 2015). Additional suggestions call for more qualitative studies to further understand the mechanism of EFCT interventions and how they assist in the reduction of symptoms of depression and hopelessness in patients (McLean et al., 2013), while others contend interventions for those suffering from heart disease should move beyond patient-only treatment towards more integration of the spousal dyad using EFCT as a promising approach (Tulloch et al., 2021). Other authors suggest EFT-based programs can be a valuable addition to psychological care following a diagnosis of a NDD (Petzke et al., 2022). Another study found that EFCT can be effective in health maintenance and promotion, as well as in enhancing the QoL for patients with CVD (Oladi et al., 2024). van Diest et al. (2023) found promising results for EFCT and cancer patients and called for more randomized control trials with larger sample sizes with dyads dealing with different types of cancer, specifically looking at the change mechanisms resulting from the intervention. Other authors suggest that more qualitative studies could be done to understand the lived experiences and challenges of the introduction of aging and illness into a relationship and how couples can grow and change through a process of EFCT (Mendelson, 2024). Finally, the authors of one of the studies suggest that using EFT with couples in a neurorehabilitation facility means working on the resilience of both the patient and the partner, helping the couple to develop a process of change and support, and engaging the hope and resiliency of both as they face the challenges ahead (Ghedin et al., 2017).
Despite the limited availability of studies looking at EFCT for the treatment of medical diagnosis specifically, there is enough evidence of the importance of adult attachment security on physical health and the efficacy of EFCT in increasing attachment security for couples’ clinicians to support this population through this modality. Those already trained in EFCT might enrich their practice through the study of the articles related to attachment and physical health.
Additionally, couples’ counselors and therapists who desire to specialize in couples with specific medical diagnosis (e.g., cancer, PD, heart disease, MS) could immerse themselves in that diagnosis by attending conferences and local community events supporting patients with that diagnosis. It is vital that counselors and therapists receive formal training in EFT to gain competency and then to practice this model with fidelity, even as they integrate the uniqueness of the specific medical diagnosis.
Conclusion
Our systematic review includes studies using EFCT-based programs for a variety of medical diagnosis with results showing positive outcome effects. In this systematic review, we identified the primary interventions utilized, the time frame for treatment, the diagnosis of the couple member, and the results of the findings from each study. More qualitative and randomized control trials with this intervention for this population could potentially add valuable data to guide clinical practice. Supporting couples who are navigating the enormous challenges resulting from health diagnosis and noticing research linking relational health and physical healing and well-being makes this subject a valuable and impactful area of clinical practice and further research.
Footnotes
Acknowledgments
The authors would like to acknowledge Dr Jonathon Ohrt for editorial assistance and guidance with this paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.