
Abstract
Introduction
Family members play a crucial supporting role in the provision of care to loved ones with pituitary conditions. Concerningly, their voice remains largely unrepresented within empirical research. Forming a group of rare endocrine conditions (McDermott, 2019), symptoms of pituitary conditions tend to present differently, contrasting markedly from one person to another and bestowing considerable clinical burden due to their chronic nature (Crafa et al., 2021). Examples of pituitary conditions include Cushing's disease, acromegaly, adult growth hormone deficiency (AGHD), hypopituitarism, hypogonadism, prolactinoma, craniopharyngioma and Sheehan's syndrome. All of which effect the production of hormones and hormonal control, with some people living with multiple conditions (Norman et al., 2021). People with pituitary conditions can require a great deal of support and understanding from family members in relation to the biopsychosocial dynamic factors experienced on the pathway through diagnosis, and the life course beyond (Biermasz, 2019; Norman et al., 2022; Su et al., 2022).
Whilst studies are emerging which evaluate endocrine condition-specific patient journey measures (Assefi et al., 2023), a limited number of studies have considered the psychosocial impact pituitary conditions have on family members explicitly (Andela et al., 2019; Inagaki & Eisenberger, 2012; Underwood et al., 2019). Taking steps to rebalance the focus of support, specific legislation has recently been introduced. The England Health and Care Act (2022) places a duty on National Health Service (NHS) Trusts in England to involve patients and their carers in planning hospital discharge (Department of Health & Social Care, 2022). This marks a critical point at which caring responsibilities are often assumed or increased for family members (Hagedoorn et al., 2020; Slatyer et al., 2019). Subsequently ensuring family members are well prepared to meet a loved one's care needs in the interest of their health and protection is of vital importance (Oxford, 2023). By legislating for improved patient and family care strategies, the diverse needs of those living with pituitary conditions should be well supported (Biermasz, 2019; Heckemann et al., 2023), lessening the burden on otherwise overwhelmed healthcare services (Jackson et al., 2019). Yet minimal research has been undertaken with families in the context of pituitary care, to better understand how their own mental health and needs could be better protected (Holman, 1987).
Approximately 6.5 million carers are recognised in the United Kingdom (UK) with a predicted increase to nine million by 2037 (Greenwood et al., 2019). In context, an estimated 10% of the population have pituitary adenomas (Melmed et al., 2022) with 1% of the UK population previously found to be living with a pituitary condition (Pituitary Foundation, 2014). Many of whom require care and support to become empowered in the management of their specific condition (Webb et al., 2020). To manage the challenges faced by both patients and their loved ones, family focused strategies have been promoted through proactive interventions that model ‘think family’ approaches (Woodman et al., 2020), situating the welfare of families at the heart of integrated services (Department of Health, 2012). The social construct of these approaches has evolved during the latter half of the 20th century (Smith et al., 2002). Broadening the narrative of the psychosocial and economic challenges faced by families who become caregivers, seeking to equip them with sufficient competencies to support their own emotional health and well-being (Vicarelli & Bronzini, 2009).
However, in the UK, several studies have concluded that ‘think family’ approaches, whilst espoused into social policy, have yet to be adequately integrated into health and social care practice (Coyne, 2013; Smith et al., 2015, 2020). Furthermore, requiring support themselves, family members are often left to navigate the complicated, unfamiliar and complex journey of diagnosis and condition management alone (Baumbusch et al., 2019; Rolland, 2018). Exploration of dynamics and interplay of kinship relationships have been explored in studies with other general long-term conditions (Cleary et al., 2022; Smith et al., 2022). The authors’ scoping of the literature revealed a notable lack of similar research in the specific and complex area of pituitary conditions. Subsequently, a large population responsible for meeting the care and support needs of those with pituitary conditions remains underrepresented.
This study offers a unique focus on the experiences of family members who provide care for a loved one with a pituitary condition, building on the work of Norman et al. (2021) who conducted a large-scale qualitative study of 748 participants living with a pituitary condition. Their findings recognised the patient experience of living with a specific hidden disability, concluding that invisible symptoms impact considerably on one's quality of life. Four key themes identified emotional and behavioural issues, appearance distress, cognitive effects and social isolation, as the main factors impacting life after diagnosis. Additionally, a patient satisfaction survey conducted for the Pituitary Foundation (Forrest et al., 2017) identified 60% of respondents had experienced a negative impact on personal relationships because of their pituitary condition. Several of the participants reported that their relationships had completely fallen apart. This highlights the importance of investigating the direct experience of family members to inform strategy and policy makers when developing appropriate tailored support with a view to empowering patients and their families, offering stability and backing so that family relationships continue to thrive.
The management of pituitary conditions is challenging due to the complex and varied nature of condition-specific symptoms. As an example of the complexity – a person initially diagnosed with Cushing's disease might receive treatment which leaves them with Addison’s disease, a life-threatening condition where they require monitoring to prevent death from adrenal crisis. Someone else might be diagnosed with acromegaly the treatment for which might leave them with no pituitary hormones and therefore in need of extensive hormone replacement. Services need a better understanding of the impact providing care for those with pituitary conditions has on their family members to improve support for them and their loved ones effectively. Therefore, the current study employed a qualitative approach to understand (a) the experiences of family members whose loved ones have a pituitary condition and (b) the information and support needs of family members.
Methods
Design
Participatory approaches (Aldridge, 2016; Cargo & Mercer, 2008; McNiff, 2017) involve working in co-operation with relevant groups and organisations, in this instance, between the Pituitary Foundation, and members of the pituitary community. Family members shared their views as experts in their knowledge and experience (Jagosh et al., 1999). The methodology was selected to provide a ‘voice to the voiceless’ (Aldridge, 2016, p. 378; Britzman, 1989) serving to empower the expression of participants in the creation of rich contextual data which to date remains absent from this specific field of enquiry.
Ethnographic studies provide a lens of transcendental phenomenology (Cerbone, 2014; Husserl, 1981) complemented by documentary data (McNiff, 2017) including scoping exercises of legislation and literature, informal interviews with families, and journalling of the researcher, along with reflections from participants in the form of ‘member checking’ (Harvey, 2015). The lead researcher's own journal considerations provided a platform for any preconceived values and judgements held about the research process and research question. Janesick (1999) describes journaling as a method of receiving feedback from oneself which acts as a medium for recognising precisely what is required from the qualitative researcher.
Participants
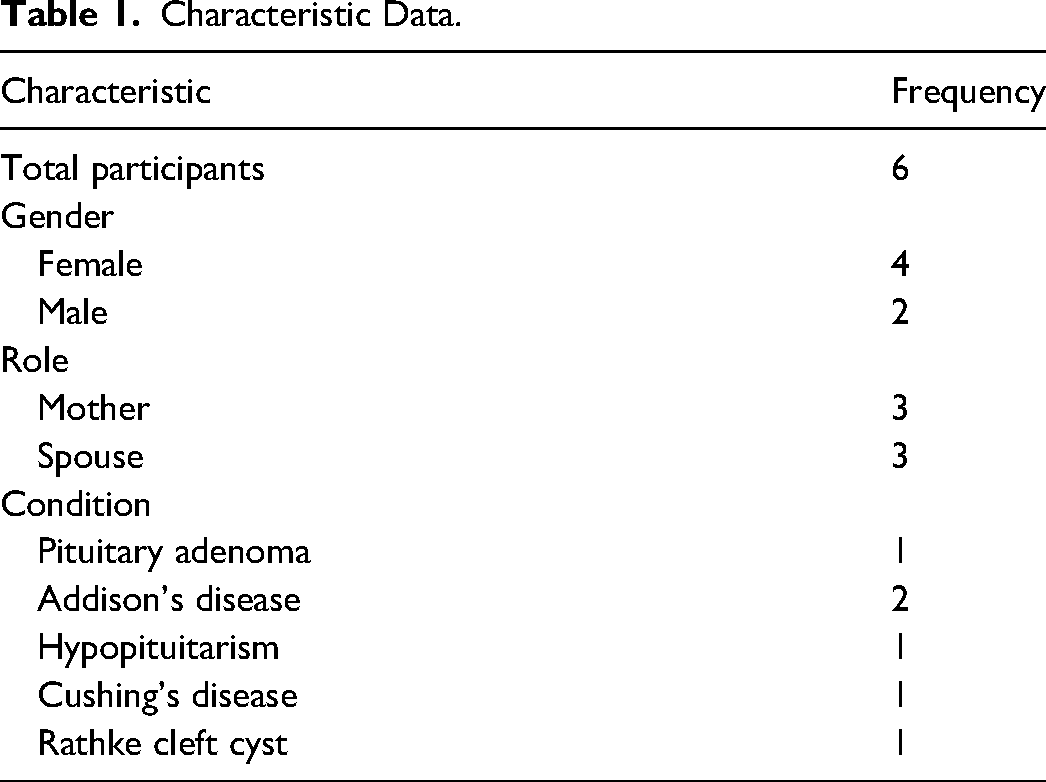
The participants were adults living within the UK who were family members of those living with a pituitary condition. Participants were recruited by means of convenience sampling to reach a defined sample of a specific group (Stratton, 2021). Advertising took place through the Pituitary Foundation via their magazine, Pituitary Life and a nominal donation was made to the Pituitary Foundation from the university research expenses fund. The advert stated the inclusion criterion that participants’ family members have a diagnosed, specified pituitary condition. Six participants were recruited (see Table 1 for demographic information) in-line with Hennink and Kaiser's (2022) systematic review which concluded small sample sizes are sufficiently able to embody rich narratives of experience fully.
Characteristic Data.
Ethical approval was granted in accordance with the university (2022) ethical protocols, compliant with the standards outlined by the British Psychological Society (2021). Recognising the potential for relationships to feel compromised, attention was given to bias and subjectivity of the researcher and participants who were drawn from a narrow third sector pool (Norman et al., 2021). However, Braun and Clarke (2022) challenge the assumed potential for such bias and respect the subjective nature of the research process as a valuable resource for analysis following Gough and Madill (2012).
Data Collection
Participants were invited to take part in a one-to-one semi-structured interview where they were asked to talk about their experiences of having a relative with a pituitary condition. They were also asked about their encounters regarding accessibility and availability of services and support. Interviews took place using online communication methods including Teams or Zoom for no longer than 60 minutes. Each participant was provided with a research information sheet prior to the interview, outlining key aspects of the study and ethical rights to ensure participants were able to provide informed consent. Once the interview was complete participants were provided with a debrief information sheet which offered contact information for support should participants require further communication following the study or experience any distress.
Participants were subsequently invited to member check transcriptions to ensure data was truly representative of their voice and contribution (Harvey, 2015). Participants were provided with the transcription and given opportunity to comment, applying synthesised member checking (Harvey, 2015), to ensure greater credibility and rigour to the qualitative process (Lincoln & Guba, 1986).
Arksey and O’Malley's (2005) mapping techniques were utilised to review the breadth of relevant literature, as this specific area of research is underdeveloped. The review laid the foundations on which to build the research, mapping the key areas of family and patient care practice, policy and legislation. These sources provided documentary data (McNiff, 2017) which gave an analytical framework for the existing research field.
Analysis
Reflexive thematic analysis was undertaken to identify themes and emotional touchpoints within the transcribed data (Braun & Clarke, 2006). Seeking truth in realities through interpretation of meaningful experiences, the data was reviewed numerous times. This provided the opportunity to make meaning of the lived experience of the family members (Schwandt, 1994).
Results
Findings
Four themes emerged illustrating the collective experience of family members: (a) experts by experience, (b) burden of mental load, (c) misconceptions of care create barriers and (d) battling for support. There was also an overarching theme of overwhelm in pursuit of understanding. Positive experiences were rooted in their shared pursuit to seek knowledge and expertise. This came about due to poor access to support and advice often unavailable from general healthcare professionals. Negative experiences included emotional burden and the impact of such on-kinship relationships (see Figure 1).
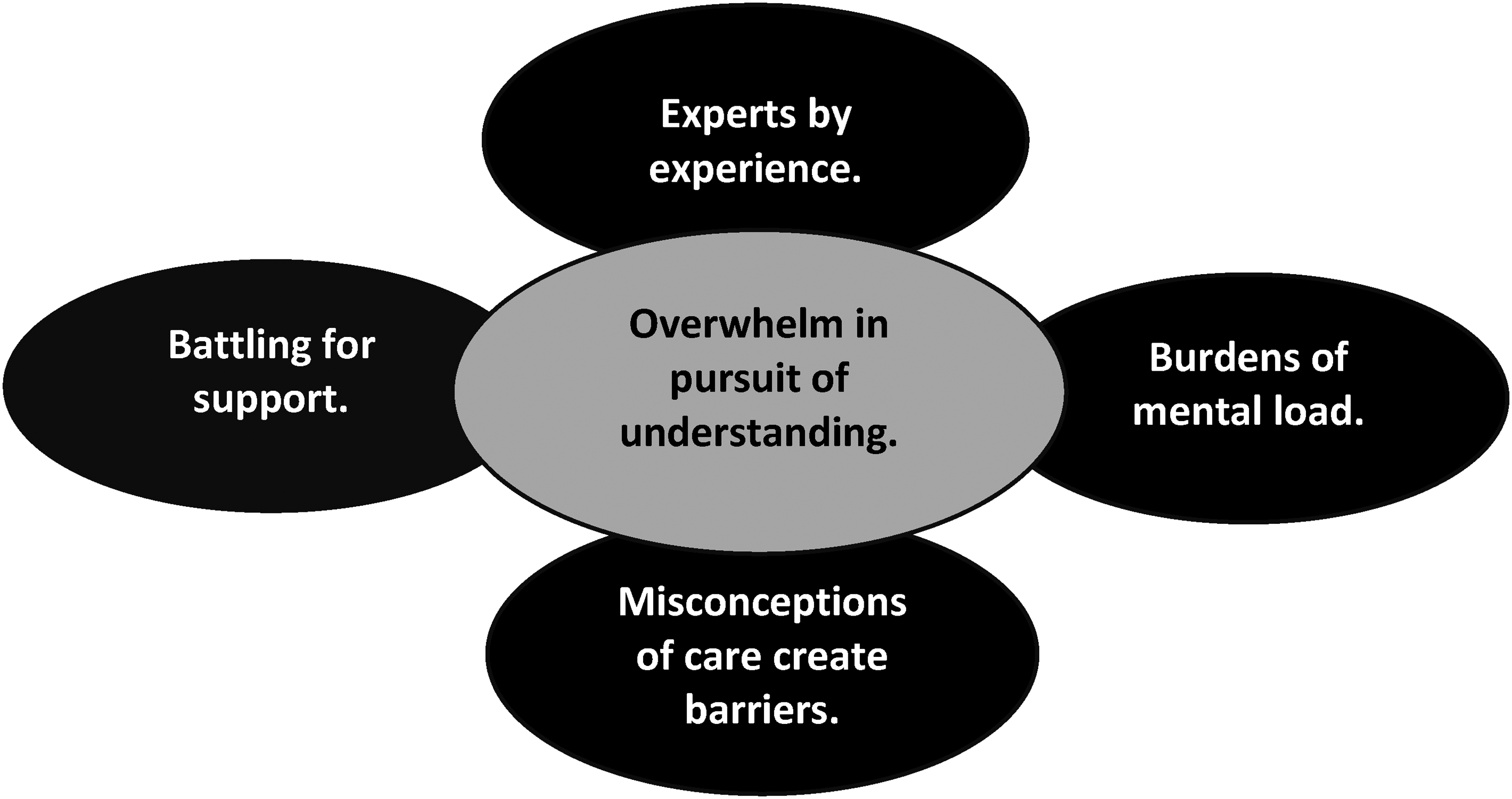
Thematic map.
These themes are described below; all study participants have been provided with a pseudonym to protect their identities.
Experts by Experience
Family members became experts by experience as a consequence of the time taken to receive a diagnosis, and due to a lack of access to specialist support post-diagnosis. Compelled to seek out information fed by curiosity, and lack of tailored support, family members become highly knowledgeable regarding the management of specific pituitary conditions. Expert knowledge in the care of their loved ones enables family members to make sense of what is happening as symptoms often lead to lifestyle changes and adaptations concerning treatment. Utilising a sense of agency, knowledge helps family members gain control over events which are otherwise overwhelming. This results in feelings of empowerment in an otherwise disempowering system. Consequently, family members use their deep knowledge of their loved one's condition to inform professionals and other services at critical points, such as reviewing condition management, or alerting healthcare professionals to their family member's exact health needs. … that some of the pituitary conditions are so rare, paramedics do not always seem to be particularly well informed, nor are the call handlers, when I’ve had to phone 3 nines to get paramedics here and you're flagging it up as being a, you know, a crisis issue. It's an adrenal crisis, so that becomes difficult having to try and explain it all… (David).
Family members consistently appreciated support available through the Pituitary Foundation. Having access to support groups where they could share their knowledge and experiences helped to provide a sense of community. This validated their experience, whether positive or negative, and as such helped to alleviate feelings of isolation. ‘It gave us an appreciation that other people within our support group, as it were, have different issues but similar experiences’ (David).
Burden of Mental Load
Significant mental load is commonly experienced by family members. The weight of bearing witness to the effects pituitary-related symptoms has on their loved ones caused a great deal of anxiety. The journey of unknowing when waiting for a diagnosis, and lack of consistent support post-diagnosis led to intense frustration. Family members reported feelings of being misunderstood by health care professionals, describing a gross lack of communication from specialists, and poor advice in the general healthcare domain. This frequently leads to devastating consequences regarding the treatment and management of specific conditions. As a result, family members were placed under tremendous emotional burden which impacted upon their own mental health and well-being with participants sharing experiences of anxiety and depression. I take antidepressant and anxiety medication now. This was very much a gradual thing, you know it’s been really sensitive, in fact we only discussed it last night, it's been with us since 2012 so it's a good ten years, it's the sort of thing that gradually wears you down and gets to you………. but we’ve adapted, and we accept it, but we don’t like it. (David)
‘You’re cut off. There's no. There's no support. There’s no psychological counselling. There's no pinpointing to somebody to support the family and it's like we’ve done our job and and now now you move on’. (Marie)
Misconceptions of Care Create Barriers
Family members’ perceptions of care and caring often created barriers to accessing support. They did not consistently view themselves as carers, justifying this with the notion that loved ones were often able to lead their lives independently providing their respective pituitary conditions were generally well managed.
Spousal relationships and maternal/paternal relationships are understood to be part of a wider caring role that encompasses general support as part of being a committed husband, wife or parent. Therefore, the perceived caring role was considered to be one of additional support, not necessarily separated from their primary kinship role. ‘I wouldn’t say that I’m a I’m a carer. I’m just his mum that supports him when he needs to know what's going off’ (Sophie). Consequently, family members did not consistently engage with services targeting support for carers as they did not always define themselves in that way. ‘No, I’ve not. I’ve not bothered. I’ve just kind of muddled on and and got myself through it in a in a way’ (Sophie).
Family members held great concerns regarding the impact pituitary conditions had on their wider family unit. This was weighted significantly against any concern for their own wellbeing. Whether they viewed their role as carer, supporter, or tolerator, they each described mediating the impact specific conditions had in relation to other members of their families, be those children, in laws, siblings, extended family members or close friends. As a result, family members described feelings of isolation, loss of friendship groups, and not wanting to overshare or burden others. Some held perceptions of their loved ones being treated differently as a result of their condition, and most found difficulty in maintaining stable family relationships. Collectively the narrative strongly offered the yearning of family members to protect their loved ones, and a desire for greater understanding for those they care for and about ‘… it's took a lot to actually get everybody to understand what's wrong with him’ (Sophie). These experiences resulted in feelings of isolation and loneliness, serving as barriers to accessing appropriate support, both internally through family and social networks, and externally.
Battling for Support
Family members consistently described an apparent lack of medical knowledge and support for their loved ones from healthcare professionals. By association, they felt under-supported in their caring or kinship role. Consequently, family members advocated for improvements in general knowledge and awareness of pituitary conditions from health care services. This would alleviate much of the mental load carried by family members. Consistent calls for clear, accessible, condition-specific information, were offered during interview discussions as the rarity of specific conditions and their symptoms resulted in family members fighting for appropriate information and service provision. ‘I suppose a bit of me feels a bit bitter and twisted because it's been quite a battle because his condition isn’t well known’ (Jane). Family members needed greater access to specialist healthcare professionals outside of the support received from the Pituitary Foundation. Family members recounted their variable encounters with different healthcare authorities across the UK in a pursuit to find hospitals in their geographical area who were able to provide specialist treatment. This added to the sense of overwhelm and subsequent negative impact on their own mental health and wellbeing.
Accessing support from the Pituitary Foundation was therefore invaluable, helping family members to share their personal experiences with others who had gone through similar situations and enabling their loved ones to identify with others. However, it was noted that support tended to be more suitable for older populations with a lack of tailored support fitting the needs of adolescents and young adults. Despite this, specialist knowledge and accessible support was greatly appreciated through a range of means including face-to-face, telephone and monitored online platforms. This support and expertise were encouraged to be shared more formally across healthcare services. In most cases support from the Pituitary Foundation had been discovered through the family members’ own research and not through routine signposting.
Overwhelm in the Pursuit of Understanding
Family members consistently described feelings of overwhelm, stress, anxiety and depression when navigating the often-unpredictable nature of chronic symptoms both pre- and post-diagnosis.
Family members sought out their own information, often from internet sources and online support groups in the absence of accessible, condition-specific information from healthcare services. As a result, healthcare services were missing opportunities to reduce the mental load experienced by family members. They required communication and reassurance in order to support themselves and their loved ones. At times participants described a sense of not being heard or believed, further compounding feelings of overwhelm and frustration. ‘I felt that I was perhaps blamed for his psychological mental health, that perhaps I was just not tolerating or moaning and whining, but I was not tolerating, moaning, and whining cause he was really hard to live with because he was psychotic really’. (Marie)
The consequence of family members seeking support more broadly from online sources can fuel overwhelm. Increasing feelings of stress and anxiety in the quest to better understand and support their loved ones was once described to the point of obsession. The risks associated with endeavours to seek understanding resulted in family members taking advice from unregulated online sources. This posed a risk concerning global translation of medical terms, available treatments and licensed medicines which differ between the UK and United States of America (USA) for example. ‘So, if I struggle with anything, I’ll literally write a post and nine times out of ten, it may come from America, which you think you have to kind of decipher everything American’ (Sophie).
Discussion
Findings from previous research exploring the psychosocial impact pituitary conditions have upon those who receive a diagnosis consistently note the negative impact on mental health and wellbeing (Biermasz, 2019; Norman et al., 2021, 2022). Similarly, the data from this study echoes the comparable experiences of family members who care for loved ones with a pituitary condition, highlighting a lack of emotional support available from healthcare services. This study has identified the collective emotional burden carried by carers which continues to serve as a significant predictor of poor mental health against the level of investment made by the carer (Oliveira et al., 2018).
The lack of communication from healthcare professionals for family members acted as a driver to them to seek their own knowledge. Becoming experts of specific pituitary conditions as they navigated the often-tumultuous journey from pre- to post-diagnosis. In doing so they transformed feelings of powerlessness into ones of empowerment in the pursuit of greater understanding (Aujoulat et al., 2007). Despite this insight, family members’ views were rarely sought by professionals, notably failing to incorporate family-centred care practices into routine healthcare provision. Echoing calls to move towards a universal model of family-centred care, Kokorelias et al.'s (2019) scoping review argues strongly for prioritising the needs of family members, involving them as experts in care to ensure the best outcomes for all concerned. This holds the potential to alleviate some emotional burden placed on family members with an imperative need for greater support to improve their own mental health and wellbeing across the life span.
The narrative running through this study calls for improved education. Education for, and offered by, healthcare services must be prioritised to offer greater access to specialist information, lessoning the burden of care for family members. This is in line with Donegan et al. (2021) who advocate for improved access to reliable information for patients (including those with pituitary tumours) to relieve the mental burden associated with diagnosis and treatment. Family members consistently addressed their desire for increased knowledge and awareness of the range of pituitary conditions and symptoms. Increased accessibility to targeted, specialist support and information provided by endocrine specialists and general healthcare professionals is therefore required to reduce the feelings of overwhelm.
The lack of acknowledgement from healthcare professionals regarding measures of support to reduce the impact of care fed into the theme ‘misperceptions of care create barriers’. When asked their views concerning their self-perceived role as carers, their answers chimed with those of Goranitis et al. (2014) observing that family members found the label presented both positive and negative associations. Family members in this study did not always consider themselves to be carers, justifying the statement with consideration of their loved one's ability to live independently when their pituitary condition was well managed. These findings are supported by comparative studies within different healthcare contexts such as Smith et al. (2022) whose study of family dynamics in dementia care recognised distinct types of kinship relationships involved in care processes. Thus, professionals failing to recognise family carers (roles which are separate from kinship relationships) create a barrier to family members seeking out and accessing mental health support (Biegel et al., 1995). Being able to express such feelings during the research process provided a small step towards personal empowerment for those who were able to share their voice (World Health Organization, 2021). Whilst an appeal to empowerment in health contexts is not without criticism for offering false hope (Kapeller & Loosman, 2023), it is imperative when validating family members in their role. To break down such barriers, a paradigm shift is required across the broad spectrum of healthcare provision, including endocrinology (Kalra & Rutten, 2023).
Matters of power and context are yet to be addressed adequately within current health and care policy (Kelly-Irving et al., 2023). Family-centred care commands principles of engagement and empowerment. These core tenets strengthen the triad of patient, family and healthcare service, anchoring the core of safe and effective care provision throughout the lifespan (Ocloo et al., 2020). The connected lives of family members are entwined and therefore arguably interdependent (Hagestad & Dykstra, 2016). The impact of a pituitary condition has the power to influence the whole family.
Participants were unanimous in their reports on the quality of information and support available from the Pituitary Foundation, concurring with findings from other studies of patient experiences (Jackson et al., 2019). Family members often came across this support through a personal quest for knowledge rather than a direct referral from healthcare professionals as found by Underwood et al. (2019) in their patient experience study. As a result, family members felt let down by information made available to them. Such conclusion is not limited to this study, with Donegan et al. (2021) equally stressing the importance of education within pituitary care from the perspective of newly diagnosed patients. The consequences had a detrimental impact upon the quality of family life, including reports of family breakdown, social withdrawal and poor mental health, confirming findings from patient experience research (Forrest et al., 2017).
As Coleman (2002) has suggested, family empowerment is multi-levelled. When patients and their families lack agency to gain autonomy over their own lives, health promotion fails to reach optimum outcomes (Downie et al., 1990). Empowerment in this context encompasses the point at which a person feels able to establish control over the dynamics which shape their lives (Gibson, 1991). To realise positive mental health outcomes for family members providing pituitary care, the focus of health services must shift from the singular patient experience to the collective impact upon the family unit.
In summary empirical research has so far neglected to acknowledge the voice of family members in relation to pituitary care. Addressing this gap, key themes have been drawn from these data to illustrate the collective experience. Family members become experts by experience, they carry a burden of mental load associated with the care, diagnosis and treatment of their loved ones. Often misconceptions of care and its meaning create barriers to family members accessing support for their own mental health and well-being needs. This contributes to their perceived battle for support from professionals who are ill-informed and services which do not deliver on statutory duties of family-centred care. Encapsulating the overarching narrative of overwhelm, family members are left to pursue their own condition-specific research to gain understanding of their loved ones needs. Information is consequently sought through a variety of means, including global online sources.
Implications for Research and Practice
Importantly, healthcare services must give greater voice to family members, in line with guidance set out in the Health and Care Act (2022), recognising them as experienced partners in the delivery of patient care. In failing to do so, health care services are missing opportunities to reduce the mental load placed upon families through a lack of education and awareness of specific pituitary conditions (Wang et al., 2023). This has a detrimental effect upon the mental health of both patients and family members alluding to findings from patient experience research highlighting the negative impact living with hidden disability can have (Forrest et al., 2017; Norman et al., 2021; Peters et al., 2020). As such further research is advocated to reduce the health inequalities expressed by family members who provide care to their loved ones with pituitary conditions.
Revisiting research such as Cherla et al.'s (2014) evaluation of effective programmes of education with family members to contribute their voice and expertise as partners and evaluators would also be worthy of further exploration. This could also include more detailed consideration to the geographical availability of support for family members to evaluate consistency and equity of support, across the UK and globally.
Limitations
This study was limited by the potential bias presented by participants who were recruited as members already accessing support from the Pituitary Foundation. As noted by Norman et al. (2022), the researchers are mindful that participants within this study have proactively sought support and therefore outcomes may differ from family members who have not accessed such third sector support.
Patton (2015) is mindful of research which draws from a limited range of sources, making this study vulnerable to potential bias from participants whose experiences are subjective in relation to the specific pituitary condition of their loved one. Therefore, recommendations are made to conduct further cycles of this generalisable research to provide broader narratives of condition-specific experiences.
Conclusions
Family members play a crucial supporting role in the provision of care to those with pituitary conditions, with often detrimental consequences for their own mental health and wellbeing. They are disempowered by the lack of empirical research from which those in positions to incite change (stakeholders, policy makers, commissioners, health and care services) can draw upon to fully understand and meet their needs. Family members require support and acknowledgement from healthcare professionals to validate them in their caring role. Family members want to be valued as carers through consistent family-centred approaches from healthcare services. Failure to engage family members in communication regarding their loved one's condition and their own role as a carer creates barriers to them seeking mental health support. With things as they stand, healthcare services within the UK are failing to ensure optimum outcomes of family-centred care concerned with the diagnosis and management of those with pituitary conditions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.