
Abstract
Women's health is a vast and complex field, encompassing diverse experiences and challenges throughout the pregnancy lifecycle. Despite advanced medical facilities in the United States, pregnancy-related mortality rates remain higher than in other countries, with alarming disparities affecting minority populations. This article explores the multifaceted landscape of infertility, focusing on women in heterosexual partnerships pursuing in vitro fertilization (IVF). In exploring the biological, psychological, and social dimensions of women's health in the context of IVF, this article employs the biopsychosocial model as a systemic framework to comprehend the comprehensive nature of the IVF process. It delves into the challenges faced by individuals and couples, emphasizing the vital role of mental health services in promoting overall wellbeing.
Women's health is an expansive field that includes a diverse array of experiences, concerns, and issues. An important area within women's health is that of the pregnancy lifecycle, which encompasses the time before, during, and after a birthing experience (Blount et al., 2021). According to the National Institute of Health (NIH), although the United States (U.S.) has state-of-the-art medical facilities and healthcare professionals, the mortality caused by pregnancy-related issues is higher than other countries (NIH, 2021). This elucidates maternal health issues, as the number of deaths has more than doubled in the past 20 years, with Black women dying at three to four times the rates of White women (Fleszar et al., 2023). Similarly, other minority populations such as Latinx women are dying at two to three times the rates of their White counterparts (Fleszar et al., 2023). Factors contributing to these disparities are beginning to emerge beyond the biological medical framework. Specifically, there are several psychological and social determinants at play during the pregnancy lifecycle (Blount et al., 2021). Individuals’ socioeconomic status, social support, access to quality healthcare, and experiences with mental health challenges are examples of determinants contributing to the overall health and wellness of pregnant women (Blount et al., 2021). Further, many people who wish to become pregnant experience challenges with this process. For the purpose of this article, the population of focus is on biological women in heterosexual partnerships, who have attempted to conceive naturally. It goes without saying that many same-sex couples use assisted reproductive technology (ART), which involves either egg donation, sperm donation, or embryo donation. The same may be true for heterosexual couples experiencing infertility issues.
Fertility issues are common in both men and women. In fact, one in six adults struggle with fertility (Njagi et al., 2023; WHO, 2023). Couples who face infertility may seek medical specialists such as reproductive endocrinologists to explore various routes for conceiving a child. Such ART includes in vitro fertilization (IVF), accounting for 99% of ART procedures (CDC, 2022; Sunderam et al., 2022). Because IVF is a process that includes multiple steps over an interval of several weeks or months, one IVF procedure is referred to as a “cycle” or “round” of treatment (Sunderam et al., 2022). Among many others, major steps in a round of IVF include hormonal treatment, egg retrieval, laboratory fertilization to attempt to create an embryo, and eventual transfer to a woman's uterus (CDC, 2022). According to the Centers for Disease Control and Prevention, 12% of reproductively aged women (defined as the age range between 15 and 44) engage with infertility services (CDC, 2022). The average age at which women use IVF can vary depending on several factors, including geographical location, individual circumstances, and medical reasons. However, women over 35 are more likely to seek IVF treatment and it is becoming more common as women wait longer to have children, wait for the right partner, and focus on career advancement (Delbaere et al., 2020). In the CDC's most recent 2020 report, there were 79,942 live births via IVF (Sunderam et al., 2022), accounting for approximately 2.0% of all babies born in the U.S. (Sunderam et al., 2022).
Women undergoing IVF face unique challenges on biological, psychological, and social levels. As such, using the biopsychosocial model (Engel, 1980) to conceptualize the health and wellness of women with infertility is fitting because it offers a comprehensive understanding and provides implications for intervening in a holistic way (Dube et al., 2021). Given the high rate of infertility within the U.S. and the growing number of people seeking treatment via IVF, the purpose of this article is to explore common experiences of women with infertility from biopsychosocial perspective to provide recommendations for promoting overall health and wellness. The biopsychosocial pregnancy model (Blount et al., 2021; Engel, 1980) includes biological, psychological, and social components of women's health, as well as risks commonly experienced by individuals in their pregnancy lifecycles.
Biological
While IVF offers the chance to conceive when natural conception may not be possible, it is important to acknowledge that this fertility treatment comes with certain risks and complications. One notable concern is the increased likelihood of multiple births, which can lead to a higher risk of early labor and lower birth weight (Mayo Clinic, 2021). Additionally, approximately 2% to 5% of IVF procedures result in ectopic pregnancy, where the fertilized egg implants outside of the uterus, leading to the termination of the pregnancy (Mayo Clinic, 2021). IVF also involves the use of injectable fertility drugs to stimulate ovulation. However, this can sometimes lead to a condition known as ovarian hyperstimulation syndrome, characterized by rapid weight gain, shortness of breath, and increased pain (Mayo Clinic, 2021). Furthermore, during the egg-retrieval procedure, there is a potential for complications such as bleeding or infection affecting the bowel, bladder, or blood vessels due to the use of needles (Mayo Clinic, 2021). It is essential for couples considering IVF to be fully aware of these risks and consult with their healthcare professionals to make informed decisions about their fertility journey.
Before the technical start of an IVF cycle, there are significant physical demands placed on couples for IVF candidacy (Harrison et al., 2021; Rao et al., 2018). This involves many laboratory tests, screenings, and specialist medical appointments both prior to and during an IVF cycle. Although there is no standardized definition for an IVF ‘cycle’ or ‘round,’ completing one takes approximately 4 to 6 weeks and can be very taxing on a woman's body as she is experiencing several blood tests, invasive procedures, lack of privacy, hormone injection therapy, transvaginal ultrasounds, additional medication, and sedation (Harrison et al., 2021). Physical side effects can include bloating, cramping, bleeding, constipation, nausea, hot flashes, headaches, breast tenderness, general discomfort as well as water retention which all have potential to negatively impact body image and confidence (Kaliarnta et al., 2011; Robertson et al., 2021). Additionally, the necessity of undergoing these tests and procedures can result in a perception of invasion of privacy and is correlated with compromised sexual self-esteem and lowered enjoyment of sexual activity with partners (Kaliarnta et al., 2011; Robertson et al., 2021). The invasive nature of IVF can sometimes lead women to feel “like a science project” and “emotionally numb” (Copp et al., 2020). Understandably, reactions to these physical experiences can lead to strong emotional responses throughout the process. As such, understanding the psychological implications of IVF is necessary.
Psychological
Undergoing fertility treatment, particularly IVF, to achieve pregnancy can take a significant toll on a woman's physical and emotional wellbeing, potentially leading to a diminished quality of life during treatment and beyond. Women going through IVF may experience high levels of emotional distress, including anxiety and depression, along with strains on their relationships and financial hardships (Domar et al., 2018; Fleszar et al., 2023; Njagi et al., 2023). Approximately 40% of women facing infertility meet the criteria for a psychiatric diagnosis, with an increased risk of experiencing suicidal ideation (Chernoff et al., 2020; Dube et al., 2021). However, many women report not discussing psychological stressors associated with infertility with their medical providers, even though the burden of stress is a primary reason cited by women for discontinuing IVF treatment (Domar et al., 2018). Consequently, women express that stress reduction education and related mental health interventions could have been helpful in continuing their treatment (Domar et al., 2018; LoGiudice & Massaro, 2018). Given the impact of IVF on a woman's emotional wellbeing and overall life satisfaction, it is crucial for healthcare professionals to consider and address the psychological aspects of infertility during the treatment process, offering support and referral for appropriate interventions to those undergoing IVF.
IVF is often considered a “technology of hope” (Copp et al., 2020; Robertson et al., 2021). The flip side is that IVF can result in a complicated emotional experience that may include disappointment, frustration, grief, anxiety, and depression dependent upon the process and outcome of a cycle (Copp et al., 2020; Domar et al., 2018). Thus, from a psychological perspective, IVF can be understood as a dialectical experience where conflicting emotions such as fear and hope coexist and experiencing contradictions between a one's internal inclination (i.e., desire for a child) and their external reality (i.e., awaiting a successful cycle) along the way (Gonen & Bokek-Cohen, 2020).
The IVF experience is often characterized by a complex mix of emotions, including ambivalence, frustration, anger, disappointment, and grief. The number of attempts taken to conceive, as well as the outcome of these attempts, impacts the emotional experience in complex ways (Kaliarnta et al., 2011; Yao et al., 2022). The grief experienced during the IVF process can manifest in two distinct ways. Firstly, there is the sorrow and heartache resulting from previous unsuccessful attempts to conceive. Those undergoing treatment may grapple with feelings of disappointment and sadness, mourning the loss of each failed endeavor. Secondly, a unique form of disenfranchised grief arises when couples contemplate the reality that they may be approaching their last attempt at IVF, and yet their desired outcome remains unknown. This emotional burden emerges from the loss of a future they had envisioned, filled with hopes and dreams of parenthood, which may never materialize in the way they hoped.
This emotional process often occurs in isolation, as many people surrounding the IVF patient are entirely unaware of what is going on. Many women undergoing IVF experience shame related to requiring ART to conceive, feeling damaged, or broken that they are not able to procreate naturally (LoGiudice & Massaro, 2018). As a result, many women keep quiet about their IVF treatment until they are far enough in their pregnancy that the risk of miscarriage is low (LoGiudice & Massaro, 2018). Of course, many IVF cycles fail for a variety of reasons, and those that initially result in pregnancy may not result in a live birth (Harrison et al., 2021). In sum, IVF patients are often without the support of important others when they need it most, resulting in diminished mental health and wellness (Gonen & Bokek-Cohen, 2020; Harrison et al., 2021; LoGiudice & Massaro, 2018).
The IVF journey is a delicate and emotionally charged one. This state of being during IVF has been described as emotional choreography where one may feel the need to suppress shame, guilt, tension, anxiety, depression, or anger and replace it with the perceived “acceptable” persona or attitude of being grateful, supportive, and excited (Gonen & Bokek-Cohen, 2020; Kaliarnta et al., 2011). According to Chernoff et al. (2020) psychological risks to women's health can also include anxiety depression, trauma, and feelings of loneliness throughout the process. These risks can make the decision to engage in IVF, which is already stressful, even more challenging. Recognizing and acknowledging the emotional distress experienced by IVF patients is vital in providing appropriate support and empathy throughout the process. Understanding the multifaceted nature of these emotions can help healthcare professionals offer compassionate care to individuals facing the uncertainties of infertility treatments.
Decision Making
IVF entails significant sacrifices, encompassing time, financial resources, and personal privacy (Copp et al., 2020; Gonen & Bokek-Cohen, 2020). While driven primarily by the inability to conceive a child, the decision to pursue IVF treatment is influenced by a multitude of factors including the woman's overall health, the potential risks associated with her age, the influence of internal and societal pressures, the availability of IVF treatment, and the personal moral considerations surrounding the use of IVF (Copp et al., 2020; Harrison et al., 2021).
Moreover, the emotional complexity of this decision is compounded by the IVF patient's previous struggles with conceiving naturally, facing the disappointment of failed cycles, and potentially experiencing additional complications such as miscarriages and stillbirths (Mayo Clinic, 2021). As they contemplate IVF, patients are confronted with the reality of risk taking: there is no guarantee that treatment will result in a baby (Harrison et al., 2021).
Age
Age is a key factor to consider when looking at birth rates, as fertility decreases with age (HFEA, n.d.). The rate of miscarriage for women who conceive using IVF is approximately 15% to 25%, like that of women who conceive naturally but increases with maternal age (Delbaere et al., 2020; Mayo Clinic, 2023). This is largely dependent on whether they elect to do preimplantation genetic screening (PGS), as many cycles fail due to chromosomal abnormalities and as such, individuals that do PGS likely have much lower miscarriage rates—and lower rates of failed cycles (Delbaere et al., 2020). Women in their early 30s reported feeling hopeful about their chances of successful treatment based on their young age, while women in their late 30s early 40s reported feeling out of time and needing to complete as many cycles as they could (Copp et al., 2020). According to the Human Fertilization and Embryology Authority (2018), the average age of an IVF patient is 35.3. Birth rates per embryo transferred were 25% for patients aged 35 to 37, 19% for patients aged 38 to 39, and 11% for patients aged 40 to 42 (HFEA, n.d.).
Pressure
In addition to a woman's biological clock, IVF treatment is riddled with both societal and self-imposed pressures as consequence to living in a pronatal society (Gonen & Bokek-Cohen, 2020). Societal pressures often stem from the outward expression of value placed on women who have children; making those that struggle with infertility feel, isolated, judged, and misunderstood (Yao et al., 2022). Furthermore, well-intentioned family members and social circles frequently asking if the treatment has worked or if pregnancy has been achieved further pushes the agenda that a round pregnant belly is expected from IVF (Yao et al., 2022). Due to the financial investment, there is often a pressure to succeed (Njagi et al., 2023; Yao et al., 2022). Experiencing failure in one or more IVF cycles can trigger intense emotional responses, often leading to heightened feelings of guilt, shame, frustration, sadness, and anger (Yao et al., 2022). These negative emotions become centered around self-criticism and self-blame, fostering thoughts of self-hatred toward their own bodies for “failing” (Gonen & Bokek-Cohen, 2020; Yao et al., 2022). Additionally, individuals may begin to question their worth as a partner, feeling inadequate or not “good enough,” and may even wonder if something is inherently wrong with them, perpetuating a cycle of negative self-perception (Gonen & Bokek-Cohen, 2020; Yao et al., 2022). These experiences can contribute to an overall negative outlook, adding to the existing self-imposed pressure to conceive and reproduce successfully as a result of IVF.
The Waiting Period
A comprehensive grasp of the IVF process includes recognizing the significant extent of waiting time it entails. A full cycle of IVF takes 4 to 6 weeks, including the time before egg retrieval to when a woman is tested for pregnancy (Cleveland Clinic, 2023). Throughout those weeks, a woman undergoes regular injection of medication, is monitored in the office every few days via ultrasound, and administers a “trigger shot” exactly 36 h before the egg retrieval. On average, 70% of the retrieved eggs will be successfully fertilized (Cleveland Clinic, 2023). If 10 eggs are retrieved, for example, about seven of those eggs will fertilize. The following 5 to 6 days includes embryo development and only 30% to 50% of those embryos progress to the point where they are suitable for transfer to the uterus, otherwise known as the blastocyst phase (Cleveland Clinic, 2023). For example, if seven eggs were fertilized, two to four of them might develop to the blastocyst phase. The embryo transfer can take anywhere from 3 to 7 days after retrieval if they’re fresh (Cleveland Clinic, 2023). If the embryos are frozen, 14 to 21 days of hormone medication followed by 6 days of injections with two to three specialist appointments are needed (Cleveland Clinic, 2023). Providers can perform blood tests about 9 to 14 days after embryo transfer to determine if a woman is pregnant (Cleveland Clinic, 2023). This perspective is included to highlight how much waiting time is involved in the IVF process. During this waiting period, there is nothing a woman can do to increase her chances of a successful treatment. This can induce anxiety, fear, and worry (Kaliarnta et al., 2011).
IVF patients who must attempt multiple cycles experience chronic periods of waiting as they repeat this process to increase their chances of success. Despite age and specialist recommendations, the outcome of previous cycles is also a factor in a couple's decision. If a couple achieved a biochemical pregnancy or collected several fertilized eggs resulting in embryos, they tend to experience hope in continuing with treatment, noting that if those minor successes hadn’t happened, they would have considered stopping treatment sooner (Copp et al., 2020). Success stories of defying the odds, or availability bias (Domar et al., 2018), also serve as a source of hope for some patients when considering continuing IVF treatment, therefore, it's important for medical specialists to provide accurate information to patients about realistic outcomes (Copp et al., 2020).
Social
Couples
The percentage of women undergoing IVF who are in a relationship or partnered can vary widely based on geographical location, cultural factors, and individual circumstances. IVF is often used by couples experiencing infertility, but it's also used by single individuals, same-sex couples, and others who may not fit the traditional definition of a heterosexual couple. While women absorb most of the emotional burden, men also reported feeling anxious and depressed (Gonen & Bokek-Cohen, 2020). In a qualitative study, Gonen and Bokek-Cohen (2020) described the experiences couples had while sharing the anxiety-inducing process of IVF. Some stated it created emotional distance within their relationship, while others reported growing closer to their partner through the challenges of IVF (Gonen & Bokek-Cohen, 2020). Other researchers (Kaliarnta et al., 2011; Yao et al., 2022) have recognized the connection between unsuccessful IVF attempts and marital resilience, quality, and symptoms of depression. They ultimately found that marital resilience is nice to have, but it's not essential to recovery after an unsuccessful IVF attempt. Feeling supported, safe, and being in mutual agreement with their partner that while depression may very well be present after an unsuccessful attempt, it is temporary and is a vital part to healing (Yao et al., 2022). The existing literature exploring the influence of IVF on a couple's relationship reveals a varied outcome, with some experiencing a strengthening of their bond while others endure strains (Gonen & Bokek-Cohen, 2020). This underscores the significance of IVF as a major factor within a partnership, making it imperative for medical and mental health professionals to carefully consider the psychological and social implications when assessing for risk in these patients.
Access
There are many barriers to accessing IVF, with the financial investment being one of the major factors (Gonan & Bokek-Cohen, 2020; Njagi et al., 2023; Yao et al., 2022). IVF continues to be a complex problem with insurance and can cost anywhere from $10,000 to $30,000 per cycle/round in the United States due to being an out-of-pocket expense (Njagi et al., 2023). The decision to pursue IVF treatment is one that women and couples do not make lightly as it can quickly deplete financial resources (Harrison et al., 2021; Kaliarnta et al., 2011). There are links to poverty and maternal wellbeing when looking at stressors such as increased risk of malnutrition, drugs or alcohol use, and psychological strain (Domar et al., 2018; Fleszar et al., 2023). Women of color are especially at risk of experiencing disparities when navigating the current healthcare system in the U.S. and these racial disparities do not stop when pursuing IVF treatment (Fleszar et al., 2023).
In addition to racial disparities, there is evidence of prejudiced attitudes toward nontraditional families pursuing IVF (Fleszar et al., 2023; Shaw et al., 2022). As societal perceptions of growing families become more inclusive, it is crucial for research and quality of care to adapt accordingly. Unfortunately, there is a lack of research on nontraditional families, such as single women and individuals/couples within the LGBTQIA + community, who are seeking IVF treatment (Shaw et al., 2022). Moreover, the financial investment for LGBTQIA + people and couples is significantly higher due to the need for egg donors, sperm donors, surrogates, or gestational carriers (Shaw et al., 2022). These challenges are further compounded by ongoing attacks on LGBTQIA + people's rights and reproductive freedom (Shaw et al., 2022). As we move forward, it is essential to address these issues to ensure equitable access to fertility treatments for all individuals and couples.
Ethics
Although it is outside the scope of this article to take an in-depth exploration of the ethical dilemmas women and couples often face when considering IVF, it is important to acknowledge how it can create interpersonal and intrapersonal conflict leading to further emotional labor within the decision-making process. Some ethical concerns include: involving discussions on embryo disposal, selective reduction, multiple pregnancies, and the commodification of human eggs. This section of the literature review delves into the ethical dilemmas and societal debates surrounding IVF, emphasizing the importance of informed consent and responsible reproductive medicine practices. The tension or guilt between desiring a family but wrestling with IVF as a process that “goes against nature” is a major hurdle for some people (Kaliarnta et al., 2011). This decision can have religious undertones as well. Considering belief systems around prolife versus prochoice, the implications of Roe v. Wade, decisions about what to do with spare embryos, the harm threshold, and general views and misconceptions toward ART innovations and their impact on women's psychophysical health often leave women and their partners in an ethical dilemma (Harrison et al., 2021; Kaliarnta et al., 2011) This may be especially apparent in the U.S., where significant political polarity exists relative to government oversight on women's rights, choice restrictions, and national discord about morality related to certain aspects of pregnancy.
Furthermore, providers have the right to refuse treatment if they believe it will interfere with the wellbeing of their patients or offspring (Siegel & Ravitsky, 2018; Sigillo et al., 2012) and in some states, if they disagree with the choices the couple are making. With this comes the potential for discrimination (Sigillo et al., 2012). From a mental health standpoint, discriminatory practices can be further amplified. The American Society for Reproductive Medicine (2018) permits the denial of IVF treatment based on mental illness. However, Siegel and Ravitsky (2018) contend that this approach lacks thorough risk analysis and fails to strike a balance between competing interests and individual rights. Such policies raise concerns about the equitable access to IVF treatment for individuals with mental health conditions and reiterate the need for a more comprehensive and thoughtful approach in assessing eligibility.
Counseling Services
Engaging in IVF is a complex process that has several implications on biological, psychological, and social levels. To address the numerous variables involved, an integrative and interdisciplinary approach to care is essential for individuals pursuing this path. This article highlights the often overlooked psychological and social factors, underscoring the significance of mental health services in the journey of couples undergoing IVF.
A 2018 review by Patel and colleagues revealed that most couples going through IVF expressed a need for psychological support. However, <25% receive mental health services, and a mere 5% seek out support groups, even when offered free of charge (Patel et al., 2018). Data suggests that couples attending counseling sessions’ average only one to three sessions (Domar et al., 2015; Patel et al., 2018). Several factors contribute to this underutilization, including lack of education and understanding about counseling services, concerns about cost, time commitment, occupational expectations, and the stigma associated with seeking help (Domar et al., 2015; Patel et al., 2018).
Understanding the professional context within which infertility treatment takes place is important. Addressing mental health concerns is not generally considered a standard aspect of care at most reproductive specialist clinics (Patel et al., 2018). However, given the emergence of integrated care clinics, implications for healthcare professionals involved on infertility teams persist. Provider education is paramount: IVF is not an exclusively medical process. Including the psychological implications of infertility and treatment into medical, residency, and specialist training programs is of critical importance to holistic patient care. Clearly and transparently communicating the need for, benefits of, and availability of counseling services while normalizing mental health counseling can increase the rates at which couples access mental health support (Domar et al., 2015; Dube et al., 2021; Patel et al., 2018).
Furthermore, it is crucial for mental health providers to recognize that women in their pregnancy lifecycle, especially those undergoing IVF, constitute a unique population (Domar et al., 2015; WHO, 2023). Enhancing the quality of care involves understanding the experiences, risks, and needs of women during this period and fostering an integrative approach to working with other healthcare professionals, ideally incorporating mental health professionals (Copp et al., 2020; Yao et al., 2022).
Recently, the online community for IVF has burgeoned. Online communities for IVF provide a valuable platform for individuals and couples going through fertility treatments to connect, share experiences, and seek support in a group setting. These communities can be a source of emotional support, information, and camaraderie during what can be a challenging physical and emotional journey. Furthermore, online chats offer anonymity, ease of communication and flexibility of chat times, and free access for obtaining resources and a wealth of personal experiences with IVF.
Discussion
This article illuminates the intricate and expansive impacts of IVF on individuals’ and couples’ wellbeing, encompassing biological, psychological, and social domains. As the field of assisted reproductive technologies advances, it becomes increasingly evident that while IVF holds immense potential, there is a pressing need for ongoing research aimed at improving success rates, enhancing safety measures, reducing stigma associated with IVF, and addressing the psychological and emotional implications that come with it. Additionally, comprehensive counseling strategies should be developed, not only to aid individuals and couples in navigating the emotional impact of IVF but also to address the familial dynamics influenced by the process. Within this context, ethical considerations also play a pivotal role, as decisions connected to IVF raise questions about genetic selection, commercial surrogacy, and long-term health outcomes related to children conceived through IVF. Moreover, access to IVF care remains a significant concern, with disparities in availability and affordability limiting many individuals from pursuing these treatments.
Considering how multifaceted this process is, we emphasize that the services provided to individuals pursuing IVF be grounded in an integrative and interdisciplinary approach, considering the medical and psychosocial aspects of fertility treatment. Notably, a gap that has emerged from current research is the often-overlooked role of mental health services in supporting couples undergoing IVF. Being equipped to address the psychosocial challenges of IVF can significantly contribute to better outcomes for individuals, couples, and families, ultimately fostering a more effective, patient-centered approach.
Importance of Mental Health Services
Mental health services play a vital role in the context of in IVF as they provide emotional support and address the psychological wellbeing of individuals and couples undergoing fertility treatments. Mental health services and counseling can help address the emotional impact of IVF, provide support for grief and loss (especially when treatments are unsuccessful), provide support for relationship issues that arise, provide support for unpartnered patients, and provide support for pregnancy and beyond. Incorporating mental health services into the IVF journey is essential for addressing the holistic wellbeing of patients (Domar et al., 2015; Domar et al., 2018; Dube et al., 2021; Patel et al., 2018). These services can help individuals and couples cope with the emotional challenges, make informed decisions, and improve their overall quality of life during and after fertility treatments (Patel et al., 2018).
Addressing the pressing need to alleviate distress associated with infertility and its treatment, prioritizing psychological interventions focused on stress management and coping skills training is imperative. Such interventions effectively address the significant personal, familial, and societal impact of infertility and its treatment, empowering couples to endure the challenges they face (Dube et al., 2021; Patel et al., 2018). It is important to recognize that the psychological burden is not confined to women alone; their partners, often neglected in research, may also require attention and support throughout the IVF process (Gonen & Bokek-Cohen, 2020).
Mental Health Practitioners
To improve the quality of care and support available to individuals undergoing IVF, we recommend focusing on education as part of training for counseling, psychology, social work, and behavioral health students at the master's level and doctoral levels. This education should encompass not only knowledge about women's health, such as infertility, pregnancy loss, and reproductive trauma, but also provide students with exposure to the intricacies of pregnancy-related issues through field experience opportunities in integrative care settings, for example. By integrating this type of training for students who have an interest in working with this population, they are provided with the chance to develop clinical skills relevant to these specific challenges. The relevant field experience component, facilitated through practicum and internship semesters, plays a vital role in bridging the gap between academic knowledge and real-world application. Understanding the multifaceted aspects of IVF, encompassing medical, emotional, psychological, and ethical dimensions is crucial for effectively supporting the emotional wellbeing of IVF patients.
Furthermore, cultivating collaboration within interdisciplinary healthcare teams aligns with the direction of modern healthcare practices. As these providers-in-training gain more clinical experience as it relates to IVF, they learn how to work within a biopsychosocial model contributing to teams that include medical professionals, reproductive specialists, and other caregivers to comprehensively address the diverse needs of IVF patients. This collaborative approach reinforces that the emotional and psychological aspects of fertility treatments are given the same priority as the medical ones, resulting in more holistic and patient-centered care.
Future Research
The field of IVF and counseling is continually evolving as science and technology advance, and as society's understanding and expectations surrounding reproductive health and family planning change. Additionally, investigations that explore diverse populations in the context of IVF are warranted to ensure equitable and inclusive care (Figure 1 includes potential research and counseling areas). This research in IVF and counseling should aim to improve the effectiveness, safety, and accessibility of IVF treatments while also addressing the emotional and psychological needs of individuals and couples undergoing fertility treatments. Collaboration between medical professionals, psychologists, social scientists, and policymakers will be essential in driving these advancements forward.
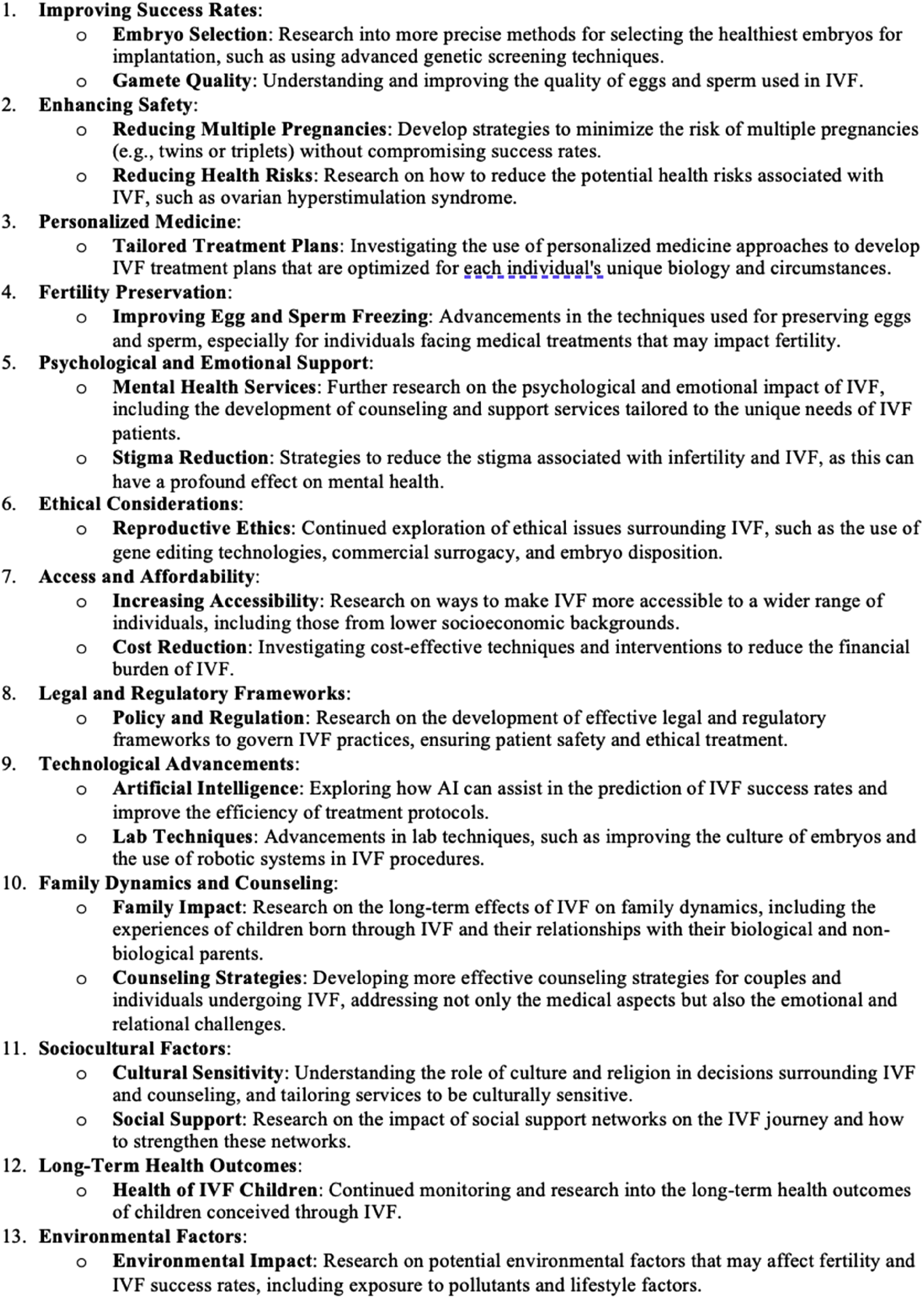
Future IVF research possibilities.
In conclusion, the utilization of the biopsychosocial framework in the context of IVF represents a holistic and comprehensive approach to understanding and addressing the complex factors involved in fertility treatment. This framework considers not only the biological aspects of infertility and IVF but also the psychological, social, and cultural dimensions that influence the experiences of individuals and couples on their fertility journey. By adopting the biopsychosocial framework, healthcare providers, counselors, and researchers can better appreciate the interplay between these various factors and tailor their interventions and support accordingly. Regarding the psychological and social factors in the context of IVF, there is a necessity for comprehensive, integrative, and interdisciplinary care. By recognizing and supporting the psychological wellbeing of individuals and couples pursuing IVF, healthcare professionals can play a vital role in reducing distress, enhancing treatment experiences, and ultimately helping couples achieve their life goals of building their families—whether through IVF or an alternate route. As we continue to advance our knowledge in this area, it is essential to prioritize mental health services and provide tailored support for diverse populations to inform best practices of care and improve outcomes for individuals and couples undergoing IVF.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.