
Abstract
Mitigating and understanding family violence is the cornerstone of this paper. Family violence can happen for multiple reasons without any exclusivity. A firsthand account of how I experienced violence in my life will be discussed to give meaning to my worldview and therapeutic lens. Exploration of family violence theories ranging from the ecological model to feminist theory will be conducted. Comprehending sexual minority violence must become a priority to move the conversation forward and emphasize inclusivity. Family violence ethical components are considered. Conclusively, understanding family violence fully prepares a therapist to deal with various presenting problems daily.
Introduction
Family violence is a modern term with primitive civilization history (Bakan, 1971). Since the establishment of statehood, family violence has been prevalent but has recently come to be viewed as a social problem (Gelles, 1985). In modern terms, family violence is considered to be a public health crisis and human rights issue (Southern & Sullivan, 2021). Prior to delving further into theory greater understanding of violence is critical. When defining violence, there is broad and specified terminology. In general, violence is described as when someone intends to cause physical harm (Barnett et al., 2011). However, varying forms of abuse are omitted from this definition. Levesque (2001) goes a step further and defines violence amongst family members as the healthy development of an individual being stifled by physical abuse, sexual abuse, emotional abuse, neglect, and additional forms of maltreatment. Reflections on personal and societal perceptions of family violence with be reviewed. My worldview of domestic violence will be shared to highlight how a therapist can be personally impacted and how one's worldly lens can be shaped. Major family violence theories will be deciphered along with an examination of their applicability to marriage and family therapy (MFT) practice. There will be a discussion on family violence assessment tools, and a screening procedure will be provided. Both types and targets of family violence will be highlighted. Systemically, family resilience will be defined, and details about childhood resilience within the context of family will be shared. Cultural and diversity factors considerations will be explored, inclusive of the impact on family violence. The COVID-19 pandemic exposed the vulnerability of violence in families both locally and internationally (Usher et al., 2020), which warrants greater exploration.
Personal and Societal Perceptions of Family Violence
There are perceptions that I carry regarding family violence based on life experience and personal observations. Personally, I have no tolerance for violence within the home under any circumstance. I have experienced family violence indirectly within my extended family and for myself as an individual. Growing up, I heard stories about how my aunt shot her husband in the foot after he beat her. My aunt stayed with her husband until she died and never spoke about the incident to family members. To my knowledge, her children seemed to emerge resilient as a result of the violence and have not experienced their own family violence. Resulting from my aunt's story, I had a perception when I was younger that if family violence was occurring, it should never be discussed. Then, when I was 14, a love interest slapped me across the face for what he called “talking back” to him when he told me to be quiet. Stemming from my younger years, I never told anyone and suffered in silence. An additional part of my perception was that victims must deal with the problem on their own and, if necessary, retaliate with more violence. As I grew older, my perception changed into resentment and disdain toward women who stay in abusive relationships. I have always perceived the journey for a woman or man to leave their abusive partner is not difficult because continuing to be beaten is much worse. Beyond intimate partner violence (IPV), I have directly experienced child abuse at the hands of my mother, which she considered to be discipline. Corporal punishment or spanking that I experienced with a wooden paddle/belt caused me trauma and a rift in the relationship with my mother for many years. My perception of corporal punishment is that it is child abuse and intolerable in all cases. Throughout my career as a therapist I must assess, evaluate, and evolve my perceptions about family violence in order to be effective.
Societal perceptions can stem from community ideals and the media. Standpoints on family violence may differ based on geographic location. For example, the United States views family violence as tolerable based on the influence violence has on family members (Damant et al., 2008). In response to dominant societal views the government has a hesitancy to get involved with family violence. With violence exposure being readily available in movies, television, and video games those who partake express increased aggressive behavior, particularly in children and adolescents (Huesmann et al., 2003). Resulting from violence exposure is a societal response of tolerance and acceptance. In terms of sexuality, objectification of women as sex objects or victims can lead to a societal response of devaluation and abuse (Stankiewicz & Rosselli, 2008).
Theories of Family Violence
There are distinctive theories of family violence that will be shared. The primary theories to be discussed are the ecological model, social cognitive theory, feminist theory, psychodynamic/attachment theory, family systems theory, and social learning theory. Premises of each theory will be detailed below.
Ecological Model
Bronfenbrenner (1979) associates family violence with human development and behavior that affects social factors explained through individual/environmental contexts such ranging from microsystems to mesosystems, exosystems, and macrosystems. These systems and factors expound on family violence occurring through a feedback loop and exemplifying circular causality. Dealing with the microsystem relationships/interactions of family members such as communication skills, expectations, and satisfaction affects the potential for family violence. Social components that may influence an individual's occupation, religion, media, and friendships represent the exosystem. While a macrosystem refers to cultural values about attitudes/beliefs that affect ontogenetic development, the microsystem, and the exosystem in totality. As a primary example, Yllo (2005) mentions how society accepts men's use of violence against women. Event/relationship in one situation affects events/relationships in another situation (Lawson, 2013). An individual development element of the theory known as ontogenetic factors in biological, genetic, and nonbiological components into family violence. The theory assumes unlearning and relearning appropriate interpersonal behaviors excluding violent acts is possible (Lawson, 2013). Presently, there is an ecological model of trauma be utilized consisting of three factors: coping capacities, traumatic experiences and outward outcomes, and degree of community support all in consideration of the environment (Dekel et al., 2019).
Social Cognitive Theory
Social cognitive theory could be considered a subdivision of microsystems within the ecological model. Social modeling is an important part of the theory, which impacts a person's motivation, thought, and action (Luszczynska & Schwarzer, 2015). Expanding further, individuals learn new behaviors and can generate demeanors beyond what is seen or heard (Luszczynska & Schwarzer, 2015). Eventually learned skills lead to expectations for behavioral outcomes (Luszczynska & Schwarzer, 2015). Relationally, violence is incorrectly representative of conflict management, power, and control. From a social cognitive theory viewpoint, IPV can be generational, resulting in children learning/witnessing violence in the process (McCloskey & Lichter, 2003). Research findings align with the theory by further revealing that children exposed to IPV, and physical/sexual abuse increases their chances of aggression in adulthood (McCloskey & Lichter, 2003). In relationship to gender/perpetrators, violence viewed through the theory is linked to 60% to 70% of abusive males having been abused in their childhood (Delsol & Margolin, 2004). Modern times associate social cognitive theory with the media. For instance, Forsyth and Ward (2022) found Honduran men who listened to the radio at least twice a week hand greater approval of IPV.
Feminist Theory
Feminist theory is affiliated with the macrosystem pertaining to sociocultural influences about male on female IPV and abuse to children/elders (Lawson, 2013). Also, the feminist theory holds the perception that society views men as possessing more social, economic, and power standing culturally (Lawson, 2013). Delving further into the feminist theorist perspective, family violence is considered to be caused by a male's sense of entitlement and gender inequality (Barnett et al., 2011). Normalization of family violence as a part of male behavior is depicted through the feminist viewpoint without any indication of an unhealthy mental state or unmanageable relational interactions. The criminal justice system is viewed as the leading solution to family violence from a feminist theorist mindset. Gover et al. (2021) note domestic violence courts have played a significant role in ameliorating family violence. For feminist theory, greater research should be conducted on how criminal justice reform effects families impacted by family violence crimes.
Psychodynamic/Attachment Theory
The entirety of psychodynamic and attachment theory is rooted in the understanding that family violence is impacted by parent and child relationship quality (Dutton, 2007). Attachment theory emphasizes the importance of children to have security, protection, and intimacy from attachment figures. If those needs are not met, children can develop maladaptive internal working models of relationships (Lawson, 2013). Lawson (2013) emphasizes that without secure attachment, anger, anxiety, grief, and fear develop, which leads to dysfunctional regulation practices in close relationships. The learned emotional regulation becomes ingrained in adulthood and ultimately influences relationships (Bretherton & Munholland, 2008). Evidential findings supporting attachment theory exclaim that children with insecure attachment are aggressive towards peers and predictive of later aggression (George & Main, 1979, Lyons-Ruth et al., 1993). To emphasize dysfunctional attachment, intimate partners who have experienced attachment injuries often times use violence to relieve their anger and rebalance closeness in the relationship (Katafiasz, 2020). On the other hand, nonviolent men have been found to have higher rates of secure attachment (Dutton et al., 1994). The following lethal combination has been associated with abusive personalities in males: being shamed by the father, insecure attachment with the mother, and witnessing interparental violence (Dutton, 2007). Yakeley (2018) describe psychodynamic as a relational concept composed of interpersonal, intersubjective, and embodied experiences involving socially/internalized worldly components. Through a psychodynamic framework violence is conceptualized as an immature/defensive act during childhood and pathological in adulthood (Yakeley, 2018). An individual's experiences, perceptions, and events shape their view of violence according to psychodynamic theory.
Family Systems Theory
Family violence is depicted as multifaceted when assessed from a family systems theory lens. A family systems perspective seeks to study both perpetrator and victim or the whole rather than its parts. In its entirety family systems consist of relationships, patterns, and parts which can give a rationale for why violence arises in the system. Family systems theorists and clinicians assess parts, structures, and processes of a given system. Varied familial relationships affect family violence (Murray, 2006). Unique dynamics pertaining to the family such as proximity and emotional investment can intensify or disrupt family violence (Marcus & Swett, 2003). Shared relatedness between individuals, families, and society conceptually encompasses family violence (Lawson, 2013). Family of origin and intergenerational transmission of violence both play factors in family systems theory understanding of violence, which serves as an opportunity for researchers to examine how the theory applies to this issue (2006). Al-Modallal et al. (2022) found in their study on risk factors associated with spousal violence in adulthood was women also experienced domestic violence in childhood. Family violence is interwoven into the causality and feedback loops recognized by family systems theorists. Through the family systems lens, victims and perpetrators can counteract on each other as a result of behavior changes in one affecting behavior changes in the other. Implications for clinical practice utilizing the family systems concept of equifinality can shed light on how different types of family violence can affect the system similarly in therapy.
Social Learning Theory
Social learning theory is the belief that family violence consists of aggression that is learned within the familial system. Abbassi and Aslinia (2010) note that dysfunctional behaviors are generational within a family system. Also, cultural heritage plays a factor in how families grow and interact with violence generationally. Family violence is a learned phenomenon according to social learning theorists. The discovery and witnessing of violence go hand in hand with direct enactment, which leads to modeling the violent behaviors. Through this theory, violence is perceived to be a cycle that continues because many offenders were once victims themselves (Simons et al., 1995). A statistic that aligns with the theory is that those who experience sexual trauma are predicted to engage in risky behavior (Batten et al., 2001). A modernized suggestion about social learning theory is socio-environment influences deviance and the adoption of deviant traits and behaviors in people (Aldridge, 2023). Conclusively, family violence, trauma, and imitation are all connected contributors to a cycle. The social learning theory should seek greater exploration clinically toward how family members, especially minorities learn about violence from each other.
Theories of Family Violence and MFT Practice
The ecological model influences MFT practice by impacting how the clinician will approach a family dealing with family violence. For example, rather than one singular event or family member being the cause of violence various elements can represent the problem through an ecological lens. Shifting to social cognitive theory, during the treatment phase for perpetrators utilizing cognitive behavioral therapy (CBT), a focus can be placed on teaching families cognitive behavioral skills. This is because the theory concludes family violence is caused by a lack of behavioral skills limiting appropriate expression and distorted cognitions of oneself (Lawson, 2013). In addition, from the ecological model stance, motivational interviewing and narrative therapy can then be practiced. Here motivational interviewing is defined as a collaborative process to help a client strengthen their commitment/motivation toward change. In addition, narrative therapy is described as a process of separating a person from the problem. These approaches would be used to assess and treat abusers for the following: motivation to change, commitment to nonviolence, and dominant discourses/attitudes toward women/violence. Although, legal ramifications are beheld as a key resolution to family violence in the eyes of a feminist there are clinical-based treatments with the same ideological framework that can be used in practice. Examples of interventions are psychoeducation, resocialization training, and guiding attitude change (away from privilege, power, dominance, and intimidation) (Lawson, 2013).
An additional way theories of violence would affect my MFT practice is in my work with couples. West and George (1999) denoted that IPV is connected to childhood trauma/abuse, abandonment anxiety, and unresolved attachment relationships that one partner may have. Gibby and Whiting (2023) noted anxious attachment is positively associated with IPV for both victim and perpetrator. I would unpack the attachment history of each partner and discuss any childhood trauma that could be impacting the relationship currently. Continuing from a systemic framework, Lawson (2013) points out that family systems theory allows the clinician to hold the abuser accountable while asserting no blame towards the survivor based on systems concepts such as feedback mechanisms/homeostasis. Recognition of setting conditions and triggering factors that contribute/lead to couple conflict, such as one partner being demanding, I, as the therapist, can help families combat these issues without exclusion. Distinctively, therapists working from a social learning theory perspective may want to discuss support systems and help clients strengthen their protective factors. An example of why engaging in support system work is important is based on Bjorkqvist (1997), highlighting that adolescents may view their parents as role models and imitate behaviors inclusive of violence. Utilizing CBT methodologies, practitioners can provide psychoeducation about healthy adaptive behaviors to children of abuse.
Family Violence Assessments and Procedures
Assessments for family violence can be conducted for individuals, children, couples, and an entire family unit. There can be assessments conducted pertaining to specific types of family violence, such as IPV and child maltreatment. One staggering statistic to consider when assessing for IPV is that couples who come in for therapy experience violence at a rate higher than 20% (Froerer et al., 2012). Procedurally, red flags that should be assessed prior to beginning couples counseling are either asking each partner in a questionnaire or verbally the following: communication, fighting/arguing, the partner is controlling, demands for sex, and physical violence. During couples counseling assessment, special consideration should be given for partners that may be intimidated or endanger of retaliation if the questions are answered and may need to be asked individually. Similarly, when assessing child maltreatment, specific questions should be asked pertaining to history and trauma. Following the probing, the therapist would conduct individual interviews for the parent and child.
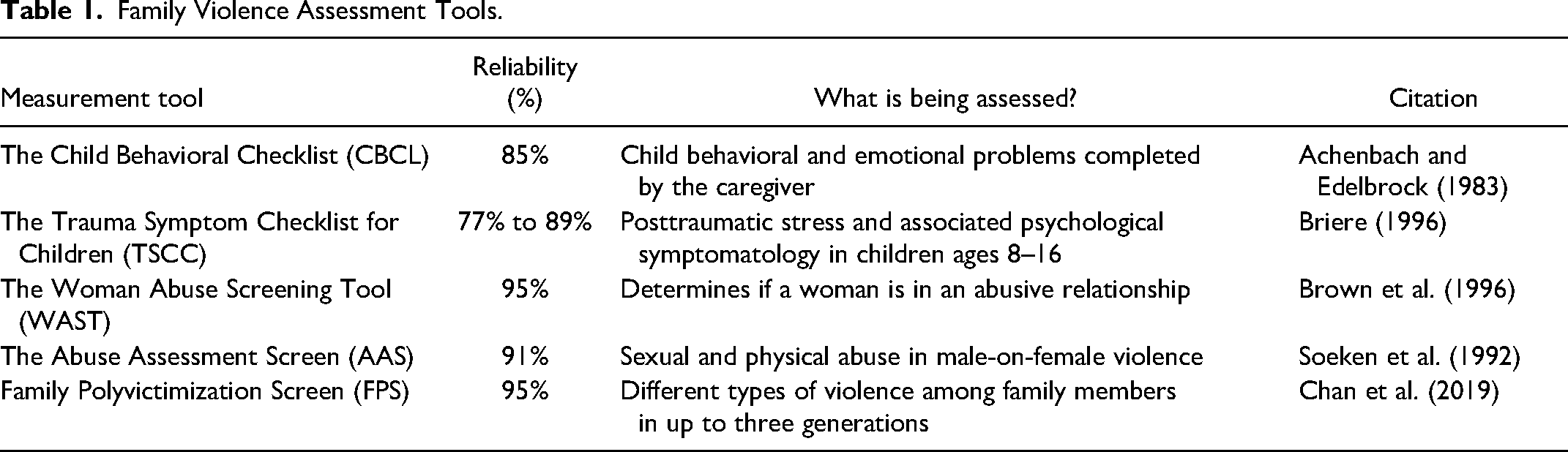
Multiple tools can be used when assessing family violence. When dealing with child maltreatment, Lawson (2013) recommends that clinicians can use the Child Behavioral Checklist and the Trauma Symptom Checklist for Children. For other types of family violence assessments, practitioners can use the following: the Woman Abuse Screening Tool, Family Polyvictimization Screen, and the Abuse Assessment Screen (AAS). Table 1 shows each assessment tool, their reliability, what is being assessed, and a citation for reference (see Appendix 1). Additionally, researchers found moderate predictive accuracy of risk assessment tool such as the Partner Violence Screen and Domestic Violence Screening Inventory (Van Der Put et al., 2019).
Family Violence Assessment Tools.
Considering that therapists are mandated reporters in most states, there should be mandatorily screening for IPV, elder abuse, and child abuse. Generally, a risk assessment should be conducted for each individual, family member, or couple. A risk assessment consists of questions about imminent danger, drug use, suicidal/homicidal thoughts, children, and substance abuse. These additional questions are more intimate, including an inquiry about mental health, and checking for children who may be in danger. Along with the risk assessment should be a systemic component that seeks answers from family members or friends who may be present in the clinical setting. For instance, questions can range from witnessing violence to serving as support/providing a safe place to stay for the victim.
Utilizing all the different aspects mentioned on what should be included in a family violence assessment leads to a specific process on how to assess for violence. Each clinician should first be aware of the clinical environment the assessment will be conducted in, such as an emergency room, clinic, or office. Answering the setting question first presents the therapist with the opportunity of knowing how much time may be available to ask questions. If a setting is fast paced, fewer questions may need to be asked. To begin, the clinician should assess for imminent danger for the client and, if involved, their children. A question that can be asked is the following: Do you believe you or your children's lives are in immediate danger due to someone that can cause harm or kill? Based on the response, the practitioner can move into how, when, and where the violence occurred? The therapist should follow up with an inquiry about the type, frequency, and severity of violence. Then the therapist should assess the client's mental health status and potential risk factors. Risk factors are inclusive of but not limited to substance abuse, living arrangements, gun access, and threats from current/former partners. From there, assessments should be administered such as those previously mentioned. Upon identifying the patient, the therapist should ask questions about support and other details of violence from family members. Questions should be asked about family members’ wellbeing and their willingness to provide the patient shelter. Lastly, all therapists should assess the client's want and willingness to go to domestic violence shelters or family crisis centers.
Recovery Model and Family Violence Treatment
Understanding the depths of applying the Recovery Model to treatment first requires the examination of fundamental principles. To begin, the basis recovery is described as the recognition and symbolization of individual's/families’ ability to rebound successfully from psychiatric illness/violence and progress to the point of living productive lives (Onken et al., 2007). Applicability of the Recovery Model to treatment is contingent upon two factors: recovery is a nonlinear process and person-centered elements are key. These elements are hope, self-determination, agency, meaning/purpose, and awareness. Once the premises are understood, there can be a shift to comprehending the language of recovery. Gehart (2012) notes that a person should be referred to as being in recovery rather than being recovered from something in treatment. In addition, in the end, when considering recovery in treatment, the prognosis should be having the ability to lead a normal life rather than the absence of pathology (Gehart, 2012).
Additionally, there are three important recovery components, which are power, wellness, and thriving. Delving further, personhood, coping skills, and sustainable wellbeing all encompass the recovery process in treatment. There are pertinent recovery model strategies that can be employed within treatment. The strategies are re-authoring, coping, and Exchanged Center Recovery. Those seeking recovery incorporate healing of the mind, body, and spirit into their treatment. Embedded in the recovery model process is an aim to address transgenerational family violence trauma for familial benefit (McCormack et al., 2021).
Types and Targets of Family Violence and Their Resilience
Varying types and targets of family violence exist, which must be identified. The different types of violence are maltreatment, abuse, and neglect. Abuse can be broken down further into physical, sexual, verbal, emotional, and sibling. Consequences of abuse are posttraumatic stress disorder (PTSD), social/interpersonal problems, and damage to a child's brain (Lawson, 2013). Distinctively, elderly abuse may result in increased risk for injuries, learned helplessness, PTSD, and increased fatality (Lawson, 2013). Neglect can be described as a failure to provide for basic needs ranging from medical to emotional. The following are consequences of neglect: criminal behavior, overeating, smoking, obesity, and cancer (Lawson, 2013). A glaring statistic to be aware of regarding maltreatment is that it's the leading cause of death for children under four (U.S Department of Health & Human Services, 2010). Each type of family violence has a devastating impact and consequential outcomes for victims.
Targets of violence are children, adults, and the elderly. Special target populations that should be considered are immigrants, racial minorities, same sex couples, and military personnel. There are distinct characteristics of each target that experiences family violence, which should be highlighted. Children exhibit aggression, self-blame, isolation, withdrawal, antisocial behavior, and avoidance. In comparison, adults possess the following characteristics: isolation, mistrust, low self-esteem, and defensiveness. Those who are elderly display features such as depression, startled response, social isolation, denial, guilt, and shame. For same-sex targets, specifically dealing with IPV may result in dependency and loneliness consequences.
Black and Lobo (2008) define family resilience as family members being able to successfully cope with adversity and embodying the characteristics of cohesion, support, and warmth. Resilient families possess factors such as positive outlook, spirituality, accord, and support. Further, resilient families can be characterized as strengthening in the face of stressors and resulting in greater unity and commitment (Black & Lobo, 2008). Throughout the family life cycle, resilience can be developed, enhanced, and refined (Masten, 2001). Research has found that children are resilient against family violence. Before discussing research findings regarding child resilience against family violence, distinct protective factors that aid resiliency should be mentioned. Ryan (2002) identified the following protective factors in reducing family violence against children: parent resilience, social support, secure attachment, and healthy relationships. Pertaining to the research, despite being raised in tumultuous environments, children have been found to thrive and be loving (Luthar & Cicchetti, 2000). Now, resilient children are described as having easy temperaments, consisting of regularity, approachability, high adaptability, positive mood, and low reactivity (Thomas & Chess, 1985). Masten (2001) declared that normal development consists of positively adapting in the face of adversity. For example, Brosi et al. (2020), revealed from their study women who experienced IPV sustained posttraumatic growth related to the following four themes: deliberateness of action (taking action), ending the cycle for the children, a changed perspective on life, and alternative perceptions of social support.
Culture/Diversity and Family Violence
Varying culture and diversity factors play a role in family violence. The diversity/cultural components are inclusive of sexual minorities, military families, gender, religion, Native Americans, and West Africans. Discussion of culture/diversity sheds light on the evolution of family violence within society. Beginning with Native Americans and West Africans, Malley-Morrison and Hines (2007) notes that before slavery/colonialization women and children were highly regarded. However, now among these cultures, violence has a high prevalence rate, and a contributing factor is oppression by many (Lawson, 2013). From a religious base, throughout history, Christianity has viewed men as having role of the putting women in submission, which remains ingrained (Dutton, 1995). As for gender, Lawson (2013) notes that various cultures consider women to be keepers of honor, which means that they are supposed to be modest and passive, never bringing shame to the family.
There are significant findings among sexual minorities and family violence. Bosco et al. (2022) emphasized IPV can occur among all couple types regardless of sexual orientation. Specifically, IPV has been found to be highest among lesbian, gay, and bisexual individuals rather than among those who are heterosexual (Edwards et al., 2015). There is a cooccurrence of different types of IPV among sexual minority individuals. Women who are sexual minorities were found to have the highest probability of being sexual IPV victims. Delving further, bisexual individuals are more likely to be victims of family violence than any other sexual minority group. Another statistic to note is that one in seven lesbians and nine in 10 gay men report being abused by their partner (Edwards et al., 2015). Edwards et al. (2015) discovered that bisexual women were more likely than bisexual men to be victims of most types of IPV, except psychologically. When assessing for gender/age among same sex relationships, girls have higher rates of physical and psychological IPV compared to boys in the same type of relationship. In terms of perpetration, lesbians, bisexuals, and gay individuals were found to have a greater number of IPV perpetrators than heterosexual individuals (Edwards et al., 2015). Motives for violence among gay and bisexual men are conflict management and attachment fears (Edwards et al., 2015). Pertaining to urgency, less than half of gay male victims of IPV report the abuse to the police (Kuehnle & Sullivan, 2003).
Culture and diversity in the context of IPV can be assessed much further with the inclusion of military families. Stamm (2009) notes that domestic violence incidents are more common in the military than in the general population. The majority of IPV victims among military couples are females (Jones, 2012). The most common type of IPV among military families is physical abuse (Rentz et al., 2006). Cantos et al. (1994) found that in terms of gender, men and women in military families are equal aggressors; however, women are more likely to suffer injury/be hit. Minority members of the military were found to be more likely to experience and report IPV (Fonseca et al., 2006). Additional characteristics of military IPV victims pertaining to socioeconomic status are unemployment, low educational attainment, and low income (Stamm, 2009).
Code of Ethics and Family Violence
There are several American Association for Marriage & Family Therapy (AAMFT) codes of ethics that are applicable to family violence. In totality, three ethics codes have shaped the therapeutic services I provide to clients dealing with family violence. The first code is 1.8, which pertains to client autonomy in decision making (AAMFT, 2021). Ultimately, I have an ethical duty to allow clients to make their own decisions after discussing the consequences. For example, if a client decides to remain with their abusive partner, therapists must not stand in the way of their decision. Secondly, code 2.1, which entails limits of confidentiality exists with the client and other third parties such as courts or social workers (AAMFT, 2021). For instance, if third parties asked therapists if a client is romantically involved with a perpetrator or expecting a child this is not considered information that must be disclosed. Therapists must protect a client's confidentiality and stand firm on the code of ethics. Lastly, code 3.3 involves seeking assistance when challenged by a case that affects performance and clinical judgment (AAMFT, 2021). As an example, when a therapist is impaired by a family that continues to experience conflict in their relationship, he/she may seek a consultation or supervision. Family violence could be a daunting and overwhelming matter without these and other AAMFT code of ethics to guide the profession.
Conclusion
Given all that has been discussed, the greatest takeaway is that family violence can be caused by multiple factors rather than one exclusive reason. Principally, my perception of family violence is crafted from lived experience and consideration of family members’ encounters. Consideration of family violence theories gives way to applying principles to practice. Grasping the understanding of how targets of violence present in therapy is an essential component of mitigating the different types of family violence. Regarding family resilience, no universal measurement exists; however, families can acquire protective and recovery factors. The culmination of the Recovery Model is grasping its essence, which is recovery is not linear and looks different for everyone recovering from family violence. In addition, the gap must be bridged between the great allotment of data that is present for heterosexual IPV and that which is lacking for sexual minority IPV to ascertain social justice/optimal awareness and gauge cultural competence within the field. Family violence impacts the overall role and work of the therapist, which calls for consideration of the AAMFT code of ethics. In conclusion, clinicians cannot be fully equipped to provide sustainable and adequate treatment without delving further into family violence.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.