
Abstract
Mild traumatic brain injury (mTBI), with symptoms beyond 3 months, may be more common than previously believed, but is poorly understood. This has resulted in contradictory and confused information for service users, which has had an impact on those with mTBI and their families. This qualitative study aimed to improve understanding of the lived experiences of families of people with mTBI, with symptoms beyond 3 months. It extends a previous study, which focussed on all degrees of traumatic brain injury (TBI) (mild, moderate, and severe). Four individuals participated in semi-structured, virtual interviews. Following an interpretative phenomenological analysis (IPA), three superordinate themes were identified: (1) Going round in circles, (2) The second secondary impact, and (3) Dialogue with myself. Findings indicate that families of people with mTBI, with symptoms beyond 3 months, may experience many of the same challenges as families of people with moderate or severe TBI, albeit at a lesser intensity. This includes difficulty making sense of TBI and challenges to their identity, both of which mirror the comparator TBI study findings. However, findings also indicated that this group may experience different challenges to families of people with moderate or severe TBI, aspects of which have not previously been reported. Feelings of ambiguous loss may be increased by incongruity between information provided and families’ experiences, and by the varied availability and content of information. Implications for service providers are that consistent, transparent, and realistic information and education may aid adjustment and assist families to support people with mTBI.
Keywords
Introduction
“…grief is hard enough anyway, but when you don’t know the truth, everything freezes and you can’t move on.” Hare (2011).
Traumatic brain injury (TBI) is defined as damage to the brain by an external, mechanical force (Polinder et al., 2018). Under the Mayo criteria (Malec et al., 2007) severity of TBI is classified from mild to moderate and severe, with mild traumatic brain injury (mTBI) defined by loss of consciousness of less than 30 min, post-traumatic anterograde amnesia for less than 24 h or skull fracture with the dura intact. mTBI is common, and represents a global public health issue (Brazinova et al., 2021). The World Health Organization (WHO) estimates that worldwide, between 100 and 300 people per 100,000 receive medical assistance for mTBI annually (Holm et al., 2005). The WHO recommends adopting a bio-psycho-social model for rehabilitation (Glintborg, 2019), with families playing a key role in providing support, and facilitating patient education and adaptation (Bannon et al., 2020). The importance of family in mTBI recovery is highlighted in a causal loop diagram (CLD) (Kenzie et al., 2018), which seeks to facilitate an understanding of the challenges and complex interplay between the biological, psychological, and social in mTBI recovery. As the CLD illustrates, the social dynamics of mTBI recovery are complex, with a strong link between supportive relationships, resilience, and coping. Surveys of those with mTBI have found that social support predicts lower symptom reporting (Quan Zeng et al., 2016; Temple et al., 2016) and increased satisfaction with life (Seidl et al., 2015). However, mTBI can negatively impact family functioning, causing disruption to relationships with the person with mTBI (Jones et al., 2020; Nelson et al., 2019; Orff et al., 2016; Pugh et al., 2018).
Families support mTBI recovery both practically (Kerrigan & Giza, 2019) and emotionally (Azman et al., 2020). Those with mTBI are not always aware of their symptoms, so it is important that families are educated about mTBI (Quatman-Yates et al., 2020), in order to provide an informant perspective to clinicians (Marshall et al., 2015). Families can also increase self-awareness and comprehension of the condition (Cichon et al., 2015) and serve as an important external reference point, which helps people with mTBI make sense of the changes they have experienced (Snell et al., 2017). Despite their importance in recovery, families of people with mTBI have reported feeling left out of rehabilitation by medical services, resulting in frustration and a perceived lack of empathy (Hyatt et al., 2014).
Ambiguous loss theory (ALT) has the potential to explain the experiences of carers of people with TBI (Kreutzer et al., 2016). ALT contends that a lack of narrative, which is consistent with experience makes it harder to adjust to loss, increasing and prolonging distress (Dahl & Boss, 2020). ALT asserts that a phenomenon can exist, even if medical services cannot measure it, and should be recognized phenomenologically, regardless (Boss, 2007). The goal (consistent with the CLD) is to maximize resilience (Boss, 2018). An important factor in families supporting recovery may be their forming a clear concept of TBI, aiding them to understand what to expect and when and how to help people with TBI (Fadyl et al., 2017). Conversely, contradiction and confusion between care professionals may hinder people's ability to recover from TBI (Fadyl et al., 2017). Recovery from acquired brain injury (ABI) (meaning either TBI or non-TBI, e.g., cerebrovascular brain injury [Tibæk et al., 2019]) involves changes in identity for people and their family caregivers (Glintborg, 2019). Whiffin et al. (2019) posit that family identity reconstruction after TBI is important to recovery, requiring a narrative that is congruent with participants’ lived experience.
Clear information is important for recovery from mTBI (Brunger et al., 2014; Minney et al., 2019; Robinson-Freeman et al., 2020; van Gils et al., 2020) in both the acute (Prince & Bruhns, 2017) and chronic stages (Hart et al., 2018). Education can promote better social support for people with mTBI by normalizing relationship changes due to injury and suggesting positive adaptations for the individual and their social support network (Bannon et al., 2020; Klonoff, 2014). There is variation in the provision and quality of information after mTBI (Norman et al., 2020; Seabury et al., 2018; Silverberg et al., 2020). Table A1 in Appendix A expands on a comparison of treatment guidelines by Silverberg et al. (2020) by including UK guidelines. It shows that TBI information provided under NICE guidelines is not mTBI specific (Doneva, 2018), which may lead to variation and reduced care in the emergency department (Choudhary et al., 2022). NICE guidelines make no mention of mTBI, potentially perpetuating the lack of education about chronic phase mTBI (Hart et al., 2018). Table A1 also shows that patient information is not provided under SIGN guidelines, which van Gils et al. (2020) claim is clinically suboptimal. Where it is provided, information may be contradictory or confusing, hampering the family's ability to support recovery (Landau & Hissett, 2008; Saban et al., 2015). Information must be realistic, honest about the limitations of medical knowledge (Ghosh & Joshi, 2020), and include both verbal and written information (Terblanche, 2020), to provide a reference for third parties (e.g., employers) (Gourdeau et al., 2020; Graff et al., 2020; Young et al., 2005).
It has been suggested that providing information results in negative patient expectations and may hamper recovery (Mittenberg et al., 1992; Suhr & Gunstad, 2002; Whittaker et al., 2007). However, a recent meta-analysis by Niesten et al. (2020), failed to find support for these claims. Others point out that such a causal relationship has not been proven (Mah et al., 2018) and stress the importance of early, realistic, and accurate patient and family education in mTBI recovery (Minney et al., 2019; Prince & Bruhns, 2017). Some posit that providing realistic information is also important in creating trust, normalizing the patient experience, reducing fear, promoting self-care and improving patient outcomes (Cavallaro et al., 2018; Chief Medical Officer for Scotland, 2015; Fenning et al., 2019; Snyder & Engström, 2016; Yeh et al., 2018; Zolkefli, 2018).
Commonly held views among physicians may be incongruent with the experiences of people with mTBI and their families, increasing ambiguity. A common hypothesis among physicians is that mTBI heals within 3 months, and symptoms beyond that time are (a) caused by other factors (Lishman, 1988) and (b) rare (15%) (Iverson, 2005; Rutherford et al., 1979; Spinos et al., 2010; Sterr et al., 2006). However, imaging evidence (Asken et al., 2018; Khong et al., 2016; Wallace et al., 2018; Yin et al., 2019) suggests a bio-psycho-social approach to mTBI etiology is more appropriate (Aliyah et al., 2018; Cole & Bailie, 2016; Snell et al., 2016; Silverberg et al., 2015). In addition, some argue that mTBI symptoms after 3 months are not rare (Brady et al., 2022; McMahon et al., 2014; Theadom et al., 2016; Wäljas et al., 2015) finding that most people with mTBI still have symptoms 12 months post-injury (Dikmen et al., 2017; Hiploylee et al., 2017; National Academies of Sciences, Engineering, and Medicine, 2022; Nelson et al., 2019). The disease process of mTBI is also poorly understood. While people with mTBI and their families are typically advised that the injury was the moment of trauma and gradual improvement follows (Masel & DeWitt, 2010), the reality is more complex (Maas, 2016), involving the unfolding of a disease process that can lead to worsening symptoms over time, as well as recovery and periods of no change (Chancellor et al., 2019; Michel et al., 2019; Pacheco et al., 2019; DeKosky & Asken, 2017; Stocchetti & Zanier, 2016; Sullivan, 2019; Wallace et al., 2018). Reassuring assessment from medical services may unintentionally raise false hope in people with mTBI and their families, leading to feelings of disappointment and increased frustration (Landau & Hissett, 2008) when outcomes are less positive than predicted.
The impact of TBI on family members has mostly been examined in terms of psychopathological outcomes (e.g., anxiety), although more recently there has been a growing focus on the subjective experiences of families (Whiffin et al., 2021). Qualitative research has been called for to reinforce quantitative research, improve clinician understanding of the priorities of family carers of people with TBI, and assist them to improve support for families (Kneafsey & Gawthorpe, 2004; Oyesanya, 2017). A number of theories have been proposed to explain the importance of clear patient information, motivation in recovery, and change in identity among people with ABI and TBI and their families, but it is not yet clear the extent to which this applies to families of people with mTBI with symptoms beyond 3 months post-injury. Hyatt et al. (2014, 2015) studied the experiences of families of a military population with mTBI, although it is not clear how generalizable these findings are (Stillman et al., 2020). Other studies cover all TBI severities without distinguishing mTBI (Whiffin et al., 2021). Landau and Hissett (2008) explored the experiences of families of people with mTBI with a relationship breakdown focus, but symptom duration was not specified. Therefore, objectives of the present study are to explore the experiences of family members of people with mTBI symptoms that persist beyond 3 months, to investigate the importance of giving information to family members through analyzing their lived experience, and to undertake a comparative analysis between the findings of the original, TBI-focussed Townshend and Norman (2018) study and the current mTBI-focussed one.
Method
Design
This study has an ideographic focus and employed interpretative phenomenological analysis (IPA) (Smith & Osborn, 2008; Smith et al., 2009), based on an ontology of minimal hermeneutic realism, and an interpretative epistemology (Larkin et al., 2006). It assumed that there is one, universal truth, but that truth is interpreted by individuals, who are never value free (McLeod, 2011; Willig & Rogers, 2017). The method was online semi-structured interviews (Lyons & Coyle, 2007). The study is both a description and an active interpretation of experiences (Alase, 2017). It sought to synthesize findings from both within-participants in the current study, and between-participants, through comparison with the Townshend and Norman (2018) study. Qualitative studies are appropriate for extension (McLeod, 2011) and insights from phenomenological research may be seen as more relevant in the real world if evidenced by more than one population (Larkin et al., 2019).
Participants
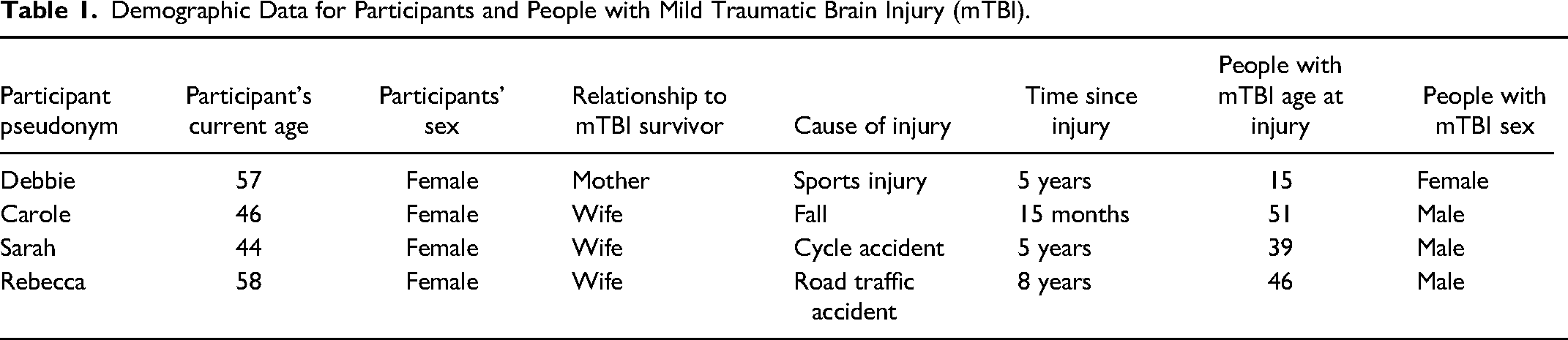
Participants were family members of people with mTBI, whose mTBI symptoms have persisted beyond 3 months. They have known the individuals with mTBI pre and post-mTBI. Participants are all English speakers over 18. Participants were self-defining, and no evidence of diagnosis was sought. Friends of people with mTBI were also sought, but none were recruited. Recruitment employed purposive sampling via The University of Derby and Headspace UK. In addition, participants were also sought via closed, mTBI-related Facebook groups. This follows the IPA approach of seeking a small homogeneous group for within-group, ideographic analysis (Pietkiewicz & Smith, 2014) and mirrors the recruitment approach for the Townshend and Norman (2018) study. Four women were recruited. No incentive was offered. Two were supported by UK medical services, one by US medical services and a fourth made use of both US and UK medical services. Demographic data regarding participants can be seen in Table 1.
Demographic Data for Participants and People with Mild Traumatic Brain Injury (mTBI).
Analytical Strategy
There were four interviews in total with a mean duration of 56 min (SD = 9 min). The sessions were transcribed verbatim with MS Word and analyzed in NVivo 12. Data were analyzed using IPA, (Smith & Osborn, 2008), as employed by Townshend and Norman (2018). The themes from the Townshend and Norman (2018) study were disregarded initially to allow fresh analysis of data from the present study. After listening to interviews and reading transcripts multiple times, transcripts were analyzed in detail (Nizza et al., 2021). Initial descriptive, linguistic, and conceptual observations (Smith et al., 2009) were recorded. A record was kept of data supporting each theme. This process was repeated for each interview, and convergences or divergences were noted (Nizza et al., 2021), new themes were added and more data was noted as supporting preexisting themes. The themes were then analyzed and grouped into superordinate themes. Themes that did not relate to superordinate themes were discarded. Superordinate themes were tested by checking back to ensure they were reflected in the data and further quotes were identified to illustrate superordinate themes. Analysis was shared with participants for participant verification (Peat et al., 2019). One participant provided feedback, verifying that the analysis was congruent with their experience. A second method of triangulation was employed, where a co-author reviewed the analysis. The basis for data interpretation was recorded and made explicit in the presentation of the analysis. A reflective diary was also used to record the lead author's thoughts and feelings throughout the study process. A comparison of findings was then made between the present mTBI study and the Townshend and Norman (2018) TBI study. This began with demographic data before the themes were compared. Evidence in the data was sought to support any commonalities or differences identified.
Results
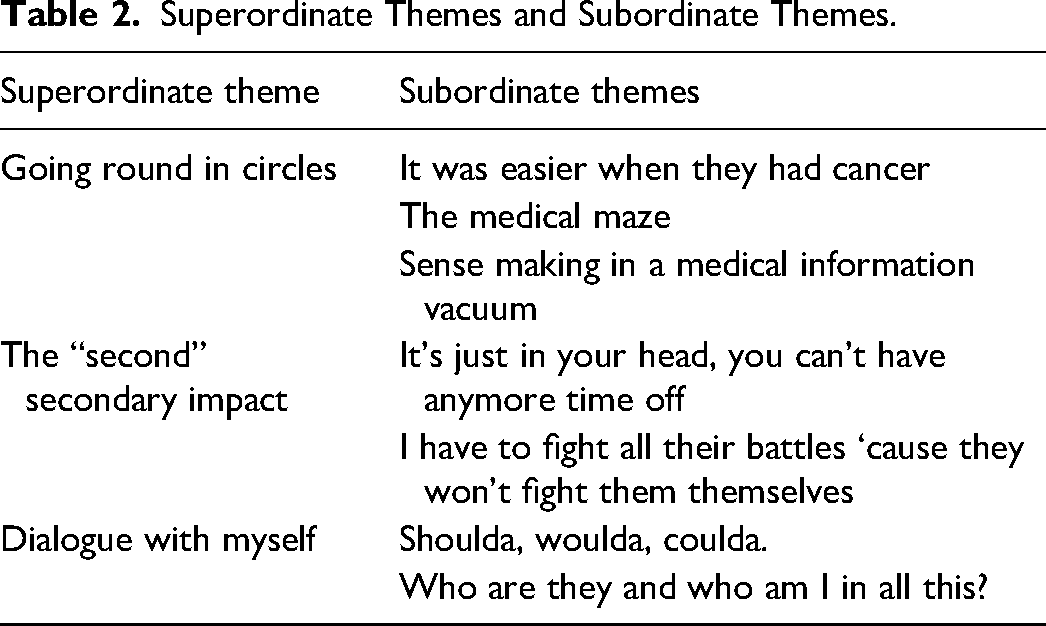
Three superordinate themes were identified in the study. These were (1) Going round in circles, (2) The “second” secondary impact, and (3) Dialogue with myself. A table of final superordinate themes and subordinate themes are shown in Table 2. Each theme is outlined in turn below, with detailed descriptions and quotes to illustrate themes.
Superordinate Themes and Subordinate Themes.
Theme 1: Going Round in Circles
Going round in circles captures the lack of meaningful direction expressed by participants as they try to navigate the medical system to seek information, treatment and try to support the recovery of their loved ones living with a mTBI.
It was easier when they had cancer
This subordinate theme captures how participants’ experience of mTBI compared to supporting people with other illnesses (real, or in “Debbie's” case an imagined other illness). “Carole” observed that accessing services for mTBI had “just been awful” compared to when her husband had cancer: It was easier when he had cancer, because there's the support systems out there … it's all just so vague.
All four participants had family who were people with mTBI with symptoms lasting more than 3 months. I just don't see that there's a flow chart of what you should do first and where you should go if you don't get better in the first three weeks to three months. (Debbie)
Rebecca regretted that the mTBI was invisible and voiced frustration that the usual prompts for understanding were missing. …you see a sling, you understand what's going on.
The repeated reference to limbo denotes an experienced lack of direction from medical professionals. Conceptually, it indicates a hampered need to be working toward recovery with clear information from medical professionals about the starting point (diagnosis), journey (treatment pathway), and destination (prognosis). None of the participants talked of hope. The negative comparison participants made with the clearer treatment pathways of other illnesses implies a sense of loss that mTBI treatment is so much harder to navigate.
Navigating the Medical Maze
All participants talked about the challenges they had navigating medical services. This subordinate theme captures participants’ sense of the “battle” (Rebecca) to be validated by the medical profession and other systems, and to find treatment. It describes how their experience of a “lack of information and lack of support for the medical side is awful” (Carole). Conceptually, the participants described their experience in terms of movement around a system, getting “stuck” (Carole) and “going round in circles” (Carole).
This search is frustrating and adds to the burden of caring and advocating for the person with mTBI. It is clear from their comparisons with other experiences of medical services that the battle and onus on them to search is unexpected and onerous.
Sense Making in a Medical Information Vacuum
This theme reflects how the lack of a narrative from medical services that is congruent with their experience leaves participants in an information vacuum. Participants report being left in limbo when they do not experience the prompt recovery predicted by medical providers.
Participants perceived information as “misinformation” (Debbie) if it was not congruent with their experience, leaving them “not knowing what to believe” (Debbie). They could not use incongruent information to make sense of their experience, so participants tried to fill the vacuum themselves. However, participants were aware they are not medical specialists and therefore lack the knowledge and capacity to make informed decisions. Rebecca states she is “willing to pay but I don’t know who to choose” or “who's good”. Similarly, Debbie is left asking “what avenue do I take?”. Rebecca thus describes herself as “Floundering about trying to get the right reports ready.”
“Floundering” evokes a sense of trying one's best but finding it “exhausting” (Sarah) and knowing that one lacks ability. This has a cost to participants’ mental well-being, as well as creating an additional burden. It's overwhelming…You just can't think what to do next…It's hard, it's mentally draining. (Carole)
The strong relief at being believed reveals the cost to her sense of self-worth of not having been believed previously.
Theme 2: The “second” Secondary Impact
The “second” secondary impact refers to the impact that family report from dealing with systems that do not seem to understand their reality. There is a primary impact of the injury on people with mTBI themselves, a secondary impact on the family of people with mTBI but then there is an additional “second” layer of impact on family from not being understood or believed, hence this being called The “second” secondary impact. It's Just in Your Head, You Can't Have Any More Time Off
This subordinate theme captures the additional impact on participants of not being believed or understood. One way this manifests itself is in participants’ experience of a “battle” (Rebecca) or “fight” (Carole) (words used repeatedly) with systems (e.g., medical, employers, and school) that don't recognize the injury. His work have been horrifically bad throughout the whole thing. (Carole)
Participants report they have no clear understanding of themselves and no “proper literature…” they “…could pass on to people” (Sarah) to explain mTBI. They report that they feel alienated from medical services because they feel unheard, not believed, and that the nuances of the condition are not understood.
This failure to recognize the condition is a shock to participants, as their expectation is that medical services and systems will not only recognize injury, but be sympathetic and supportive. When this does not happen there is disappointment and anger. One of the people at work said to him “Shit happens.” “Just get on with it.” That was the welfare person. (Rebecca)
Choosing to report the phrase “Shit happens” suggests Rebecca experiences an uncaring system that does not understand or sympathize with her. There is a sense of being let down in the language used by all participants. Their extreme language (“horrific”) indicates shock and disappointment. I Have to Fight All Their Battles ‘Cause They Won't Fight Them Themselves
This theme summarizes participants’ experiences of being an advocate for the person with mTBI. You’re almost suddenly thrown into being an advocate straight away. Having to sign all the paperwork because he's too fuzzy to know what's going on. (Carole)
All participants express the view that people with mTBI lack the ability to fully advocate for themselves. Whether it is the practicality of chasing medical referrals, the fact that people with mTBI “can't always articulate what's going on” (Carole) or that they lack the energy to struggle to access help. Yeah, well he doesn't fight it. Yeah. He’ll just roll over and play dead about it. (Rebecca)
Participants report that medical services do not recognize the extent to which people with mTBI lack the capacity to self-advocate. No, he can't do it. He's got a head injury. That is the whole point we need to. I need to do it on his behalf. (Carole)
This perceived lack of appreciation of incapacity by medical services seems to create a barrier to participants advocating for the person with mTBI. Medical services may not recognize the lack of capacity to self-advocate but participants are all too aware, and this adds to their workload and worry.
Theme 3: Dialogue with Myself
Dialogue with myself reflects participants’ struggles to make sense of the disease process through internal dialogue and revisions to their sense of self and other. Shoulda, Woulda, Coulda.
This subordinate theme relates to all participants’ regret over their earlier medical decisions. Debbie expresses this most clearly: There were just a lot of mistakes made, that maybe caused this injury to last. You look back and you say “woulda, coulda, shoulda”.
When Debbie looks back with regret, it is with the implication that she should have known better.
I had been, if I knew, but I just, I think in the beginning of the thing you just don't think they're not going to get better. (Debbie)
Participants differ in how they express regret. Unlike Debbie, Rebecca expresses anger at medical services for not investigating brain injury and some crossness at herself for not having thought of it. She is more forgiving of her past self than Debbie. I think we got lulled into that sense of “ohh it might take six months”. (Carole)
I think I didn't want to go to anyone, because I want everything to be OK. (Sarah)
There is a sense that Sarah too thinks she has been foolish, which seems to go against her otherwise competent identity. Who Are They and Who Am I in All This?
This final subordinate theme describes the impact of the person with mTBI's injury on the participant's identity and their perceived identity of the person with mTBI. All participants remarked on changes to the person with mTBI's identity post-injury. The person with mTBI was described as not being “right” (Rebecca and Sarah) and “not really him anymore” (Carole). This profound change forms a significant aspect of participants’ internal dialogue. All participants recounted a change in the person with mTBI's occupational identity. The loss of doing work and leisure activities that the person with mTBI loved, often came with a loss of social connections, leading to isolation for participants and the person with mTBI.
Discussion
This IPA study aimed to explore the experiences of families of people with mTBI symptoms that persist beyond 3 months. Data from semi-structured interviews with participants were summarized into three superordinate themes: (1) Going round in circles, (2) The “second” secondary impact, and (3) Dialogue with myself. The study compared findings with Townshend and Norman (2018) which focussed on people with mild, moderate, and severe TBI. All the Townshend and Norman (2018) themes were mapped to themes in the present study. Findings indicate that families of people with mTBI, where symptoms last more than 3 months, may experience many of the same challenges as families of people with moderate or severe TBI, albeit at a lesser intensity. This includes difficulty making sense of TBI and challenges to their identity, which mirrors the findings of Townshend and Norman (2018). In addition, they may experience some challenges in a different way to families of people with moderate or severe TBI. These challenges are not present in the Townshend and Norman (2018) findings. For example, they may feel frustration, caused by lack of congruity between patient education and their experience. Also, their experience of ambiguous loss may be further complicated by the lack of availability and quality of information about mTBI. The quest for information and care is experienced by all participants and this is widely reported among families of people with mTBI (Carlozzi et al., 2016; Landau & Hissett, 2008; Hyatt et al., 2014). Chronic phase support is more frequently provided to people with moderate or severe TBI and their families, whose needs for rehabilitation are greater and more complex (Hart et al., 2018; Graff et al., 2018).
As predicted by ALT (Boss, 2007; Boss, 2018; Dahl & Boss, 2020), participants experienced an inability to adjust to a new normal due to the ambiguity of their loss. This is consistent with findings by Landau and Hissett (2008), and consistent, but less extreme than, findings in families of populations that included more severe TBI (Giovannetti et al., 2015; O’Keeffe et al., 2020; ThØgersen & Glintborg, 2022). Participants also appeared demotivated by the lack of clear patient information, as predicted by Self Determination Theory (Adams et al., 2017; Kusec et al., 2019; Ryan & Deci, 2019). This echoes the findings in an mTBI population by Auclair-Pilote et al. (2021), who speculated that poor patient education led to diminished competence, which was a causal factor in lower motivation for recovery. This finding raises the possibility that confusion may demotivate people with mTBI, as well as their families.
This may be further explained by Identity Process Theory (IPT) (Breakwell, 1986; Jaspal & Breakwell, 2014), which understands identity after change in terms of assimilation of change and evaluation. As has been discussed, identity disruption in family caregiving is common (Cooper, 2021; Eifert et al., 2015). TBI represents an existential change for people and their families that requires a reconstruction of identity (Glintborg et al., 2018; Whiffin et al., 2019). Consistent with IPT and findings from Landau and Hissett (2008), all participants reported being hampered in assimilating change due to a lack of narrative from medical services that was congruent with their experience. Participants also reported feeling negatively evaluated by medical services and not feeling believed or supported, which IPT predicts would further hamper their ability to assimilate change. This negative evaluation and lack of congruent narrative was not reflected in the themes of the Townshend and Norman (2018) study.
Consistent with Social Identity Theory (SIT) (Scheepers & Ellemers, 2019; Tajfel, 1974), the poor evaluation and lack of understanding by medical services (salient others) reported by participants may also hamper the families’ ability to maintain or reconstruct their identity post-injury. The impact of injury on family member identity was a major finding of the Townshend and Norman (2018) study. It was mirrored in the present study, albeit to a lesser extent (possibly because the present study focussed on less severe TBI). In the present study, there was more emphasis on the impact on wider socializing and the resulting isolation. Participants’ lives were changed in terms of self-image, family role, relationships, and social group membership. SIT predicts that social groups are important in identity formation and self-esteem (Scheepers & Ellemers, 2019; Tajfel, 1974). Participants experienced a negative impact on their identity from leaving groups post-injury. Another common finding by Townshend and Norman (2018) was the reference to people with TBI being “off-center” (p. 80) and them but not them, consistent with qualitative findings by Saban et al. (2015). TBI is experienced as an invisible injury by families in both studies. This invisibility adds to the person with mTBI's challenge of being understood and supported by medical services (Childers & Hux, 2016). As discussed, patient education often sets the expectation of recovery within 3 months (Torbay and South Devon Trust, 2018; University Hospitals Birmingham Trust, 2018), despite recent findings that most people with mTBI experience symptoms beyond then (Hiploylee et al., 2017; Nelson et al., 2019; Dikmen et al., 2017; Theadom et al., 2018; McInnes et al., 2017). Townshend and Norman (2018) describe “repeated stages of unrealised hope for improvement” (p.13), which was also articulated by participants in the present mTBI study, albeit from a particular perspective. Participants described the gap between the recovery trajectory they understood from medical services, and their experience. By contrast, the Townshend and Norman (2018) study described a hoped-for recovery, but did not refer to expectations set in patient information being at odds with participants’ experiences. This possibly explains why the sense of injustice and anger regarding the quest for care in the present findings and elsewhere (Carlozzi et al., 2016; Landau & Hissett, 2008) is absent from the Townshend and Norman (2018) study. The concept of a battle for care and information is also missing. Participants in the present study experience care ending after 3 months. Koehmstedt et al. (2018) suggest that the ideal TBI caregiver information would be part of a long-term care plan, although it is not clear how this relates to mTBI, since Koehmstedt et al. (2018) did not discuss the severity of TBI. For the families of people with TBI in the Townshend and Norman (2018) study, patient education is perceived as inadequate for them to fully participate in recovery. In the present study it is experienced as inadequate, but also confusing, leading participants to feel frustration consistent with the Landau and Hissett (2008) study of people with mTBI and their families.
Participants struggled to make sense of the disease process, and experienced guilt at missing earlier opportunities to support the person with mTBI. This echoed findings that symptoms develop and change over time (Tenovuo et al., 2021) and information (Silverberg et al., 2020) and medical support can be sporadic (Holloway et al., 2019), leaving caregivers of people with TBI to make the best decisions they can, while being aware that they lack capacity (Graff et al., 2018; Koehmstedt et al., 2018). For participants, this seemed to create a fertile ground for hindsight guilt (hindsight bias [Klein et al., 2017; Fischhoff, 1975] resulting in guilt), where past decisions are interpreted as though participants had had present knowledge. Participants feel guilty, because they feel they should have known better. Such guilt can lead to poorer functioning and reduced quality of life (Griffin et al., 2019). Also, while Townshend and Norman (2018) and the present study both discuss the challenge of reduced capacity of the person with TBI, only the current study findings suggest advocating for people with mTBI is a challenge. This is, however, articulated in other literature surrounding TBI and mental capacity and appears to be because the reduced capacity of people with TBI to self-advocate is not always recognized by medical services due to the relative invisibility of their injury (Holloway & Norman, 2022; Moore et al., 2019; Norman, 2016).
Ambiguous treatment pathways were discussed by all participants but not mentioned in Townshend and Norman (2018), suggesting some ambiguity may be specific to mTBI. As discussed, ALT (Dahl & Boss, 2020) predicts that adjustment to loss requires ambiguity to be clarified or at least accepted. However, current mTBI patient information may not support that. Patient information is not always provided (Norman et al., 2020; Seabury et al., 2018; Silverberg et al., 2020) and where it is, patient education (Torbay and South Devon Trust, 2018; University Hospitals Birmingham Trust, 2018) does not reflect the current, partial understanding of mTBI (Maas et al., 2017; Mayer et al., 2017; Nguyen et al., 2016; Pozzato et al., 2020; Sharp & Jenkins, 2015). In this context, Norman et al. (2020) have called for an acceptance of what is not known for the benefit of people with TBI and their families. Such information would be a basis for realistic conversations with providers (Chief Medical Officer for Scotland, 2015; Fenning et al., 2019), which may assist families to adjust to the injury (Cavallaro et al., 2018; Hyatt et al., 2014; Landau & Hissett, 2008; Snyder & Engström, 2016; Yeh et al., 2018; Zolkefli, 2018) and maximize their resilience to live with ambiguity, consistent with ALT (Boss, 2018).
Reflexivity
The lead researcher is a person with mTBI, with symptoms that have persisted beyond 3 months post-injury. Rather than using Epoché to fence off this experience, IPA has allowed the lead researcher to consciously use their experience, to interpret the participants’ interpretation of their experience. In this way, a double hermeneutic approach has been taken (Eatough & Smith, 2017). By making these assumptions explicit and documenting reflection and decisions made during the study, the researchers aim to maximize transparency and enable critical review (Peat et al., 2019).
Limitations
Since this was an IPA study, a homogenous sample was sought (Smith & Osborn, 2008; Smith et al., 2009). All participants were civilian, English-speaking, adult, White, women, and educational attainment and mental health data were not collected. Also, this research focussed on families, whereas people with mTBI may have other support, or none.
Conclusion
This qualitative study aimed to explore the experiences of family members of someone with mTBI symptoms that persist beyond 3 months. It sought to extend and compare findings of the Townshend and Norman (2018) study, which focussed on all severities of TBI. Through extending that study to examine mTBI, the present study has found that families of people with mTBI, where symptoms last more than 3 months, may experience many of the same challenges as families of people with moderate or severe TBI, albeit at a lesser intensity. This includes difficulty making sense of TBI and challenges to their identity. They may experience different challenges to families of people with moderate or severe TBI, such as frustration caused by lack of congruity between patient education and their experience. Although they may experience ambiguous loss, in common with families of people with moderate and severe TBI, their experience of ambiguity may be exacerbated by a lack of clear mTBI patient information. Expectations set by patient education may be unrealistic and based on outdated research. Patient education that includes an acceptance of what we do not know, may benefit families of people with mTBI by reducing ambiguity, helping them to adjust to the injury, have realistic conversations with medical services and maximize their resilience to living with remaining ambiguity. Findings suggest that people with mTBI may not always have the capacity to fully self-advocate. Families may benefit from medical services facilitating more family advocacy. More research is needed to explore how generalizable these findings are and to develop theory in this area.
Footnotes
Acknowledgments
The authors would like to thank the participants for their time and insight and Headway UK for their help with recruitment.
Author Note
James Gamgee is now at the School of Social Sciences, Herriot Watt University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article