
Abstract
In this study, we explored how psychological violence within a partner relationship relates to resilience and alcohol abuse of Portuguese women, particularly, testing the mediating role of resilience. A cross-sectional sample of 464 Portuguese women with a partner relationship was screened for psychological violence, alcohol abuse, and resilience. Results showed differences in terms of age, marital status, and current employment situation. Psychological violence was negatively related to resilience and positively related to alcohol consumption. Resilience also showed a negative relationship with alcohol consumption. A partial mediation was found between psychological violence and alcohol consumption through resilience, supporting the crucial role of resilience to break the negative “chain” between psychological violence and alcohol consumption.
Introduction
Intimate partner violence is a current worldwide issue assumed as being a multidimensional phenomenon (Martín-Fernández et al., 2019; World Health Organization [WHO], 2019), which occurs regardless of social and economic strata, religion, culture, gender, race, or color, affecting mostly women as victims (Coll et al., 2020). Currently framed as being a form of interpersonal violence, intimate partner violence is seen as a serious violation of human rights and freedom, appearing as a serious attack on human dignity, independence, and respect, affecting individual ethical principles and rights (Bartolomei, 2015; Devries et al., 2013). Intimate partner violence is a public health problem, being estimated that nearly one-third of women are likely to experience some form of violence during their lifetime (Devries et al., 2013; WHO, 2019), with a significant impact on the victim's physical integrity and mental health but also for exposed children (e.g., Bair-Merritt et al., 2006; Bowen, 2015; Mikton, 2010). Intimate partner violence increases the likelihood of child peer problems (Bowen, 2015), as the development of socio-emotional and neurological problems (Mueller & Tronick, 2019) or later becoming perpetrators or victims (Pereira et al., 2020; WHO, 2019). Also, several studies addressing the subject of violence victimizing women showed devastating results in terms of physical and mental health, increasing the risk of other long-term health problems such as depression, chronic pain, drug abuse, and alcohol (WHO, 2012). However, despite the adversities faced by those victims, some of them can face and adapt positively to the traumas experienced, showing overcoming behavior, growth, and personal strengthening, a fact that shows their resilience ability (Gopal & Nunlall, 2017; Herreira Trigueiro et al., 2014; Howell et al., 2018). In line with this argument, going a step further, through the present study, we aim to contribute to filling the gap in the literature by analyzing the relationship between psychological violence within a partner relationship and women's alcohol consumption including the analysis of the mediating role of women's resilience.
This work has the potential to contribute to literature and practice. First, as Sáez et al. (2020) noted, the relationship between psychological violence and victims’ use and abuse of alcohol remains understudied. Thus, studies like the current one could offer an important contribution to the literature. Second, we explore the mediating role of women's resilience in the relationship between psychological violence and alcohol consumption. As such, the present study also has the potential to contribute to the literature by testing a more complex model that includes the analysis of both a traumatic or stressful situation (i.e., being a victim of psychological violence within a partner relationship) and an outcome (i.e., lower alcohol consumption) of increased women's resilience. Finally, considering that resilience is not a fixed or immutable characteristic the individuals “have” (Cicchetti, 2010), despite some doubts and inconsistencies in resilience programs (Leppin et al., 2014), evidence suggests that it might be developed or trained under adequate circumstances and methods (Joyce et al., 2018). With the results obtained, we expect to contribute to the intervention with women who were victims of psychological violence.
Intimate Partner Violence: A Framework
Intimate partner violence consists of continuous violent behavior or coercive control over anyone who lives or does not live in the same household (WHO, 2012). This pattern of continuous violent behavior results in “physical, sexual, emotional, and psychological damage, and in the imposition of social isolation or economic deprivation of the victim, to dominate him/her, make him/her feel subordinate, incompetent, worthless, or make him/her live in a climate of permanent fear” (Ribeiro et al., 2009, p. 11). This traumatic experience causes changes in the personality of the victims (Pereira et al., 2020), as well as in their way of being in the world. Furthermore, experiencing this situation may lead to post-traumatic stress, anxiety, depression, sleep disorders, eating disorders, low academic performance or job productivity, and the use of alcohol and other drugs (Devries et al., 2013; WHO, 2008, 2012).
According to the World Health Organization (WHO, 2012), there are several forms of intimate partner violence. Physical violence is defined as the intentional use of physical force to cause harm, injury, or damage (e.g., throwing away something that could hurt, pushing, shoving and slapping the victim; Machado et al., 2018). Sexual violence consists of the use of physical force to coerce the person into a nonconsensual sexual act, including abusive sexual contact or rape, obliging the victim to have sex without a condom, or completing a sexual act with a person who is unable to decline participation in the act (Machado et al., 2018). Emotional or psychological violence is defined as the use of insults, shouting humiliation, threats, or other verbal abuse (Machado et al., 2018). Violence is linked to constant intimidation and belittlement, where the aggressor is constantly diminishing the victim as a person, making the victim feel inferior (Pereira et al., 2020). Also, controlling behaviors, such as isolating the person from their significant persons, monitoring movements, or restricting access to resources are types of violence (Pereira et al., 2020). However, despite the differences among the several forms of intimate partner violence previously mentioned, they are likely to occur simultaneously (Krebs et al., 2011).
Psychological violence is assumed to be the form of violence most frequently practised by an intimate partner, i.e., the spouse/partner of the victim (Dokkedahl et al., 2019; WHO, 2012). It is an intentional act, by verbal or nonverbal intimidation, to cause pain, damage or anguish through threats and humiliations to the victim's self-concept and self-esteem, by restricting sources of emotional support, as well as, by limiting the personal territory and the victim's freedom (e.g., isolation, stalking). Although several studies have pointed out the harmful effects of psychological violence on mental health, the conceptualization of the phenomenon is still ambiguous both in research and in clinical practice. Despite the lack of consensus about its conceptualization (Martín-Fernández et al., 2019), it is simultaneously, the most elusive and difficult form of violence to identify, recognize and prove, generating deep and lasting suffering in the victims. Thus, only the subsequent effects of psychological abuse are noticeable in the long run.
Similar to what is observed in other European countries, in Portugal, high rates of intimate partner violence have been identified. In 2020, domestic violence, which includes intimate partner violence, represented 35.8% of the criminality registered in the country concerning the category of criminality against persons (Secretaria Geral Ministério da Administração Interna ([SGMAI], 2021). Generally, the situations of domestic violence resulted in minor injuries (35.3%) or absence of physical injuries (64.3%) for the victim; however, it should be noted that in less than 1% of the cases the resulting injuries were serious (SGMAI, 2021). Psychological violence was present in 82.2% of the situations, physical violence was present in 68.2% of the situations, economic violence was present in 8.0% of the situations and sexual violence was present in 2.8% of the situations (SGMAI, 2021). Victims were mainly female (81.4%), married (42.3%), aged 42 years on average, and not economically dependent on the aggressor (82.6%). Most of the victims had educational qualifications equal to the ninth grade or lower (62.1%). Half of the victims were employed (51.9%).
Portugal signed and ratified the Istanbul Convention, i.e., the international human rights treaty on violence against women and domestic violence (European Institute for Gender Equality [EIGE], 2020). In Portugal, it is possible to make an anonymous report of intimate partner violence to the authorities, without the consent of the victim, since it is a “public” crime (EIGE, 2020).
Psychological Violence and Individuals’ Resilience
Due to these remarkable events in the lives of the victims, we would be likely to expect the victims as having difficulty trusting people again and this difficulty to be a “lasting legacy” in the lives of these women (Howell et al., 2018). When faced with a traumatic situation, some women are unable to accept the problem or face it; on the other hand, some women manage to face the problem and adapt positively, showing overcoming behavior and establishing meaningful lives after the violence (Herreira Trigueiro et al., 2014; Howell et al., 2018). Chen and Bonanno (2020) described this capacity as resilience, defining it as the ability that adults, exposed to an isolated and highly disturbing or even traumatic event, have to maintain relatively stable and healthy levels of psychological and physical functioning. As such, resilience can be understood as a process that makes it possible to transform a traumatic situation into a possibility of learning and personal growth (Herreira Trigueiro et al., 2014; Tsirigotis & Łuczak, 2018).
Resilience has been studied in a variety of models, particularly since the seventies of the twentieth century (for a review, read Masten et al., 2021). Based on studies concerning children of alcoholic or mentally ill parents, authors explored this process either as a trait, referring to individual characteristics (e.g., self-efficacy, good social skills), as well as a process, which considers it as a set of factors, internal and external to the subject, that interact with each other (Wlodarczyk et al., 2017). In this vein, it is possible to affirm that resilience is not limited to a personality trait or a fixed attribute of certain people, but as a construct created within the process of social interaction, where risk and protection factors are at stake, including individual responses and the contributions related to family ties and social support networks (Chen & Bonanno, 2020; Dias et al., 2016; Masten et al., 2021).
At a personal and individual level, resilience is considered by some authors to be something innate, arguing that people who adjusted positively to stressors, had favorable characteristics such as self-esteem, intelligence, and independence (Gopal & Nunlall, 2017). However, the development of this field allows us to understand the interactive relationship between personal characteristics and the context within the stress process (Wlodarczyk et al., 2017; Masten, 2001). More than an extraordinary process, it is an ordinary magic process that allows people to develop and adapt to challenging contexts and systems where they are developing (Masten et al., 2021). Bonanno (2004) suggests that, when facing loss and trauma, resilience exists more often than is assumed. This way, resilience can be understood but also promoted (Anderson et al., 2012; Masten et al., 2021).
Violence is one of the significant challenges people are exposed to (Bonanno, 2004). Existing evidence suggests that women experiencing and facing domestic violence present lower resilience (Tsirigotis & Łuczak, 2018). Particularly domestic violence perpetrated by fathers, but also intimate partner violence exerts a significant effect on resilience. Moreover, resilience in battered women was found to be correlated with lower psychological distress (Humphreys, 2003). Bearing in mind the literature, this study's first hypothesis was as follows:
Hypothesis 1: Psychological violence within a partner relationship has a significant and negative relationship with women's resilience.
Women's Resilience and Alcohol Consumption
Alcohol is the most popular drink in the last ten thousand years in occidental countries (Pascual, 2004). Being associated with religious rituals, ceremonials but also celebrations, alcohol has also an important role in economics and public policies (Garcia del Castillo & Dias, 2015). According to official data, in 2016, more than 2.3 billion people aged more than 15 years used to drink alcohol currently, and more than half of those people were from the Americas, Europe, and Western Pacific (WHO, 2018). Despite the cultural acceptability of alcohol use, sufficient evidence exists regarding its negative consequences in mortality and morbidity and is being considered one of the leading risk factors for global disease burden (e.g., Griswold et al., 2018; Shield et al., 2020; WHO, 2018). As such, it is important to analyze variables that may contribute to decreasing individuals’ alcohol consumption, such as resilience, in victims of psychological violence.
Concerning the studying of intimate partner violence, empirical evidence regarding the use and abuse of substances by intimate partner violence victims remains scarce (Sáez et al., 2020). Moreover, the existent empirical evidence usually focuses on the use and abuse of substances as a coping strategy for facing continuous violent experiences (Sáez et al., 2020). More precisely, review studies tend to associate alcohol consumption with social reasons to obtain valued social outcomes or as a coping strategy to manage emotions or internal feelings (Cooper et al., 2016). Despite some discrepancies in the literature, systematic review and meta-analysis studies present a clear link between alcohol use and victimization among women, despite the difficulties to understand the directionality between these variables (Devries et al., 2014).
Apart from the association between alcohol use and violence, literature allows us to understand the negative correlation between resilience and alcohol use. Cohort studies with youth report lower levels of resilience among alcohol users (Kennedy et al., 2019). Also, studies with twins allow us to find a significant role of resilience in the protection of alcohol use disorders (Long et al., 2017). Considering the literature review, the following hypothesis was formulated:
Hypothesis 2: Women's resilience has a significant and negative relationship with alcohol consumption.
Indirect Effects: A Proposal for the Mediating Role of Women's Resilience
Resilience is commonly conceptualized as a mediating variable in several studies (Yang et al., 2020) and, by doing so, it can be hypothesized as a way through which women face psychological violence and do not “refugee” themselves in alcohol consumption. In fact, the study conducted by Meneses-Gaya and Ferro (2015) showed that students who did not consume alcohol had higher levels of resilience, and the results of their research indicated that resilience would function as a protective factor against alcohol consumption. Another study carried out by Wingo et al. (2014), using a cross-sectional study with 2024 adults, including both men and women, suggests that resilience seems to mitigate the risk of harmful alcohol and illicit drug use despite traumatic experiences and childhood abuse.
In summary, resilience can be defined as a set of protective factors, mechanisms, and processes that contribute to obtaining a good adjustment of the individual, despite the occurrence of experiences with stressors that predict a greater risk of developing psychopathology. Therefore, a mediating hypothesis was derived as follows:
Hypothesis 3: Women's resilience has a mediating effect on the relationship between psychological violence within a partner relationship and alcohol consumption.
Method
Participants and Procedure
A sample of 464 Portuguese women was collected. The women ranged in age from 18 to 74, with an average age of 32.69 (SD = 12.28). Most women had a university degree (51.50%), were single (51.10%), and were employed (58.8%). A description of the sample is reported in Table 1.
Demographics of the Sample (n = 464).
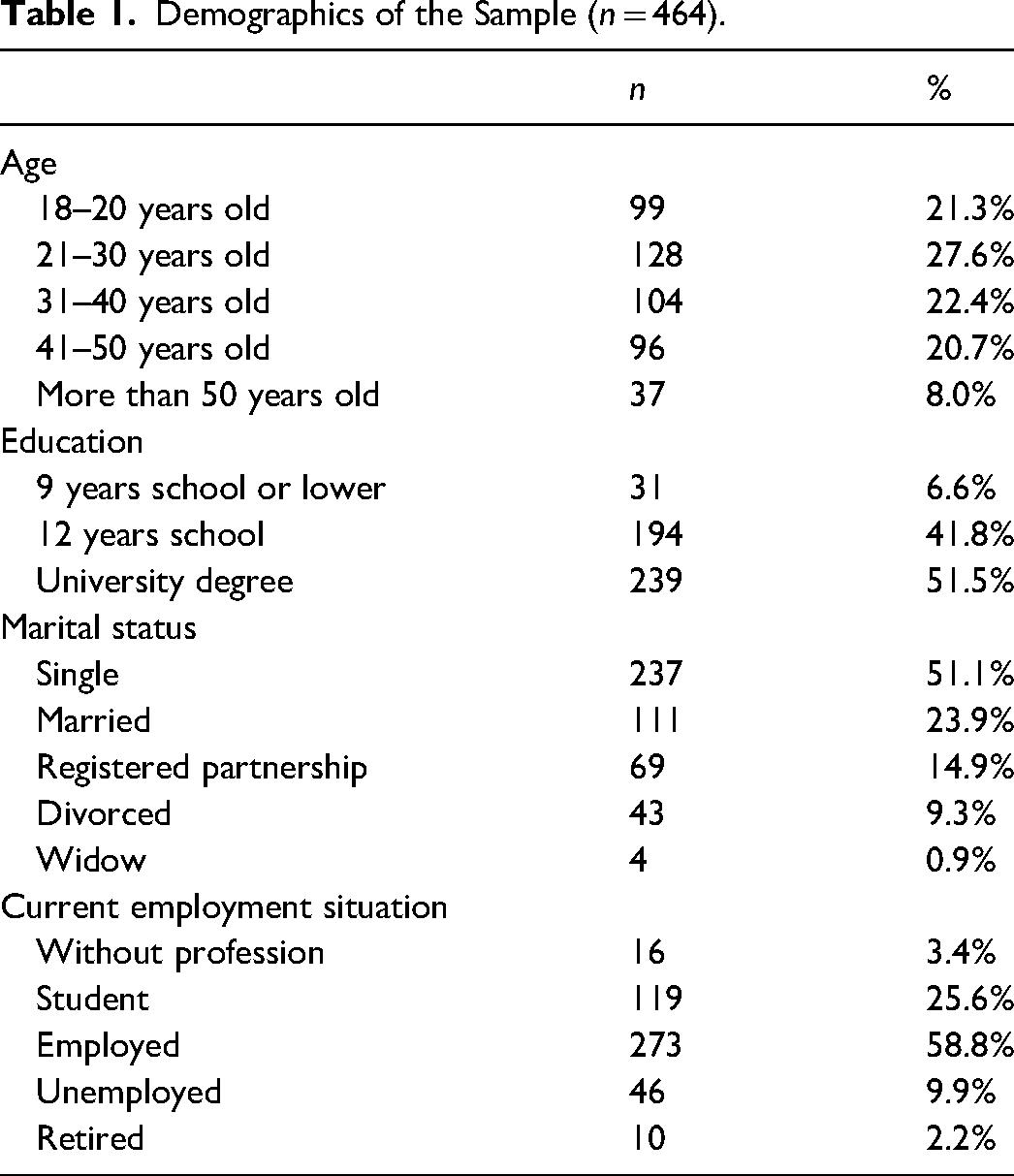
A nonprobabilistic sample was used and data were collected by convenience. More precisely, answers were collected through an online questionnaire, using a snowball process. The link to the online questionnaire was disseminated through social solidarity institutions, and social media within the scope of domestic violence. After clicking on the link of the questionnaire, potential participants were provided first with information on the study, the contacts of the researcher-in-charge, and the informed consent form. Anonymity and voluntary participation were guaranteed in the Informed Consent form which also presented the main goal of the study. More precisely, no personally identifying information was collected (e.g., names, phone numbers, email addresses), and we clarify if participants opted to participate, they could voluntarily give up the study at any time without providing any justification. The opportunity to receive overall feedback on the global results of the research was assured by providing the e-mail address of the researcher-in-charge. Only participants who provided informed consent were able to participate in the study. The inclusion criteria were as follows: female sex, aged 18 years or older, with at least one intimate heterosexual relationship in their past, and living in Portugal. The exclusion criteria were as follows: transgender or transsexual individuals.
Measures
In addition to the ad hoc sociodemographic questionnaire, to collect information regarding age, marital status, education, professional status, regular alcohol consumption, types of violence perpetrated in the past, and its frequency, participants completed the following self-administered tools:
Alcohol consumption
Alcohol Use Disorders Identification Test (AUDIT; WHO, 1989), in its Portuguese version validated in 2002, is being used for the diagnosis of alcohol-related problems. With AUDIT we can verify the existence of four types of patterns of consumption according to the obtained scores: low probability of excessive alcohol consumption, for quotations equal to or less than 7 points; risk consumer for scores between 8 and 15 points; harmful use at the time of results between 16 and 19 points; and likely dependance on scores of 20 or more (SICAD, 2014). The reliability of the Portuguese version was evaluated with Cronbach alpha = .73 (Fonte & Mota-Cardoso, 2013). In the present study, this scale presented an alpha coefficient of .84.
Resilience
The Resilience Scale – Short Version (Wagnild, 2009) was used. The original version was developed by Wagnild and Young (1993) and aims to identify the degree of individual resilience (personal competence, acceptance of self and acceptance of life), that increases individual adaptation. It was composed of 25 items, organized according to a Likert-type scale of 7 points (the value 1 corresponds to "strongly disagree", the value 4 corresponds to "neutral," and the value 7 corresponds to "I strongly agree" with the statement). The reduced version, with items and the same answering scale, presents good psychometric properties, considering an Alpha of Cronbach of .93, which indicates a high internal consistency and a strong correlation with the original version (r = .97, p = .001). In RS-14, total scores range from 14 to 98, with the highest results indicating greater resilience. This version is adapted to Portuguese with good psychometric properties (Dias et al., 2016). In the present study, this scale had an alpha coefficient of .92.
Data Analysis
The data analysis consisted of three steps. First, with the AMOS 26.0 program, a confirmatory factor analysis (CFA) was used to analyze the proposed measurement model and compare it with another alternative model, following the two-step approach recommended by Anderson and Gerbing (1988). By performing a CFA, we analyzed the extent to which the different variables analyzed are empirically distinguishable (Mathieu and Taylor, 2006). Therefore, control variables were not included in the CFA.
Next, the descriptive statistics (mean and standard deviation) and intercorrelations among the variables in the study were calculated with the SPSS 26.0 program. The third step consisted of testing our hypotheses with the PROCESS macro in SPSS IBM Statistics 26.0 software. The model used for performing the PROCESS macro was Model 4 (Hayes, 2013) which allows up to 10 mediators to operate in parallel. For testing the mediation hypothesis, we used 5,000 bootstrap samples with a 95% bias-corrected bootstrap confidence interval for all indirect effects.
Results
Confirmatory Factor Analyses
A test of the measurement model was conducted to control for common method variance and to establish discriminant validity (Podsakoff et al., 2003). The one-factor model (with all items, of each studied variable, loading into one latent factor) exhibited poor fit to the data [χ2 (270) = 1,765.90, p < .01, Standardized Root Mean Square Residual (SRMR) = .14; CFI = .73; Incremental Fit Index (IFI) = 0.73; Root Mean Square Error of Approximation (RMSEA) = 0.11]. However, the three-factor model, i.e., the theoretical model, obtained an acceptable fit [χ2 (268) = 717.98, p < .01, SRMR = .05; CFI = .92; IFI = 0.92; RMSEA = 0.06], significantly better than the one latent factor model [Δ χ2 (2) = 1,047.92, p < .01]. These analyses revealed that the factor structures of the research variables were consistent with the conceptual model and that the manifest variables loaded, as intended, on the latent variables.
Descriptive Statistics
The average value in psychological violence (M = 0.55, SD = 0.50) indicates more than half the sample was a victim of psychological violence (i.e., 55.2% of the total sample). The average score on the resilience scale (M = 77.24; SD = 14.27) suggests a moderate level of women's resilience. The mean value obtained for alcohol consumption (M = 2.51; SD = 4.94) indicates a low probability of excessive alcohol consumption in the sample. In general, the observed pattern of correlations indicated that psychological violence correlates positively and significantly with alcohol consumption (r = .25, p < .01). Moreover, we found a significant negative relationship between psychological violence and resilience (r = −.15, p < .01), and a significant negative relationship between resilience and alcohol consumption (r = −.21, p < .01).
The analyses with this sample pointed out significant correlations among the studied variables (i.e., psychological violence, resilience, and alcohol consumption) and demographic variables. More precisely, older women seem to present a higher level of resilience [F (5,464) = 3.87, p < .01]. Additionally, single women seem to report suffering higher psychological violence [χ2 (df = 4, n = 464) = 26.10, p < .01], and lower levels of resilience when compared with married women [F (4,463) = 2.55, p < .05]. Furthermore, divorced women seem to be among the participants who engage more in alcohol consumption [F (4,463) = 4.41, p < .01]. Moreover, unemployed women or women without a job were also the ones who presented a higher level of alcohol consumption [F (4,463) = 2.51, p < .01].
Hypothesis Testing
Following the correlation results, it was possible to have a general idea of the pattern of the relationships among all the constructs. By performing the PROCESS macro in SPSS IBM Statistics 26.0 software, it was possible to complete regression analysis and analyze the existence of mediation effects.
Before the mediating testing, we established a model where only the direct relationship between psychological violence to alcohol consumption was included. This model was tested without adding the hypothesized mediating variable (i.e., women's resilience), and a positive and significant relationship was observed (β = .25; p < .01.). Proceeding with the hypotheses testing, a new model was tested with the hypothesized mediating variable (i.e., women's resilience) introduced. As can be seen in Figure 1, regarding the relationship between psychological violence and women's resilience, was found a negative and significant relationship (β = −.30; p < .01). Thus, Hypothesis 1 was supported by the data. Concerning the relationship between women's resilience and alcohol consumption, a negative and significant relationship was also observed (β = −.17; p < .01.), thereby supporting our hypothesis 2.
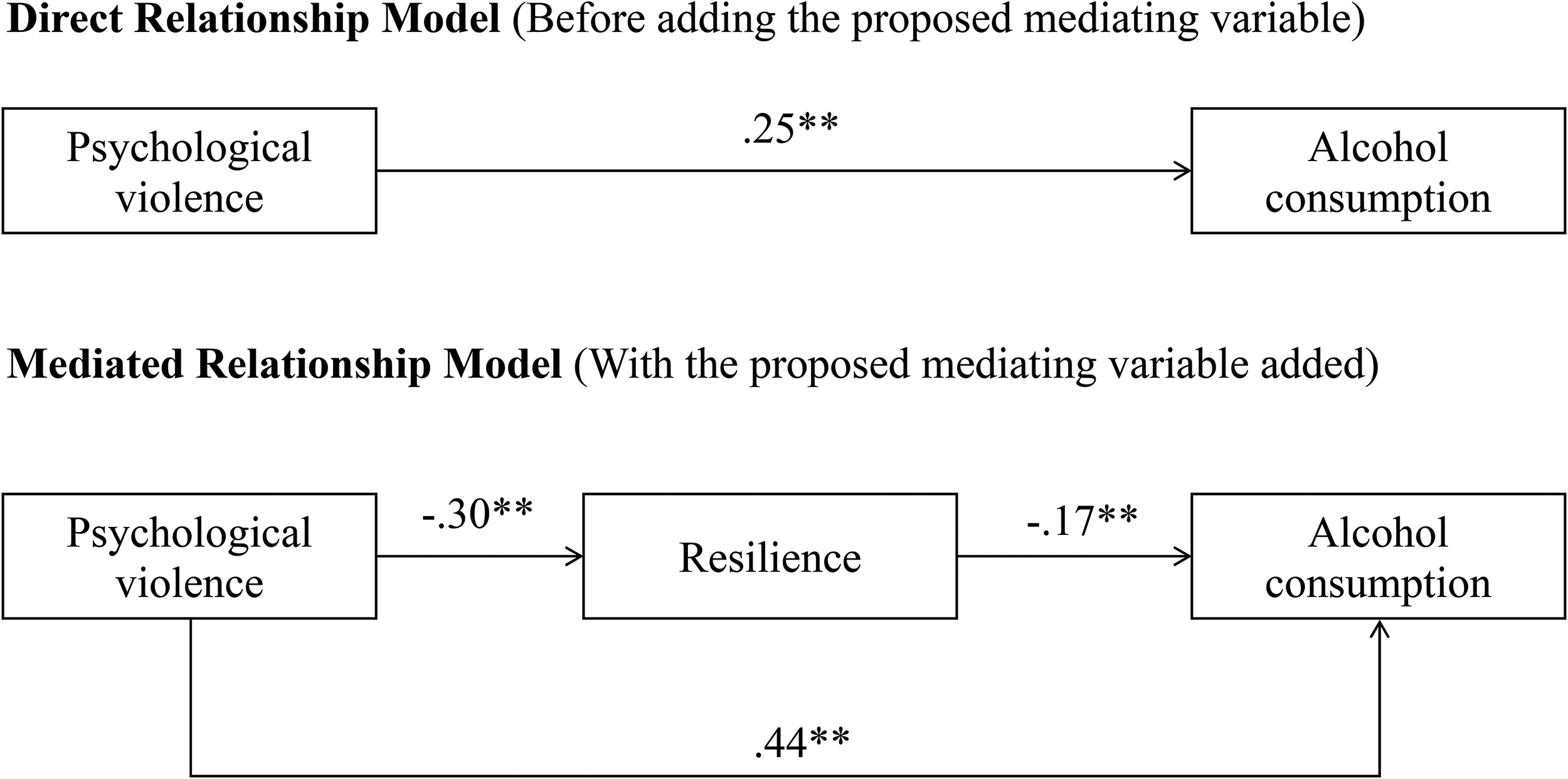
Models with standardized estimates. Note. **p < .01; *p < .05.
Regarding the mediating role of women's resilience in contributing to explaining the relationship between psychological violence and alcohol consumption the indirect effect from psychological violence and alcohol consumption through women's resilience was found as being significant (Estimate = 0.26, 95% CI [0.05, 0.58]), confirming Hypothesis 3.
Discussion
The main purpose of the present research was to explore the relationship between psychological violence within a partner relationship and alcohol consumption including the analysis of the mediating role of resilience with a sample of Portuguese women. By testing these relationships, this empirical study contributed to the literature by giving new insights regarding the mediating role of resilience in the relationship between psychological violence and alcohol consumption.
In line with what was suggested by previous studies (e.g., Herreira Trigueiro et al., 2014; Howell et al., 2018; Tsirigotis & Łuczak, 2018), we observed a lower level of resilience in the sample and a negative relationship between psychological violence and resilience. A higher level of psychological violence seems to harm resilience. Previous research demonstrates how intimate partner violence tends to be related to exposure to violence in the original family but also in romantic relationships (Kaufman-Parks et al., 2017). Although some authors argue individuals’ resilience is somewhat innate and dependent upon individual characteristics such as self-esteem, intelligence, and independence (Gopal & Nunlall, 2017), traumatic or stressful situations, like being subject to psychological violence, may weaken women's resilience. Thus, the perpetration of psychological violence, which is recurrently a continuous phenomenon, under a situation of abuse of power and control by abusers (Porrúa-García et al., 2016), contributes to decreasing an important women's psychological resource (Howell et al., 2018; Tsirigotis & Łuczak, 2018), and this negative link must be a concern to the practitioners. More precisely, as noted by Hobfoll et al. (2015), “resource losses increase the likelihood of additional loss” (pp. 178), and these losses lead to a situation of loss spiral, which means an increasingly fragile situation for women victims of psychological violence. As such, it is important to build up resilience ability jointly with women victims of psychological violence in the psychotherapeutic setting (Reynolds, 2019). Particularly, cultural characteristics regarding “familism,” community pressure and shame and acculturation, that has a strong presence in our context, contribute also for the explanation of the phenomenon (Graca, 2018), demanding further research to a deeper explanation of the role of these social and structural factors.
Concerning the relationship between resilience and alcohol consumption, the current research also demonstrated the existence of a negative and significant association between the two variables, which is in line with the findings of the study of Kennedy et al. (2019) and Long et al. (2017). Higher levels of resilience seem to be related to lower alcohol use, which is well-known as a health problem with negative repercussions of alcohol consumption on individuals’ mental health (e.g., Griswold et al., 2018; Shield et al., 2020). Having in mind the high prevalence of alcohol use and abuse in our context (World Health Organization, 2018), promoting individuals’ resilience can be a very useful tool to prevent women from alcohol abuse. As such, the clinical practice could guide the therapy building on this finding and contribute to promoting and developing women's resilience (Anderson et al., 2012; Reynolds, 2019). This could be done in several ways. Apart from measures to support and assist victims, particularly in their material resources (Saunders, 2020), psychotherapeutic support must be provided.
Upon leaving an abusive relationship, psychotherapy could promote and develop key facets, or tools, of resilience, with social and interpersonal support, to foster active coping skills and enhance engagement with life through the involvement in pleasurable social and physical activities (Reynolds, 2019). Additionally, psychotherapy should contribute to women's increase in their sense of control of their lives and cognitive reframing (Anderson et al., 2012; Reynolds, 2019). Professionals should consider women's role in challenging and overcome of trauma and support the evaluation and change in social networks allowing the disengagement of negative relationships and strengthening of more positive ones (Anderson et al., 2012). Not to deny the violent experience but allow women to understand the dynamics of abusive relationships the “why” and “what” happened, assisting them to understand how resilience can emerge from traumatic situations.
Finally, in the current research, resilience was found as being a partial mediator of the relationship between psychological violence and alcohol consumption. Recent studies are exploring the role of resilience as a buffer of stressful or traumatic events on alcohol use (Cusack et al., 2021; Sheerin et al., 2021). In these studies, no interaction effects were found. However, in this more specific scope of intimate partner relationship, partial mediation was found. Probably the relationship between psychological violence and alcohol consumption is explained due to other intervenient variables, besides resilience. Other protective or cultural factors should be explored for a deeper understanding of the phenomenon.
According to the EIGE report (2016), in Portugal, violence against women continues to be underreported and stigmatized. One possible explanation for this underreporting could be due to a lower level of trust the authorities would do something (Gama et al., 2020). Moreover, limited access to or a lack of awareness of how to access support services may contribute to underreported cases (EIGE, 2020). In addition, the study by Gama et al. (2020) showed that most victims do not seek help since they consider it unnecessary, they believe help would not change anything and they feel embarrassed about what happened. Moreover, it should be noted, Portugal rates 6.6 points below the EU's score concerning the Gender Equality Index. In Portugal, like in other European countries, women continue to earn less than men, and they are much more likely than men to do housework every day for at least 1 h (Gender Equality Index [GEI], 2020). These social inequalities can also contribute to a less fair and increased violent society (Jordão, 2021). Given the lack of quantitative research on this issue, this can be considered a positive contribution to pursue. Future studies should continue analyzing the mediating role of resilience in the relationship between psychological violence and alcohol consumption but adding some other constructs as mediators like contextual variables, such as perceived social support or individual characteristics like self-blame (Sáez et al., 2020), spirituality or history of violence (Howell et al., 2018) or other contextual variables as the trust in institutions or social inequality (Gama et al., 2020; Jordão, 2021).
Study Limitations, Recommendations for Future Studies and Implications
Although this study has several strengths some limitations should be noted. First, it is important to underscore that the sample evaluated in this study comprised women from only one country (Portugal), which may constrain the generalization of these results. Furthermore, most of the participants had a university degree, were single, and were employed. In line with previous studies (e.g., Goroshit & Eshel, 2013; Lee et al., 2013; Swendsen et al., 2009), the current findings demonstrated significant relationships among demographic variables, such as educational level, marital status, age, and professional situation, and the studied variables – i.e., psychological violence, resilience, and alcohol consumption. Thus, future studies could replicate this study with women who possess a lower educational level, a different marital status, are unemployed, and are from other countries to broaden the findings of the present study. Additionally, the current study has a cross-sectional design and causality cannot be established among the studied variables. It is therefore important that future research examine these relationships over time. Finally, future work should consider other methods of measurement for the constructs assessed here beyond self-report; for example, blood alcohol content test or breathalyzer alcohol test. Replicating these findings with other methods of measurement may be useful in validating and better elucidating the possible contribution of past and recent psychological violence on resilience and alcohol consumption. However, to minimize this limitation, we followed the methodological recommendations of Podsakoff et al. (2003); namely, by conducting CFA, guaranteeing the anonymity of the answers, and indicating that there were no right or wrong answers.
Nevertheless, findings contribute to the literature by demonstrating initial support for the importance of reliance in understanding the relationship between psychological violence and alcohol consumption and point to several areas for future research. More precisely, future longitudinal studies could test theoretically driven hypotheses related to the mediating role of resilience in explaining the relationship between psychological violence and alcohol consumption over time. Additionally, future studies might explore the relative importance of resilience in contributing to breaking the negative “chain” between other forms of intimate partner violence, such as economic and physical violence, and alcohol consumption. Finally, results should be replicated among a larger more heterogeneous sample, from other non-European countries.
In terms of implications, this study might support interesting clinical and health interventions. Considering that resilience can be promoted (Anderson et al., 2012; Masten et al., 2021), the results of this study support the need to promote adequate evaluation of risk and protective factors but particularly the role of resilience. Also, it highlights the role of resilience interventions to prevent alcohol use and abuse, but also to promote the mental health of victims within a partner relationship. The development of appropriate interventions and evaluation of their efficacy might have important implications for policy and practice. For instance, Sani and Pereira (2020) conducted semistructured interviews with Portuguese women victims of intimate partner violence. The findings of this study showed professionals, through their technics, may contribute to increasing victims’ resilience by working based on the Resilience Portfolio Model (Grych et al., 2015). More precisely, over time, through the therapeutic sessions, professionals may help the victim to identify external strengths (e.g., family support, community support), and strengthen the victim's meaning-making through the development of new understandings of their experience of victimization. These technics, in turn, may enhance intrinsic forces, such as self-regulation to overcome obstacles. A meta-analysis and systematic review of resilience-promoting interventions conducted by Liu et al. (2022) also showed the effectiveness of resilience interventions in promoting overall coping, psychological well-being, and searching for external resources.
Footnotes
Data Accessibility
Data is available by request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
The study was approved by the Board of the Research Center and was performed following the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fundação para a Ciência e a Tecnologia (grant number UID/FIL/00683/2022).