
Abstract
The effects of suicide are both widespread and long-lasting in the lives of those closest to the deceased. According to the World Health Organization (WHO), suicide is the third leading cause of death in adolescents. Some research has shown that families who lose someone to suicide are at a higher risk of complicated grief compared to those bereaving from other types of losses. These risks may be emphasized given the socio-cultural context surrounding suicide that may problematize the grieving process. In this review, we analyzed 58 qualitative studies describing the experiences of family who lost someone to suicide. We discuss how negative social interactions due to cultural views towards suicide impacted their grieving process. We provide an integrative interpretation of the experiences of family who lost someone to suicide across the following themes: social withdrawal, family communication approaches, role change, cultural attitudes, the role of professional support, interactions with health care providers, and interactions with religious institutions. We examine these findings using the Assumptive World Theory which proposes that humans seek preservation of their reality by using their perceptions of the past to establish expectations for the future. We find that suicide loss is an experience that challenges people's assumptive worlds; suicide loss can be an unexpected trauma that can have a “shock effect” on the assumptive worlds of the bereaved. The assumptive worlds of relatives grieving suicide loss face unique challenges compared to other forms of bereavement because of ambiguity in social norms surrounding suicide that influence interactions.
Introduction
The effects of suicide are both widespread and long-lasting in the lives of those closest to the deceased. Results from a study conducted by Cerel et al. (2019) revealed that for every suicide death in the United States, 135 people were exposed to that suicide. According to the World Health Organization (WHO), suicide is the third leading cause of death in adolescents. The WHO's description of suicide as a “public health priority” is a reminder of the community-wide impact of suicide, and that it occurs across regions with distinct cultures. Avrami (2005) identifies suicide as a phenomenon which takes place in its social and cultural context. The social interactions of suicide-bereaved individuals are also strongly related to the socio-cultural context of the suicide.
Suicide is defined as “a fatal self-injurious act with some evidence of intent to die” (Turecki & Brent, 2016). In this review, suicide survivors or participants are defined as friends and family members who have experienced the death of a loved one by suicide. Alongside the significant global rates of suicide, the uniqueness of bereavement from suicide compared to other causes of death is notable. Some research has shown that suicide survivors are at a higher risk of complicated grief opposed to those bereaving from other deaths. Complicated grief involves strong desires of reunion with the deceased, behaviours to feel close to the deceased, suicidal ideation, and feeling estranged from others (Tal Young et al., 2012). At the same time, interpersonal relationships of suicide survivors can have a significant impact on the grief process. Suicide bereavement is a social phenomenon where relationship expectations and assumptions evolve with time.
Although the current literature recognizes the existence of complicated grief in suicide survivors, there is a need to contextualize the role of various social interactions in the grief process in familial spheres, institutions, and on a societal level. Difficulties in social interactions can also be a result of suicide stigmatization, self-stigmatization, and various negative emotions such as shame and guilt (Ross et al., 2021). This research aims to identify recurrent themes and reactions of suicide survivors in their varying social interactions following the suicide and the impact of these social interactions on the grief process.
Materials and Methods
Approach
We conducted a qualitative evidence synthesis (QES) using the qualitative meta-synthesis approach (Sandelowski & Barroso, 2003). This approach allowed for the integration of findings from multiple qualitative studies to formulate a comprehensive interpretation of the subject matter whilst ensuring adequate representation of findings from each individual study (Sandelowski & Barroso, 2003). With this methodology, we were able to develop a more concrete understanding of the topic over a wider range of cultural and social contexts than would be examined in any one primary study (Thomas & Harden, 2008). Furthermore, our interpretations are representative of a broader range of dimensions and concepts because they are integrative of multiple primary studies.
Database Searching and Screening
We developed and conducted a database search strategy for qualitative studies on grief and bereavement across PsychINFO, MEDLINE, Embase, CINAHL, and Web of Science. We used exp/ Grief and exp/ Bereavement among others as the primary keywords and subject headings. From this general search, we conducted title and abstract screening on articles pertaining to grief from the suicide of a loved-one. To ensure we found all studies on the topic, we also conducted hand searching of reference lists as well as searching journals that published the included studies for relevant articles.
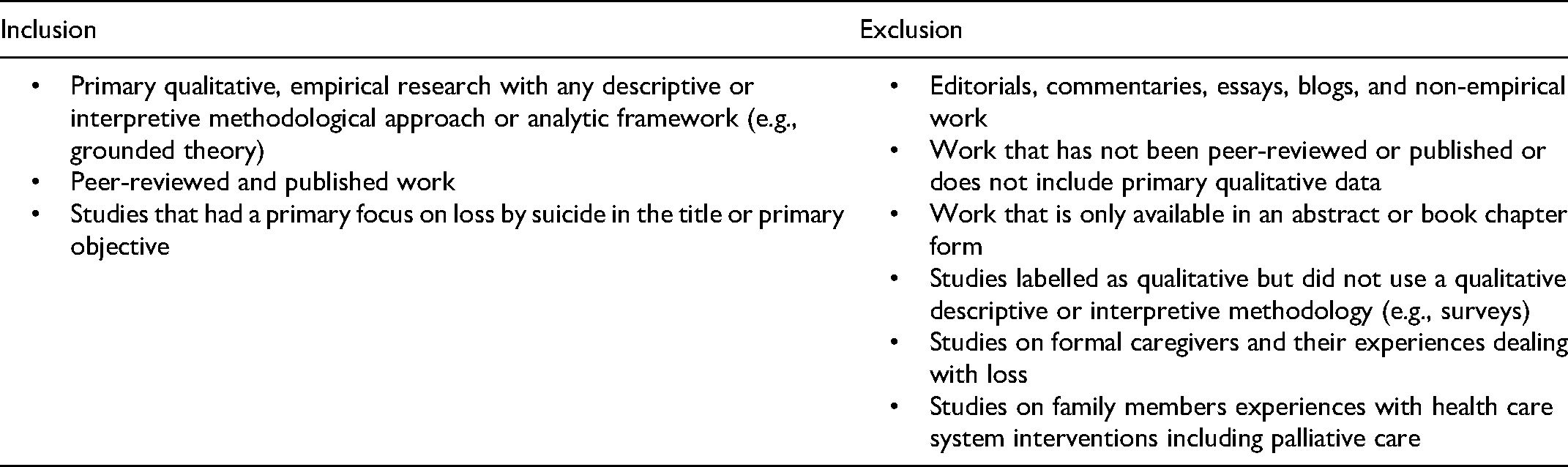
We were interested in studies that had a primary focus on loss by suicide. We included primary, qualitative or mixed-methods, and empirical studies with any descriptive or interpretive methodological approach or analytic framework. We excluded any non-peer-reviewed studies such as editorials, commentaries, essays, blogs, and non-empirical work and studies that did not include primary qualitative data. We also excluded studies that were only available in abstract or book chapter form. We excluded studies on formal caregivers and their experiences with loss as well as studies on family members’ experiences with health care system interventions including palliative care. Our full list of eligibility criteria is shown in Table 1.
Eligibility Criteria
Data Extraction
We developed a standard data extraction form to document the descriptive features of included studies and their respective study populations. We extracted the following details: author, year of publication, title of study, research objectives, country of publication, qualitative methodology or analytic approach, data collection method(s), number of participants, relationship to the deceased, proportion of male participants, age range of participants, and overall findings or themes in each study. We calculated descriptive statistics to summarize the study characteristics.
Data Analysis
We conducted multiple rounds of initial and focused coding to capture recurring themes and reactions. We employed a two-staged coding process that was informed by thematic analysis and constant comparison (Aronson, 1995; Boeije, 2002). In the first stage, we conducted initial coding on the first four included studies to construct a preliminary schema with the concepts captured from these studies. This schema was modified in the second round of initial coding with the next four articles. The themes outlined in the schema were then utilized to code for the remaining articles in the form of analytic memos. We refined and expanded the schema continuously to best encapsulate the recurring themes and reactions of participants. In each round of coding, the researchers noted recurring emotions and experiences as well as participant quotes. Following the completion of this stage, the researchers reviewed the analytic memos and constructed narrative summaries of each theme. One author then integrated the narrative summaries on personal reactions, while another author integrated the summaries on social reactions. Because of the depth of analysis and the quality of the data we found, this article focuses on social reactions only.
Results
Search Results
We screened the titles and abstracts of 8398 studies of which we conducted full-text screening on 92 studies. We excluded 34 studies because they did not fulfill one or more eligibility criterion. We analyzed 58 studies in this review. Figure 1 shows the screening and selection process.
Social Interactions
Death by suicide marked various initial reactions, emotions, and changes in the lives of the bereaved. Prominent grief emotions and reactions described included loneliness (Avrami, 2005; Barnes, 2006; Chapple et al., 2015; Demi & Howell, 1991; Gamondi et al., 2015; Schotanus-Dijkstra et al., 2014), shame (Adams et al., 2019; Avrami, 2005; Azorina et al., 2019; Barnes, 2006; Biddle, 2003; Chapple et al., 2015; Maple et al., 2010; McKinnon & Chonody, 2014; Nic an Fhailí et al., 2016; Peters et al., 2016; Wood et al., 2012) and internal and external blame (Chapple et al., 2012; Demi & Howell, 1991; Dransart, 2017; Dutra et al., 2018; Fielden, 2003; Hagström, 2019; Kasahara-Kiritani et al., 2017; Lubens & Silver, 2019; McKinnon & Chonody, 2014; Van Dongen, 1991; Wood et al., 2012). In this section, we discuss the various social interactions that participants had following the loss of their loved-one to suicide that contributed to these grief emotions and reactions.
Social Withdrawal: Fear of Loss and Abandonment
A total of thirteen studies mentioned that the bereaved adopted social withdrawal because of the fear of loss and abandonment (Azorina et al., 2019; Bartik et al., 2013; Begley & Quayle, 2007; Dransart, 2017; Fielden, 2003; Gamondi et al., 2015; Kasahara-Kiritani et al., 2017; Nic an Fhailí et al., 2016; Ross et al., 2018; Van Dongen, 1990; Van Dongen, 1991; Van Dongen, 1993). Social withdrawal was defined by participants in included studies as “avoiding contact with others” and “taking a break from family” (Fielden, 2003, p. 78). Such a withdrawal was preceded by a sense of decreased patience and discomfort with family and friends; this kind of emotional strain was intimately tied to the suicide that contributed to a fear of “break[ing] down” in front of others (Gamondi et al., 2015; Ross et al., 2018; Van Dongen, 1990; Van Dongen, 1991). For example, one participant stated: “I told someone about my brother's assisted suicide and he wanted to know more and more. So I said: “‘Look, one day or another I’ll tell you, but not now.’ Two years have passed now and I’m not ready to face what happened. Because it means…living it all again” (Gamondi et al., 2015, p. 5).
Such emotional strain and lack of energy pushed certain participants to social withdrawal, which, in turn, may have the unintended outcome of reducing opportunities for social support. Attributes of social withdrawal included insecurity, rejection, low self-esteem, difficulty making new friends, and a lack of trust in social relationships (Azorina et al., 2019; Bartik et al., 2013; Begley & Quayle, 2007). The bereaved feared losing their close friends and significant others by sharing their grief and emotional burdens with them (Azorina et al., 2019; Bartik et al., 2013). One study found that when these obstacles were overcome, re-engagement in social activities helped to re-establish feelings of connectedness and trust (Kasahara-Kiritani et al., 2017). Despite withdrawing, the bereaved felt a longing for connection (Azorina et al., 2019).
Family Communication Approaches
Alongside the fear of loss and abandonment, fears of judgement and embarrassment prevented participants from freely expressing their grief in social situations (Fielden, 2003; Kasahara-Kiritani et al., 2017; Kennedy et al., 2021; Pitman et al., 2018c). Particularly with family members, participants avoided sharing emotions to prevent burdening their family (Adams et al., 2019; Begley & Quayle, 2007; Kawashima & Kawano, 2017; Tzeng et al., 2010; Van Dongen, 1990; Van Dongen, 1993). At times, silence was misinterpreted by family as a sign that participants were either successfully coping or insensitive to the situation. A fear of being misperceived led the participants to withdraw socially as they never found the “right time” to resume social activities (Van Dongen, 1993). With this withdrawal and avoidance of sharing grief openly with family members, the bereaved felt that they were left to process the suicide alone and their grief was compounded with both the loss and a lack of social support (Adams et al., 2019; Azorina et al., 2019).
Six studies addressed conflicting coping processes between family members that led to tension and strained relationships (Adams et al., 2019; Begley & Quayle, 2007; Dransart, 2017; Kasahara-Kiritani et al., 2017; Kawashima & Kawano, 2017; Van Dongen, 1993). Although some parents applied protective silence to prevent further distress in bereaved children, a conflicting grief reaction was noted in one study that found mature adults were typically “dialoguers,” openly sharing their grief with family members, whereas younger participants were “mood changers”, disguising their emotions (Kasahara-Kiritani et al., 2017). This impact of opposing coping processes on familial relationships was compounded when family members experienced different stages of grief at different times: “I found it very hard myself, I would listen to the girls being very bitter at times, their father saying nothing, and I felt like screaming…” (Begley & Quayle, 2007, p. 29).
Role Change
Eight studies noted a change in roles within the family structure following the suicide (Adams et al., 2019; Clark & Goldney, 1995; Demi & Howell, 1991; Dransart, 2017; Dutra et al., 2018; Dyregrov, 2009a, 2009b; Pitman et al., 2018a; Van Dongen, 1991). Participants felt forced to assume caretaking roles or take on the responsibilities of the deceased. The assumption of caretaking roles was preceded by the loss of emotional support. For this reason, some participants expressed how they had to sacrifice time, energy, and their occupations to adopt new roles in the family (Pitman et al., 2018a).
The suicide led to disturbed family dynamics with parents of a deceased child facing marital conflict and mutual blaming behaviours (Van Dongen, 1991). If the deceased were the primary income generators of the household, families experienced financial challenges that led to family stress. Moving away from the family house, city, or job was deemed helpful for recovery in three studies (Dutra et al., 2018; Fielden, 2003; Kasahara-Kiritani et al., 2017). Grandparents or siblings were expected to fill in for parenting roles but were either too young or too old to fulfill this role well (Demi & Howell, 1991). Disturbed family dynamics generated a need for a reorganization of the family and parenting styles (Dutra et al., 2018; Fielden, 2003). For example, some parents adopted safety measures such as protective silence. In protecting bereaved children, one study found that following the suicide, some parents became more lenient with other children. These parents adopted a laissez-faire parenting style with the bereaved children due to a fear of repeating suicide in their family: “After that I was pathetically weak, too frightened to say no to my other children because I was frightened that if I said or did anything that they didn’t want that they’d be next (to complete suicide). I didn’t want to upset them” (Fielden, 2003, p. 77).
Cultural attitudes, values, and expectations
A recurring theme among the studies was participants’ effort to conceal the cause of death due to societal stigma towards suicide (Clark & Goldney, 1995; Demi & Howell, 1991; Fielden, 2003; Gamondi et al., 2015; Kasahara-Kiritani et al., 2017). The bereaved found it challenging to reveal the cause of death to others and felt paranoia and shame from being at the centre of community gossip. At the same time, participants felt rejected by the deceased as they viewed the suicide as a voluntary, conscious choice to leave behind the bereaved. Blame by others was seen as a “second rejection” in addition to the rejection by the deceased, and this led participants to fear starting new relationships (Clark & Goldney, 1995). The second rejection consisted of subtle and overt avoidance. In contrast to blaming the bereaved, participants of one study described how non-family more often stressed the innocence of participants and vilified the deceased by using words like “chose” to commit suicide (Hagström, 2019).
Participants noted having to stay vigilant during their conversations with others and being careful in expressing negative emotions. Participants also found it acceptable to share their grief with non-family shortly after the death, but public expressions of grief were discouraged after some period of time because it was regarded as a private family matter (Adams et al., 2019; Azorina et al., 2019; Begley & Quayle, 2007; Chapple et al., 2015; Peters et al., 2016). Some bereaved also noted that non-family would “reject” them in subtle ways such as avoiding social interactions with them. They described friends as seemingly avoiding them at work, church, or the grocery store (Adams et al., 2019; Avrami, 2005; Azorina et al., 2019; Chapple et al., 2015; Dransart, 2017; Kalischuk & Hayes, 2004; Van Dongen, 1993). Participants indicated that this kind of social rejection was evident through implicit behaviours (i.e., changes in routine interactions and passive avoidance in public locations), rather than through direct behaviour.
The cultural stigma surrounding suicide was found to inhibit the bereavement process for participants by preventing them from sharing their grief with others (Bottomley et al., 2019; Kasahara-Kiritani et al., 2017). One study conducted in China found that for other types of deaths, family members held the funeral in a large-scale venue, invited relatives to attend, brought the dead person into the familial ancestry, and had offspring sometimes worship the deceased. However, suicide deaths were seen as unlucky because it was contrary to “natural laws.” As a result, the funeral was kept low-profile, the deceased was ostracized by the family, and the event was kept hidden from distant relatives, ancestors, and offspring (Tzeng et al., 2010).
Silence was noted within the family structure as a protective strategy; however, six studies also noted the use of silence to conceal the cause of death to avoid cultural stigma towards suicide (Avrami, 2005; Azorina et al., 2019; Barnes, 2006; Bottomley et al., 2019; Kasahara-Kiritani et al., 2017; Kawashima & Kawano, 2017; Tzeng et al., 2010). In studies from Israel and Japan, protective silence was established with the understanding that other forms of death such as disease or death in a war were “better” than death by suicide (Avrami, 2005; Kawashima & Kawano, 2017). The memory of the deceased was considered as something to be hidden because of the cause of the death: “I thought—if he had to die, why not in a war, something heroic, and not something to be ashamed of…” (Avrami, 2005, p. 73).
The Role of Professional Support
Eleven studies discussed reactions to professional support and the role played by counsellors and peer groups in the grief process (Adams et al., 2019; Barnes, 2006; Bartik et al., 2013; Begley & Quayle, 2007; Chapple & Ziebland, 2011; Clark & Goldney, 1995; Dyregrov, 2009b; Dyregrov et al., 2011; Kasahara-Kiritani et al., 2017; McKinnon & Chonody, 2014; Ross et al., 2018). Due to the fear of burdening family members, protective silence was employed in the family sphere. On the other hand, one study posed that recourse to professional support may be due to the bereaved not feeling as though they needed to protect trained professionals from their grief reactions. Participants were able to share their grief reactions with professionals without having them overreact to their emotions or suicidal ideation negatively, which often happened with family (Adams et al., 2019). The majority of young participants in one study recognized the need to request professional support post-suicide and wished that their close friends and family encouraged it (Dyregrov, 2009b). Participants found it difficult to access support services by themselves, “I think you don’t have the energy when you’re needing the help the most, you don’t have the energy to seek it out…” (McKinnon & Chonody, 2014, p. 238). Participants generally found counsellors to be helpful in encouraging introspection and leading the discussion from answering ‘why’ to more insightful questions, preparing them to live with the uncertainty that they may never find an adequate answer to why the suicide occurred (Clark & Goldney, 1995; Ross et al., 2018). Professional support was also helpful in shifting the participant's locus of control from feelings of guilt to an external locus of control in identifying the suicide as a result of actions outside their control (Kasahara-Kiritani et al., 2017).
“I became mentally sick and that's how I got to know the medical service personnel and peer supporters … They helped me and, gradually, I could speak about my brother's death. Eventually, I admitted that I had been afraid to talk about the matter for a long time; I think … If I had missed the chance to meet them, my life would have been more difficult. Moreover … I had both rational thoughts and strong feelings of guilt that I had killed my brother. The inseparable mixture of thoughts had tormented me” (Kasahara-Kiritani et al., 2017, p. 451).
Professional support was not always seen in a positive light. Therapists were sometimes seen to be unsympathetic and too distant from the experience, following a “textbook” approach by speaking abstractly about suicide (Chapple & Ziebland, 2011; McKinnon & Chonody, 2014). In some instances, participants shared how psychologists lacked empathy, understanding, did not ask individualized questions, and were passive in their questioning. Participants did not understand the benefit of telling “their entire life story” and found that the psychologists they visited overemphasized the past more than the issues that were bothering them (Dyregrov, 2009b). Participants found that therapy felt patronizing due to the therapist's lack of personal experience with the suicide grief process. In contrast, sharing grief with those who have experienced similar circumstances was found to be helpful in grief recovery, survival techniques, and viewing their guilt objectively (Clark & Goldney, 1995). Some participants in one study believed that suicide support should be exclusive to those who have had lived experience of suicide, as those who did not have a personal experience of suicide could not fully appreciate its overwhelming impact on a person's life (Begley & Quayle, 2007). In this way, some peer support groups were effective in ensuring that individuals felt supported. However, certain support groups had the opposite effect; participants felt it was difficult to listen to other people's stories, the group did not provide the healing they were looking for, and there was insufficient focus on recovery (Kasahara-Kiritani et al., 2017; McKinnon & Chonody, 2014).
Interactions With Health Care Providers
Four studies included interactions of the bereaved with health care providers (Adams et al., 2019; Leavey et al., 2017; Peters et al., 2013; Ross et al., 2018). Participants were disappointed with health services and professionals, finding them to be unhelpful, since they were reluctant to assist participants in order to maintain the deceased person's privacy (Peters et al., 2013). This was seen as an immense struggle for the family of the deceased as they felt more information about the particular situation prior to the suicide would have been helpful in addressing the needs of the deceased in a timely manner. The bereaved were also generally frustrated with how health care providers treated the deceased prior to the suicide and felt more could have been done in preventing the suicide (Leavey et al., 2017; Ross et al., 2018).
“I don’t think they did the right thing for her. They were treating her and checking her out of hospital five days later into the same environment where she came from. Is this the right way to treat these sorts of people? I suppose I’ll always question why the medical system had to let her down. I’m looking for somebody to blame, somebody's ass to kick. How did this happen? What could you do to prevent it?” (Ross et al., 2018, pp. 3–4)
Blame was assigned to health care providers for these reasons. Additionally, some participants found that first responders lacked respect for family members at the death scene because they denied siblings access to the deceased (Adams et al., 2019).
Interactions With Religious Institutions
Seven studies discussed stigma surrounding suicide perpetuated within religious institutions (Barnes, 2006; Demi & Howell, 1991; Dransart, 2017; Dutra et al., 2018; Kalischuk & Hayes, 2004; Ross et al., 2018). One study found an interplay of cultural and religious stigma in Black churches that did not discuss suicide because it was a religious and cultural taboo (Barnes, 2006). The current and previous attitudes toward suicide in churches further stigmatized participants (Clark & Goldney, 1995). Participants generally found this stigma to be implicit. Since there was no outright ostracization of those coping with the loss of a loved one from suicide, participants found it difficult to navigate social interactions during religious activities.
“We weren’t outcasts or anything, but he was in the choir and I remember I heard some people at church saying that he was in hell now because of what he did. Some people would say something like, ‘Oh, I could just kill myself,’ and then they’d look at me and draw back” (Demi & Howell, 1991, p. 352).
Discussion
Review of Findings
This qualitative evidence synthesis analyzed 58 studies to examine the social interactions of individuals following the suicide of a loved one. Participants detailed their interactions with family members, friends, religious and cultural institutions, and health care providers. Frequently noted by survivors were changes in expectations and assumptions of those around them such as changes in assumed family roles, expectations of the length and type of coping in the grief process and changing perceptions of the deceased as a result of societal stigma towards suicide. In the following sections, we link our qualitative findings to the broader literature on bereavement and the Assumptive World Theory.
The Assumptive World Theory
The Assumptive World Theory, conceptualized by Parkes and Janoff-Bulman, describes the assumptive world as constituting of “[…] assumptions or beliefs that ground, secure, or orient people, that give a sense of reality, meaning, or purpose to life” (Beder, 2005). This theory emphasizes the human yearning for predictability and preservation of human reality from perceptions of the past to expectations for the future. These perceptions and expectations are subject to changes in the life-space (environmental, biological, social, and psychological influences that constitute one's unique reality). Janoff-Bulman (1992) identifies the following three crucial assumptions for shaping one's assumptive world:
The world is benevolent The world is meaningful The self is worthy
The belief that the world is benevolent refers to the perception that the world is a good place, that others are kind and well-intentioned, and that events typically confer positive outcomes. A meaningful world is a belief in the cause-and-effect relationship between events and outcomes; individuals search for meaning in events and their causes continuously. The understanding that the self is worthy is a perception of inherent goodness, capability, and morality of self. According to this theory, a loss of one's positive worldly and personal assumptions, one's assumptive world, involves a loss of beliefs about the goodness and meaningfulness of the world as well as one's self-worth. This loss then requires the bereaved to modify or revise their assumptive world. This includes integrating traumatic information into their modified assumptive world which requires an expansion of fundamental world assumptions and a greater awareness of vulnerability (Kauffman, 2002). The task of modifying one's assumptive world involves considering factors that can and cannot be carried from the previous assumptive world into the modified assumptive world. Matthews and Marwit (2004) explain how grieving becomes more complex when there is more reconstruction and remodification required of the bereaved depending on the circumstances of the loss.
Janoff-Bulman (1989) noted three principles for the “distribution of outcomes” (i.e., the balance of positive and negative events that take place in one's life) that people in Western society generally adopt: 1) the “just world theory” (Lerner, 1980), which assumes that the distribution of outcomes reflects personal deservingness or moral character; 2) personal behaviour, in that people can determine and influence outcomes with their actions; and 3) randomness, an understanding that one's own moral character nor personal behaviour can justly reflect the distribution of outcomes. It is found that generally speaking, trauma victims such as people who have lost a parent or sibling, view themselves as less worthy of positive outcomes, are more likely to adopt the third principle of randomness, and as a result, more likely to hold negative views of the impersonal world and self-worth (Janoff-Bulman, 1989; Lilly et al., 2011; Mikkelsen & Einarsen, 2002).
Unexpected Trauma and the Assumptive World
Trauma can severely impact one's assumptive world and force oneself to recreate assumptions to better reflect a new reality. For example, Rando (1993) articulates the “unnaturalness” of a child's death in parents’ worldview; the death of a child challenges parents to modify their assumptions and expectations that they will die before their children. Grieving parents, in revising their assumptive world, must reflect on what constants from their assumptive world can be brought into the modified world. Reconstructing an accurate world view can complicate the grieving process. A study examining the assumptive worldviews of parents bereaved by murder found that the consequence of murder-bereaved parents in attempting to preserve their assumptions of the predictability of the world was guilt for the murder (Matthews & Marwit, 2004). This was because these parents felt that they had not done enough to avoid the event and by perceiving the event as preventable and avoidable, the event can no longer be seen as random. According to Rando (1993), events that can be construed as random acts of nature are alarming because they imply that one cannot fully control the events that take place in one's life, and therefore, one's safety is compromised. Maintaining the belief that events are not the result of random chance aids in maintaining a perception that one has control of their life and the world. Shifting this locus of control from self may be necessary for the grief process because otherwise grief may persist with intense guilt and self-blame. The study also found that illness-bereaved parents had time to anticipate the impending death of their child which allowed them the opportunity to incorporate this reality into their assumptive world. These parents were better able to adapt (Parkes, 1975), experienced personal growth, and maintained their self-worth (Schaefer & Moos, 2001) compared to cases of unexpected death, accident, and homicide. In a study exploring maternal grief, mothers described the opportunity to anticipate and prepare for their child's death as facilitating adaptation (Gerrish et al., 2014). A recently published review found that anticipatory grief provided the opportunity to process the impending loss, which reduced the physical and emotional outcomes post-loss (Majid & Akande, 2021).
All unexpected deaths may have a “shock effect” on the assumptive world of the mourner but we argue that suicide deaths, in particular, have a unique effect on the bereaved partly due to the immense ambiguity in social norms and interactions with others following the suicide. Jordan (2017) noted that this ambiguity contributes to avoidance behaviour and ultimately isolation of the bereaved in their social networks. The isolation resulting from avoidance may prompt greater rumination and guilt in suicide survivors than those that have lost a loved one to an accident, expected natural death, or unexpected natural death (Camacho et al., 2018). This rumination and feelings of guilt may also be associated with the survivors’ breakdown of their assumptive world. The suicide death of a loved one is a unique trauma that challenges one's assumptions of self, the deceased, and those around them. According to our findings, assumptions of caretaking roles in the family sphere were tested as survivors were forced to take on new roles that were filled by the deceased (Clark & Goldney, 1995). Participants’ perception of the deceased was also being revised with the integration of the death and can be significantly influenced by the societal stigma of suicide. Hearing suicide described as a “choice” can leave the survivors feeling rejected by the deceased, challenging their own beliefs of self-worth (Hagström, 2019). On the other hand, survivors who felt guilty for the death of their loved one maintain their assumption that they are in control of their situation (Bartik et al., 2013; Matthews & Marwit, 2004).
Our findings on interactions of suicide-bereaved with health care providers prior to the death revealed frustration and disappointment with these institutions which can be attributed to the loss of one's assumptive world. As Jordan and McIntosh (2011) point out, assumptive worldviews of suicide survivors whose loved one was receiving professional care in health care institutions may be threatened in a unique way. This is because of established trust in health care institutions and caregivers and often unrealistic expectations of the abilities of health care professionals. These survivors may have held unrealistic perceptions of these professionals as having the knowledge, skill, and expertise to “save” someone experiencing suicidal ideation. Throughout their lifetime, survivors may have developed a sense of trust and confidence in the ability of health care professionals and the suicide of their loved one can challenge that trust. The loss of trust in health care institutions can compound existing grief in these survivors, and it is vital for survivors to reframe their assumptive world in this professional space as well. Based on our findings, suicide survivors were generally frustrated with the lack of communication and involvement of the family in the health plan due to the need to maintain patient confidentiality (Peters et al., 2013). If survivors have an opportunity to collaborate and work alongside professionals to better understand and incorporate the needs of their loved one, a more effective treatment plan can be implemented.
A study on parental bereavement stress and preventive intervention following the violent deaths of an adolescent or young adult child found that talking through the event can allow survivors to revise it in ways that make it more tolerable and to impose order on experience (Murphy, 1996). This form of cognitive reframing and assimilation can also result in fewer episodes of intrusive thoughts and images. Intrusive thoughts can contribute to the distress experienced by the suicide-bereaved and are also a common symptom of complicated grief, thus, addressing this issue is vital in minimizing bereavement stress (Ennis & Majid, 2020). Dunn and Morrish-Vidners (1987) found that respondents in their study seemed eager to talk in detail. They noted that “[…] suicide survivors have a dire need to talk about their tragedy; however, they usually have little opportunity to express their thoughts and feelings openly” (p. 181).
Implications for Grief Counselling
Due to the uniqueness of suicide bereavement from other types of bereavement, providing counselling to this population will also be a unique process. It may be helpful for survivors to be made aware of the potential changes that may occur in their various social interactions. Informing survivors of common fears such as fears of loss, abandonment, and judgement can prepare survivors to recognize these in their own lives and find comfort in knowing that they are not alone in their experience. Being warned of varying grief processes in families, ambiguity of social norms following suicide and avoidance from friends can also be helpful in seeking out ways to accommodate for these challenges. We recommend family counselling if possible as this could encourage families to dialogue through their grief early on. Storytelling and testimony with other loved ones are acts of both recall and mourning which aids in rebuilding their assumptive world. It is important to address the many reasons suicide bereaved may avoid grief counselling and the necessity for friends and professionals to be proactive in offering support (Ross et al., 2021). Suicide bereaved may feel that they do not need professional support, believe that there is minimal benefit they can get from counselling, have previous negative experiences with professionals, or have experienced barriers to accessing professional support (Pitman et al., 2018a). Due to these reasons and many more, it is imperative for support of the suicide bereaved to extend beyond counselling. The results of a study by Pitman et al. (2018a) indicate that family and friends were the most valued sources of support. This includes support provided through extended social networks, such as neighbours, colleagues, religious communities, and the relatives of the deceased.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Umair Majid receives financial support from the Canadian Institutes of Health Research and the Government of Ontario, Canada. Neither party was involved in the design and conduct of this research.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.