
Abstract
This work focuses on different roles individuals might adopt in their family of origin: hero, scapegoat, lost child, mascot, caretaker, and mastermind. It was explored whether family dysfunction in the family of origin makes it more likely that individuals will take on certain roles, in particular those of “scapegoat” and “lost child.” Further, it was tested whether the problematic roles of scapegoat and lost child are linked to greater depressive symptoms later on during adulthood. Support for these predictions was found in two correlational survey studies of young and older adults retrospectively reporting the roles they assumed in their family of origin (N = 176 and 366, respectively). Findings are discussed in terms of their implications for family therapy.
Within groups, group members often assume different roles. Certain individuals might end up as “social secretary” or gain a reputation to be the “troublemaker” and not play by the rules. Families are no different—within family systems, parents and children might find themselves, voluntarily or not, adopting certain behaviors and roles. This article will investigate six potential roles (see Sanders et al., 2014; Verdiano, 1987) individuals might adopt within their family while growing up. These are the roles of hero, scapegoat, lost child, mascot, caretaker, and mastermind. This article will look at both antecedents and consequences of family roles individuals might adopt. Specifically, it will be tested how roles relate to levels of family dysfunction and what their consequences are for the manifestation of depressive symptoms later in life.
Roles
Within families, people have expectations about who does what and who behaves how. These are tacit or explicit rules about the division of labor and behavior that is appropriate for different family members. For example, gender stereotypes inform expectations of how men and women are supposed to behave within the family (Gere & Helwig, 2012), but people also have expectations about the roles children should adopt within the family system.
Verdiano (1987) described four roles children might adopt. The “hero” typically tries to be a high achiever out of a desire to please the parents rather than out of intrinsic motivation, the “scapegoat” is nonconformist and rebellious and acts out as the catalyst for problems inherent in the family system, the “lost child” tends to be emotionally sensitive and might feel overlooked and ignored within the family, and the “mascot” is the group’s comedian and entertainer of the family. Verdiano found that the roles of scapegoat and lost child were particularly negatively related to family satisfaction, giving some indication that these two roles might be particularly difficult (see also Verdiano et al., 1990).
The importance of the four roles highlighted by Verdiano (1987) was also emphasized, and alternative measurement approaches were proposed by other scholars (Kier & Buras, 1999; Potter & Williams, 1991; Wampler et al., 2009). Although it is encouraging that these roles have repeatedly been found to have meaningful associations with relevant outcomes, several of these studies focus on participants’ self-descriptions that are very generic and do not specifically refer to the family system (e.g., “I am shy, lonely, solemn” rather than “Within my family, I act shy”; see Wampler et al., 2009). The present work aimed to improve on this because domain-specific measures (i.e., those that actually ask about the family context of theoretical interest rather than about generic, global personality tendencies) are better able to tap into the processes of interest (Wu & Yao, 2007).
The present studies also aimed to go beyond previous contributions by extending the scope of roles under study from four to six, by adding another two potential roles. These are the roles of “caretaker” and “mastermind.” One important phenomenon that has been described particularly for adult children of alcoholic parents is role reversal, sometimes referred to as parentification, where children are forced to assume the roles of caretaker in their parents’ stead (Burnett et al., 2006; Pasternak & Schier, 2012). Abraham and Stein (2013) demonstrate a similar process for children of mentally ill parents. Typically, role reversal between parent and child has been associated with negative consequences (Nuttall et al., 2019). In an attempt to do justice to the importance of role reversal in parent–child relations, in the present investigation, the role of caretaker was added to the roles previously described by Verdiano (1987).
One final role was also added to the list. Helicopter parenting (e.g., Cui et al., 2019; Ginott, 1969) is a parenting style where caretakers constantly “hover overhead” and pay extremely close attention to a child’s experiences and problems. This trend is associated with parents catering to their children’s every whim, doing things on the children’s behalf, and minimizing discomfort for the children as much as possible. Helicopter parenting might be seen as a worrying trend because it has been linked to poor psychosocial adjustment of children (Schiffrin et al., 2019). Children of helicopter parents can be assumed to regularly feel that they are “getting their own way.” Because of the potential significance of this trend, the role of “mastermind” was also included in the study, to tap into those feelings of “always getting my way.”
Family-of-Origin Dysfunction
In dysfunctional families, conflict, misbehavior, child neglect, or abuse feature regularly. While the most extreme forms of dysfunction are captured in research on adverse childhood experiences (ACE; Bellis et al., 2018; Rudenstine et al., 2019), other attempts have been made to also capture the less extreme but still unhealthy dynamics at play in dysfunctional families. One widely used scale is by Epstein et al. (1983). The Family Assessment Device (FAD) consists of seven subscales that tap into problematic problem-solving, problematic communication, unclear roles, lack of affective responsiveness, lack of affective involvement, behavior control, and general functioning issues. Those dimensions are combined into a global index of dysfunction.
Dysfunction as captured by the FAD is often related to severe problems such as alcoholism and mental illness. For example, Friedmann and colleagues (1997) found dysfunction levels to be higher in families struggling with mental illness compared to control families. Family dysfunction is often passed on to, and reenacted by, the next generation (Morrison, 1977). It is well demonstrated that experiences during childhood can negatively impact later psychosocial adjustment and outcomes (Chen et al., 2009; Johnson et al., 2015; Maleck & Papp, 2015; Mothersead et al., 1998).
The Link Between Dysfunction and Roles
One question the present work aimed to address is whether certain roles are more likely to be assumed by children in families characterized by dysfunction. It has been argued that children in dysfunctional families often experience parental inconsistencies, double-bind messages, hidden feelings, incomplete information, shame, uncertainty, and mistrust, and this can lead to the adoption of rigid roles which might lead to problems later on (Wegscheider, 1981). Others agree that while in a healthy situation individuals should adopt different roles with a certain degree of flexibility, roles become more fixed and rigid in unhealthy social systems (Buelow et al., 1994). Indeed, Jenkins and colleagues (1993) found that a history of alcoholism and dysfunction was linked to the adoption of certain unhelpful family roles.
Potter and Williams (1991) suggest that the roles of scapegoat and lost child in particular should be problematic, and they should emerge more readily in dysfunctional families. They found less evidence for the roles of hero and mascot to be linked to family dysfunction. In agreement with this, Alford (1998) also found family dysfunction to be linked to the role of scapegoat and lost child. We therefore hypothesized that the present studies would replicate these earlier findings: Family dysfunction would be associated with greater adoption of the roles of scapegoat and lost child but not be associated with the adoption of the roles of hero and mascot.
With regard to the roles of caretaker and mastermind, which have not previously been studied, no strong a priori hypotheses were held. It seemed plausible that family dysfunction would necessitate more caretaker role adoption in children, although this might not be the case in very dissociated, distant families (which is also a type of dysfunction the FAD taps into). Moreover, it seemed plausible that the child as mastermind, who usually gets their own way, would be more likely to emerge when family dysfunction is low, but then again, the level of attention and parental support implied by making the child the master might not be available in strongly dysfunctional families, which will be preoccupied by other issues. In sum, then, there are reasons to assume that caretakers and masterminds would feature both more and less strongly in dysfunctional families, which means these roles were only included for initial, exploratory purposes.
The Link Between Roles and Depressive Symptoms
Certain roles have been found to be related to negative outcomes, such as anxiety and other psychological disorders, as stated by Wampler et al. (2009). Fischer and Wampler (1994) found that the role of scapegoat in particular was associated with own abusive drinking in adult children. Moreover, as mentioned above, Verdiano (1987) found the roles of scapegoat and lost child to be particularly negatively related to family satisfaction. Prior research has, to our knowledge, not tried to link family roles to depressive symptoms. However, because the scapegoat and lost child roles have been linked to other negative outcomes such as alcohol abuse and problematic family relationships, we hypothesized that these two roles would also be linked to the manifestation of depressive symptoms. We expected the roles of hero and mascot, which have not been linked to negative outcomes to the same extent, not to be associated with depressive symptoms.
Again, no strong a priori hypotheses were held regarding the roles of caretaker and mastermind. On the one hand, both of these roles contain an element that might be experienced as empowering. Being able to help others (caretaker), and being effective at having one’s interests recognized and met (mastermind), might arguably be positive experiences, which should be linked to fewer depressive symptoms. On the other hand, having to take care of others when one feels ill-equipped to do so might reasonably be expected to trigger depression. Frequently getting one’s own way might also be expected to negatively impact on mental health, on the basis of the adverse effects of helicopter parenting on children’s adjustment which is now an emergent finding in the literature (e.g., Schiffrin et al., 2019). Moreover, the recipients of helicopter parenting are also being sent the subtle message that they might not be able to cope by themselves, without parental support. Again, then, there are reasons to assume that caretaker and mastermind roles might be both positively and negatively related to depression as an outcome variable, which is why no strong directional predictions were made about the potential effects of these two roles.
To sum up, following previous research, it was expected that family-of-origin dysfunction would be associated with more adoption of the roles of scapegoat and lost child but that it would be unrelated to the adoption of the roles of hero and mascot. No strong a priori predictions were made about the association with the roles of caretaker and mastermind, but these two roles were included for exploratory purposes.
Further, the roles of scapegoat and lost child were hypothesized to be associated with more depressive symptoms, whereas the roles of hero and mascot were not expected to have an effect on this outcome. Again, caretaker and mastermind were included for exploratory purposes, but no strong a priori predictions were made about these two variables. Predictions were tested in two correlational survey studies of young and older adults reporting the roles they assumed in their family of origin, family-of-origin dysfunction, and current depressive symptoms.
Study 1
Method
Participants
The sample consisted of one hundred and seventy-six people. The mean age was 18.65 years (142 females, 33 males, and one participant did not declare their gender). Participants were recruited at a university open day, and further participants were recruited in public spaces (e.g., a university library) by research assistants. The open day was targeted at secondary school students in their penultimate or final year of schooling; hence, those participants were still living with their parents. Because we wanted participants to respond in relation to dysfunction in their family of origin (not a family they themselves might have founded), only participants aged 22 or younger, that is, those who were still dependents living with their parents, were included in the final sample (leading to the exclusion of responses by teachers, some of whom also chose to fill out the questionnaire). This cross-sectional correlational study included the following measures.
Measures
Family dysfunction was measured with a shortened 24-item version of the FAD (Epstein et al., 1983) which taps into the family’s ability to constructively solve problems, communicate efficiently, have clear rules, and other aspects of functioning. Participants were asked to think of everyone living in their household and to indicate to which extent the following statements are true for them (1 = not at all to 7 = very much). Example items are as follows: “we usually act on our decisions regarding problems,” “we are good at talking to each other,” “we make sure members meet their family responsibilities,” “in times of crisis we can turn to each other for support,” and “individuals are accepted for what they are,” α = .91.
Family roles were assessed with items designed to tap into the roles described in Verdiano (1987) and Potter and Williams (1991; hero, scapegoat, lost child, mascot), plus the additional two profiles (caretaker and mastermind). Two items were used to measure each role (1 = not at all to 7 = very much). For Hero, the items were “I must achieve lots in life, for my parents’ sake” and “I am someone who my parents can rely on to be good.” Because the α for these two items was unacceptably low, it was decided to only use the first item as a single-item indicator. For scapegoat, the items were “I am someone who causes lots of worries for my parents” and “My parents wrongly blame me for what is wrong with our family,” α = .65. For lost child, the items were “I am someone who hardly gets noticed” and “My needs often go unmet within the family,” α = .53. For mascot, the items were “I am someone who often makes fun to cheer everyone up” and “I am good at making people laugh,” α = .80. For Caretaker, the items were “I am someone who provides emotional support to my parents” and “I am a shoulder for my parents to lean on,” α = .82. For mastermind, the items were “I am someone who usually gets what he/she wants” and “I am good at getting my own way within the family,” α = .82.
Depressive symptoms were measured with 12 items similar to those used in Zagefka and Jamir (2015; six reversed, 1 = strongly disagree to 7 = strongly agree). Example items are “Have you recently been able to concentrate on what you were doing?” “Have you recently lost much sleep over worry?” and “Have you recently felt that you are playing a useful part in things?” (reversed), α = .88.
The questionnaires for both studies also included a number of other questions which are not relevant in the present context and which will not be discussed further here. Full materials as well as the data for both studies are available from the first author upon request. All aspects of the research were in line with American Psychological Association and British Psychological Society ethics guidelines. Participation was voluntary, and no monetary compensation was offered.
Results and Discussion
Descriptives and bivariate correlations for all measures are displayed in Table 1. As can be seen from Table 1, family dysfunction was positively associated with the roles of scapegoat and lost child. It was not associated with the roles of hero, mascot, caretaker, or mastermind. Moreover, none of the roles were particularly highly correlated with each other, providing evidence that they represent distinct sets of behavior.
Bivariate Correlations and Means for Study 1.
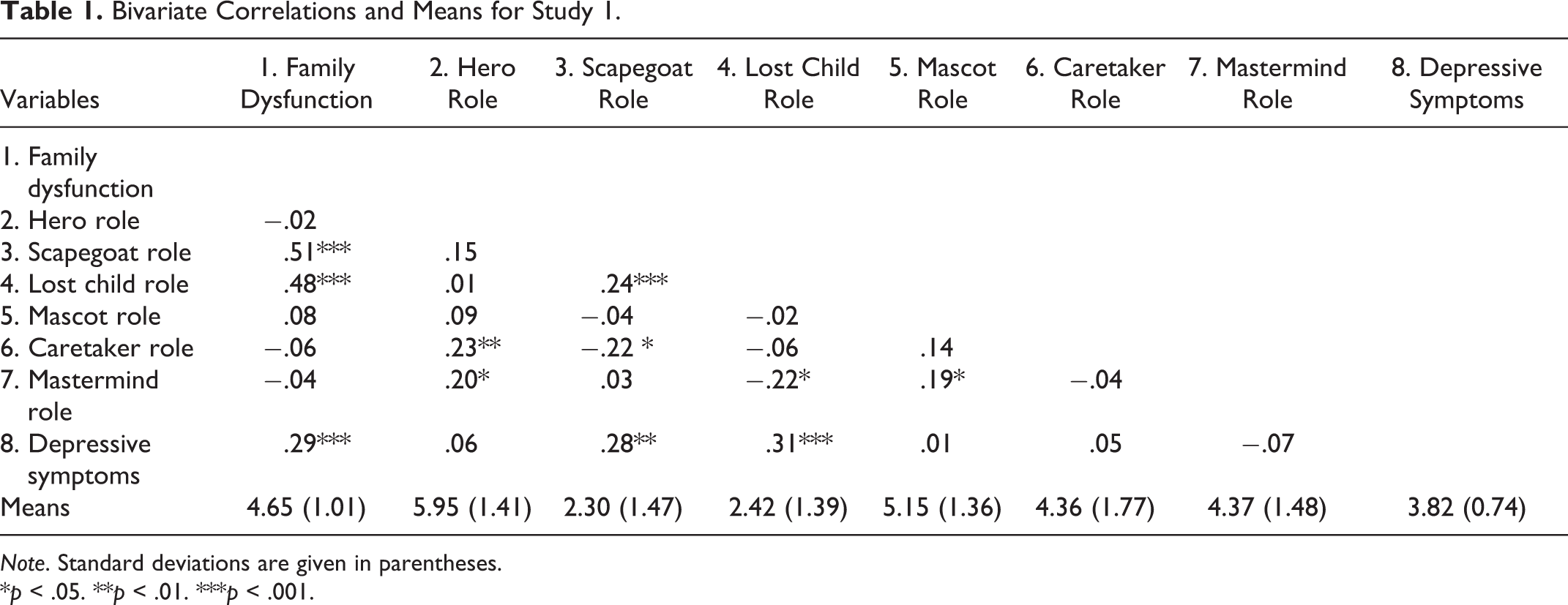
Note. Standard deviations are given in parentheses.
*p < .05. **p < .01. ***p < .001.
To test the effects of the roles on depressive symptoms, a multiple regression was run with depressive symptoms as dependent variable and the six roles as independent variables. Results are displayed in Table 2 (note: Table 2 presents results from both Studies 1 and 2, for ease of comparison across studies). As is apparent there, having the roles of scapegoat or lost child was positively associated with depressive symptoms, whereas none of the other roles was significantly related to depressive symptoms.
Regression Results Studies 1 and 2, Predicting Depressive Symptoms From Family Roles.
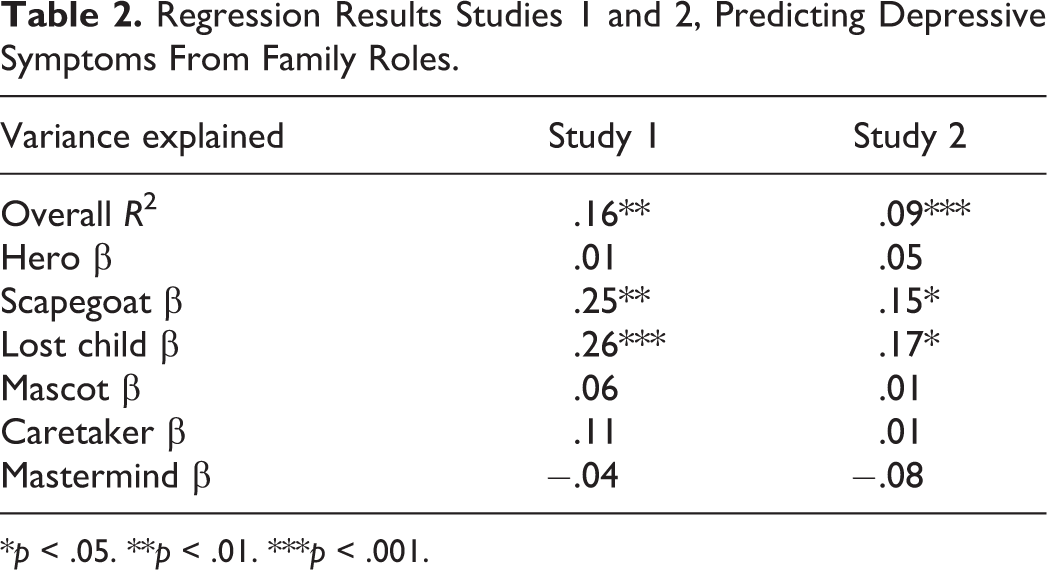
*p < .05. **p < .01. ***p < .001.
To sum up, results were in line with predictions. Dysfunction in the family of origin was associated with children assuming the roles of scapegoat and lost child, which were themselves associated with more depressive symptoms reported in adulthood.
A second study was conducted to test the robustness of observed effects and to see whether results would replicate with a second, independent sample. A further aim of the second study was to improve on the design. One issue with Study 1 was that because of the way the family dysfunction question was worded (referring to everyone living in the household), these questions only clearly referred to the family of origin for young participants who were still living with their parents. To enable us to also include older participants in the sample, these questions were reworded for Study 2.
Study 2
Method
Participants
Three hundred and sixty-six participants completed this online study (mean age = 33; 145 males, 217 females, and four chose the category “other” to specify their gender). This was a convenience sample accessed by student research assistants recruiting personal contacts and encouraging them to recruit others via a snowballing effect. Everyone who was willing to participate was included in the final sample. This cross-sectional correlational study included the following measures.
Measures
Family dysfunction was again measured with a version of the FAD (Epstein et al., 1983), this time shortened to 14 item. Whereas in Study 1 participants had been asked to think of everyone living in their household, this time they were explicitly instructed to think about their “family growing up.” This alteration was made to avoid having to impose an age limit on participants; now, even very senior participants were eligible to be included in the final sample because with this wording, the questions referred clearly to the family of origin for all participants. As in Study 1, items were assessed on a 7-point scale (1 = not at all to 7 = very much), α = .91.
Family roles were assessed with items designed to tap into the same roles as in study 1 (hero, scapegoat, lost child, mascot, caretaker, and mastermind). Two items, very similar in wording to Study 1, were used to measure each role (1 = not at all to 7 = very much). For hero, the items were “I felt I must achieve lots in life, for my parents’ sake” and “I was a child who my parents could rely on to be good.” Again, the α for these two items was low, and only the first item was used as a single-item indicator. For scapegoat, the items were “I was a child who caused lots of worries for my parents” and “My parents wrongly blamed me for what was wrong with our family,” α = .69. For lost child, the items were “I was a quiet child who hardly got noticed” and “My needs often went unmet within the family,” α = .67. For mascot, the items were “I was a child who often made fun to cheer everyone up” and “I was good at making people laugh,” α = .77. For caretaker, the items were “I was a child who provided emotional support to my parents” and “I was a shoulder for my parents to lean on,” α = .87. For mastermind, the items were “I was a child who usually got what it wanted” and “I was good at getting my own way within the family,” α = .83.
Depressive symptoms were measured with a shortened eight-item version of the one used in Study 1 (four reversed, 1 = strongly disagree to 7 = strongly agree), α = .80.
Results and Discussion
Descriptives and bivariate correlations for all measures are displayed in Table 3. As can be seen from the table, family dysfunction was positively associated with the roles of scapegoat and lost child. Dysfunction was also correlated with the role of hero in this study, but this effect was noticeably smaller than the association with the roles of scapegoat and lost child. Dysfunction was not associated with the roles of mascot, caretaker, or mastermind.
Bivariate Correlations and Means for Study 2.
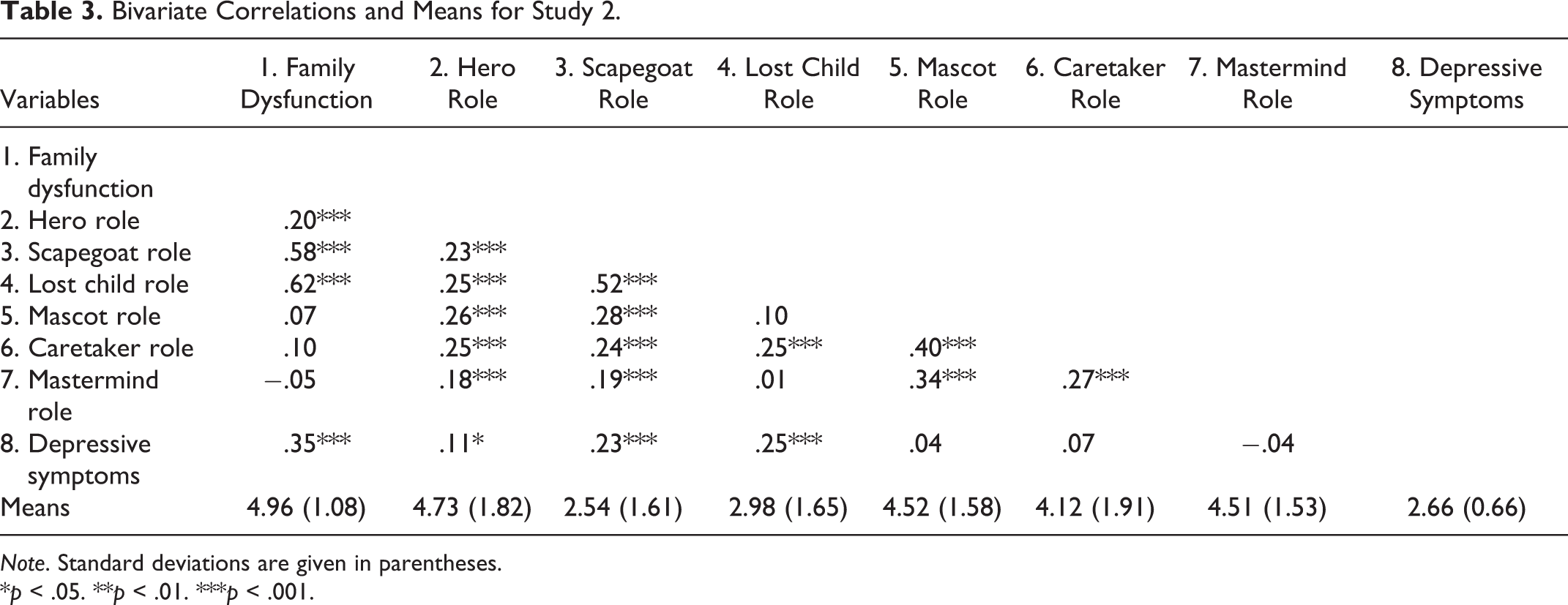
Note. Standard deviations are given in parentheses.
*p < .05. **p < .01. ***p < .001.
To test the effects of the roles on depressive symptoms, a multiple regression was run with depressive symptoms as dependent variable and the six roles as independent variables. Results are displayed in Table 2. As is apparent there, and mirroring the results of Study 1, having the roles of scapegoat or lost child was positively associated with depressive symptoms, whereas none of the other roles was significantly related to depressive symptoms.
The results of the second study mirrored those of the first study. Again, dysfunction in the family of origin was associated with the roles of scapegoat and lost child but also hero. Scapegoat and lost child roles were, in turn, associated with the reporting of more depressive symptoms.
General Discussion
Across two studies, evidence was found that dysfunction in the family of origin is associated with self-reports of having assumed the roles of scapegoat and lost child in the family of origin but not with the extent to which individuals reported having assumed the roles of mascot, caretaker, or mastermind. Dysfunction was not associated with the extent to which individuals reported having assumed the roles of hero in Study 1, although a positive correlation was observed in Study 2. Importantly, the roles of scapegoat and lost child were associated with more depressive symptoms during adulthood. The results are compatible with the idea that family dysfunction during childhood makes it more likely for children to fall into certain behavioral patterns and roles and that these roles then have a negative impact on psychosocial adjustment later in life.
These findings demonstrate one potential mechanism through which ACE impact on later adult outcomes. Previous work has highlighted other mechanisms such as self-views and worldviews (Chen et al., 2009) or attachment patterns (Mothersead et al., 1998). The present work goes beyond these existing insights, by emphasizing the importance of not focusing on individuals but on the relationship between individuals, and on the roles children assume in dysfunctional family systems.
Gestalt therapy (Cole & Reese, 2017) and other counseling approaches that emphasize group process, for example, family systems therapy (Bowen, 1972; Popovic, 2019), agree that complex dynamics are at play within groups, and often different group members take on different roles within the group to generate the group’s unique dynamic. They also agree that pathology must often be understood not as a phenomenon resultant from individual disposition but as a reaction to the environment—it is to be understood and treated in relational terms. Group psychotherapy and family systems approaches to counseling go beyond the 1-2-1 counseling approach by emphasizing relational dynamics. In the same vein, this article goes beyond intraindividual factors, by highlighting the importance of roles within the family system as a mechanism able to explain the effects of family-of-origin dysfunction on later adult health.
Of course, there are some limitations to this work which should be acknowledged. Maybe most importantly, insights are based on participants’ self-reports. Although some research suggests recall of particularly stressful life events during childhood to often actually be quite accurate (Baugerud et al., 2014), the fact that human recall and memory is fallible and often inaccurate is also well-documented (Herrmann et al., 2005), and recall imprecisions might be particularly pronounced among people suffering from depression (Orchard & Reynolds, 2018). There can therefore be assumed to be a measure of inaccuracy in the participants’ recall of dysfunction in the family of origin and the roles participants recall to have assumed in the past. This issue is hard to address, other than through the use of prospective and longitudinal studies, which would of course be very resource intensive.
Related to the previous point, a further limitation is that the studies present correlational data, which means caution is indicated when trying to make inferences about causality. To put it simply, the data cannot demonstrate that it is really roles that lead to depressive symptoms. Although the pattern of results is compatible with the hypotheses, they are also compatible with the idea that those who are more depressed as a consequence recall having had different roles. Again, expensive prospective studies would be needed to generate stronger evidence regarding the proposed causal direction of effects.
Moreover, the total effect of roles on depressive symptoms was quite small. Future research could determine whether other factors need to take into consideration to account for a bigger proportion of the variance or whether measurement error might have played a role. It is clearly possible to improve on the measurement approach to family roles. Two item measures are possibly not the most robust way of tapping into these constructs. Although the fact that the pattern was in line with predictions, and consistent across studies, strongly suggests that measurement of roles is sufficiently accurate to yield meaningful results, clearly, future work could be directed at devising stronger measurement instruments.
There are some further interesting avenues for future research. First, the present findings demonstrate an effect of general dysfunction, measured by a very global index based on the McMaster FAD. This measure has good internal consistency, suggesting that different areas of dysfunction strongly covary (e.g., families who have trouble communicating tend to also have trouble with affective involvement and constructive problem-solving). However, there are of course many different types of dysfunction. For example, some families struggle with alcoholism or domestic violence, while others struggle with incest. As Tolstoy observed in “Anna Karenina”: “every unhappy family is unhappy in its own way.” There is thus an urgent need to examine the processes observed here under a more fine-grained lens. It is possible that certain types of dysfunction are not associated, as seen here, with the roles of scapegoat or lost child, but instead with other roles. There is some evidence this might be the case. For example, siblings of mentally ill children have been found to be more likely to assume the roles of lost child, which would mirror the findings of the present investigation, but also of hero (Sanders et al., 2014). Future research is needed to test the boundary conditions of the effects found here.
Second, future research could also test whether the roles that were associated with negative outcomes here will always have this effect and whether the roles that were not associated with negative outcomes here will always have these consequences. Again, this is a question of boundary conditions. For example, the roles of hero and caretaker both have an empowering element to them—the hero is competent and able to achieve and the caretaker is competent in looking after others. These positive competencies might be good for mental well-being unless the person in question feels overwhelmed by their responsibilities. Hence, one might propose that whether these roles have positive or negative consequences will be moderated by perceived ability to cope or possibly perceived amount of choice in taking on these roles (whether they are entered into voluntarily or whether individuals feel they are pushed into them). Future research could investigate this.
Third, the six roles studied here do, of course, not constitute an ultimate list. We did already go beyond the previous literature by studying not only the four roles highlighted by Potter and Williams (1991) but adding also the potentially important roles of caretaker and mastermind. However, other roles might potentially be assumed by children and might show strong relationships to later outcomes. One example is the role of mediator (Dimitropoulos et al., 2009). Future, ideally bottom-up qualitative work could shed light on other roles that might feature within family systems.
Finally, as outlined above, some scholars have suggested that problematic outcomes might not be due to the adoption of certain roles but due to the rigidity with which roles are held and adhered to (Buelow et al., 1994). An attempt to design stronger measures of family roles could take this into account and explicitly include questions about participants’ recall of how rigid and fixed certain roles were within the family system. Included could also be questions about the extent to which roles were assumed voluntarily or not. An exploration of the extent of perceived rigidity and degree of choice would certainly be very interesting.
The findings have clear implications for the design of therapeutic interventions. They suggest that family therapists should be particularly alert to children exhibiting behaviors commensurate with the role assignment of scapegoat or lost child because those seem to be linked to particularly adverse effects later on (a caveat should be added about the need to test these inferences with stronger, prospective data, but these seem reasonable conclusions on the basis of the present, imperfect evidence). The first step of a therapeutic intervention could be to make families aware of existing role dynamics, and the second step could be to attempt to gently intervene and improve them.
Insights in this article are based on responses from (across both studies) 442 individuals. With conclusions drawn on the basis of statistical data and numbers, it is easy to lose sight of the phenomenological experience of individuals. Although participants are represented in the analyses in terms of numbers, within the sample, there were people who reported on their subjective, and often unpleasant, experiences. There were individuals who reported feeling strongly that they were unfairly blamed by their family for existing issues, who reported feeling that they and their needs did not get any attention within the family, and who reported high levels of current depressive symptoms. Responses such as these are alarming, and for the sake of these participants and others like them, it is hoped the present article can spark further research into the crucial role family dynamics can play for later outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.