
Abstract
The current study investigated the mediating role of depressogenic and intimate relationship distress-maintaining attributions in the association between depressive symptoms and relationship distress in an undergraduate dating sample. Results indicated that taken together, depressogenic and distress-maintaining attributions significantly mediated the association between depressive symptoms predicting relationship distress for women, but not men. Examination of the specific indirect effects revealed that distress-maintaining blame attributions had a significant indirect effect in this association for both men and women. Possible clinical implications for the treatment of depressive symptoms and relationship distress are discussed.
Numerous cross-sectional and longitudinal studies have found an association between depressive symptoms and intimate relationship distress (i.e., poor functioning and low satisfaction in intimate relationships; see Whisman, 2001 for a review). In recent years, research in this area has expanded to investigate potential factors that may mediate this well-established association (e.g., Heene, Buysee, & Van Oost, 2005, 2007). Cognitive variables, in the form of attributions (i.e., assigning cause to actions or behaviors), are an example of one such factor, as general attributions and attributions about one’s partner’s negative relationship behavior have been linked to depression and relationship discord, respectively (e.g., Bradbury & Fincham, 1990; Cropley & Macleod, 2003; Fincham, 1994; Rotenberg, Costa, Trueman, & Lattimore, 2012; Sanjuán & Magallares, 2009). However, no mediational studies to date have considered both general and relationship-oriented attributions simultaneously when predicting either depression or relationship distress outcomes. Moreover, there has been a conscious shift away from determining the directionality of this relationship (Davila, 2001; Whisman, 2001), yet the direction of this association is important when investigating potential mediators, both theoretically and clinically, and therefore needs to be taken into consideration. Thus, the purpose of the current article is to help clarify the role of both general and relationship-oriented attributions as potential mediators in the association between depressive symptoms and intimate relationship distress within a student sample in dating relationships.
Years of research on depression has shown that individuals who are depressed have a propensity to make internal, stable, and global attributions for negative events (e.g., blaming themselves for negative events or outcomes; Cropley & Macleod, 2003; Rotenberg et al., 2012; Sanjuán & Magallares, 2009). Similarly, individuals who are dissatisfied in their intimate relationships also tend to make internal, stable, and global attributions about partner’s negative relationship behaviors (e.g., seeing their partner as the cause of, and holding their partner responsible for, negative relationship events or outcomes; Bradbury & Fincham, 1990; Fincham, 1994). Although the association between depression and relationship distress has been well documented, and each of these variables alone has been linked to specific types of attributions, there is a lack of research integrating both general and relationship-oriented attributions as predictors of depression and relationship outcomes.
We are aware of only one study that has identified the relative influence of these different attributions on relationship distress and depression outcomes (Horneffer & Fincham, 1996, 1997). Using structural equation modeling, two competing attributional models predicting both depression and marital distress outcomes were tested in a sample of 150 married couples. Attributions that were associated with depression were labeled depressogenic attributions, whereas attributions consistent with intimate relationship distress were labeled distress-maintaining attributions. The first model tested an attribution-specific model in which both depressogenic and distress-maintaining attributions simultaneously predicted both depression and relationship distress. The second model was a general negative attribution model in which only depressogenic attributions predicted both depression and relationship distress. It was based on the assumption that a similar attributional process was operating for both types of attributions, thus positing that distress-maintaining attributions were a subset of depressogenic attributions (Horneffer & Fincham, 1996, 1997). Results indicated that the attribution-specific model (i.e., the model that included both depressogenic and distress-maintaining attributions) was a significantly better fit to the data than the general attribution model (i.e., the model that only included depressogenic attributions) for both husbands and wives. Furthermore, in the attribution-specific model, depressogenic attributions uniquely contributed to relationship distress and relationship distress-maintaining attributions uniquely contributed to the prediction of depressive outcomes. This highlights the importance of including both types of attributions when examining the role of attributions in depression and relationship distress outcomes, as they both uniquely predicted variance in these variables.
Although Horneffer and Fincham’s (1996, 1997) findings represent an important advancement in understanding the role of both types of attributions in the depression and relationship distress association, subsequent studies examining attributions as a possible mediator of the association between relationship distress and depression have not integrated these findings into their work. As a result, the scant research in this area has only considered distress-maintaining attributions as a possible mediator in the association, overlooking the influence of general or depressogenic attributions.
Of the few studies that have investigated distress-maintaining attributions as a possible mediator of the association between relationship distress and depression, results have been mixed. For example, Heene et al. (2005) examined causal and blame attributions about partner’s negative relationship behaviors and found that causal attributions mediated the association between intimate relationship distress and depressive symptoms for both men and women, in a nonclinical sample. In addition, blame attributions were a mediator, but only for men. In a follow-up study that included both clinical and nonclinical samples, Heene et al. (2007) found that causal attributions, but not blame attributions, mediated the association between intimate relationship distress and depression for both men and women.
In an effort to extend the existing literature, Smith (2011) included both self- and partner-focused attributions for negative relationship behavior in a mediation model. Although the inclusion of both self- and partner-focused attributions better approximates the integration of relationship-oriented and general attributions offered by Horneffer and Fincham (1996, 1997), the self-focused negative relationship behavior attributions used in this study were more likely a subset of distress-maintaining attributions rather than general depressogenic attributions. Moreover, these self-focused attributions were not actually included in the mediation model because this variable was not found to be significantly associated with depressive symptoms. Nevertheless, Smith (2011) was able to examine partner-focused attributions (causal and blame subscales were combined) for negative relationship behavior in a subsample of college students, finding that these attributions partially mediated the association between depressive symptoms and relationship distress. This finding was consistent with work by Heene and colleagues (2005, 2007).
In contrast, Gordon and colleagues’ study with a nonclinical community sample revealed that partner-focused attributions (causal and blame) did not mediate the association between relationship discord and depressive symptoms (Gordon, Friedman, Miller, & Gaertner, 2005). These findings are consistent with earlier work in this area (Fincham & Bradbury, 1993; Heim & Snyder, 1991), although these previous studies did not formally test mediation but instead examined associations between variables via regression analyses. Although these findings evidence a potential discrepancy regarding the role of relationship-oriented attributions in the association between intimate relationship distress and depression, the paucity of work in this area makes it difficult to determine their role more conclusively.
In addition to limitations related to the type of attributions, prior work has conceptualized the direction of the association between relationship distress and depression unidirectionally, with some studies modeling depression preceding relationship distress and others modeling the reverse. Despite the fact that the association between depression and relationship discord has been well documented, its directionality is poorly understood, with some arguing that depression likely precedes intimate relationship distress (Coyne, 1976), while others maintain that the temporality of the association is likely to be in the opposite direction (Beach, Katz, Kim, & Brody, 2003; Beach, Sandeen, & O’Leary, 1990; Whisman & Bruce, 1999). Still others argue that the association is likely to be bidirectional (e.g., Davila, Bradbury, Cohan, & Tochluk, 1997; O’Leary, Riso, & Beach, 1990). Given the recent trend to investigate potential mediators of this association (e.g., Gordon et al., 2005; Heene et al., 2005, 2007; Smith, 2011), the direction of the association between relationship distress and depression may be important to consider, as the mechanisms may differ based on the direction of the association. Thus, modeling mediational analyses both from depressive symptoms to relationship distress and vice versa will further inform the current understanding of the mediating role of attributions.
Advancing work in this area, the current study examined both depressogenic and distress-maintaining attributions in a model with depressive symptoms predicting intimate relationship distress, and vice versa, using bootstrapping mediational analyses. We hypothesized that (a) when taken together, both depressogenic and distress-maintaining attributions would mediate the association between depressive symptoms and intimate relationship functioning, in both models, and (b) depressogenic and distress-maintaining attributions would both independently mediate the association, in both models. Although the current state of the literature did not lead us to make specific hypotheses with regard to sex differences, previous work in this area has shown different findings across men and women (Heene et al., 2005, 2007). Thus, consistent with prior studies, mediational analyses were conducted separately for men and women.
Method
Participants
Participants were 204 (n = 127 females; n = 77 males) undergraduate students enrolled in a psychology course at a large Midwestern university in the United States. Each received partial course credit for their participation. In order to be eligible to participate in the study, participants had to be at least 19 years of age, fluent in English, and had to be in an intimate relationship for at least 1 month. The mean age of the sample was 19 years of age (standard deviation [SD] = 1.42) and participants were primarily Caucasian (>96%). The majority of participants endorsed being in monogamous dating relationships (86%), with the remainder engaged, cohabitating, or married. On average, participants were in their relationship for approximately 17.11 months (SD = 14.19). There were no differences between men and women on any of the variables.
Measures
Beck Depression Inventory (BDI)
The BDI (Beck, Ward, Mendelsohn, Mock, & Erbaugh, 1961) is a 21-item self-report measure of depressive symptoms. Each item is measured on a 4-point scale, ranging from 0 to 3. The BDI has strong psychometric properties (Beck, Steer, & Garbin, 1988). Higher scores indicate greater depressive symptomatology. In the present study, the α coefficient for this measure was .86.
Dyadic Adjustment Scale (DAS)
The DAS (Spanier, 1976) is a 32-item self-report measure of intimate relationship distress. Higher scores represent better relationship functioning. Scores below 97 on this measure are considered to be indicative of clinical relationship distress. Prior research has supported the psychometric properties of this measure (Sharpley & Cross, 1982). The DAS has been used in previous research with dating samples of similar age and relationship length (e.g., Cornelius, Shorey, & Beebe, 2010; Holland, Fraley, & Roisman, 2012). The α coefficient for the DAS was .85 in the present study.
Attributional Style Questionnaire (ASQ)
The ASQ (Peterson et al., 1982) measures the degree to which one makes causal attributions for negative events along three dimensions: locus (internal vs. external), globality (global vs. specific), and stability (stable vs. transient). The ASQ consists of 12 scenarios, 6 positive and 6 negative. A modified version of the ASQ was used for this study. The modified version included only three negative event scenarios and is consistent with work by previous researchers (see Barnett & Gotlib, 1988). Participants rated the dimensions of attributions for each scenario using a scale ranging from 1 to 7. Higher scores on each subscale indicate more internal, stable, and global attributions. The psychometric properties of this measure were tested in a college sample, with the alpha coefficients for the attributional dimensions for negative events ranging from .46 to .69 (Peterson et al., 1982). Similarly, in the present study, the overall α coefficient for the ASQ was .50.
Relationship Attribution Measure (RAM)
The RAM (Fincham & Bradbury, 1992) assesses the attributions that individuals make about their partners’ relationship behaviors. There are two subscales on the RAM: causal attributions and responsibility/blame attributions. Causal attributions measure the locus, stability, and globality of partner behaviors, and the responsibility/blame attributions measure the perceived intent of, and motivation for, partner behavior, as well as the extent to which an individual believes his or her partner should be blamed for his or her behavior. The measure utilizes four hypothetical situations, and participants rate the extent to which they agree on six different attributions for that behavior. Higher scores indicate greater ascription of causal and responsibility/blame attributions for partner behavior. Previous work has indicated that the RAM has strong psychometric properties, with good internal consistency for the subscales (α coefficients ranging from .84 to .91), and responses have been shown to correlate with attributions for real partner’s negative behavior (Fincham & Bradbury, 1992). In addition, the RAM has been shown to have adequate reliability in previous research with college dating samples (Hall & Fincham, 2006). In the present study, the α coefficient for the total scale was .86.
Procedure
Participants were informed of the study via an undergraduate psychology study pool, and those who were interested in participating contacted the researcher. Each participant gave informed consent before completing a self-report questionnaire package in a psychology laboratory that included measures assessing relationship functioning and mental health. The study was approved by the institutional review board at the university and all participants received partial course credit for completing the study.
Analyses
We initially conducted correlational analyses to determine the bivariate relationships between the variables of interest. Then, multiple-mediator models were used to test for distress-maintaining and depressogenic attributions as mediators in the association between depressive symptoms and intimate relationship functioning. Both subscales of the RAM (causal and blame) were used to account for distress-maintaining attributions; depressogenic attributions were comprised of the three facets drawn from the ASQ (locus, stability, and globality). In the first model, depressive symptoms predicted intimate relationship functioning; in the second model, intimate relationship functioning predicted depressive symptoms. We tested separate models for men and women which resulted in the testing of four models.
We followed procedures outlined by Preacher and Hayes (2008a) in conducting the multiple-mediator model analyses, using the Statistical Package for the Social Sciences (SPSS) macro designed by these authors. This procedure allowed for testing the effect of the independent variable (IV) on the dependent variable (DV) through the proposed mediators (M); this is known as the indirect effect. The indirect effect is the product of the direct effect of the IV on the M, a, and the direct effect of the M on the DV, partialling out the effect of the IV, b. Thus, ab is the calculation for the indirect effect. We used the bootstrap approach to create an empirical sample distribution of ab, using 5,000 estimates, from which point estimates and 95% confidence intervals (CIs) were derived. If CIs did not include zero within their parameters, then the indirect effects were considered to be significant.
The study employed bias-corrected and accelerated CIs because they correct for skewness in the distribution (Preacher & Hayes, 2008a; Williams & MacKinnon, 2008). It is important to note that the use of bias-corrected CIs may lead to inflated Type I error rates (MacKinnon, Lockwood, & Williams, 2004); yet the use of this method for conducting mediation is still advocated, given the increased statistical power garnered and more accurate CIs, as shown in empirical simulation studies (Fritz & MacKinnon, 2007; MacKinnon et al., 2004). Furthermore, in the absence of an overall model producing significant mediation, Hayes (2009) recommends that the specific indirect effects still be examined. Thus, the current study examined overall mediation as well as specific indirect effects.
Results
Bivariate correlations between the variables of interest, as well as variable means and SDs are included in Table 1. There were significant negative correlations between the BDI and DAS for both men and women; however, the ASQ locus and stability variables were not significantly correlated with either the BDI or the DAS for men or women. Most of the mediator variables were correlated with the BDI and the DAS in the expected directions. Specifically, the BDI was positively correlated with RAM blame for both men and women; for women only, RAM causal was positively correlated with the BDI, and for men only, ASQ globality showed a positive association with the BDI. Moreover, the DAS showed negative correlations with both RAM subscales for both men and women; and for women only, the DAS also showed a negative association with ASQ globality. Of exception for men, the RAM causal subscale was not significantly associated with depressive symptoms and none of the ASQ subscales were significantly associated with the DAS. For women, ASQ globality was not significantly associated with depressive symptoms.
Pearson Correlation Matrix for Model Variables and Variable Means by Participant Sex.
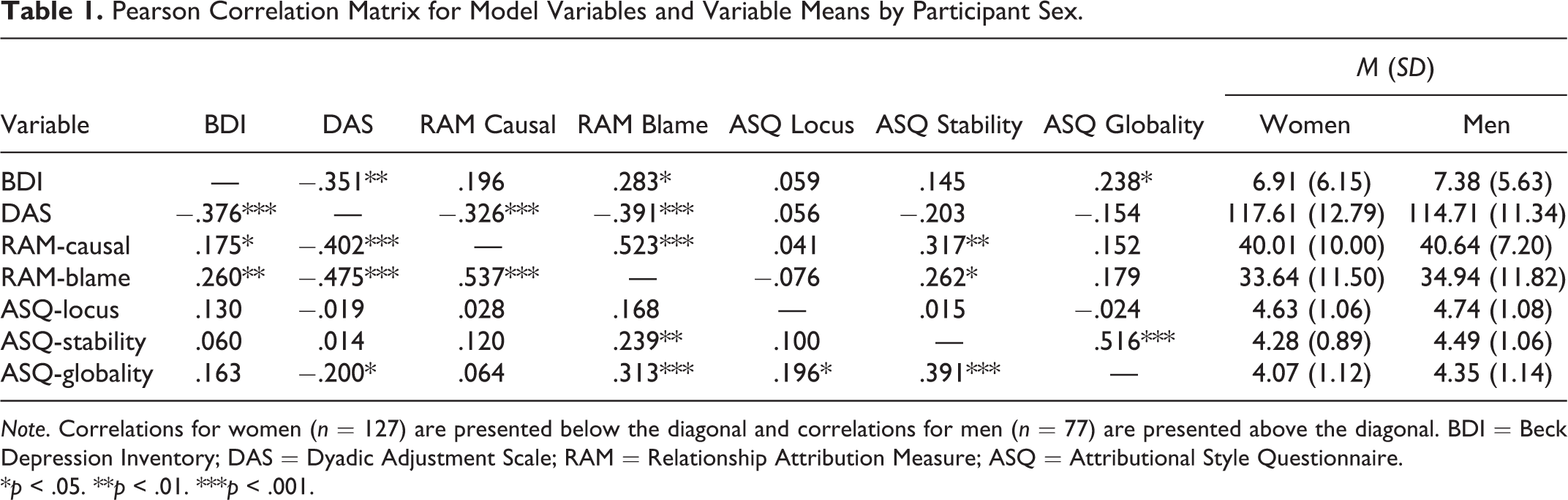
Note. Correlations for women (n = 127) are presented below the diagonal and correlations for men (n = 77) are presented above the diagonal. BDI = Beck Depression Inventory; DAS = Dyadic Adjustment Scale; RAM = Relationship Attribution Measure; ASQ = Attributional Style Questionnaire.
*p < .05. **p < .01. ***p < .001.
Mediational Analyses
In the first model for women, with depressive symptoms predicting relationship functioning, the overall indirect effect was significant, indicating that when taken together, both distress-maintaining and depressogenic attributions significantly mediated this association (see Table 2). However, when examining the specific indirect effects, only the relationship-oriented blame attributions (RAM blame) served as a significant indirect effect, with depressive symptomatology positively associated with blame attributions for partner’s negative behavior, which in turn predicted poorer intimate relationship functioning. In the second model for women, with relationship functioning predicting depressive symptoms, taken together the attributions did not mediate the association, nor were any of the specific indirect effects significant.
Summary of Mediation Results With Depressogenic and Distress-Maintaining Attributions as Mediators for Women and Men.
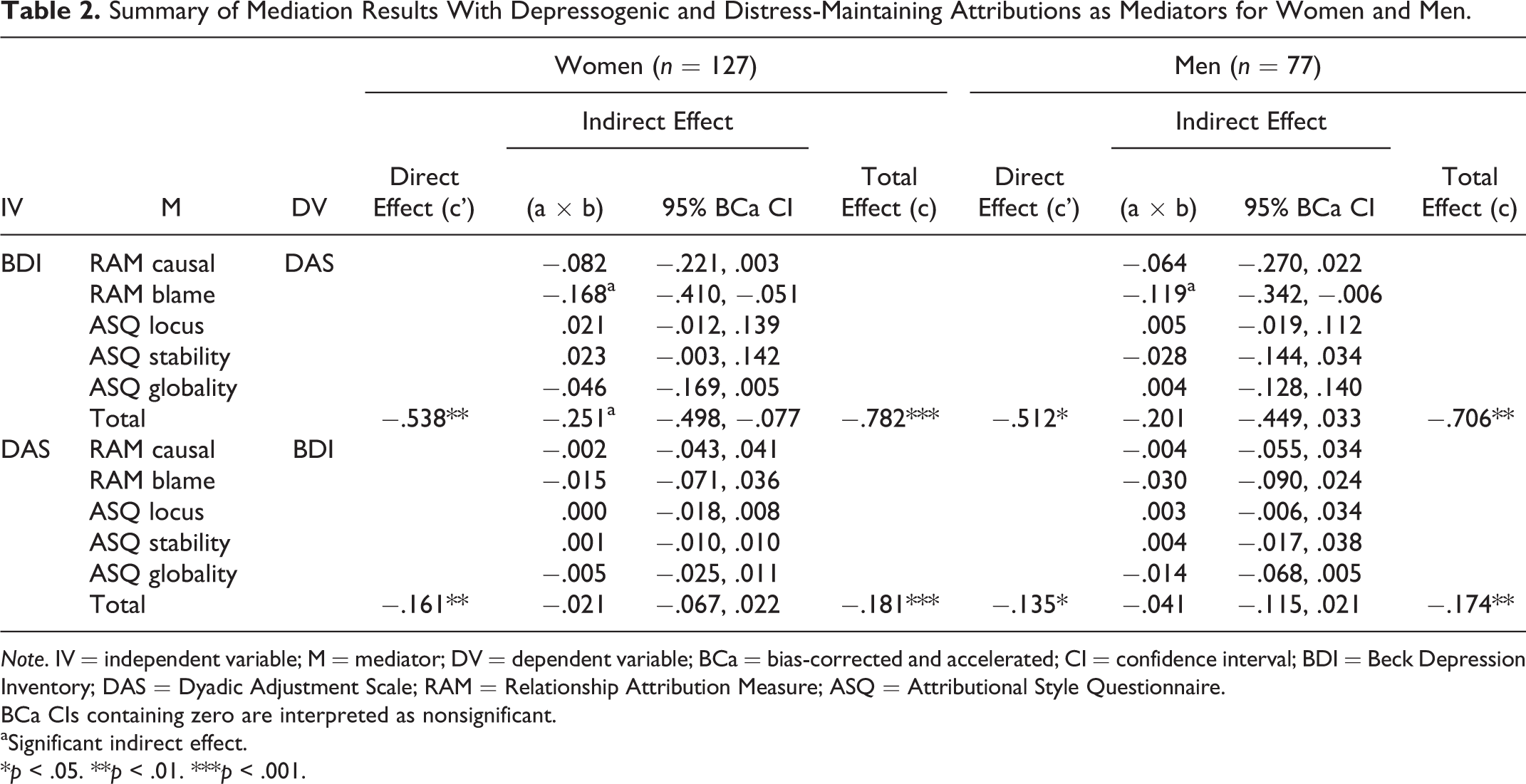
Note. IV = independent variable; M = mediator; DV = dependent variable; BCa = bias-corrected and accelerated; CI = confidence interval; BDI = Beck Depression Inventory; DAS = Dyadic Adjustment Scale; RAM = Relationship Attribution Measure; ASQ = Attributional Style Questionnaire.
BCa CIs containing zero are interpreted as nonsignificant.
aSignificant indirect effect.
*p < .05. **p < .01. ***p < .001.
For men, when the proposed attributions were considered together, neither model produced any significant mediators (see Table 2). However, in the exploration of the specific indirect effects of the first model, relationship-oriented blame attributions (RAM blame) served as a significant indirect effect, with depressive symptomatology positively associated with blame attributions for partner’s negative behavior, which in turn was associated with poorer intimate relationship functioning. None of the specific indirect effects were significant in the other model.
Discussion
The purpose of the present study was to help elucidate the role of depressogenic and distress-maintaining attributions as potential mediators of the well-established negative association between depressive symptoms and intimate relationship functioning in a sample of primarily dating undergraduate students. This was done by including both types of attributions as mediators and modeling the association in both directions (i.e., depression to relationship functioning and vice versa), for both male and female students, using bootstrapping mediational analyses.
Results partially supported our hypotheses. Although depressogenic and distress-maintaining attributions together mediated the negative association between depressive symptoms and relationship functioning for female students, they did not mediate this association for male students. Years of research examining gender differences in the association between mental health and relationship functioning have documented that the mental health of women is relatively more affected by the quality of their intimate relationships than that of men (e.g., Kiecolt-Glaser & Newton, 2001). This consistent finding suggests that the mechanisms by which these variables are associated may be different between the sexes, thus explaining the differential findings in the current study. However, the nonsignificant finding for men may also have resulted from the relatively small number of male students in the study and the low statistical power that occurred as a result.
When examining the proposed mediators independently, blame attributions (i.e., the extent to which individuals believe that their partners should be blamed for their negative relationship behaviors) mediated the negative association between depressive symptoms and relationship functioning for both male and female students. Consistent with previous research (Heene et al., 2005), depressive symptoms were positively associated with partner-focused blame attributions, which in turn were negatively associated with relationship functioning. However, in contrast to previous research (Heene et al., 2005, 2007), causal attributions (i.e., the tendency to attribute a partner’s negative relationship behaviors to stable and global causes within the partner) did not mediate the negative association between depressive symptoms and relationship functioning for either male or female students. Although the results of Horneffer and Fincham’s (1996, 1997) study suggest that both depressogenic and distress-maintaining attributions may be important when examining attributions in either depression or relationship functioning outcomes, results of the present study suggest that distress-maintaining attributions (i.e., blame attributions) may be more important than depressogenic attributions for understanding the negative association between depressive symptoms and relationship functioning, at least in this predominantly dating sample of undergraduate students.
The inconsistent findings between the present study and previous research could be partially explained by the entailment model of marital conflict (Fincham & Bradbury, 1987), which proposes that attributions of cause may lead to attributions of blame, which in turn, lead to marital distress. Previous research has supported this proposed sequence, with blame attributions mediating the negative association between causal attributions and relationship functioning (e.g., Davey, Fincham, Beach, & Brody, 2001; Lussier, Sabourin, & Wright, 1993). Following from these previous findings, causal attributions may not have been a significant mediator of the negative association between depressive symptoms and relationship functioning in the present study because blame attributions may have been more proximal to relationship functioning for this predominantly dating sample of male and female students.
Alternatively, the differential findings between the present study and previous research may also be a result of varying methodologies. For example, our sample consisted of undergraduate students, whereas other studies included older community control participants or clinical participants with significant depressive symptoms and relationship distress (e.g., Heene et al., 2005, 2007). Participants in the present study reported minimal levels of depressive symptoms and low levels of relationship distress, on average. In addition, participants in the present study were predominantly in dating relationships, and only a small percentage of the sample was married (1.5%), whereas in the other studies, most participants were married. Finally, the use of different measures for the constructs examined (e.g., the Symptom Checklist-90, Derogatis, 1977, vs. the BDI), as well as the various statistical practices that were used, may have contributed to the discrepant findings.
In the current study, the negative association between relationship functioning and depressive symptoms was not mediated by depressogenic and distress-maintaining attributions for either male or female students. In addition, no specific subscales of depressogenic or distress-maintaining attributions were found to mediate this direction of association. These results are consistent with Gordon et al. (2005), who also found that distress-maintaining attributions did not mediate the negative association between relationship functioning and depressive symptoms (depressogenic attributions were not investigated in this study). However, given that Gordon et al. found that distress-maintaining attributions did moderate the association between relationship functioning and depressive symptoms, it may be that distress-maintaining and depressogenic attributions play a different role when this association is framed from relationship functioning to depressive symptoms than when it is framed from depressive symptoms to relationship functioning. Based on the findings of the present study, it appears that depressive symptoms may increase an individual’s propensity to make distress-maintaining attributions (i.e., blame attributions), which in turn may create a stressful and nonsupportive environment that may include relationship distress.
Although this study included a nonclinical, undergraduate sample, the results have important clinical implications that may apply to individuals with clinically significant depression and/or relationship distress. Specifically, given the mediating role of blame attributions in the negative association between depressive symptoms and intimate relationship functioning for both male and female students, results of the present study suggest that it may be beneficial to target and modify distress-maintaining attributions for individuals who may be experiencing higher levels of depressive symptoms, as well as relationship distress. Similarly, results of the present study could also have important prevention implications for depressed individuals who are in satisfied relationships. Since depressed individuals are likely to struggle more if their closest relationships terminate, it may also be beneficial to target and modify any blame attributions that these individuals have in an effort to prevent their intimate relationships from deteriorating. Furthermore, given that previous research has documented that cross-spouse effects between one spouse’s blame attributions and the other spouse’s report of martial distress are of a similar magnitude as within-spouse effects (Davey et al., 2001), it may also be beneficial to include an individual’s partner in treatment to maximize the change that can be made with regard to the individual’s intimate relationship functioning. A meta-analysis found that couple therapy for depression, which targets both distress-maintaining and depressogenic attributions, was more effective than individual therapy for depression, which targets depressogenic attributions only, for reducing relationship distress (Barbato & D’Avanzo, 2008). Future studies with clinical samples are required to test these aforementioned hypotheses.
The present study had several methodological strengths, including the use of bootstrapping, which is currently considered best practice for the assessment of mediation (Preacher & Hayes, 2008a, 2008b), and testing the associations separately for men and women. In addition, following Horneffer and Fincham’s (1996, 1997) recommendation, the present study simultaneously investigated depressogenic and distress-maintaining attributions, rather than exclusively focusing on just one type. However, it also had a number of limitations. First, a nonclinical, undergraduate sample was used; thus, future studies with clinical samples who endorse significant depression and/or relationship distress are needed. Second, the relatively small sample size, particularly the low number of male students, may have resulted in low power for our statistical analyses. Therefore, future studies with larger samples should be conducted. In addition, given the minimal variation in demographics (i.e., young age of participants, relatively short duration of participants’ relationships, and limited diversity in race/ethnicity), future research could benefit from investigating the mediating role of depressogenic and distress-maintaining attributions in the association between depressive symptoms and relationship functioning with older, more diverse samples who are in longer term relationships. Third, a modified version of the ASQ was used, and the internal consistency for this questionnaire was found to be low in the present study, although similar to what previous research has found (e.g., Barnett & Gotlib, 1988). Thus, it is possible that some of the nonsignificant findings may be due to this scale’s low reliability. Future research that includes measures with greater reliability is needed to corroborate the present study’s findings. Fourth, the present study relied on the use of self-report measures from only one partner within the relationship. Future studies should use clinical interviews, as well as self-report measures in order to reduce method bias. These studies would also benefit from the inclusion of both partners. Fifth, given the cross-sectional nature of this study, future studies that utilize a longitudinal design will be required to fully understand the directionality of the association between relationship functioning and depression. Finally, this study investigated attributions as potential mediators, although it is possible that there are other third variables (e.g., conflict communication; Heene et al., 2007) that play an important mediating role in this association.
In summary, results of the present study suggest that distress-maintaining attributions may play a more important mediating role in the negative association between depressive symptoms and relationship functioning than depressogenic attributions. Specifically, blame attributions were found to mediate the negative association between depressive symptoms and relationship functioning. These results may have clinical implications for the treatment of depression and prevention of relationship distress in those individuals who are struggling with depression, and suggest that these individuals may benefit from focusing on reframing their blame attributions. By improving our understanding of the underlying mechanisms that may be mediating the relationship between these constructs, we may be able to improve treatment outcomes for depressed individuals who have varying levels of relationship distress.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.