
Abstract
Fast, effective, and accurate emergency medical treatment can save lives. Quick access to the specific equipment that emergency medical personnel need facilitates more efficacious treatment during emergencies. This project focuses on designing an improved emergency response kit for medical first responders. The kit currently in use has no organizational standard for the way the medical items it contains are placed inside. With a user-centered method, we designed a kit that better fits first responders’ requirements and found that the kit – a backpack and a vest – is both easier to use and carry, based on emergency care priorities.
Keywords
Fast, effective, and accurate emergency medical treatment can save lives. This project focuses on a user-centered design for emergency response kits for medical first responders.
Background
Prehospital Care – The First Responder
First responders are a vital part of prehospital care. As the first element in the prehospital emergency care chain, their task is to assess, report, provide lifesaving treatments, and help additional medical services personnel as they arrive at an emergency scene. Their primary focus is to initiate immediate lifesaving care for critical patients (National Highway Traffic Safety Administration, 2007). They, therefore, possess the basic knowledge and skills, and the necessary equipment, to provide lifesaving interventions before additional emergency medical service (EMS) personnel arrive (Tintinalli, Cameron, & Holliman, 2010).
Magen David Adom, the Israeli national EMS, operates a national first responders’ unit that provides the first level of response in medical emergencies, aiming to get to the patient before standard rescue vehicles arrive (“First Responders,” 2019). Each member of this unit is equipped with a unique kit containing basic first aid and resuscitation equipment and an oxygen tank. However, the bags in the current kit are bulky and unorganized in essentially one large compartment, within which items are seldom clearly labeled (see Figure 1). This can impede responders’ rapid access to equipment and can also lead to confusion, potentially harming patients (Grundgeiger et al., 2014).

First responder’s current life support emergency response kit.
As a short, out-of-hospital treatment interval can positively affect patient survival, it is critical that prehospital care be fast and effective (Feero, Hedges, Simmons, & Irwin, 1995). Administering this care should be made as simple, sustainable, and efficient a task as possible (Kobusingye et al., 2006, Chapter 68). Since motor-vehicle collision is a main cause of death among young people between 15 and 29 years old worldwide (World Health Organization, 2015), treating collision injuries is a major concern for EMS. With this in mind, in collaboration with Magen David Adom, we worked to design an emergency response kit for first responders that would improve their ability to provide effective treatment to motor-vehicle collision victims.
User-Centered Design
User-centered design is a broad term used to describe design processes in which end users influence how a design takes shape (Abras, Maloney-Krichmar, & Preece, 2004). Similarly, this design is guided by the physical and psychological capabilities of the user. It refers to the function to which the products will be put and to relevant aspects of the physical environment that may affect the user’s needs and abilities. Thus, this design approach incorporates instructions for developing all the equipment elements with which the user must interact.
In our case, the design needed to account for several characteristics inherent to this particular user experience including the following:
Design for a stressful situation: Emergency situations, such as motor-vehicle collisions, are often stressful and confusing. Such situations result in suboptimal decision-making processes both for the victims and for those who come to help them (Klein, 2011). This stress might cause first responders to fail to collect critical items from their bag when they need to perform specific clinical procedures.
Organization: Today, individual first responders organize and stock their kit in their own particular way. This arbitrary organization could cause them to lose precious time searching for an item, or recalling where they placed it.
Prioritization: Important and frequently used items should be located where they are visible, accessible, and easy to activate (van Cott & Kinkade, 1972). Therefore, equipment should be positioned according to its priority in providing treatment during emergencies.
Mobility: It is important to be able to take all necessary equipment from the vehicle to the victim in just one trip. Yet the kit should be light, comfortable, and easy to carry. A system that offers more than one transport option (backpack straps, an adjustable shoulder strap, or handles) ensures that movement will not be inhibited in any setting, whether the responder is running through an open space or moving through a crowd. Multiple transport options also provide critical backup in the event that one of the carrying methods fails on the scene.
Supplies: While the kit’s contents are not universally regulated, it should stock sufficient supplies to provide life support in the event of an anticipated type of trauma and should match the training and certification level of the first responder. The quantity of supplies is also determined by the number of expected calls and the length of time away from the first responder’s base without resupply.
Kit materials: The kit should be made from durable materials that allow it to endure the harshest conditions. Tough woven materials such as cordura (nylon), vinyl, and tarpaulin are the optimal choices for durability. These materials are abrasion resistant even after numerous washings and continuous use.
EMS recognition: Use of bright colors, reflective straps/stripes, or the universal Star of Life logo makes it easy for people to quickly recognize first responders. It may also assist in finding and collecting all the equipment after an incident.
Project Objective
The emergency response kit is the first responder’s most important tool. Our goal was not only to design a prototype for a kit that is convenient to carry and use but also to create a standard for organizing its medical items based on emergency care priorities.
We used mixed methods including focus group interviews, an internet questionnaire, and a usability test to design the guidelines and then evaluate the advantages of the new design. These methods resulted in both qualitative and quantitative data. We partially followed guidelines for qualitative research and usability testing (Tong, Sainsbury, & Craig, 2007; usability.gov, 2019).
Data Collection
Focus Group
We began the project by visiting Magen David Adom’s main headquarters, where we received an overview of the first responders’ role within the organization and the type of care they are expected to provide. After this visit, we organized a meeting with eight first responders who volunteered to participate in a focus group following a call that was distributed through internal communication channels. All participants had at least 1 year of active experience. During a session of more than 2 hours, we asked them a series of open-ended questions ranging from the general (e.g., How do you see your role in the EMS organization?) to the specific (e.g., What equipment do you use for various treatments?). After each question, we had a short discussion during which the participants offered insights from their experience, and these conversations were recorded.
To analyze the data collected during the focus group discussion, two of the authors listened to the recordings, categorizing statements to one of four themes: first responders’ role at the scene, the equipment they had, the equipment they used, or what did not work with the current kit. The themes were not identified in advance but were derived from the data. These themes guided us in understanding the challenges first responders face at an emergency scene and their approach to the equipment they carry.
The primary insights from the focus group were as follows:
The first actions that first responders take when arriving to an emergency call are donning medical gloves, putting on the first responder vest for recognition, and carrying the kit.
The handiest items in the kit are trauma shears, bandages, medical gloves, and a glucose meter.
In cases where the ambulance is close to the scene or there are already other first responders on site, it is not necessary to take the whole kit, and responders would prefer to carry only a few must-have items.
Each first responder organizes their kit in a different way. As a result, using someone else’s kit is problematic.
Even though the responders in our focus group claimed to know their own kit’s organization very well and knew the name of all the items and their use, when we asked them to use the kit and reach for a specific item, they lost time and effort searching for it.
The kit does not currently include a headlamp, and according to the focus group, this makes it difficult to work at night.
Carrying the kit with a shoulder strap or a hand strap is uncomfortable. The group proposed that the new kit be designed as a backpack.
The usability test that was done following the design phase also validated our findings from the focus group.
The current kit is presented in Figure 1. Visible items are not organized by clinical procedure; therefore, first responders must search deeper in the bag to find complementary items for specific clinical procedures.
Internet Questionnaire
After our meeting with the focus group, we used an internet questionnaire to gather additional concrete data from a large group of first responders. The combination of the two data sources helped us understand the users’ needs from varied perspectives, adding to the product-detailed design.
The short first responders’ questionnaire included the following three questions (two open-ended questions and one question where they had to choose one of three possible answers):
What are the first actions you usually take when you arrive at the scene of a motor vehicle collision and which items from your first responders’ kit do you usually use?
Which type of equipment do you find most essential for treating motor-vehicle collision victims and which items do you think are missing from the current kit?
Select the type of bag you would like to use to carry the first responders’ equipment kit: (a) a backpack, (b) a vest that includes a small backpack, or (c) the current bag. (The three options were presented using small pictures.)
A Google Forms questionnaire was sent through Magen David Adom’s first responders’ mailing list to all its members, of whom 233 answered. Their main responses can be summarized as follows:
Question #1 – Actions and items: Fifty-three respondents (36%) marked the cervical collar as the first treatment they generally apply to victims of a motor-vehicle collision. A further 33 (22%) marked taking clinical measurements such as blood pressure and heart rate as their most common first action. Another common first action cited by 29 (19.5%) was treating bleeding (hemorrhages). The equipment mentioned for taking clinical measurements were pulse oximetry and a blood pressure monitor, and for treating bleeding, they noted triangular bandages, medium wound dressings, gauze sponges, and tourniquets.
Question #2 – Necessary equipment: The equipment marked as most needed were bandages 70 (29%), a cervical collar 67 (28%), triangular bandages 26 (11%), and tourniquets and blood pressure monitors, both with 15 responses (6%).
Question #3 – Equipment carrying preference: Forty-three percent wanted to carry the equipment in a backpack and 22% preferred a vest.
Drawing Conclusions from the Data
We used the data we collected from the focus group and the internet questionnaire to support our new design effort. First, we had to define the kit structure. The questionnaire showed that more than 65% of the first responders wanted to change the way the kit was structured. Since placing all the equipment in a vest was not possible, a new kit structure had two options: (1) to replace the current bag with a backpack or (2) to replace the current bag with a combination of a backpack and a vest. To compare these two options with the current bag, we considered a list of scenarios that was mentioned by the first responders during the focus group discussion. For each scenario, we evaluated how the first responders’ access to the equipment item during motor-vehicle incidents would be affected by its placement in each kit structure option. The combination of a backpack and a vest was the only option that was preferable or equally preferred for all scenarios. This was mainly because this option allows direct and quick access to all the items that are necessary for immediate response – most from the vest. Having all the equipment in a bag offers reduced accessibility to immediately needed items. Therefore, we concluded that the most effective storage option would be the combination of a vest and a backpack.
Another concern was that in the current bag, the frequently used equipment does not have a defined place. First responders usually put these items in one of the pockets in the outer bag, which makes locating it confusing as there are several pockets located there. Most of the equipment is located in one large compartment, within which items are seldom clearly labeled. The combination of a vest and a backpack, on the other hand, would offer flexible organization optimized for priority, clinical procedures, and frequency of use. Equipment for immediate use could be located in the vest, and other items could be grouped by use during clinical procedures in dedicated cases within the backpack’s main compartment, where they would not be quickly accessible if needed. For example, one way equipment could be distributed is – Bandages: one bandage kept handy for immediate application in the vest, while the rest would be placed in a dedicated case in the backpack; Cervical collar: placed in the vest back pocket, so it is handy for immediate application; Triangular bandages: several bandages kept in the vest and the rest in a dedicated case in the backpack; Tourniquet: placed in the vest front pocket, accessible for immediate application; Blood pressure monitor: placed in a dedicated case in the backpack’s main compartment.
Considering additional equipment that needs to be available such as medical gloves and a two-way radio device would also favor the combination of a vest and backpack since the vest provides good storage for small components, and it keeps them very handy in any usage scenario.
Design Guidelines
Based on all the information we collected from the first responders, conclusions from our previous studies (Bitan, Ramey, & Milgram, 2019), and the suggested structure of the vest and backpack, we defined parameters to guide the design of the new kit.
Equipment Organization
The most commonly used items will be in the vest. Placing them here will also ensure that the first responders have them even if they choose not to carry the entire kit.
All the items in the backpack will be grouped by category, placing each category in a separate case. Grouping was determined by items used during clinical procedures and was informed by feedback from the focus group.
The backpack will open in a way that will allow direct access to all the cases.
When the first responders need equipment for a specific procedure, they can open the case and have all the equipment they need. This method is more efficient than the current organization where the equipment is in a common compartment, and first responders need to find and “collect” the necessary items for a procedure.
Each case will have a distinct color to help first responders quickly identify the case they need (Dzulkifli & Mustafar, 2013; Farley & Grant, 1976).
Each case will also be clearly labeled with the name of its category. This will compensate for the possibility of color blindness and for situations in which colors are hard to see (e.g., at night). The labels will also allow first responders who have less experience using the kit to easily identify each case without trying to remember the coded meaning of different colors.
The text on the label will have high contrast with the background, and the font size will allow it to be read from 2 meters away. This will ease searching for the right label even when the cases are on the ground and the first responder is standing.
Name labels will be placed in transparent holders, making the case name both visible and easily changeable.
Each case will have a dedicated location inside the backpack and be attached with Velcro™. A handle will make it easier to withdraw the case from the backpack.
Materials
The vest will be made from a breathable cloth that wicks moisture away to improve overall comfort.
The backpack will be made from a durable and waterproof fabric, suited to extreme environments and easy to clean.
Recognition
The kit color will be orange-red, an easily visible color identified with the EMS organization.
Reflective straps will be added to both the backpack and the vest to make first responders more visible at night.
A headlamp will be added to the kit and placed in the vest. This will make first responders more visible and help them to see better in the dark.
Detailed Design
The design guidelines for the vest and backpack were translated into detailed instructions for manufacturing. The design dictated the placement of all items, defining a binding standard for how to organize the kits across the organization.
The Vest
Since the vest’s lower pockets are more accessible, the most commonly needed items are placed there, with the most needed items located on the right-hand side since most of the population is right-handed. The items and their location are detailed in Table 1. The equipment location is also marked in Figure 2.
Equipment Items and Their Location in the Vest
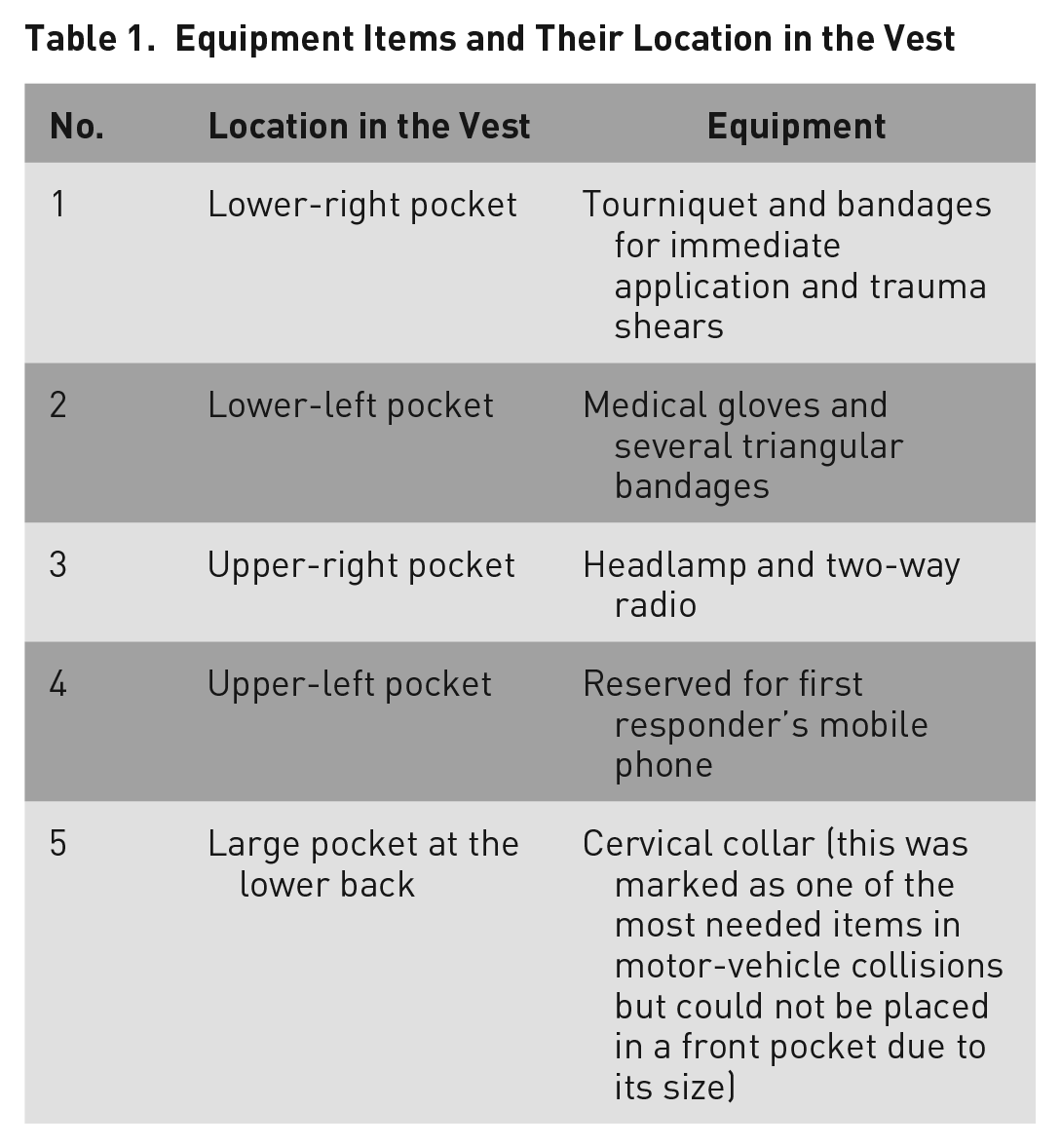
The EMS organization should consider adding pulse oximetry and a glucose meter to the vest’s inventory.
Even though the first responders noted that a blood pressure monitor is an item they use frequently, we recommend locating it in the backpack and not in the vest since it is heavy and bulky.

The vest.
The Backpack
The items that need to be placed in the backpack were grouped by their use during clinical procedures; each group was placed in a dedicated case with a distinguishable color. After grouping the items into cases, we measured the cases and placed them in the backpack according to the following guidelines:
The backpack will open like a clam shell, exposing all the cases. Thus, when the first responder opens it, all the equipment will be directly accessible.
The cases will be distributed in the backpack in a way that keeps it balanced and, therefore, easy to carry.
The backpack can be carried in two ways: by hand with handles or on the back with backpack straps.
A sketch of the cases in the backpack is presented in Figure 3, and the final backpack is presented in Figures 4 to 6. These figures present the standard way the kits will be placed in the bag.
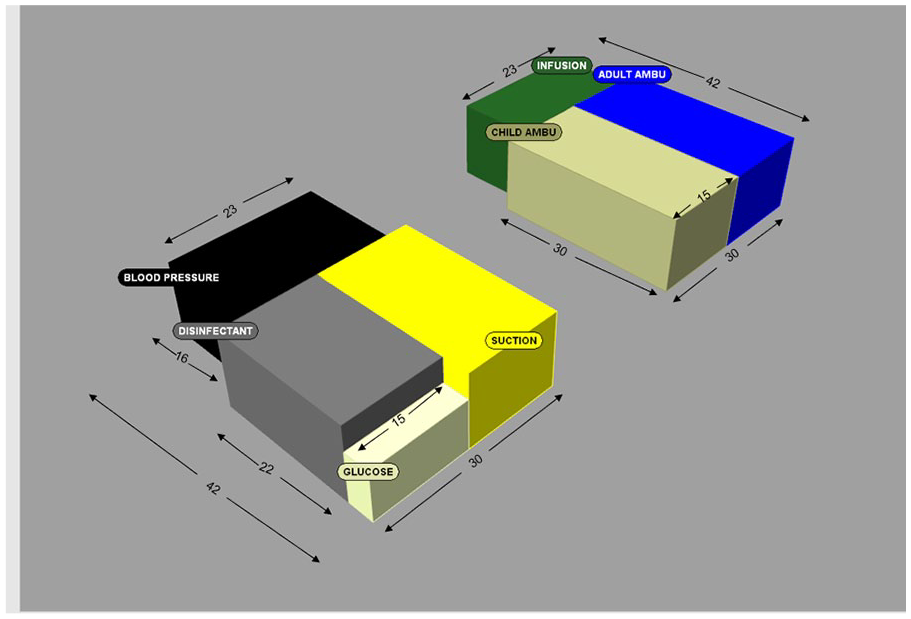
Sketch of the cases in the backpack (units in centimeters).

Front of the backpack.

Back of the backpack.

The opened backpack and all its cases.
Usability Test
The first responders’ procedures are simple; each involves only a few equipment items. Therefore, the usability test goal was to evaluate the overall performance through the first responders’ experience rather than to capture specific errors or to record access time to each item.
We created a prototype of the entire kit (vest and backpack) and tested it for ease of use with a group of six EMS first responders who had at least 1 year of active experience and who volunteered to participate in the usability test following a call that was distributed through internal communication channels. The participants were introduced to the new kit design and had some time to try it before they were briefed on the scenario they were about to simulate. The scenario was a simple simulation of a victim in a motor-vehicle collision who was suffering from intensive bleeding from one leg and had a head and neck injury. As the goal was to test the new kit’s usability and not clinical procedures, the first responders were instructed only to grab the equipment they needed to use and not to provide the actual clinical care. Each participant arrived in their own vehicle to the simulated scene, removed the kit from the car trunk, and hurried to the victim, who was sitting in the driver’s seat of their car. The simulation was repeated three times, each with a different set of equipment: only with the vest, only with the backpack, and with the entire kit (the vest and the backpack). Figure 7 presents a first responder during the simulation. After each simulation, the participant was asked to provide feedback on the kit’s usability through a short, structured interview. The qualitative data that were collected included feedback about pathways they took, problems they experienced, and recommendations and comments regarding the new design. Two of the authors analyzed the verbal responses, categorizing statements to six main themes. The themes were not identified in advance but were derived from the data. Highlights from this feedback is presented below.
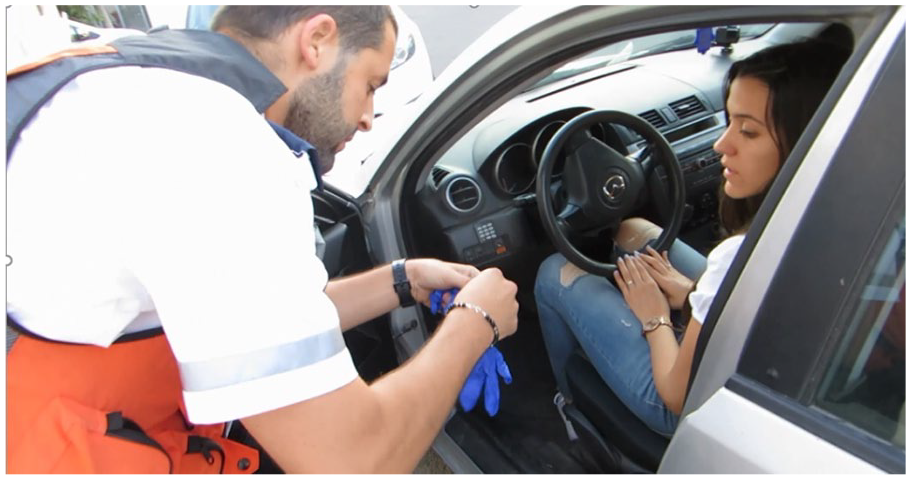
The first responder talks with the casualty while wearing medical gloves taken from the vest.
Usability Test Result
The combination of vest and backpack worked well for the first responders – the items required for the first actions when treating a motor-vehicle collision are in the vest and, therefore, easily accessible.
The vest and the backpack were comfortable to transport. The backpack’s weight is equally distributed on the first responder’s back. In addition, while carrying the backpack on the back, the first responder’s hands are free for other actions – for example, transporting the casualty.
The combination of vest and backpack gives the first responder the option of wearing only the vest to the scene. Today, in some cases, the first responders arrive on the scene without the kit. The new kit design allows them to take the vest and leave the backpack in the vehicle. After they finish evaluating the scene, they can instantly start providing immediate care to casualties using the materials in the vest.
The cases in the backpack, categorized by treatment type, allow first responders to provide treatment without searching for the relevant items in different pockets. Responders can also withdraw the case in a single movement instead of searching for and removing multiple items.
Despite the fact that the first responders used the prototype kit for the first time, they used it properly. The color and name label helped them to immediately recognize the relevant case without error.
The headlamp was accessible, and the first responders acknowledged the advantage of locating it in the upper part of the vest.
Conclusion
Currently, there is no standard for first responders’ emergency response kits. Each individual in an EMS organization packs their kit in a different way. In this project, we created a prototype kit (vest and backpack) that was designed based on information we collected from first responders. A small-scale usability test highlighted the advantages of the new design.
The new design can serve as a standard solution for first responder kits. The main concept of separating the equipment between a handy vest and a backpack that is organized with dedicated cases where items are grouped according to their use during clinical procedures might also be applicable to other health care domains. Our study focused on motor-vehicle collisions and the simple procedures first responders provide in these situations. Future research might look at the way experienced paramedics work in more complicated scenarios. The design principles implemented here could be used to design bags in other EMS areas, but more elaborated usability tests might be necessary.
Footnotes
Acknowledgements
The authors would like to thank Ela Liberman Pincu for her assistance in the detailed design, and all the first responders who shared their knowledge and experience with us.
The study was supported by the Israeli Research Fund of Insurance Matters.
![]() .
.