
Abstract
The modern hospital bed is a sophisticated medical device, and its users represent a diversity of abilities and needs. To develop a new bed, Hill-Rom studied these users in nearly 500 hr of observation across 29 hospital units. Focus groups were used to evaluate early concepts, and formative usability testing included over 130 users to evaluate design prototypes. This research and testing resulted in the development of the Centrella bed, which includes new features to address patient satisfaction, patient safety, and caregiver efficiency. The resulting design is the winner of the 2017 Stanley Caplan User Centered Design Award.
Keywords
Considering changes in health care legislation and patient and staff wellness, a redesign of traditional hospital beds could transform overall hospital care.
Over the past two decades, great upheaval in the health care industry has presented numerous new challenges for hospitals. In 2007, the Centers for Medicare and Medicaid Services (CMS) announced Medicare will no longer pay for additional costs of preventable errors, including “never events” (e.g., patient falls, pressure injuries, hospital-acquired infections; Agency for Healthcare Research and Quality, 2017). The Hospital Consumer Assessment of Healthcare Providers and Systems Survey, a standardized survey instrument in use since 2006, became tied to reimbursement reductions if scores were not collected and reported. This public reporting also had the effect of driving competition among hospitals for patients (Geiger, 2012). Reimbursement challenges together with the Great Recession created cost pressures that forced hospitals to find new ways to deliver care more cost-effectively. To meet these demands, requirements for patient care changed as higher-acuity cases were moved to non–critical care units and more initiatives attempted to reduce length of stay (L.E.K. Consulting, 2012). During this period, technologies like touch screens became more cost-effective, and patient expectations evolved based on their personal experience with consumer technologies (Deloitte Consulting, 2012).
Amid the political and economic changes in health care, high rates of musculoskeletal disorders among caregivers have continued to plague health care facilities. In 2016, nurse assistants ranked second and nurses ranked sixth for occupations with the greatest number of musculoskeletal disorders (Bureau of Labor Statistics, 2016). These injuries are associated with manual patient-handling activities, which are commonly performed in or near the bed (Marras, Davis, Kirking, & Bertsche, 1999), and may also result from moving occupied beds or stretchers (Wiggermann, 2017).
The decision to design a new hospital bed, which would be named Centrella™, was primarily motivated by these evolving conditions in the health care sector and unmet needs in facilities. The redesign allowed for the consideration of external technological advancements, such as microprocessors, touch screens, and new user interfaces. A redesign also provided the opportunity to incorporate internal advancements, such as frame designs that minimize patient migration (Davis & Kotowski, 2015) and improved technology intended to reduce risk of pressure injuries. Additionally, the project addressed evolving standards (i.e., ANSI/AAMI HE75:2009; Association for the Advancement of Medical Instrumentation, 2009; IEC 60601-2-52; International Electrotechnical Commission, 2009; IEC 62366; International Organization for Standardization, 2015) as well as draft guidance from the Food and Drug Administration (FDA) regarding Human Factors and Usability Engineering (FDA, 2016).
Development Process
Intended users
A particularly unique challenge for designing a hospital bed is the diverse needs and capabilities of its users. The Centrella bed was designed for use in medical-surgical units (med-surg), intensive care units (ICU), and long-term acute care units. Targeted users for this bed included patients, nurses, nurse assistants, housekeeping staff, biomedical technicians, and physical therapists. Physical capability, cognitive state, and level of education vary greatly across these groups. Furthermore, diverse activities are performed when using the bed that include eating and sleeping, cleaning and disinfecting, repairing, positioning for therapy, positioning for patient comfort, weighing patients, transporting a patient throughout the hospital, or performing emergency procedures such as CPR or intubation. Ease of use and intuitive design were especially important because of this diversity and because health care facilities often do not provide training for hospital beds.
Contextual inquiry
The contextual inquiry or “immersion” process at Hill-Rom places development teams in environments and situations that will help them better understand the reality of clinical practice, work flow, and patient experience. The goals of this process are to collect evidence for the identification of needs and design requirements.
Sites for the immersion related to this project were selected to represent the range of facility types and care environments that the product would serve. Between March and November 2013, a total of 495 hr of observation occurred across 29 units in seven hospitals in North America. Immersion was arranged only at facilities that allowed the project team to take photos and record video, including of patients and caregivers who provided written consent. Health care staff included in this research were nurses, care technicians, transporters, housekeepers, health unit coordinators, monitor technicians, patients, patient families, lab technicians, clinical engineering staff, information technology staff, and administrators. Thirty Hill-Rom staff participated, including engineers, ergonomics specialists, industrial designers, market researchers, the product manager, and clinical consultants. After this initial effort, other ad hoc supplemental activities were conducted to explore specific topics.
In addition to immersion activities conducted in the clinical environment, hundreds of individuals participated in quantitative and qualitative research to evaluate design concepts and prototypes. Participants included patients, clinical staff, and other staff involved with procurement decisions (e.g., nurse managers, directors, physicians, C-suite executives, procurement leaders, and directors of quality).
Photos, videos, and notes collected during the immersion process were synthesized to reveal several themes of unmet needs of caregivers and patients. One clear theme was the rapidly increasing importance of patient satisfaction. To improve patient satisfaction, hospitals are rethinking nearly every aspect for how they provide care, which also affects their selection of equipment. A strong focus on patient safety was consistent across facilities and remained the primary consideration when evaluating equipment or care practice. Finally, cost pressures and patient acuity levels continue to strain caregivers’ time, meaning very little tolerance for equipment or procedures that require extra time or training to use.
Design constraints and considerations
Numerous design constraints were observed for the Centrella bed to be compatible with diverse hospital environments across various health care facilities. The Centrella bed needed to provide clearances to be physically compatible with devices such as patient-handling equipment, overbed tables, and portable X-ray machines. Attachment points were needed for traction equipment, oxygen tanks, IV poles, sequential compression devices, optional mattress replacement systems, drainage bags, and patient restraints. The bed needed to fit in the elevators, doorways, and smaller rooms in older health care facilities. Centrella also needed to communicate with a variety of nurse call systems and adopt displays and icons that were consistent with similar products.
The Centrella bed is compliant with IEC 60601, Medical Electrical Equipment, Part 2-52: Particular Requirements for the Basic Safety and Essential Performance of Medical Beds. This technical standard is developed by experts in the field of medical device design, is updated periodically, and is accepted by regulators in most countries. The standard outlines safety-critical design requirements, essential performance elements, and test methods for validating the design. Significant considerations in the standard include requirements for side rail and deck design to prevent patient entrapment, structural stability and balance, electrical safety, and clearances to prevent pinching or collision with user fingers and appendages.
Some design requirements were in direct conflict with each other, such as the need for the bed to travel low to the floor for shorter patients while meeting other objectives for side rail design. IEC 60601-2-52 dictates a minimum side-rail height, so if the bed travels too low, the side rails will interfere with the back of the patient’s thighs when side sitting. Furthermore, a bed that is too low can be difficult for taller patients to egress and can present a fall risk to patients returning to bed (Merryweather et al., 2015). The design team used simulation, human testing, and clinical focus groups to identify the optimal design in these circumstances.
Usability testing
In addition to mechanical and electrical testing, usability testing was performed throughout product development. Over 20 formative usability studies were conducted across four stages of design prototypes. These studies included over 130 nurses, nurse assistants, transporters, patients, physical therapists, respiratory therapists, physicians, and biomedical technicians, who collectively provided over 400 hr of feedback. Environments simulated included med-surg, ICU, long-term care, and hallways for transport. Electronic interface simulations helped identify potential usability issues before the interface was even programmed. Results from simulated use and usability testing improved controls, side rail designs, labels, instructions for use, visual and auditory displays and alerts, and the graphical user interface. For example, some formative testing occurred in dimly lit rooms simulating nighttime patient egress and ingress. Clinical consultants, designers, and engineers observed how test participants interacted with the bed in little- to no-ambient-light scenarios. These tests contributed to several safety advancements in the areas of nightlight and side rail performance in low-light environments.
Some formative usability studies concerned many parts of the bed, whereas others were conducted to test specific questions that arose during development. In another example, a design change to the head section of the bed was evaluated to confirm there was sufficient access to the patient to perform intubation. Testing included 10 nurse anesthetists who regularly intubate patients, who provided feedback while performing simulated intubation tasks. When the design was finalized, summative usability tests were performed. Preliminary field evaluations also occurred at three hospitals.
Anthropometry
The anthropometry of patients and health care workers affected many elements of the bed design, but most available anthropometric data sets are limited in their applicability to design. For example, ANSUR (Gordon et al., 1989) is a large data set of over 100 attributes but includes only a military population, whereas the National Health and Nutrition Examination Survey (Centers for Disease Control, 2018) studies a civilian population but includes relatively few attributes. Due to the lack of relevant data, Hill-Rom worked with Anthrotech (Yellow Springs, OH) to develop more representative anthropometric percentile estimates for the user population.
Selected Design Elements Resulting From Development Process
Fall prevention
A patient fall prevention program was consistent across all patient safety initiatives observed by the development team. Patient falls are a concern not only for patient well-being but also for hospital finances, with falls becoming a key indicator of hospital quality and the treatment of related injuries not reimbursable under current CMS guidelines. These guidelines govern how hospitals are reimbursed for patients with Medicaid and Medicare, who constitute more than half of the patients in U.S. hospitals. To address this challenge faced by facilities, the Centrella bed includes features designed to reduce patient falls and fall-related injury.
Patients requiring assistance typically use the nurse call feature to request help. Often, for a variety of reasons, the nurse call can be disconnected or not functional, and when this occurs, the status is not communicated to the patient. Patients may continue to press the nurse call button in a vain attempt to get assistance. When there is ultimately no response, some patients may try to get out of bed independently, which can result in a fall injuring the patient. To address this risk, the Centrella bed utilizes an industry-first “dead-front nurse call button” (Figure 1). A dead-front design consists of a membrane panel with a button or indicator that is not visible until illuminated. Centrella recognizes whether the nurse call is connected, and if so, the button is illuminated and visible to the patient. If the nurse call is not functional, the button is not displayed to avoid confusing the patient. However, if it is illuminated, patients or caregivers who have activated nurse call can be confident that their call was placed.
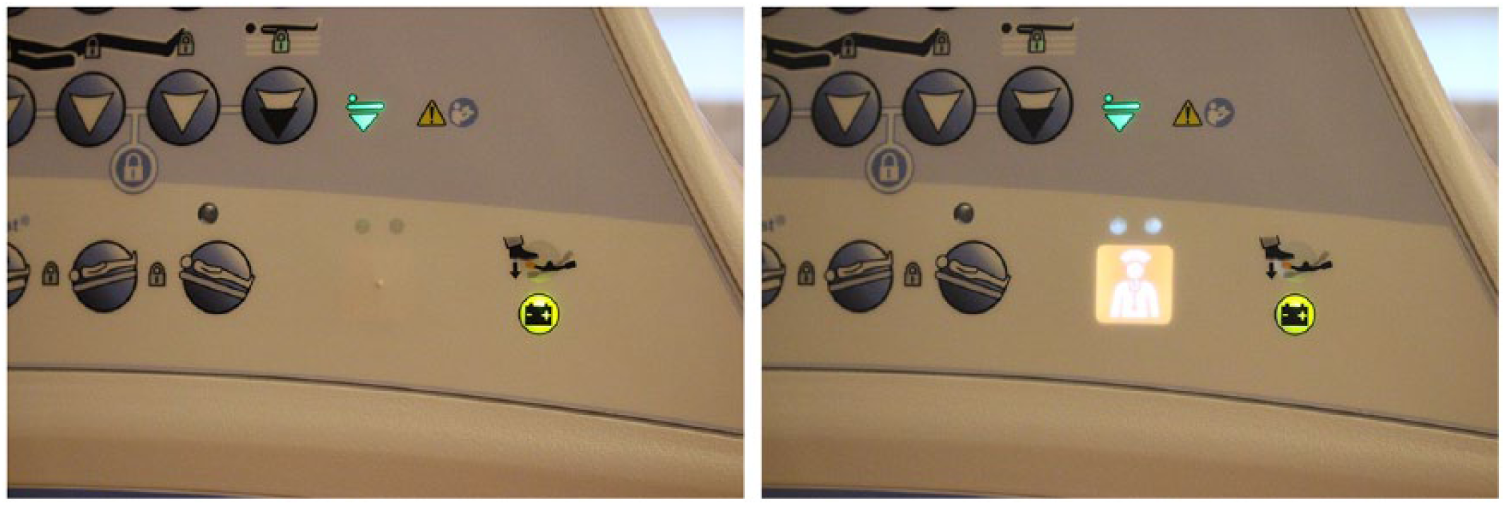
Intelligent nurse call button becomes visible only when the bed is connected to a functioning nurse call system. This feature prevents the patient from mistakenly believing a request for help has been placed when it has not.
To reduce the risk of falls during low-light conditions, the Centrella bed development team created the IllumiGuide handgrip. The IllumiGuide handgrip is a lighted side-rail grip that glows a soft blue, providing an easy visual reference to the patient where to place his or her hand while egressing or ingressing. Complementing the IllumiGuide handgrip is a new advanced night-light that brightens during ingress and egress to illuminate the area around the bed as the patient moves to and from the bathroom or bedside chair (Figure 2).

IllumiGuide Siderail Handgrip (top) provides illumination and a guide for where patients can grip the bed when entering or egressing the bed. Enhanced night-light (below) lights the area around the bed to guide egress and return to bed from the bathroom and dims when the patient is in bed and still.
The Centrella bed includes a bed-exit alert system that, when enabled, alerts staff to patients attempting to egress without caregiver assistance. Although this feature is available on many products, the development team leveraged customer feedback and usability testing to address safety-critical errors that occurred during its use. For example, caregivers often disable the bed-exit alert for many care activities, including assisting the patient to the bathroom, repositioning the patient in bed, or performing physical therapy. Afterward, caregivers commonly forget to rearm the system. The Centrella design team developed a system that allows caregivers to suspend the bed-exit alert with an “auto-rearm” when the patient returns to bed. Caregivers can use 1- and 5-min “suspend” time-outs to prevent unwanted bed-exit alerts while also preventing the need to remember to reenable the system. After the patient care, Centrella automatically rearms the bed-exit system.
Observation in the clinical environment and focus group feedback showed that many caregivers were confused or overwhelmed by bed displays that often communicated complex or important status information using cryptic combinations of icons and small LED lights. These indicators were often overlooked, resulting in a misunderstanding of the status of the bed. SafeView lights on the Centrella bed were developed to better communicate important safety-related status information. The SafeView system consists of indicators in the foot section and light projections onto the floor that clearly display the status of the bed-exit alert, bed height, and side rail protocol compliance (Figure 3). These projections allow caregivers to easily see the status of Centrella’s safety features from the hallway, including in dual-occupancy rooms with curtains drawn.

SafeView projection lights allow caregivers to see the status of safety-critical components (e.g., bed-exit alert, bed in low position, and side rail position) at a glance, even from the hallway.
Line management
The management of electrical cords and fluid lines is a continual challenge for both caregivers and patients. During interviews, patients commonly complained of tangles of lines. Caregivers described lines getting caught in side rail mechanisms, getting snagged on the bed and pulled out of patients, being occluded, and even getting tangled around patients. To address this, Centrella’s headrail features a specially molded shape that is intended to help caregivers safely position cords and lines (Figure 4). This feature is designed not to grab lines but simply to allow them to lie safely across the headrail, thus keeping them from being damaged by the side rail mechanism or tangled with the patient. This design also means that the lines are free to move with the patient when they egress from the bed.

Patient pendant that has fallen out of reach (left). Awkward reach for a patient to the controls in the side rail (center). The Centrella pendant design (right) includes attachment points that make controls easier to reach and prevent the pendant from falling or getting lost in the bedsheets.
Patient experience
With contextual inquiry revealing the increasing importance of patient comfort, over 300 hr of comfort testing of over 50 subjects across three waves of testing were performed to evaluate iterations of prototypes. These tests benchmarked the evolving design prototypes to existing Hill-Rom products and competitors. For the first time on an air-powered therapeutic mattress, the patient controls on the Centrella bed allow patients to adjust the firmness of the mattress. The range of adjustment does not allow pressures to exceed limits that could increase the risk of pressure injury, and the adjustment can be disabled by the caregiver.
Patients that slide down in bed have less torso elevation, which can increase risk of ventilator-acquired pneumonia (Wiggermann, Kotowski, Davis, & VanGilder, 2015) and require repositioning by caregivers, which is associated with risk of caregiver injury (Marras, Davis, Kirking, & Bertsche, 1999). When testing Centrella, the design team used Hill-Rom’s motion capture lab, mirroring methods from previous collaboration (Kotowski, Davis, Wiggermann, & Williamson, 2013) to minimize the migration that resulted from articulating the bed.
To promote patient independence and reduce patient handling, the shape of the side rail was carefully studied and iterated to assist patients when repositioning themselves in bed. Several grip points on the upper side rail are available for patients to use to move within the bed (Figure 5). The length and location of the side rail is designed so that the pivot of the bed matches the bend of the hips. This increases the likelihood that when getting into bed, the patient is positioned properly along the length of the bed.

The line manager provides catch points at the top of the side rail that are intended to allow lines lie without sliding off, catching, or kinking (a). Grip points are available at the top of the side rail (a) and cut into the side rail higher (b) and lower in the bed (c, d) to help patients turn or reposition themselves up in bed. A USB port is also standard for charging personal electronic devices (e).
Ethnographic research and patient interviews revealed that patients often struggle to operate the controls of the bed, which increases their reliance on caregivers. Patient controls are usually placed on the inside of the upper side rail and are very difficult for patients to reach, requiring contortion of the arm and awkward line of sight (Figure 4). Some hospital beds have attached pendants to control the bed, but they commonly are buried in the sheets or fall on the floor. To address this issue, a standard patient pendant was developed with attachment points around the bed, including at the lower side rail, where the patient can easily reach.
During immersion, the Centrella development team saw a trend of patients increasingly relying on personal electronic devices (PEDs). Patients are bringing their cell phones and tablets to the hospital, and these PEDs are important for providing entertainment and maintaining connections to friends and family. This trend was observed across all segments of the population. Furthermore, caregiver interviews revealed that these devices were increasingly responsible for patient falls. Because of inadequate charging solutions, patients were putting themselves at risk reaching or exiting the bed to charge and retrieve their devices. To address this patient safety and patient satisfaction concern, the Centrella bed includes a built-in USB charger in the patient headrail (Figure 5) to allow patients with limited mobility to charge and continue using their PEDs.
During immersion, the development team observed that patients often lacked an adequate location to store their urinals, so many patients place used urinals beside their food on the overbed table. This situation presented an infection control risk and may also have negatively affected patient satisfaction. The Centrella team created a designated area on the side rails with special notches to accommodate many different-sized urinals (Figure 6). In addition to reducing the risk of infection to the patient, this feature also reduces the chance that the urinal could accidently be knocked over.

Urinal holders are placed in many locations, including on cluttered overbed tables (left). This inspired the urinal holder on the Centrella bed inset into the side rail (right).
Patient handling and transport
Caregiver observation and feedback has shown that caregivers are resistant to using any feature that requires extra steps or time, even when such features reduce the physical stresses on the body. Consequently, a major objective of the Centrella development team was to provide assistive features designed to be simpler and faster than previous designs. Turn assist, a feature that partially rotates the mattress to help caregivers turn patients (Wiggermann, 2016), was redesigned to actuate in less than 30 s, compared to from over 1 min with other designs.
Other features were designed to reduce the physical stresses on the body when transporting patients in the bed, a task that was associated with increased risk of injury. The IntelliDrive system consists of a powered fifth wheel that provides assistive force commensurate with user push or pull forces measured by force gauges in the push handles. Other than squeezing either handle to activate a “dead-man switch,” which is a safety mechanism required to operate the power drive, the user does nothing differently than on a bed without power drive. On similar products, these powered drives have been shown to reduce push and pull forces (Wiggermann, 2017) and spine compression loads (Davis, Kotowski, & Marras, 2011). The size of the IntelliDrive system was reduced compared with earlier designs to allow lift equipment and overbed tables to more easily move under the bed (Figure 7).

Close-up of the power drive wheel disengaged (left) and engaged (right).
A hospital ergonomist advisory board provided feedback that handles of previous products were too low for taller users, so a study was performed to evaluate ideal and acceptable handle heights when pushing (Zhou & Wiggermann, 2017). The findings indicated that the range of acceptable push heights for shorter and taller individuals do not overlap, suggesting that a fixed push height cannot accommodate all users. As a result, transport handles were oriented vertically to accommodate the preferred grip height for shorter and taller users (Figure 8).

Push handle with universal grip design accommodates shorter and taller caregivers while keeping wrists in neutral position (left). Handles fold down without extending beyond the edge of the bed (right).
Centrella is equipped with a Boost feature that places the bed in the Trendelenburg position (i.e., tilts backward) and provides additional inflation to the air mattress with a single button press. This position is designed to reduce the physical requirements of caregivers when repositioning patients up in bed. These assistive features, such as Boost, turn assist, and IntelliDrive, can reduce the cumulative physical stresses on caregivers and may be part of a broader strategy to the reduce risk of musculoskeletal injury in caregivers.
Product Release
After approximately 3 years of development, the Centrella bed was released in late 2017. Nearly a year after release, sales have been strong and customer feedback has been positive. From its inception, the new contextual-inquiry process and expanded user testing was supported at all levels of management and promoted by the chief technical officer. However, the success of Centrella has validated the importance of these process improvements and helped to ensure that these enhancements are a permanent part of the company’s product development process. Much of the success of the contextual-inquiry process was afforded by the close relationship between Hill-Rom and its customers that has grown over many years. Furthermore, the legal agreements governing the user research took many months to negotiate. Practitioners planning user research in the health care setting should be aware that customer relationships need to be developed and maintained far in advance of a product development schedule. This customer input is not merely helpful but essential in designing a product that addresses the needs and surpasses the expectations of patients and caregivers.
Footnotes
The authors prepared the work as employees of Hill-Rom.