
Abstract
Negative cognitions play a key role in the development and maintenance of depression. To reduce depressive symptoms, most interventions either encourage adolescents to change negative cognitions, theorizing that the presence of negative cognitions underlies depression, or to acknowledge negative cognitions, theorizing that one’s reaction to negative cognitions underlies depression. We compared these two therapeutic strategies in a multilevel meta-analysis of the effects of changing versus acknowledging cognitions on adolescent depression. We searched three databases in June 2022 and identified 104 randomized controlled trials (335 effect sizes). The sample comprised 27,978 adolescents (sample mean age 14−18 years) with all levels of depressive symptoms (Mage = 15.6 years; 63% female; 65% ethnic majority). The overall effect of interventions on depression was small (d = 0.21, p < .001). We found no evidence that either strategy was superior to the other. Strategies to acknowledge (d = 0.23, p = .016) or change cognitions (d = 0.20, p < .001) both reduced adolescent depression. Our findings suggest, though based on self-reported outcomes, that both strategies are effective in reducing adolescent depression, which allows for flexibility for clinicians and patients. The next step to further understand these strategies is to scrutinize the relative effects of single versus combined approaches to change and acknowledge negative cognitions.
Affecting around 280 million people, depression is one of the most prevalent and debilitating mental health disorders in the world (Reynolds et al., 2012; Stanaway et al., 2018; World Health Organization, 2021). Adolescents are especially at risk for (lifelong) struggles with depression because depression typically manifests itself for the first time in adolescence (Davey et al., 2008; Hankin et al., 1998) and depression in young people tends to be recurrent and persistent—with recurrence rates up to 70% in adulthood (Harrington & Dubicka, 2001). Depression is maintained by negative cognitions such as automatic negative thoughts, critical self-evaluation, and the tendency to focus on failures (David-Ferdon & Kaslow, 2008; Driessen & Hollon, 2010; Hofmann et al., 2012). Most established therapeutic strategies target these negative cognitions, yet they adopt meaningfully different strategies for how adolescents can deal with these cognitions to relieve their depressive symptoms. Some therapeutic strategies focus on changing, while others focus on acknowledging negative cognitions. In the present meta-analysis, we will examine which strategy is more effective in reducing depression in adolescents.
Changing Negative Cognitions
Cognitive behavioral therapies such as cognitive behavioral therapy (CBT) focus on changing negative cognitions. These are also referred to as traditional CBT (S. C. Hayes, 2004). Strategies to change cognitions are based on the premise that the mere presence of negative cognitions contributes to developing and maintaining depression (Clark & Beck, 2010; Driessen & Hollon, 2010). These strategies seek to eliminate negative cognitions through cognitive restructuring—a technique in which individuals are enabled to (a) recognize negative thinking patterns, (b) incorporate more beneficial cognitions, and (c) counteract the original negative cognition (D. A. Hope et al., 2010; Quilty et al., 2008). Correcting negative cognitions may alleviate depressive symptoms by reducing the distress and low mood that follow from negative cognitions (Hofmann et al., 2012). There is sound empirical evidence that programs that promote changing cognitions reduce adolescent depression (March et al., 2004; Weersing et al., 2006). For example, Stice and colleagues (2008) found that a 6-week cognitive behavioral prevention program is more effective in reducing depressive symptoms of high-risk adolescents than a supportive-expressive group intervention: The cognitive behavioral program was moderately effective (d = 0.44). The supportive-expressive intervention was significantly less effective (d = 0.28).
Acknowledging Negative Cognitions
Acceptance and Mindfulness Based Therapies such as Dialectical Behavior Therapy (DBT), Mindfulness-Based Stress Reduction (MBSR), or Acceptance and Commitment Therapy (ACT) focus on acknowledging negative cognitions (Nilsson & Kazemi, 2016). These are also referred to as third-wave CBTs (S. C. Hayes, 2004). Strategies to acknowledge cognitions are based on the premise that depression is not induced by the presence of negative cognitions per se but by how one relates and reacts to negative cognitions (Bishop et al., 2004; S. C. Hayes, 2004; S. C. Hayes et al., 2006). These strategies seek for individuals to redefine their relation to their negative cognitions through the inclusion of (a) mindfulness—present moment awareness of one’s current experience, (b) decentering—a healthy distance to one’s experience, and (c) acceptance—a non-judgmental and compassionate stance to one’s experience (Brown et al., 2018; Brown & Ryan, 2003; Coffman et al., 2006; L. Hayes et al., 2011; van der Velden et al., 2015). The extent to which these components—mindfulness, decentering and acceptance—are included or implemented differs among Acceptance and Mindfulness Based Therapies (Johannsen et al., 2022). For example, in ACT, individuals learn to re-define their relation to negative cognitions through mindfulness and start accepting them and commit to actions for a positive life (S. C. Hayes et al., 1999). For this strategy too, there is empirical evidence of its effectiveness to reduce depression (Zoogman et al., 2015). For example, a randomized controlled trial (RCT) by Biegel and colleagues (2009) examined the effect of adding mindfulness-based stress reduction to regular treatment of adolescent depression in an outpatient psychiatric facility. The study results revealed that over a 5-month period the mindfulness group had a significantly better improvement in depressive symptoms (d = 0.95) compared with regular treatment (d = 0.31). In sum, both changing cognitions and acknowledging cognitions seem superior to other strategies.
Changing Versus Acknowledging Negative Cognitions
That both strategies to acknowledge and strategies to change cognitions can be effective in reducing adolescent depression raises the question of how the two strategies compare to each other. Little is known about this because the two are often studied in separate trials and rarely combined or compared against each other (but see Petts et al., 2017; Shomaker et al., 2019 for exceptions). Available comparative research mostly comes from adult samples, where comparing different intervention strategies against each other is more common (e.g., Cherkin et al., 2016; Garland et al., 2016). Yet, findings are also inconclusive in the adult literature: Some studies suggest that there is no difference between interventions focused on changing versus acknowledging negative cognitions (e.g., Forman et al., 2007; Manicavasagar et al., 2014; Thurston et al., 2017), whereas other studies suggest the superiority of one strategy over the other. For example, Webb and colleagues (2019) found mindfulness skills to be superior to CBT skills to reduce depressive and anxiety symptoms in adults.
The Present Study
It is thus poorly understood how the two strategies compare to each other, especially in adolescence. To improve our understanding of this, we conducted a multilevel meta-analysis on the relative effectiveness of each intervention strategy. We compared both their overall relative effects and their relative effects in prevention versus treatment settings. We did this for two reasons: first, samples with less severe depression (i.e., prevention samples) tended to yield smaller effects than in samples with more severe depression (i.e., treatment samples; Whisman, 1993). Second, we know from related fields that symptom severity sometimes interacts with intervention content in predicting intervention effects (e.g., Leijten et al., 2018). In other words, the aim of this study was to identify whether strategies to change cognitions (i.e., CBT and CBT-like strategies) or strategies to acknowledge cognitions (i.e., mindfulness and mindfulness-like strategies) are more effective for reducing adolescent depression and whether this difference varies by prevention versus treatment settings. We tested this by meta-analyzing the evidence of RCTs that allow for drawing causal conclusion about the effects of both strategies.
The contribution of answering this question is twofold. First, understanding the most effective way to target negative cognitions for reducing depressive symptoms refines our understanding of the role of negative cognitions in the development and maintenance of depressive symptoms in adolescents. We did not have any specific hypothesis or expectations but wanted to examine whether there is a differential effect between both strategies. Should, for example, strategies to acknowledge cognitions be more effective, it would suggest that it is not the mere presence of negative cognitions that contribute to depression, but how one relates and reacts to these cognitions. Second, it will provide guidance to policymakers and practitioners on what types of programs are most likely to benefit adolescents.
Method
Data Sources and Study Selection
We identified RCTs that evaluated the effects of intervention programs focusing either on changing negative cognitions (e.g., CBT-based programs) or acknowledging negative cognitions (e.g., mindfulness or acceptance-based programs) to reduce depressive symptoms in adolescents. Search terms were entered in the advanced search function of three databases: PsycINFO, Medline, and Web of Science. We used the following search terms and their synonyms in various combinations: Cognitive Behavioral Therapy, Mindfulness-Based Therapy, Acceptance and Commitment Therapy, Adolescents, Depression, Therapy, Randomized Controlled Trials. We also searched the reference lists of relevant reviews and meta-analyses. Our search included studies that had been published by June 2022. We placed no restrictions on the time period in which the studies needed to be conducted, publication year, cultural context, or geographical region. The full search strategy with the keywords used to search databases is provided in the Supplemental Materials (see Supplementary Table S1 through Table S3). We applied our selection criteria first to the titles and abstracts of identified studies. If studies seemed potentially eligible, we examined their full texts. Uncertainties were discussed and the authors agreed on the final list of included trials. While our search was systematic and thorough, we acknowledge that it is possible that not all trials might have been identified. Figure 1 shows the study search and identification flowchart.
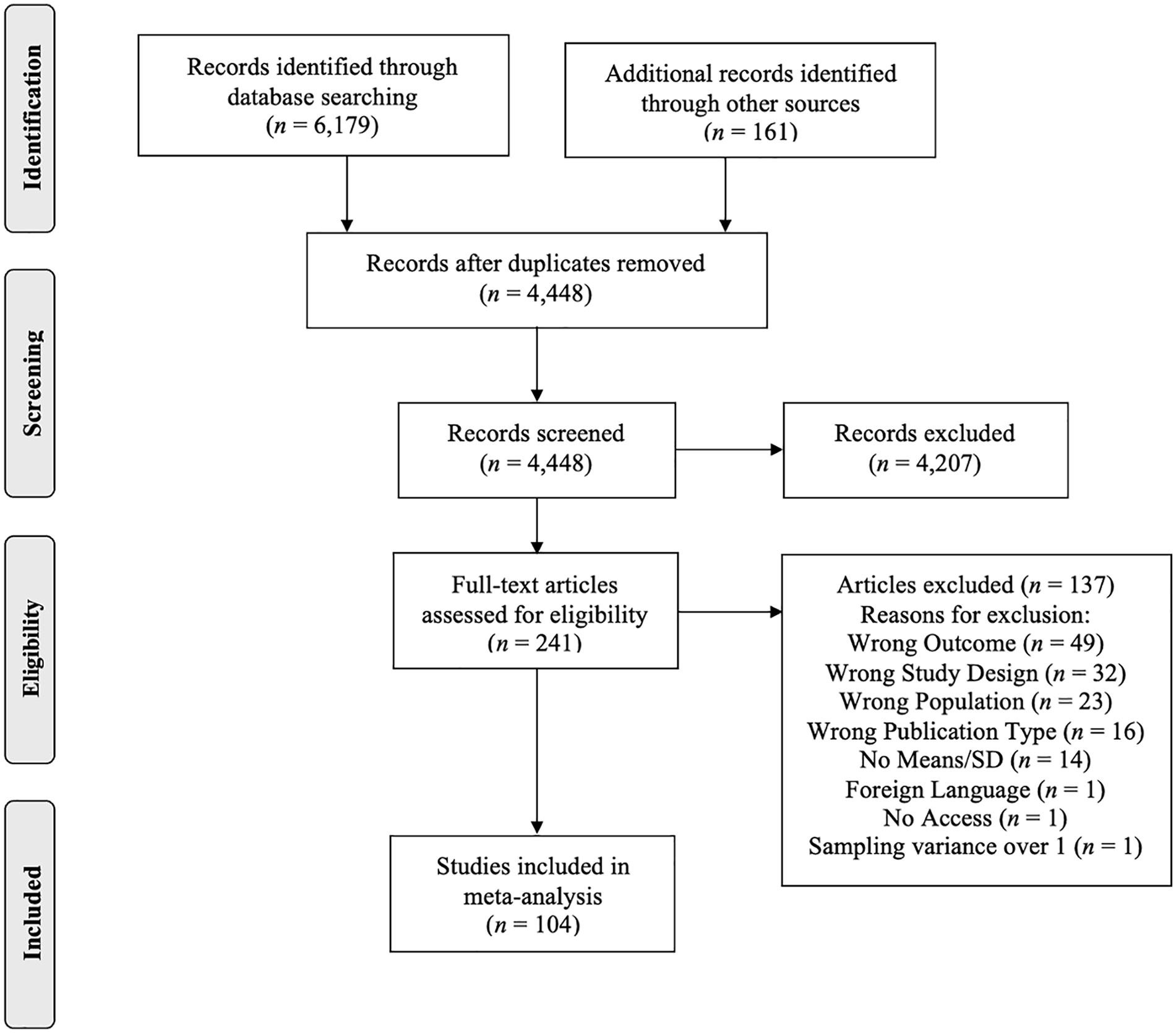
Flowchart of Study Selection.
Inclusion and Exclusion Criteria
Inclusion criteria were: (a) comparing one of the therapeutic strategies (i.e., changing or acknowledging negative cognitions) to any type of control condition.; (b) including adolescent depression as one of the outcomes; (c) random assignment to conditions, either individually or in clusters (e.g., schools); (d) mean sample age between 14 and 18 years. We focused on this age group because depression rates typically increase around the ages of 14−15 (Essau et al., 2000); (e) targeting adolescents directly (as opposed to targeting solely parents or teachers); (f) publication in peer-reviewed academic journals to ensure comparability of the two strategies; and (g) studies were written in English, German or Dutch.
We excluded samples with medical conditions (e.g., cancer, diabetes, irritable bowel syndrome, chronic pain), intellectual disabilities, and/or other severe disabilities. We also excluded samples who experienced trauma (i.e., war, natural disasters, child abuse, etc.), who were incarcerated, or homeless. These populations were excluded because they are more likely to experience functional impairment, loss of loved ones, different forms of violence, meaningful activity, and/or (mental) health services, and insecure prospects for the future, among others (Durcan & Zwemstra, 2014; Malas et al., 2019; Summerfield, 2000). Hence, they might have different underlying causes of depression that interfere with the relative effects of changing versus acknowledging negative cognitions. We placed no restrictions on the delivery method (e.g., in person or online), baseline levels of depression (i.e., we included both prevention and treatment trials), and any comorbid mental health problems in the sample (e.g., anxiety or attention deficit hyperactivity disorder—except for post-traumatic stress disorder due to the reasons mentioned above). Reporting was guided by the Meta-Analysis Reporting Standards.
Data Extraction
General Study Characteristics
We coded characteristics of the participants (e.g., percentage of girls, age, percentage of minority ethnic groups), intervention level (i.e., prevention or treatment), type of control condition (i.e., active or passive), intervention length (i.e., number of weeks implemented), intervention dosage (i.e., hours of implementation) and intervention setting (i.e., group or individual setting). We further coded the characteristics of the study design (e.g., intention-to-treat analysis), study quality (e.g., dropout rate, type and number of instruments), and measures for the calculation of effect sizes (e.g., means and standard deviations of depression measures). The coding manual with all coding categories can be found in the Supplemental Materials (see Table S4).
Changing Versus Acknowledging Cognitions
We defined changing cognitions as techniques to modify negative cognitions, specifically, by challenging negative thoughts and replacing them with alternative, more positive ones (Burns & Beck, 1978; Clark, 2013). Furthermore, we defined acknowledging cognitions as techniques to cope with negative cognitions, without trying to change them, specifically, through non-judgmental acceptance of negative cognitions, mindfulness, meditation, and/or breathing exercises (Baer, 2003; Reina & Kudesia, 2020). Interventions, using cognitive behavioral and modifying strategies, were classified as strategies to change cognitions. Interventions, using mindfulness and other strategies focusing on observing or accepting (but not changing) negative cognitions, were classified as strategies to acknowledge cognitions. Interventions mixing the two strategies such as mindfulness-based cognitive therapy (MBCT) were excluded from this comparison because they could not be assigned to either acknowledging or changing cognitions. Instead, programs that combined the two strategies were examined separately. The included trials were coded by the first author and in the case of difficult decisions, uncertainties were discussed in the author team.
Effect Size Calculation
Effect sizes, expressed as Cohen’s d, were calculated using the following formula:
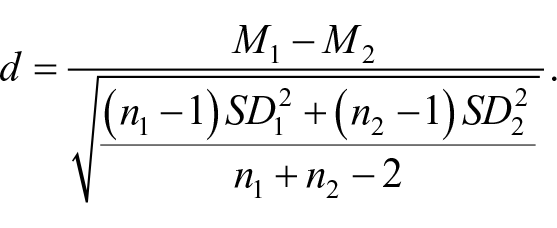
In cases where standard errors, minimum and maximum values, or 95% confidence intervals (CIs) were reported instead of standard deviations, we converted these to standard deviations before calculating the Cohen’s d values. In accordance with the cut-off thresholds established by Cohen, the effect sizes were interpreted as small (d ≤ 0.20), moderate (d ≥ 0.50) and large (d ≥ 0.80), respectively (Cohen, 1988). We included multiple effect sizes per study, if studies included multiple post-intervention assessments (e.g., immediate and later follow-up), multiple measures of depression (e.g., Beck Depression Inventory; Children’s Depression Inventory), multiple informants (e.g., adolescents and their parents), and/or multiple intervention arms.
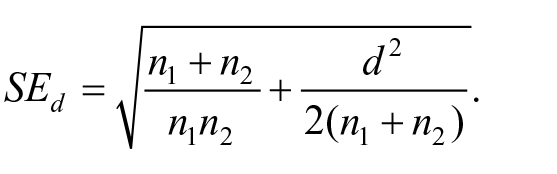
The standard error of effect sizes was calculated using the following formula:
Data Synthesis
Three-Level Meta-Analysis
Most studies (70%) yielded multiple, and on average three, effect sizes. We tested a random effects model using the “metafor” package in R-Studio for three-level meta-analysis, version 4.2.1 (RStudio Team, 2022). We applied a three-level structure (Assink & Wibbelink, 2016; Cheung, 2014; Hox et al., 2017), accounting for the sampling variance (Level 1), the variance of effect sizes within studies (Level 2), and the variance of effect sizes between different studies (Level 3). Hence, this model allowed the effect sizes to vary between participants, within studies (i.e., across assessments), and between studies. Models were estimated using restricted maximum likelihood and α = .050 was used as a cut-off value to assess the significance level.
Missing Data
Some of the included trials did not report on all relevant study characteristics (e.g., percentage of ethnic minorities). These cases are presented in the Supplementary Table S5.
Outliers
Extreme Cohen’s d values were identified using the boxplot method (Tukey, 1977). There were 36 effect sizes (11% of all effect sizes) exceeding the cut-off values of the lower (f1 = q1 – 1.5H-spread = −0.67) or upper fence (f3 = q3 + 1.5H-spread = 1.01). However, these values were not removed nor replaced as outlying effect sizes may be of most interest to examine in moderator analyses.
Bias Assessment
To assess the quality of included studies, we used the Cochrane Risk of Bias Tool (Higgins et al., 2011), rating them as high, low, or unclear, for blinding of personnel or study participants, participant attrition over all time measures, and measurement objectivity. We further assessed the likelihood and potential impact of publication bias using the trim-and-fill analysis (Duval & Tweedie, 2000a, 2000b) and Egger’s test (Egger et al., 1997).
Results
Study Selection
We included 104 RCTs, which generated 335 effect sizes. Eighty-one studies evaluated strategies to change negative cognitions (292 effect sizes; 52% immediate post-intervention and 48% later follow-up). Twenty studies evaluated strategies to acknowledge negative cognitions (32 effect sizes; 63% immediate post-intervention and 37% later follow-up). Finally, three studies combined the strategies to acknowledge and change cognitions (5 effect sizes; 60% immediate post-intervention and 40% later follow-up). Although there is a considerable difference in the number of included trials and effect sizes between strategies to change and strategies to acknowledge cognitions, this difference was not significant, t(1, 329) = 0.71, p = .481. Almost all studies (97%) relied exclusively on self-report measures of depressive symptoms (90% of the 81 studies on changing cognitions; all of the 20 studies on acknowledging cognitions). Some (17%) included more than one informant and about a third of the trials used more than one questionnaire to assess depression. Participant age ranged between 12 and 22 years; the mean percentage of females was 63%. About 65% of all participants were from the ethnic majority, but, importantly, only one third of included trials reported on the participants’ ethnicity (e.g., Black, Asian, Latino, etc.). The average length of the interventions was 9 weeks (SD = 6.2) with an average total duration of 10 intervention hours (SD = 7.5). A comparison of study characteristics between strategies can be derived from Table 1. More detailed study characteristics and the references of the included trials are presented in the Supplemental Materials (see Supplementary Table S5). Three studies (5 effect sizes based on 1,049 participants) evaluated interventions combining both strategies (e.g., MBCT). This number of studies was too small to statistically compare against the effects of either single intervention strategy, but the overall effect size was d = 0.40, t(4) = 8.30, p < .001, 95% CI = [0.27, 0.53], suggesting significant small to moderate effects. The study and participant characteristics of studies with combined strategies did not differ from the studies of either intervention strategy, except for control condition. Studies that combined both strategies had only passive control conditions.
Comparison of Study Characteristics Between Intervention Strategies.
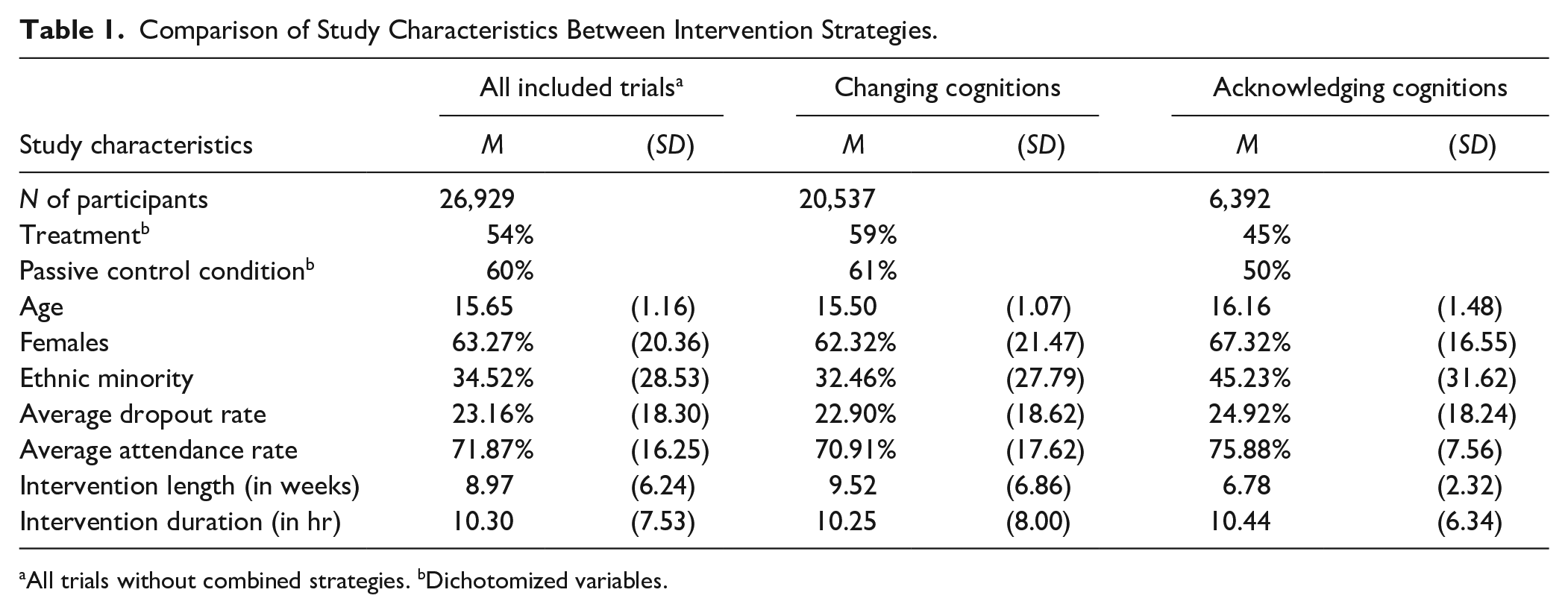
All trials without combined strategies. bDichotomized variables.
Synthesis of Results
Overall Intervention Effect on Depression and Effect Size Heterogeneity
Across all strategies, interventions successfully reduced depressive symptoms, d = 0.21, t(334) = 5.27, p < .001, 95% CI = [0.13, 0.29]. This overall effect was based on all included trials, including the ones examining a combined approach of strategies (e.g., MBCT). Not including these latter trials yielded a similar overall effect of d = 0.20, t(329) = 4.95, p < .001, 95% CI = [0.12, 0.28]. The two one-tailed log-likelihood ratio tests revealed significant within-study variance in effect sizes, σ2within = 0.008, χ2 (1) = 8.37, p = .004, as well as significant between-study variance in effect sizes, σ2between = 0.135, χ2(1) = 141.30, p < .001. Of the total variance, 11.2% could be attributed to sampling variance (Level 1), 4.9% to within-study variance, and 83.9% to between-study variance (Level 3). These results indicate that the effect size distribution was heterogeneous and that moderator analyses could be performed to identify variables that may explain within- and/or between-study variance.
Moderator Analyses
Changing Versus Acknowledging Cognitions
There was no evidence to suggest that either strategy was superior to the other. Both strategies to acknowledge cognitions, d = 0.23, t(328) = 2.42, p = .016, 95% CI = [0.04, 0.41], and strategies to change cognitions, d = 0.20, t(328) = 4.38, p < .001, 95% CI = [0.11, 0.29], successfully reduced adolescent depression and strategy type did not moderate the overall effect, F (1, 328) = 0.08, p = .782. In other words, it does not make a difference whether adolescents are encouraged to acknowledge or change negative cognitions—both strategies have a small, but positive effect on relieving their depressive symptoms.
Prevention Versus Treatment
We coded studies as (a) prevention if the program targeted healthy youth, or youth at higher risk for mood disorders (e.g., youth with depressed parents); or as (b) treatment if the program targeted adolescents who displayed (sub-)clinical levels of dysthymia or depression; or were referred to outpatient clinics for mental health problems. We tested whether the intervention level (prevention versus treatment) predicted effect sizes. This was not the case, F(1, 328) = 0.97, p = .325. Treatment, d = 0.23, t(328) = 4.85, p < .001; 95% CI = [0.13, 0.32], yielded larger effects than prevention, d = 0.18, t(328) = 3.75, p < .001; 95% CI = [0.09, 0.27]. Both prevention and treatment programs are effective in reducing depressive symptoms in adolescents but effects seem a little stronger for individuals in treatment settings relative to individuals in prevention settings. However, they do not impact the overall effect interventions have in reducing adolescent depression.
Active Versus Passive Control Condition
The effects that RCTs generate depend on the type of control condition they use (Mohr et al., 2009). We conducted post hoc sensitivity analyses to detect any possible moderation effects by type of control condition. We coded studies as (a) active control condition: adolescents received some kind of program or help (i.e., minimal intervention, standard, or enhanced care as usual); or (b) passive control condition: adolescents did not receive any support or guidance (i.e., placebo, waitlist or no treatment conditions). Active control conditions yielded smaller effects, d = 0.19, t(328) = 3.99, p < .001, than trials with passive control conditions, d = 0.21, t(328) = 4.70, p < .001. Yet, the type of control condition did not predict the overall effect size, F(1, 328) = 0.25, p = .617.
Intervention Dosage
Because intervention dosage can impact the efficacy of intervention programs (e.g., Smokowski et al., 2016), we conducted post hoc sensitivity analyses to detect any possible moderation effects by intervention dosage. As dosage, we used intervention length (in weeks) and intervention duration (in hours), in separate analyses. While intervention duration, F(1, 328) = 0.15, p = .699, did not have any moderating effects, intervention length did, F(1, 328) = 4.70, p = .031. More intervention weeks are associated with slightly lower effect sizes (β = −0.011, SE = 0.005). But this difference is marginal and can be disregarded.
Bias Assessment
At the individual study level, about 38% of studies had low risk of bias regarding the blinding of the personnel or study participants. Furthermore, 31% of the included studies had a high attrition rate (≥25%). However, most of the included trials had small samples (45% had <100 participants), meaning that the drop-out of even a few participants results in a larger attrition rate. Also, 56% of the included studies had at least one follow-up assessment post-treatment. Considering the difficulty of retaining study participants over longer periods of time, attrition rates of under 25% appear tolerable. Finally, most studies (84%) had low measurement objectivity because they relied on self-report measures. However, as depression is an internalizing problem, self-measures may be the only way for researchers to access unique information they would not be able to obtain otherwise (T. L. Hope et al., 1999). Overall, there are certain acceptable risks of biases, which might lead to systematically overestimated intervention effects. Hence, our findings should be interpreted with caution, as the actual effect sizes might be smaller than the ones we found. Details on the assessment of the risk of biases are presented in the Supplemental Materials in Table S6.
To address publication bias, we conducted a trim-and-fill analysis and the Egger’s test in which we tested the standard error as a predictor of effect sizes in a three-level meta-analytic model. The results of the trim-and-fill analysis revealed that 62 effect sizes (extracted from 37 studies) had to be imputed on the left side of the funnel plot to restore its symmetry (see Figure 2). Adding these “missing” effect sizes to the dataset produced an “adjusted” effect size in which the overall effect shrank down to d = −0.02 (95% CI = [−0.12, 0.08], Δd = 0.23), indicating that the results may have been affected by publication bias. The Egger’s test revealed that effect sizes increase as their standard error increase (i.e., higher effect sizes are produced by less precise studies). This is in line with the results of the trim-and-fill analysis and also indicates that the results may have been affected by publication bias (b1 = 1.88, p < .001, 95% CI = [−1.27, 2.50]). However, these results should be interpreted cautiously. Any technique for assessing bias has its limitations, especially when there is heterogeneity in effect sizes and when effect sizes are synthesized in three-level meta-analytic models.
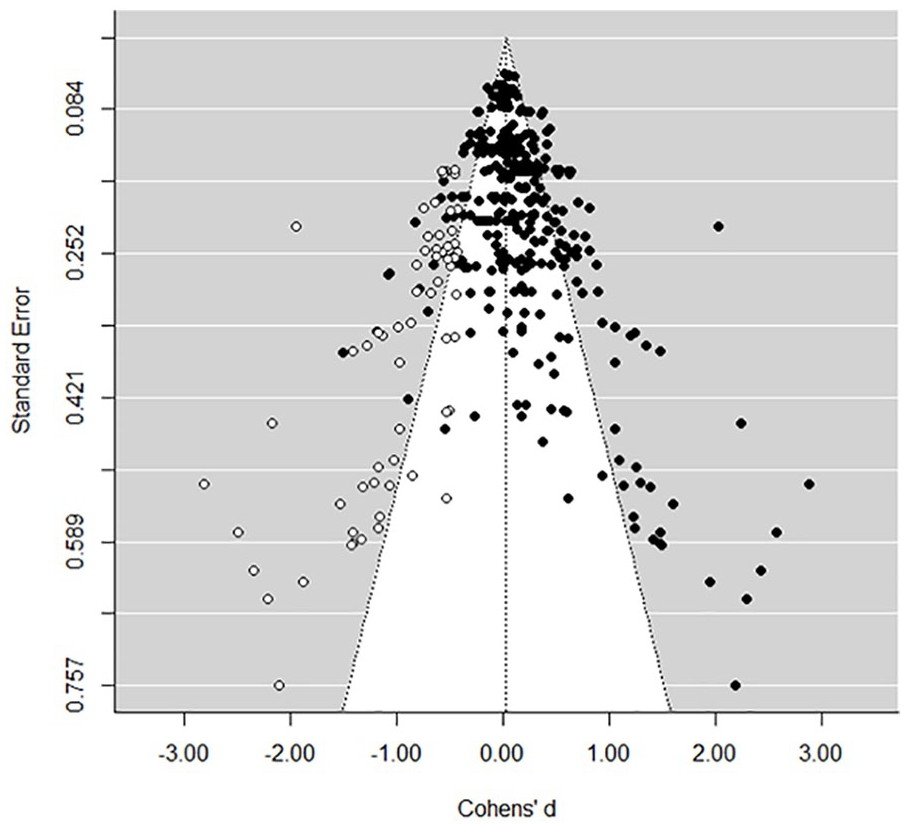
Funnel Plot.
Discussion
Therapies for adolescent depression typically target cognitions because these play a crucial role in the development and maintenance of depression. We synthesized the available evidence of the effects of two meaningfully different strategies to deal with negative cognitions: either actively changing or acknowledging them. Our results indicate that both strategies effectively reduce adolescent depressions, with no evidence suggesting the superiority of either one. That both strategies effectively reduced adolescent depression fits the phenomenon often referred to as the Dodo Bird Verdict: “all have won, all must have prizes” (Luborsky, 1975). Therapy equivalence suggests that intervention effects are either a function of so-called common factors (Frank & Frank, 1991) or reflect different pathways to recovery. Common factors such as placebo effects and providing a support system may contribute to recovery regardless of the specific therapy that is provided (Arch & Craske, 2008; Asay & Lambert, 1999; Bohart, 2000). Pathways to recovery refer to the mechanisms through which the different strategies may result in the same outcome. For example, for symptoms of depression to subside, negative cognitions need to change—either by acknowledging or changing them. This change can occur in different ways (DeRubeis et al., 2005). In strategies focusing on changing negative cognitions, the change is induced directly by challenging them. Individuals react to the negative thought and correct it by, for example, fact-checking the content of negative cognitions or counterposing them with positive thoughts. In strategies focusing on acknowledging negative cognitions, this cognitive change may happen in the long run by observing and acknowledging negative cognitions. Instead of reacting to negative cognitions, individuals redefine their relationship to such cognitions and thus change the cognitive processes around them: Negative cognitions can now be perceived as cognitions that pass by rather than a reflection of reality (Coffman et al., 2006). The emotional reactivity changes, and with it the perception of negative cognitions changes (Williams et al., 2006). This redefined relation to negative cognitions can be considered cognitive change and reduces symptoms of depression. In other words, cognitive restructuring happens in both cases—for cognitive behavioral strategies by working on the cognitive content, and for mindfulness and acceptance-based strategies by working on the cognitive process. In the end, however, both strategies achieve the same outcome (Johannsen et al., 2022).
The Additive Effect of a Combined Strategy
There were too few trials on interventions that combined both strategies in one program (e.g., MBCT) to compare their effects against strategies to either acknowledge or change negative cognitions. Descriptively, the overall effect of this combined strategy (d = 0.40) seems to combine the effects of acknowledging cognitions (d = 0.23) and changing cognitions (d = 0.20). This would suggest that the combination of non-judgmental awareness, self-compassion, and cognitive restructuring is particularly effective in reducing depression. More specifically, it suggests that strategies to acknowledge negative cognitions and strategies to change negative cognitions not only can go together, but the effect of one may amplify the effect of the other (S. C. Hayes & Hofmann, 2017). One possible explanation for this could be that acknowledging negative cognitions is the gateway to changing them. Importantly, however, the number of trials on MBCT was very limited and more rigorous comparisons, especially within-study comparisons of different intervention strategies, are needed to test the relative individual and combined effects of both strategies (James & Rimes, 2018; Leijten et al., 2021).
Ruling Out Moderators
We conducted sensitivity analyses to examine whether there are any moderation effects by intervention level (i.e., treatment versus prevention), control condition (i.e., passive versus active) and intervention dosage (i.e., intervention length and duration). No moderating effects could be found for any of the variables except for intervention length, with longer interventions showing smaller effects. However, the moderating effect was so small that it can be disregarded. Our finding that intervention effects did not differ by the level of prevention or treatment was surprising. A possible reason for this finding may be that prevention samples in some cases consisted of youth with other mental health disorders (e.g., anxiety or eating disorders). These samples were prevention samples in the sense that youth were not recruited based on depressive symptoms, but treatment samples in the sense that youth had already developed clinical levels of mental health problems.
Study Limitations
Several study limitations should be mentioned. First, we compared the effects of each strategy as evaluated in separate trials. This means we examined the association between strategy and effect sizes—individuals were not actually randomized to either one strategy or the other within the same trial. Associations are an essential, but not sufficient step toward understanding relative causal effects. Second, we almost exclusively relied on adolescents’ self-report measures of depressive symptoms because this is what the original studies relied on. Adolescents may over or underreport depressive symptoms (Beck, 1961). Fortunately, evidence suggests that self-report questionnaires are a valid alternative to clinical interviews (De Los Reyes et al., 2015; Hodges, 1990). Third, we were unable to statistically test the two individual strategies against interventions that combined both strategies (e.g., MBCT) because our search identified only three trials that met inclusion criteria. Descriptively, the effect of the combined approach seems to be stronger than that of the single approaches, but this comparison could not be tested statistically. Fourth, the trim-and-fill analysis and Egger’s test suggest that our results may have been affected by publication bias. However, the performance of these tests is limited because we applied them to a three-level meta-analytic model and thus may not produce reliable results (Egger et al., 1997; Idris, 2012; Peters et al., 2007; Terrin et al., 2003). Fifth, we relied on one coder of the studies, increasing risk of researcher bias. However, clear guidelines and criteria had been established before starting the coding procedure and uncertainties were discussed among the authors. Sixth, there was much variation in intervention length between studies. We examined whether intervention length predicted effect sizes and this effect seemed very minimal. Seventh, our search resulted in unequal sample sizes for each strategy, reducing the statistical power of the moderator analyses.
Implications for Research
For future work, it will be important to further scrutinize the relative effects of single versus combined approaches to change and acknowledge negative cognitions. Such work would ideally also include analyses of individual differences in intervention benefit. Because depression often co-occurs with other mental health problems (Avenevoli et al., 2015), for example, it will be important to test how comorbid mental health problems may influence the effectiveness of both single and combined strategies.
Conclusion
We compared two different intervention strategies (i.e., changing cognitions versus acknowledging cognitions) in terms of their absolute and relative effectiveness for reducing adolescent depression. Our findings do not indicate overall superiority of one over the other, suggesting that practitioners and adolescents can choose a strategy depending on the adolescent’s preferences. No meaningful moderators were identified. This seems a positive outcome, offering practitioners and clients flexibility in the use of either evidence-based strategy to reduce reducing depressive symptoms in adolescents.
Supplemental Material
sj-pdf-1-ebx-10.1177_10634266231154209 – Supplemental material for Changing or Acknowledging Cognitions: A Meta-Analysis of Reducing Depression in Adolescence
Supplemental material, sj-pdf-1-ebx-10.1177_10634266231154209 for Changing or Acknowledging Cognitions: A Meta-Analysis of Reducing Depression in Adolescence by Şeyma Uluköylü, Patty Leijten and Mark Assink in Journal of Emotional and Behavioral Disorders
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.