
Abstract
Masculinity refers to varied hierarchies of socially constructed descriptions of men’s identity and includes practices that allow the continued dominance of men in society. Previous research focused on examining the intersection of hegemonic masculinity, gender, and single chronic illness. Limited research exists on the intersection of multimorbidity, gender, self-management, and hegemonic masculinity. This study illuminated the interplay of gender, hegemonic masculinity, and self-management of multimorbidity through a narrative inquiry of men’s experiences. Eight interviews were conducted with men between the ages of 36 to 49 who had been living with multimorbidity for 5 to 8 years. Using narrative thematic analysis, four composite case studies were generated to capture how hegemonic masculinity influenced self-management: Concealing Bodily and Affective Struggles, Seeking Help is Dishonorable, Conquering illnesses Symbolizes Strength, and Preserving “Social Manliness”. Men with multimorbidity strived to preserve their hegemonic masculinity by concealing their intrapersonal struggles and avoiding familial and social assistance.
Multimorbidity refers to three or more chronic conditions (Almirall & Fortin, 2013). Globally, there is an increase in multimorbidity with an estimated global prevalence of 42.4%, 38% in low-income or middle-income countries, and 44.3% in high-income countries (Ho et al., 2022). Multimorbidity increases with age (Lee et al., 2021). However, discrepancies are reported regarding the differences in multimorbidity, mortality, and disease progression among men and women. Some studies noted that the prevalence of multimorbidity and disease progression is similar by sex and gender (Kim et al., 2021; Wang et al., 2022). Many studies noted a higher prevalence in women (Abad-Díez et al., 2014; Jiao et al., 2020; Roman Lay et al., 2020; Schäfer et al., 2012). Some studies also noted that men have a greater incidence and prevalence of primary and secondary multimorbidity (Kim et al., 2021; Lee et al., 2021; Shang et al., 2020). Overall, a consensus is that some diseases are more prevalent among men than women (Crimmins et al., 2019; Schäfer et al., 2012). For example, cardiovascular and metabolic disorders are more prevalent among men, and anxiety, stress, and arthritis disorders are more common in women (Coste et al., 2022; Crimmins et al., 2019; Kim et al., 2021; Needham & Hill, 2010). Nevertheless, it is well-established that men and women have different behavioral, emotional, social, and psychological responses to chronic diseases and self-management (Coste et al., 2022; Younas, Zeb, Tejada-Garrido, & Durante, 2024; Zeb et al., 2021).
Studies have reported that men are often concerned about the impact of chronic illness on their capacity to provide for their families and the negative impact on their ability to make decisions in the family. However, women worry about their ability to manage family responsibilities (Hjelm et al., 2005; Younas, Zeb, Tejada-Garrido, & Durante, 2024; Zeb et al., 2021). In some cultures, women with chronic illnesses are often concerned about ensuring that their spouses are effectively cared for in homes and communities. Therefore, women sacrifice their self-care needs to better care for their families (Younas et al., 2024c; Younas, 2017; Zeb et al., 2021). Men have delayed health-seeking behaviors and are often less observant about the self-management of chronic illnesses in social settings (Mathew et al., 2012; Thompson et al., 2016) for two reasons. First, globally, women are more informal caregivers than men (Bhan et al., 2020; Swinkels et al., 2019; Sharma et al., 2016). In some cultures, women are expected to care for men’s health needs in homes and community settings. Therefore, men often do not actively engage in self-management (Younas, Zeb, Tejada-Garrido, & Durante, 2024; Novak et al., 2019; Sharma et al., 2016). Second, men are reluctant to seek health care for their chronic health issues to adhere to the macho culture and to sustain their masculinity (Mursa et al., 2022; Novak et al., 2019; Olanrewaju et al., 2019). In South Asian and Pakistani context, the culturally dominant notion of manliness—mardangi, ghairat—is linked to man’s role as a provider, protector of the family, and the primary decision making in households (Qaiser, 2022; Shah, 2023; Younas & Zeng, 2025). This ideal masculinity is characterized by emotional suppression, physical endurance, and self-reliance, which translates into a cultural imperative to conceal weakness and reject help-seeking as it implies a failure to fulfill one’s duty or a loss of social standing (Awan et al., 2025; De Visser et al., 2022). This expectation is heightened by the patriarchal structure where a man’s honor is often intertwined with his perceived strength and control over his body and household (Younas & Zeng, 2025).
Masculinity refers to varied hierarchies of socially constructed descriptions of men’s identity and includes practices that allow the continued dominance of men in society (Connell & Messerschmidt, 2005). Ample research focused on examining the intersection of hegemonic masculinity, genders, and chronic illness such as diabetes (Quaglia, 2020), Parkinson’s disease (Gibson & Kierans, 2017), stroke (Kvigne et al., 2014), prostate cancer (Green, 2021), multiple sclerosis (Riessman, 2003), fibromyalgia (Sallinen et al., 2019), and breast cancer (Solimeo et al., 2017). These studies demonstrated that men embody health behaviors to redefine predominant masculinity beliefs and reconstruct their identities to adhere to their inherent social beliefs. Research within the South Asian context also demonstrate a clear intersection between chronic physical conditions and emotional distress influenced by cultural factors and multiple forms of inequality (Awan et al., 2022). Specifically focusing on South Asian men, research highlighted how social determinants of health, traditional masculine roles, and the need to negotiate multiple identities is linked to providing and suppressing vulnerability, which contributes to this emotional distress during long term illness (Awan et al., 2025). However, to date, there is limited empirical research on the intersection of multimorbidity, gender, emotional distress, self-management, and hegemonic masculinity. Therefore, this study was conducted to address this research gap and provides insights into how masculinities intersect with men’s self-management abilities within their sociocultural context.
Purpose
To explore the interplay of gender, hegemonic masculinity, and self-management of multimorbidity through a narrative inquiry of men’s experiences of living with multimorbidity.
Theoretical Underpinnings
We used Connell’s initial account of hegemonic masculinity (Connell, 1987(Connell, 1987)) and the refined conceptual view by Messerschmidt (2018) as the theoretical foundation for this study due to their unique capacity to analyze gender hierarchies that are present globally and intersect directly with men’s health behaviors. Connell (1987) considers hegemonic masculinity as a type of masculinity that pertaining to inequitable gender relations between men and women in a particular sociocultural context. Connell and Messerschmidt (2005) refined the concept. They argued that hegemonic masculinity requires a more inclusive view of gender-based hierarchy that acknowledges the agency of persecuted individuals and the power of predominant ones, and the mutual conditioning of social dynamics. They argued that hegemonic masculinities could be analyzed at the local, regional, and global levels. The local level refers to examining hegemonic masculinity during in person interactions among families, corporations, and close and connected communities. Regional examination entails an analysis of cultural, social, and demographic levels. Finally, the global level refers to examination at a political, multinational enterprise, and media levels (Connell & Messerschmidt, 2005 (Messerschmidt, 2019)).
Despite the Western origins of these theories, we selected Connell and Messerschmidt’s theories to inform this study for two reasons. First, these theories can operate across the local, regional, and global levels of analysis allows for a systematic examination of the specific power dynamics and gender hierarchies inherent in the Pakistani context. While Western models often focus on individualism, which may not directly apply to the collectivistic, religious, and patriarchal context of Pakistan, the structural concepts of gender hierarchy, discursive social structures, and structured action are essential and broadly relevant. These theories allow us to explore how these intersecting forces contribute to the delayed health-seeking and self-management struggles among men with multimorbidity. Second, these theories’ emphasis on the “social construction of gender” provides the necessary analytical lens to interpret the health-related practices and there are no such existing frameworks in the South Asian context. The concept of discursive social structures is crucial for understanding how prevailing notions of Pakistani “manliness” are actively constructed, reproduced, and embodied by men managing multimorbidity. The frameworks are thus used here not to impose a Western template, but as a sensitizing concept to identify and map the locally specific configuration of gender power relations and the social-structural forces that shape men’s self-management abilities.
Messerschmidt (2018) proposed the theory of structured action to provide an exemplified understanding of hegemonic masculinity. According to this theory, sexuality, gender, and sex are social constructs. These constructions emerge from embodied sociocultural behaviors and social structures. Social structures are characterized as recurrent patterns of social practices and discourses that tend to cross spatial and temporal boundaries. Messerschmidt (2018) describes two salient social structures: relational and discursive.
Relational social structures define social ties between people regarding sex, gender, and sexuality by establishing the linkages among humans in specific social environments through social practice. Examples of such structures include sex, gender, and sexual “cliques” in schools and workplaces. Discursive social structures are symbols, concepts, and sign systems that form social and cultural meanings for individuals. These structures create sociocultural orders of “truth” and “reality” in specific circumstances through social practice. An excellent example of discursive social structure is how to dress according to sex, gender, and sexuality (Messerschmidt, 2018). According to Messerschmidt (2018), understanding social action theory and relational and discursive social structures is necessary to develop a holistic understanding of hegemonic masculinity. Therefore, hegemonic masculinity justifies inequality ‘between men and women and masculinity and femininity’. Individuals achieve hegemonic masculinity through discursive persuasion and cultural influence, which promotes consent and compliance rather than direct control of uneven gender relations (Messerschmidt, 2018).
Methods
Design
This narrative inquiry was conducted as a part of a larger study of psychological distress and coping among individuals with chronic illnesses in Khyber Pakhtunkhwa, Pakistan (Younas et al., 2022 (Younas et al., 2024) (Younas et al., 2024)). A subset of sample included individuals with multiple chronic diseases who were interviewed for this study as well as some additional interviews conducted of men residing in Rawalpindi and Islamabad, Pakistan. For this narrative inquiry, we adopted the three-dimensional narrative inquiry space (Clandinin & Connelly, 2004) to study men’s experiences of multimorbidity. Clandinin and Connelly (2004) generated this framework based on Dewey’s theory of experience. It entails mainly three ideas, namely, situation (i.e., place), continuity (i.e., past, present, and future), and interaction (i.e., personal and social). The three dimensions of the narrative inquiry framework are temporality, sociality, and place. Being attentive to temporality entails thinking about how individuals link their varied experiences through reflections on their past and future and lateral movements within the present. The notion of sociality aligns with the idea that individuals always interact at intrapersonal, interpersonal, and social levels within their contexts and with their experiences. The intrapersonal level includes personal conditions such as hopes, desires, and beliefs. Social conditions include environments and situations influencing and informing individuals’ context and situational experiences. The third-dimension place refers to the idea that each interaction and experience takes place in a given concrete and specific place and context. Therefore, the researchers should be attentive to the place and context and make sense of individuals’ narratives within the sociocultural context (Clandinin & Connelly, 2004).
Sample
A purposive sample was used as the intention was to gather stories of those men who had extensive stories to share. The sample size of the study was determined based on Riessman’s (2008) recommendation that in narrative inquiry participants should be finalized during data collection and analysis. During data collection attention was paid to the depth of participants’ stories rather than their number. Creswell (2007) asserted that one to two participants can be adequate if they provide a rich story. Other methodologists suggest that 6-10 interviews are adequate for a narrative inquiry as the number of participants also depends on the accessibility, type of population, and research purpose (Guetterman, 2015; Morse, 2000; Subedi, 2021). After five interviews, the stories appeared to have similar themes. Therefore, three additional participants’ stories were gathered to ensure a reasonable sample size.
Data Collection
Due to the pandemic, in-depth unstructured interviews were conducted virtually in Urdu language from August 2022 until October 2022 using Zoom. The interview technique outlined in Jovchelovitch and Bauer (2000) was used. During initiation (First phase), the men who agreed to participate were provided with a general overview of the subject, and explained about the purpose, timing, and process of the interview. Consent signing was completed before the interviews and electronically signed consent was obtained. During narration (Second phase), the participants narrated their stories while the interviewer took notes for questioning in the later stage. Broad questions that were asked of the participants included: please share your story of developing multiple chronic conditions? How multiple chronic conditions have impacted your daily life? Please describe how being a man living in a male dominant society affects your everyday life and ability to manage multiple chronic conditions? During the narration, the participants were listened to attentively without any interruption. When the coda (i.e., the interviewee signals completion of the story) was marked, the interviewer asked the participants “if they would like to tell them anything else”. In the questioning phase (Third phase), the interviewer asked questions to clarify the narrative and develop a richer understanding of participants’ stories. No “why” questions and questions exploring beliefs and attitudes were asked. Instead, the focus of the questioning was to explore events and what happened during, before, or after an event as narrated by the participants. In the concluding talk (Fourth phase), the interviewer asked why questions to discover more about the narrative and gather pointers for analysis and interpretation. The interviewer made additional notes during this small talk to avoid missing important information (Jovchelovitch & Bauer, 2000).
Data Analysis
The data were analyzed using thematic narrative analysis outlined in Riessman (2008), which focuses on the meaning of the story and its content. This narrative analysis is relevant to applied research on illness experiences when the stories are collected through interviews or group conversations. In thematic narrative analysis, the researchers are interested in generating a biographical narrative of the participants and drawing on interpretations from the broader sociocultural context (Younas & Inayat, 2025). There is little emphasis on the local context of the interviewer and the narrator, such as where the interview was set (Riessman, 2008). While undertaking thematic narrative analysis, we analyzed full stories and then generated themes that were theorized across all the stories (Sandberg, 2022). The step-by-step was as follows.
First, we read the transcripts multiple times before initiating narrative coding. In narrative coding, we utilized the analytical tools of broadening, burrowing, storying, and restorying (Connelly & Clandinin, 1990). Using broadening, we coded the narratives for the broader context such as participants’ descriptions, characters, values, and social, historical, or cultural situations and circumstances. Second, during burrowing, we focused on detailed feelings, understandings, dilemmas, events, and situations and their impact on the participants and their experiences. The focus of analysis at this stage was on particulars that were experienced by our participants from their viewpoint. After broadening and burrowing the narratives, we generated stories and restories of the narratives to bring the lived experiences to the surface (Connelly & Clandinin, 1990). We analyzed a single interview at a time and isolated and ordered significant events into a sequential biographical narrative. After completing the same process for all the interviews, we identified our inherent assumptions in each narrative and coded them (Riessman, 2008). To capture the interplay of hegemonic masculinity and self-management of multimorbidity, we generated four composite case studies to illustrate general patterns and themes. Finally, we compared the underlying assumptions of these cases. Throughout this process, we examined and discussed the impressions of narratives and their content and agreed on the core aspects of the narratives. Each of the composite cases is presented with direct quotes taken from multiple participants to demonstrate the commonality of the case in their narratives.
Research Rigor
We used the methodological bricolage metaphor for establishing and strengthening the research rigor (Pratt et al., 2022). The bricolage metaphor is a way of thinking and entails using and pertinent analytical moves for strengthening the design and conduct of qualitative inquiries. It calls for flexible use of pertinent data collection, analysis, and interpretation methods in each inquiry. Bricolage approach is useful as it enhances the trustworthiness of qualitative research by cobbling multiple methodological decisions and choosing most pertinent and varied analytical moves, hence promoting competence, integrity, and benevolence. Competence pertains to careful selection of study methods and analytical moves to achieve study purpose. Integrity refers to the extent to which analytical moves cobble together and fit with the overall methodology and each other. Finally, benevolence pertains to ensuring that participants voices and experiences are adequately captured in interpretation and reported (Pratt et al., 2022).
We used several analytical moves. Prolonged engagement was maintained with the participants during narrative interviews and recommended guidelines for the interviews were followed (Riessman, 2008). Initial analysis was completed in local language so as to capture the essence of participants’ stories (Younas, Cuoco et al., 2022; Younas et al.,2022). The translation and transcription of interviews into the English language was rigorous to ensure that the core of the experiences was captured without losing the essence of the participants’ experience (Clark et al., 2017; Younas, Cuoco, et al., 2022). During data analysis, it was ensured that premature closure of analysis does not occur hence a segmented method of analysis was completed by analyzing pieces of participants data until a thorough composite case was developed (Inayat et al., 2024). The composite cases were developed by staying close to the data and the decisions were explicitly noted to maintain an audit trail. Reflexivity was practiced by keeping reflective journals and jotting down any presumptions and biases about participants and their stories. We used the MIRACLE narrative framework to provide authentic and contextualized narrative of participants’ experiences (Younas et al., 2023).
Findings
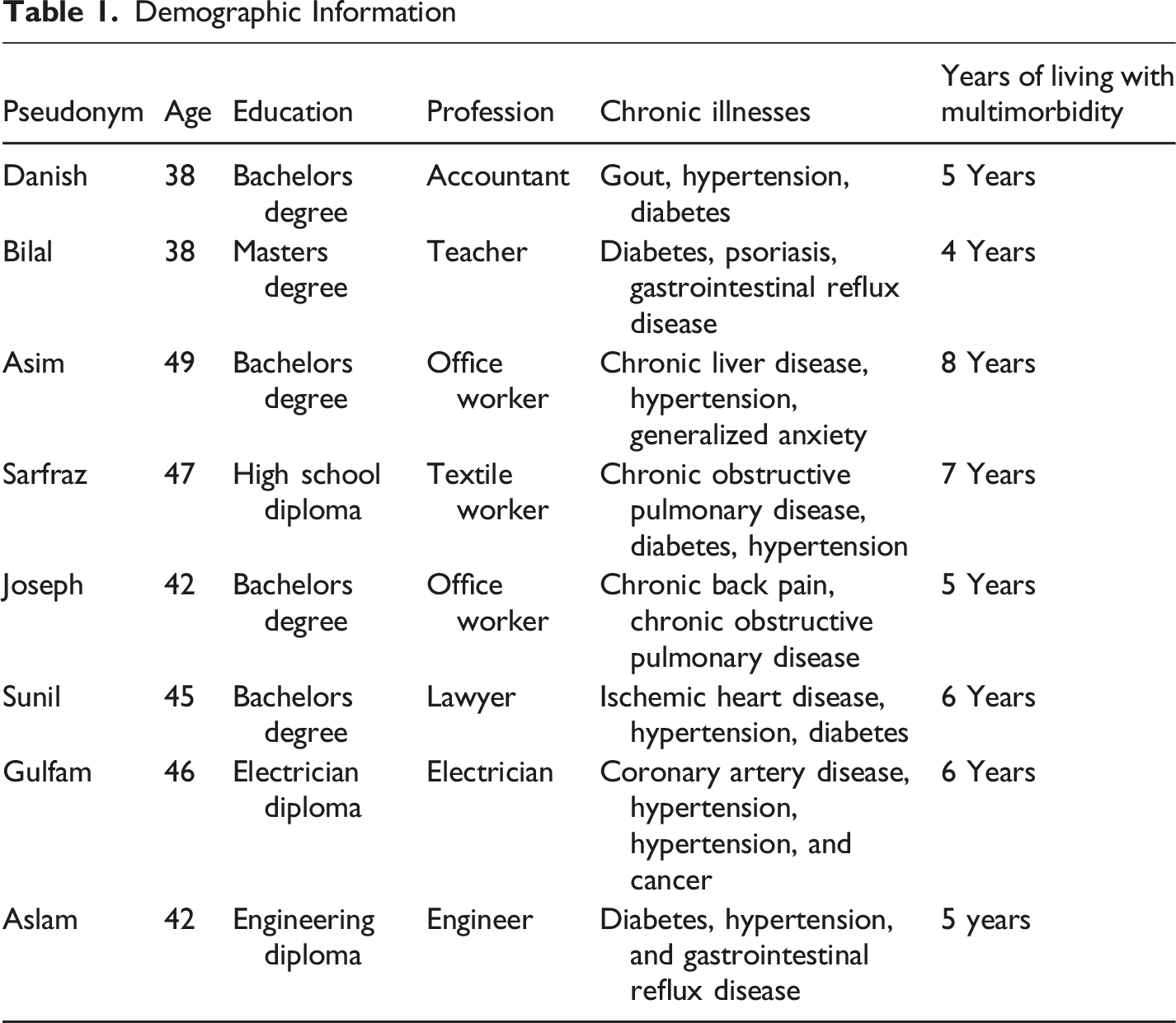
Demographic Information
Composite Case Studies
First Composite Case: Concealing Bodily and Affective Struggles
I was raised in a middle-class family that taught me that men “should not express their emotions and physical weakness and develop the strength to learn to live with physical and emotional stress”. I have always remembered this learning and made sure I keep my emotions to myself and learn to live with any physical and emotional turmoil. The men in my family told me that “expressing stress, pain, and emotions is not a man’s job” and that men should bottle up their feelings. Men who cannot control their emotions and feelings are not respected in their families. I learned that men should support their families when certain family members have emotional challenges and stress. Our duty is to “protect those who are emotional, stressed, and weak,” so if I show my emotions, I will be considered a weak family member. When I was in grade eight, I fell from a bike, injured my wrist, and could not use my right hand for three to four weeks. My father needed some help putting some big boxes in the storeroom and asked me to bring up those boxes. When I told my father that I could not lift these small boxes because my wrist still hurt, he scolded me for refusing to lift small boxes because of mere pain. He told me that crying in pain is not a man’s job.
When I was first diagnosed with a chronic condition, I “did not disclose it to my family.” I knew I could “hide it” from them and move on with my life. There was no point in telling anyone in the family. If I had told them, my brothers would have made fun of me. They teased me when I broke my ankle while playing football and when I stubbed my finger catching a ball during a cricket match. They gave me names that I did not like, and then they told my friends that “I could not do things that they all could do”. It was “embarrassing for me” to be in a group of friends when they would bring up my emotional side. They all looked at me in a strange way when I hurt my ankle during a football game in school. Then they started laughing and calling me softy. I became the talk of the class and school. After this event, anytime when I would play, my friends and other teammates would smirk at me as If I would end up injuring myself again. Then, when I was first diagnosed with high blood pressure, I did not tell my friends and family and would keep eating food with salt. I did not want them to know and call me softy. Eating salt would increase my blood pressure and affect my work, but I would take the pills that the doctor gave me, and I had those hidden in my bag.
I have kept my emotions and feelings to myself and learned to tackle them. The physical symptoms, stress, and negative emotions resulting from my chronic conditions hurt and are a nuisance, but eventually, they go away as time passes. Concealing my emotions and suffering hidden is the best way to avoid any pity from my siblings and now my spouse. I do not want them to show pity on me because I know how to take care of myself. I have lived with multiple chronic conditions for a while and know how to take care of myself. I do not need people to look at me like I am crippled. If I started displaying my emotions and physical struggles, my spouse would see me as weak. I “do not want to come across as a weak personality”. I should be taking care of my children and spouse and not complaining about my physical and emotional struggles. When the doctor told me that I had COPD because of my smoking, I was scared. He told me all about this condition and told me to make sure I cut down on my smoking and take my medications regularly. I knew it will be difficult to keep it to myself and hide from the family, but I told them that I have an allergic cough, and it will just go away. It hasn’t gotten worse since I was diagnosed because I cut down on my smoking. But a while back, my wife figured it out that there was something wrong. I have to tell her, but still, I am good at hiding my breathing problems and my ongoing issues and carrying on with my work. I will hide my deteriorating health issues until I am no longer able to hide it.
Concealing emotional and physical struggles can become challenging at times particularly when there are exacerbations of some symptoms, but I use avoidance strategies like “going out”, “distracting myself”, and “sleeping” so that my family cannot find out that something must be wrong. Usually, it works because they think I am just tired from work. I know I would not be able to hide this suffering for a long time and eventually they will find out, but I hope by that time I would have taken care of most of my family responsibilities.
Second Composite Case: Seeking Help is Dishonorable
I loved helping my friends and siblings in their times of need. In 10th grade, I started working with an “expert electrician who lived across our street. He hired me as a trainee and taught me life skills and electrical work. I think working as an electrician and being man, I need to help people in their tough times.” I would spend hours working in homes “tackling short circuits and flooding-related electrical issues” because I just wanted to be made sure I can diligently help others. Helping others became my second nature. I am reluctant to seek help from others. I do not think others cannot help me. I “do not like to be on the receiving end.” My mentor instilled in me the yearning to always help others. Now that I have these illnesses and I sometimes feel depressed, I cannot ask for help. My mind does not accept that I can be dependent on others. I need to keep do things for myself and not rely on others. For me, the meaning of life is helping others. When God created Adam in the Garden of Eden, He wanted him to take care of the garden and all its creatures. Religion teaches us that men should care for the world and its creation. I am responsible for being available to my siblings and those who are weak, needy, and sick. Even if I feel sick sometimes, I must not refrain from helping others. I can do things on my own and do not need help.
I do not like having to depend on my family to take care of me. I have worked hard and earned a living for my wife and daughters all these years. They have never felt deprived of any luxuries in their lives. I want to keep doing this for my grandchildren. I cannot let go of my self-respect and ask for help. Sometimes I feel that “maybe I am too hard on myself” and should ask for help when needed. But simultaneously, “I am scared of dishonoring men.” Men should always provide for their families and should not ask for help. Instead of asking for help, I should continue working on my strengths and caring for my family. These minor symptoms and diseases are part of life, and I believe I need to develop the strength to overcome these on my own. My sister asked me if I needed money to buy new medicine. I told her I did not need her help. I said, “I would rather die than ask for money from my sister.” My sister is married, and she has a new family now. I am never going to accept her help. As a man, accepting help is like showing you are weak. I am not weak. I have some medical problems, but that does not mean I am on deathbed. When I reached that stage, the story may be different. If I had accepted money from my sister, it would have lowered my respect in the family, and I cannot afford that.
I had no idea that these illnesses could seriously affect my emotional self. I am more aware of my ongoing weakness and emotional strength, and sometimes I feel like a failure. Still, I am not ready to ask my spouse, daughters, sons, and relatives to put me to bed or bath me. I have enough strength in me to carry out all of these activities. I wish to be available to them and offer my support as I always have supported and protected them. “I often get mad when people offer me help,” especially when I did not ask for it. Asking for help is not in my gene. You know, I want to be as strong as I used to be to do what I always liked for my family. I provided for them; I worked hard for them, and I worked long days and nights to make enough money for them. If they offer their help, I like their kindness, but sometimes I also get angry. I feel agitated that as being the decision maker of the family I need to ask for help. I am not going to damage my standing. I am still strong, and very well capable of providing for them. Asking for help is just not my thing.
Third Composite Case: Conquering Illnesses Symbolizes Strength
I studied in a public school in a semi-urban area. Once I heard a story of a man who had one arm, but he never backed down from any challenge in his life. This man was determined and courageous and never let his broken arm come in his way. Handling all the struggles that man ends up becoming the most successful and well-known person in his country. The lesson of this story was never to give up and continue your hard work until you reach the highest level of success. I have always remembered this story, and it has helped me to “stay steadfast during my physical and emotional suffering” brought down by these multiple health issues. Staying resilient in during tough times is important because strength defines human beings. I believe struggle is part of a man’s life, but staying strong during struggling times is the greatest quality of a man. I don’t let my emotions affect my strength and my judgment about myself. I keep my emotions separate and focus on getting through bad days with a strong mind. I feel men are born with extra strength and they should remember that strength should be an essential part of their daily lives.
Receiving multiple diagnoses during my adolescence was a shocker for me. It was the peak time of my life to make a difference in society by becoming successful and known. The first few weeks were tough, and I had trouble learning to live with these diseases. I never gave up and kept doing my part to overcome any obstacles that blocked my path to success. I have learned that if I let diseases take over me, I can feel weak inside. I do have bad days, but on those bad days, I encourage myself to stay resilient. I remind myself that this is not the end of the world, and I need to keep going to reach my goals. I have conquered my fears, physical and emotional problems, and daily struggles and showed others and myself that “relying on personal strengths can help you move rocks”. Being a man is not easy. I feel there are a lot of expectations from us. Our families and friends want us to be strong and courageous. I work long hours, and sometimes it affects my ability to manage my illnesses, but I have learned to use my courage and determination to stay on top of these illnesses. You know, if I had given up on myself, I would have been dead now. It is my courage and toughness that help me overcome these diseases. My father had cancer, and he still lived a long life. He told me that men should show through their actions that they are the strongest beings in this world. He used to share stories of many great men like the Mughals, Muhammad Bin Qasim, and Alexander the great to teach me how men have conquered the world. When I got these diseases, I knew I had to conquer these illnesses with my courage.
Now I am at a late stage in my life, and my physical strength has weaned off to some extent, but my internal desire and determination to stay healthy and strong is growing with my age. I have learned from many failures that I can overcome my struggles without help. Sometimes I need help and motivation to keep going, and my friends always support me. They remind me that “the greatest man of all eras had internal strength” in them that kept them moving forward. I often wonder how long I will live with these multiple illnesses, but I quickly shake off those feelings and focus on using valor to overcome this misery. Using my strength and overcoming challenges is a part of my identity, and I feel proud of myself. Despite these illnesses, I can keep working and providing for my family. This strength helps me overcome my fears and move forward to achieve more in my life.
Fourth Composite Case: Preserving “Social Manliness”
I was born and raised in a society where “men are primary decision makers” in all aspects of life. They have higher positions in schools, politics, games, and media. Women’s job is to work at home and take care of their families. Our culture and religion teach us that women should be protected from the evils of this society and man should be their protectors. This social image of men as the leading figures in all spheres of life is crucial to my identity as a man. I wake up daily reminding myself that maintaining my social image is essential and I should do everything to ensure the “world sees me as the true man”. In our society, “men do not give up”. They do not show emotions, are strong in mind and body, and uphold their values. You must have heard this saying “I am a man of my word”. For me, this saying meant that as a man, I needed to uphold the values and image expected of men. I do not let my emotional side get in touch with my masculinity. I make sure to keep them apart. If I let my emotions get in the way, I will lose my ability to prove to this society what real men are capable of. You know, I was always the strongest one among my friends. Whenever we had fights in school, they would all come to me to help them sort things out, and I showed them what men could do. I keep my promises and my words, and that’s what a real man does in our society.
I do read many books and learned that from ancient times men have kept their masculine characteristics intact. I focus on “preserving my social image as a man”. People in my neighborhood, my office, and my family want me to be a strong being who can overcome obstacles with strength and only a little difficulty. I need to meet those expectations and ensure that no one questions my ability to perform the tasks that I should perform as a man. Men are great thinkers, scientists, judges, lawyers, doctors, and engineers. I believe men hold the most prestigious positions because of their strength, rational decision making, and endurance to overcome any physical, psychological, or emotional illness. I have never “let my illness come in my way of being a successful, capable, and courageous man”. If society expects me to be the strength of my family, I am there for them in my good times and my bad times. I am never letting some sickness take this away from me. Let me give you an example of what is expected of men and how we show out strength. A soldier who fights at the border or during a war never fears his enemy because his country wants him to fight for its safety and freedom. You tell me, “Do soldiers leave the border when they have sniffles, cough, body aches, or high blood pressure.” I am telling you they do not leave their position because they are expected to defeat their enemies and win battles or die as a man. I do not see women in our army because they cannot handle the tension and trauma that war can bring them. If they join the army, they work in the office, homes, or away from the borders. A man is expected to be strong and courageous, and that’s exactly what I am doing. I do not let my symptoms distract me from fulfilling my social responsibilities.
My mother and father have always taught me to be a man who can preserve his status in society. If I were to let my emotional and physical distress negatively affect my decision making and my social and family life, she would not be happy with me. She taught me to be a responsible man who never fears any challenges and moves forward with persistence. I always handle my emotional and psychological distress in a way that others do see me as a feeble man. I confront my emotions, physical struggles, and relational issues that these illnesses have brought me with great courage and insights from my experience of growing up with the men in my family. All the “men in my family were daring and determined and lived long lives,” making their name in the community and family. I want to walk in their footsteps and never let my emotional and physical issues take over my logical and clear thinking and approach to life. I believe preserving my male psychological skillset and harnessing them as I move forward is the key to my success in dealing with these illnesses.
Discussion
This narrative inquiry offers an account of hegemonic masculinity in multimorbidity intertwined with the social and cultural view of men’s roles and responsibilities and society’s expectations. The men’s stories exemplify the account of hegemonic masculinities that could be analyzed at the local and regional levels, as outlined by Connell and Messerschmidt (2005). Men shared that they conceal their struggles, consider help seeking a dishonor to self, and conquer their illnesses as a demonstration of their strengths. These three composite cases highlight how hegemonic masculinity combined with men’s self-care approaches occurs at a local level. The men linked their ideology of self-care to their seemingly underlying belief that men do not need help and support in self-care even if they have increasing symptom burden. Men’s reluctance to disclose their emotions and seek help was connected to their engrained social belief that men cannot disclose their weakness because they have a familial and social obligation to fulfill. These men align with idealized social and cultural values and beliefs about men’s expected roles. Men saw themselves as breadwinners, protectors, decision makers, and heads of their families. They did not want to show their emotions because of their inherent belief that they may lose their authoritative roles in their families. Kvigne et al. (2014) also noted that young men with chronic illness continuously negotiate their masculinities while striving to preserve their strength, power, control, and decision making in their families.
As Messerschmidt (2018) pointed out that “socially constructed power relations” (p. 119) among men and women are integral to the expression of hegemonic masculinity. The stories of these men shed light on the social and family power dynamics where men are in charge of themselves and their families and refrain from losing their authority and dominance in their families despite physical and psychological turmoil during their multimorbidity. Men also supported their socially legitimized power and authority over their families by sharing the idealized role of men articulated in religious scriptures. Nyhagen (2021) articulated that religious men often express a hybrid form of hegemonic masculinity by embracing the values of love, care, and humility while sharing their idealized views of differences in the roles of men and women in religious society. In Nyhagen’s (2021) research, men were willing to express emotions, cry, and demonstrate love. However, religious men in our study have a strict view that men should not express emotions that can be perceived as weak and feminine in society. Molina (2015) asserted that while religious masculinity is supported by religious doctrine, the expression of masculine behaviors aligning with such masculinity are not different from hegemonic masculinity. Men’s behaviors in this study are consistent with Molina’s premise because these justified their socially accepted masculine behaviors with religious doctrine.
Men in their stories alluded to preserving their social manliness, an expectation from men in their sociocultural context to maintain and harness male specific characteristics such as courage, strength, power, authority, persistence, logical decision making, and lack of emotions. This is in line with the regional examination of hegemonic masculinity (Connell & Messerschmidt, 2005) as men evaluated their self-care ability and approach to care for self through what is expected of men who get sick in society. Green (2021) illustrated that men with prostate cancer compared themselves with other members of society and male figures to develop a sense of masculinity and experience. Consistently, men in this study drew comparisons between their beliefs, characteristics, and identities with men figures they idolized in their families. They exemplified that their experiences with male figures helped them shape their beliefs about themselves and how men should act in tough times. Men’s stories highlighted the “discursive social structure” outlined by Messerschmidt (2018) that refers to symbols and sign systems that form sociocultural meanings for individuals. These men shared that men are known for their courage and persistence; therefore, they do not express their struggles and act masculinely.
These findings open up many areas of inquiry in the field of hegemonic masculinity. Future research should focus on exploring a more nuanced relationship between a religiously idealized view of masculinity and socially constructed meaning and how these two views intersect in the lives of men in other types of chronic illnesses, particularly illnesses viewed as feminine (e.g., breast cancer). Narrative inquiries into the meaning of men’s idealized male figures and how they influenced young men to align with hegemonic masculinity can provide insights into the role of familial and social upbringing in shaping masculinity. Inquiry into the lived experiences of men who view conquering illness as a symbol of strength can offer valuable insights into the meaning of strength for men and how it influences their relationship with their family members and spouses.
Limitations
This narrative inquiry may have limited transferability because the Pakistani men were interviewed. Nevertheless, the findings may be helpful when understanding self-care experiences of South Asian men residing in other countries such as India, Sri Lanka, Bangladesh, Nepal, and Afghanistan, and Western countries and their relationship with families during multimorbidity. It should be acknowledged that two of the researchers grew up in a similar culture, and their views on men and their roles in society may have influenced the interpretation of men’s stories. However, reflexivity was practiced during data analysis and recording stories to counteract any biases. Specifically, these researchers were conscious of their own deeply embedded views on male stoicism and the expectation to prioritize family over self-care, which are norms in the shared culture. To mitigate the risk of confirming these assumptions, these two researchers consistently engaged in critical reflexivity and had extensive discussion during data analysis and interpretation with three other team members from Italy (i.e., European). This helped ensure that participant’s voices, rather than researchers personal views, cultural beliefs, familiar cultural lens, drove the findings.
Conclusions
Men’s stories shared draw attention to the intersection of hegemonic masculinity and religious masculinity in the self-care behaviors of men with multimorbidity. Men strived to preserve their hegemonic masculinity by concealing their intrapersonal struggles and avoiding familial and social assistance. Self-management of men in multimorbidity was influenced by their perceived and learned familial and social beliefs concerning men’s roles, social identities, and characteristics. Health care professionals can use this knowledge about men’s struggles interlinked to hegemonic masculinity to have nuanced dialogues about their unhealthy and healthy self-care behaviors.
Footnotes
Ethical Considerations
Ethical approval for the study was obtained from the Institutional Review Board (IRB) of Saidu Medical College, Mingora Swat (Approval#18-ERB/2021). Additional amendment was submitted to the IRB for this this narrative inquiry. Identifying information such as names and addresses were not collected to ensure anonymity and confidentiality.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.