
Abstract
This study explores how traditional masculine norms affect mental health help-seeking attitudes in men residing in regional, rural, and remote Australia. Participants (N = 271) were men living outside of major cities of Australia. Analyses of survey data found increasing endorsement of masculine norms was predictive of more negative attitudes toward help-seeking. Perceived barriers to help seeking partially mediated relationships between masculine norms and help seeking. Full mediation was present for gender role conflict through perceived barriers and help seeking. These findings suggest efforts to improve mental health of men from non-urban communities may consider the way health messages could be targeted to optimise help seeking. Increasing engagement with stakeholders, such as clinicians, community groups, government agencies, and mental health organisations is warranted when engaging men living in non-urban areas.
Public Significance Statement
Introduction
This article provides findings regarding Australian men from regional, rural, and remote communities and the relationships between traditional masculine ideologies. Traditional masculine norms were predictive of more negative help-seeking attitudes and this relationship was mediated by perceived barriers. For men living in non-urban areas of Australia there are complex dynamics to consider which may affect health promotion interventions – further research is warranted.
Psychological help-seeking involves individuals recognising, expressing, accessing, and addressing psychological challenges (Hammer et al., 2018). Despite low life satisfaction, reluctance to seek help can persist (Goodwin et al., 2016). Men, specifically, often defer health professional visits, relying on coping strategies before seeking treatment (Baker et al., 2014; Mansfield et al., 2005; Seidler et al., 2018; Shea et al., 2019). Masculinity’s influence on men’s mental health help-seeking is emerging, with traditional norms hindering it (Seidler et al., 2016; Smith et al., 2008; Vogel et al., 2011). Conforming to these norms is associated with negative outcomes, including heightened suicidal ideation risk (Pirkis et al., 2017). Furthermore, how men perceive their own masculinity significantly influences their health-related behaviours (Griffith et al., 2016; Piatkowski et al., 2020), and this has posited to be largely a product of socialisation, explained by a number of theoretical frameworks.
Socialisation refers to the process through which individuals internalise societal norms and rules (Levine & Moreland, 1994). Aligned with Social Role Theory (Eagly, 1987), individuals are assigned gender-specific roles, where men, for instance, often adopt traditional masculine norms encompassing traits like assertiveness, competitiveness, and emotional restraint (Feder et al., 2010; O’Neil et al., 1986). Consequently, societal expectations position men as providers of help rather than recipients (Eagly & Crowley, 1986). Social Identity Theory (Tajfel et al., 1979) further underscores that men’s adherence to in-group norms depends on the significance of these norms to their sense of belonging. Recent research has posited this, in turn, may drive men who strongly embrace masculine norms to avoid behaviours perceived as non-masculine, including seeking help (Kantar & Yalçin, 2023b). This socialised adherence to traditional masculine ideals can be negatively compounded by group norms and identity (Piatkowski et al., 2022) and negatively impacts men’s willingness to seek help for mental health concerns (Levant et al., 2013; Lynch et al., 2018; Seidler et al., 2018; Smith et al., 2008). Conflicting notions of masculinity, shaped by societal norms, result in gender role conflicts and discrepancies between expressed and idealised forms of masculinity (O’Neil, 2008; Rowbottom et al., 2012). This discordance is associated with negative attitudes towards mental health help-seeking (Griffith et al., 2016; O’Neil, 2008; Rowbottom et al., 2012), identifying traditional masculinity as a barrier to seeking psychological assistance (Levant et al., 2013; Seidler et al., 2018; Smith et al., 2008).
Masculinity has been largely conceptualised as a static construct, devoid of contextual influences and viewed through a deficit-based lens as wholly pathological and requiring a one-size fits all approach (Griffith et al., 2016; Robertson et al., 2016; Thompson Jr. & Bennett, 2015). More recently, researchers have acknowledged a conceptualisation of a masculinity that is diverse in formation and expression, is malleable over time, and involves the integration of contextual, social, and cultural factors (Berk et al., 2018; Griffith et al., 2016; Robertson et al., 2016; Thompson Jr. & Bennett, 2015). Despite some attention given to the dynamic arising between masculinity, mental health, and suicide in non-urban settings (Alston & Kent, 2008; Bryant & Garnham, 2015; Silva, 2002; Wainer & Chesters, 2000), there remain gaps in measurement rigour, impacting the generalisability research thus far. For example, extant work has employed measures of masculinities sampled from, and validated on, largely homogeneous populations - generally using young, white European, heterosexual, college aged males from the United States (Mansfield et al., 2005; Shea et al., 2019; Thompson Jr. & Bennett, 2015). Further, a content analysis of articles published in a prominent men and masculinities journal found dominant characteristics of those sampled were White (60–77%), college students (61–65%), and only 7% identified sexuality other than heterosexual (Wong et al., 2010). Therefore, in generalising the research to men living in non-urban settings in Australia, there are clear gaps which warrant further investigation.
The Australian Men’s Health Strategy 2020–2030 has identified that men living in regional, rural, and remote (RRR; hereon also referred to as “non-urban”) Australia are a population of concern for mental health and suicide related disparities (Department of Health, 2019). Men living in non-urban areas, in comparison to men from major cities, experience higher rates of mental ill-health and suicide rates that increase with level of remoteness and often do not seek help, except during crises (Bryant and Garnham, 2015; Gardiner et al., 2019; McPhedran et al., 2013; Pierce et al., 2016). These men face a range of unique stressors associated with life outside of a major city (Fennell et al., 2018; National Rural Health Alliance [NRHA], 2017) including fewer opportunities, lower incomes, less financial security than those in urban areas, and greater likelihood of exposure to natural disasters (Griffith et al., 2016; Mahalik et al., 2007; NRHA, 2017). Additionally, mental health service deficits that create additional barriers to help seeking include: fewer services; inadequate and insecure funding of rural services; difficulty in maintaining confidentiality in smaller towns; and a lack of allied health services specifically trained in recognising these rural contextual factors, particularly in times of natural disaster (Fennell et al., 2018; Griffith et al., 2016; Hart et al., 2011; Mahalik et al., 2007; NRHA, 2017).
There is emerging research exploring factors that perpetuate health inequities for men living in non-urban areas of Australia. There is a recognised need for special attention in these areas of Australia as the mechanisms which create and maintain disparities in mental health outcomes are not well known (Judd & Humphreys, 2001). Specifically, researchers have called for more focused research within these populations to acknowledge the dynamic and diverse conditions and contextual factors within rural Australia (Fraser et al., 2002). Thus far, extant work has explored the intersections of masculinity and help seeking for mental health in relation to self-reliance and identity in farmers (Hull et al., 2017), rural unemployed (Fragar et al., 2010), rural stoicism (Alston & Kent, 2008; McPhedran & De Leo, 2013; Murray et al., 2008), and mental health stigma among adolescents (Boyd et al., 2006). What remains unclear is the degree that masculinity or rurality is a key determinant maintaining mental health disparities. For example, research examining stereotypes regarding rural stoicism and self-reliance in South Australian farmers demonstrates stoicism as a factor in decision making for mental health (Hull et al., 2017). Contrastingly, men in Queensland were found to have little difference in the contribution of masculinity and stoicism to help-seeking between urban and rural populations (McPhedran & De Leo, 2013). Further, McPhedran and De Leo (2013) suggested that mechanisms preventing help seeking are far more complex than attributing a lack of help seeking to either masculinity or rurality. As such, the degree that masculinity exists and is predictive of attitudes toward help seeking for men in non-urban settings remains unclear. Therefore, there may be other contributing factors which warrant exploration.
Intrinsic and extrinsic barriers may play a role in shaping the way men engage with help seeking for mental health. Intrinsic barriers to help seeking are the diverse, internal attitudes (cognitive, affective, and value oriented) men hold that influence perceived barriers to seek help such as stigma, self-stigma, stoicism, perceived therapeutic efficacy, or value placed on seeking help (Clement et al., 2015; Giallo et al., 2017; Shea et al., 2019; Vogel & Wei, 2005). Negative intrinsic barriers and attitudes may make men initially ambivalent to seeking help for mental illness, drop out of services prematurely, or delay or defer help seeking altogether (Mansfield et al., 2005; Seidler et al., 2018). Extrinsic barriers to help seeking include difficulties in affording or accessing appropriate services, knowledge of mental health conditions, or the ability for men to recognise signs of their own mental ill-health (Baker et al., 2014; Salaheddin & Mason, 2016; Shea et al., 2019). Given the dynamic relationship between help seeking, the influence of psychosocial factors may fluctuate dependent on environmental context.
For Australian men living in non-urban settings, the image of a rural mythology encouraging self-sufficiency, resilience, and hardiness, complicates clear understanding of the degree that intrinsic barriers (e.g., stoic masculinity) exist. Given the unique and diverse factors experienced in regional, rural, and remote Australia, a combination of intrinsic and extrinsic barriers such as economic, political, social, and cultural factors may contribute to differences in expressions of traditional masculinity. There has been an identified need to focus on work identity, financial stressors, hope for the future, community stress, inadequate and insecure funding of rural services, and a lack of a workforce trained to recognise these rural contextual factors, especially in times of natural disaster (Hart et al., 2011). Contention exists regarding rural populations being treated as a homogeneous entity, particularly without adequate acknowledgement or understanding of the differences within non-urban populations and difficulties faced in these regions such as cyclical natural disasters and reduced access to mental health services (Fraser et al., 2002; Hunter, 2007; Judd & Humphreys, 2001). The degree to which masculinity and non-urbanality predominate as maintaining factors for mental health disparities in non-urban populations is yet to be determined.
The overall aim of this project was to investigate whether traditional masculine norms impact attitudes toward mental health help seeking in Australian men living in regional, remote, or rural settings. The following research hypotheses were examined: H1) Conformity to masculine norms and attitudes toward seeking psychological help are negatively related; H2) Conformity to masculine norms and barriers to help-seeking are positively related; H3) Barriers to help-seeking and attitudes toward seeking help are negatively related, and H4) The association between conformity to masculine norms and attitudes toward seeking psychological help was mediated by barriers to help-seeking. We postulate that barriers to seeking help may mediate the relationship between adherence to traditional masculinity norms and attitudes toward psychological help, given their potential to amplify normative influences. These barriers may intensify the impact of masculine norms, thereby shaping attitudes and behaviours related to mental health help-seeking. Lastly, we hypothesised H5) that gender role conflict will significantly influence men’s attitudes toward seeking support for mental health services, with higher levels of gender role conflict being associated with more negative attitudes towards help-seeking, and that H6) perceived barriers to help-seeking will mediate the relationship between gender role conflict and attitudes toward seeking mental health support. These hypotheses are informed by an extensive body of literature demonstrating that adherence to traditional masculine norms, often leading to gender role conflict, is consistently linked to men’s reluctance in seeking mental health support, thereby underscoring the proposed negative relationship between gender role conflict and attitudes towards help-seeking.
Methods
Procedure
Participants were recruited through paid advertising on a dedicated study Facebook page (2020 Men and Mental Health Survey - @CQUMensHealthSurvey) as well as through personal networks and word of mouth. Inclusion criteria were i) males, ii) currently living in Australia, and iii) aged 18 years and over. There were no exclusion criteria. Consenting participants responded to demographic questions and validated measures of masculine norms, perceived barriers to help seeking, and attitudes to help-seeking for mental health issues. Participants with full-completion survey responses were eligible to enter the draw for an AUD$100 gift card. Participants entering the draw were redirected to a secondary survey to ensure anonymity of their response. The draw was conducted using a Microsoft Excel random name formula after the completion of data collection. Ethics approval was obtained from the Central Queensland University Human Research Ethics Committee (approval number 2020–005).
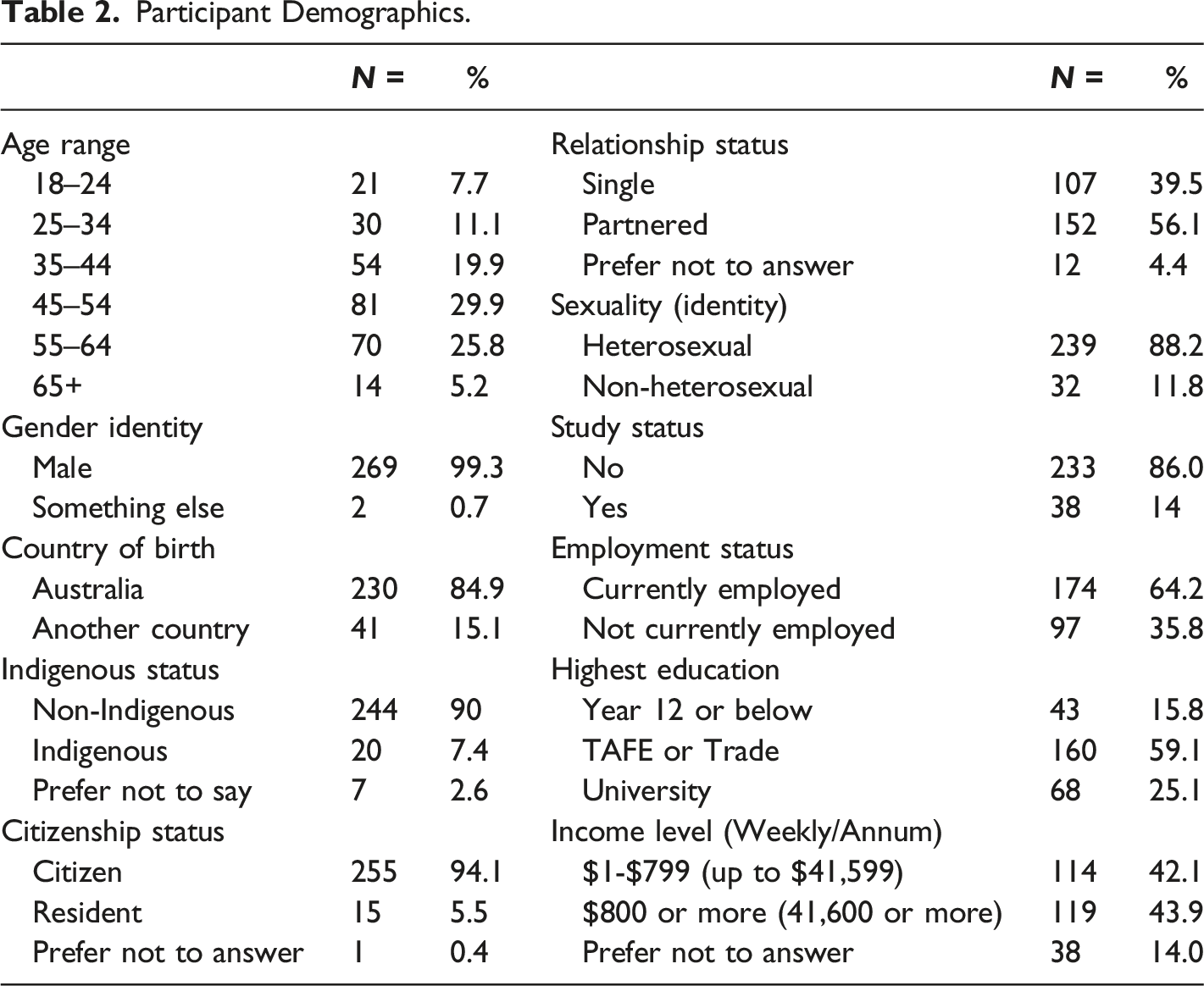
A total of 532 participants were recruited across Australia. The final sample comprised of a relatively even split between participants in a Major City (N = 261) and men living in Inner or Outer Regional areas (N = 171; N = 90 respectively), with a small minority of participants indicating they lived in Remote (N = 8) or Very Remote (N = 2) areas of Australia. Note, the present research has an identified target population of men living in regional, rural, and remote Australia. As such, the final sample for the primary analyses of focus in the current paper is the consolidated non-urban group (N = 271).
Measures
Demographics
Demographic variables were adapted from the 2016 Australian Census (Australian Bureau of Statistics [ABS], 2016) and included: Age, sex, country of birth, Aboriginal or Torres Strait Islander identity, citizenship status, language spoken at home, relationship status, state or territory, postcode and/or town, whether residence has changed in the past 5 years, employment and/or study status, highest year of secondary education completed, highest post-secondary qualification, and weekly or annual income.
Help Seeking Patterns
Additional questions were asked about patterns of engagement with health general practice (“Have you seen a GP in the past 12 months?”) and psychological services (“Have you seen a psychologist or other mental health professional in the past 12 months?”), and regarding who participants would seek help for psychological concerns (“Who would you go to for help if you were experiencing a personal mental health problem?”). A single item was added asking a participant’s sexuality (Do you consider yourself to be: straight or heterosexual, bisexual, gay or homosexual, something else, prefer not to answer). Primary residence was determined by a systematic recoding of responses to demographic variables (state, postcode, and/or town). ABS methodology was used to sort responses into one of five geographic locations: Major City, Inner Regional, Outer Regional, Remote, Very Remote. This approach adopts the Accessibility or Remoteness Index of Australia (ARIA+) standard, and these locations were characterised based on the most recent 2016 Australian Census.
Traditional Masculinity
Two common measurements of concepts attributed to masculinity are the Male Role Norms Inventory – Short Form (MRNI-SF) (Levant et al., 2010) and Gender Role Conflict Scale – Short Form (GRCS-SF; Wester et al., 2012, adapted from original GRCS; O’Neil et al., 1986).
The
The
Barriers to Help Seeking Scale
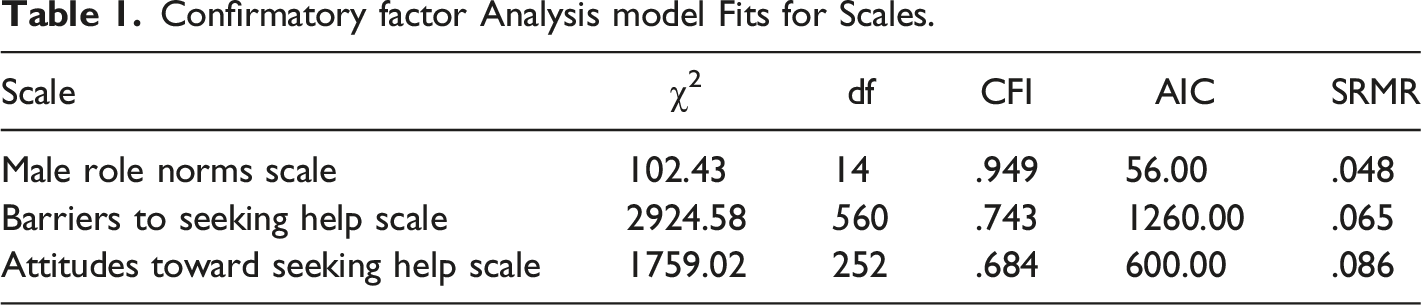
A 39-item version of the BHSS (Fennel et al., 2018, adapted for Australian context from the original BHSS; Mansfield et al., 2005) was used to establish the degree to which perceived barriers to help seeking may exist within the population. Responses are on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), rating the degree to which participants agree that an item is a perceived barrier toward seeking help. The reliability of the scale was strong in this study (α = .94).
Inventory of Attitudes Toward Seeking Mental Health Services
The IASMHS (Mackenzie et al., 2004) is a 24-item measure assessing an individual’s attitudes towards seeking mental health services. Responses are on a 5-point Likert scale (1 = disagree to 5 = agree), with participants endorsing their level of agreement with a particular attitude or perception toward mental health support. Nine items are reverse scored to yield summed domain scores and a total attitude score, with higher scores indicating more positive attitudes toward help seeking. The reliability of the scale was strong in this study (α = .90).
Statistical Assumptions Tests
We conducted assessments to ensure the statistical assumptions of multivariate analysis were met. The research variables demonstrated normality, indicated by skewness and kurtosis values falling within the ± 2 range (George & Mallery, 2010). Adequate internal consistency was affirmed by reliability coefficients exceeding .70. Moreover, the dataset was complete without any missing data. Outlier detection using Mahalanobis Distance led to the exclusion of 12 individuals from the dataset as outliers (Hayes, 2022).
Power Analysis
We conducted a Monte Carlo Power Analysis for Indirect Effects (Zhang, 2014) as an a posteriori procedure to determine the power of the study. Utilising this R-based tool, we computed the target sample size for conducting two consecutive mediational analyses. The calculation yielded a power of .35 at a significance level of .05, below the recommendations for a serial multiple mediation model (Schoemann et al., 2017).
Statistical Analysis
Confirmatory factor Analysis model Fits for Scales.
The Baron and Kenny (1986) four step process was used to establish the appropriateness of mediation. Statistical analyses were performed using the IBM SPSS Statistical Software package V26. Main analyses were run in a stepwise manner. First, multiple regression investigated whether any of the demographic variables were significantly predictive of attitudes toward help-seeking for mental health issues – the outcome of focus in the current paper. Second, multiple regression was conducted, to establish the relationship between the total scores on the two masculinity-related predictor variables (MRNI-SF, GRCS-SF) as traditional masculinity and the outcome variable (IASMHS). Mediation analyses were conducted using the PROCESS Macro for SPSS (Hayes, 2017). Direct and indirect effects were estimated using bootstrapping based on 5000 replications with 95% bias-corrected confidence intervals.
Results
Sample Demographics
Participant Demographics.
Measured Constructs
Means, Standard Deviations, and Correlations of Predictor and Outcome Variables.
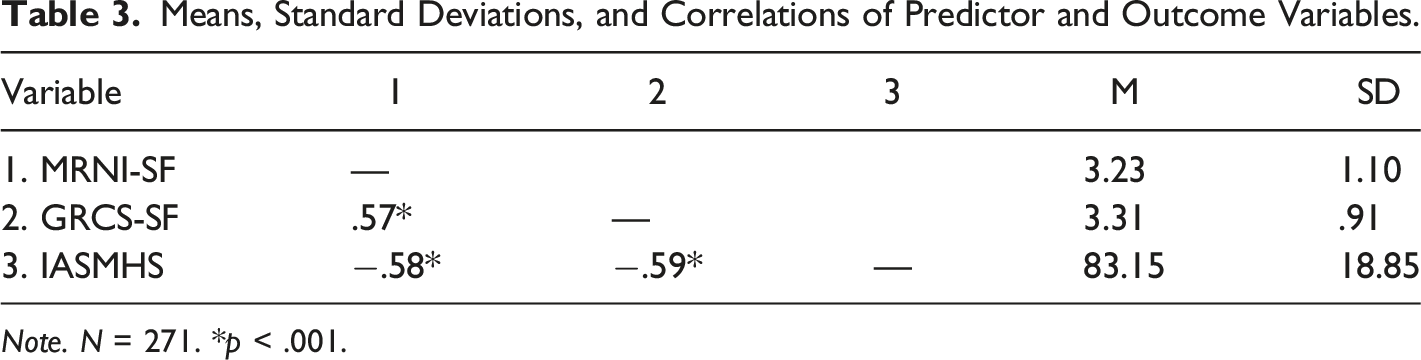
Note. N = 271. *p < .001.
Attitudes Toward Mental Health Help Seeking
Regression Analysis Summary for the MRNI-SF as Predictor of Attitudes Toward Help-Seeking for Mental Health Issues.
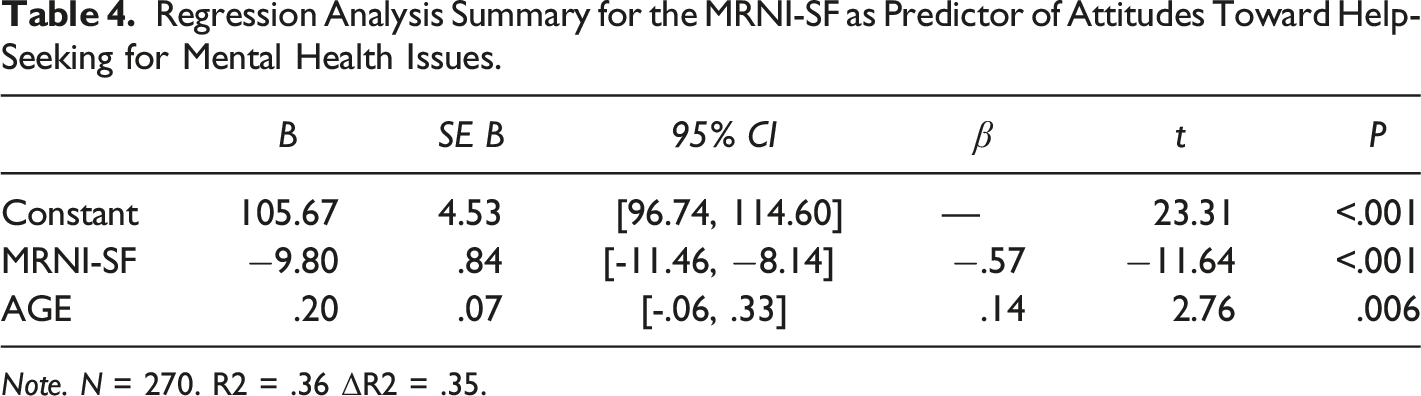
Note. N = 270. R2 = .36 ΔR2 = .35.
Regression Analysis Summary for the GRCS-SF as Predictor of Attitudes Toward Help-Seeking for Mental Health Issues.
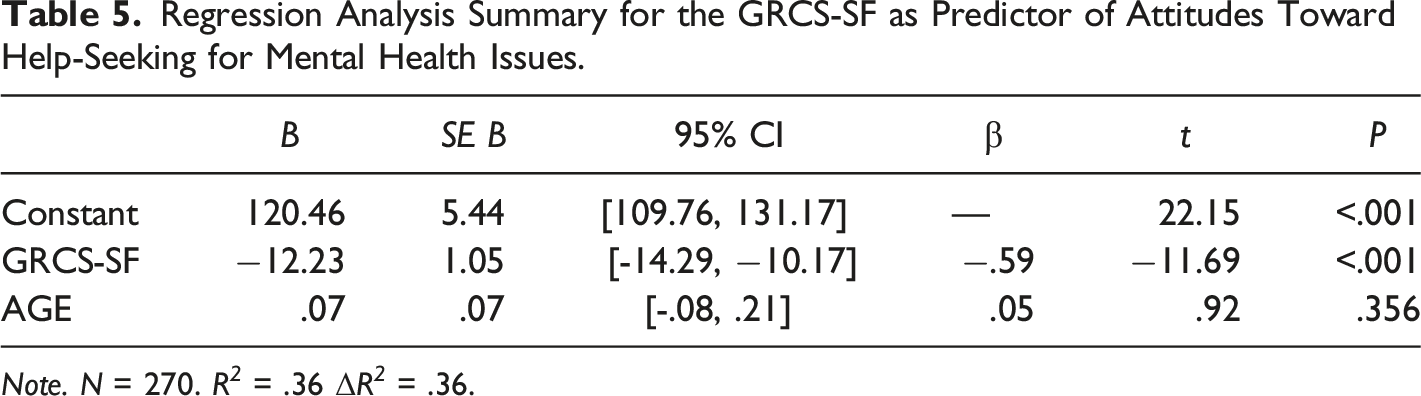
Note. N = 270. R 2 = .36 ΔR 2 = .36.
Barriers as a Mediating Factor
Male Role Norms
The standardised direct effects of male role norms on perceived barriers to help seeking was statistically significant (b = .57, SE = .84, p < .001, 95% CI [-11.46,-8.14]), as were the direct effects between perceived barriers and attitudes toward mental health help seeking (b = −.66, SE = 1.23, p < .001, 95% CI [-20.14, −15.31]). The direct effect of male role norms on attitudes toward mental health help seeking was significant (b = −.20, SE = .71, p < .001, 95% CI [-8.09, −5.30]). The indirect effects of traditional masculinity on attitudes toward mental health help seeking (b = −.57, SE = .84, p < .001, 95% CI [-11.46, −8.14]) demonstrated partial mediation through the perceived barriers to help seeking.
Gender Role Conflict
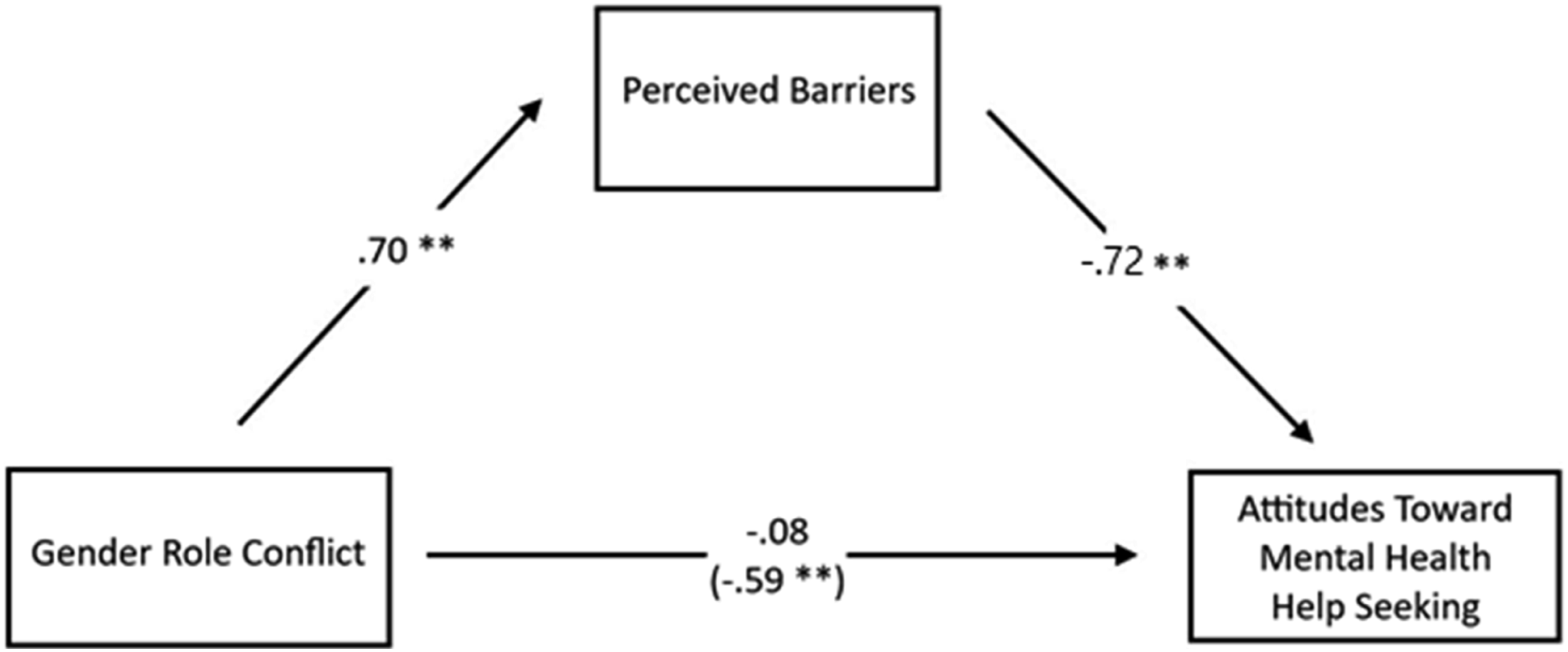
The standardised direct effects of gender role conflict on perceived barriers to help seeking was statistically significant (b = .59, SE = .1.05, p < .001, 95% CI [-14.29, −10.17]), as were the direct effects between perceived barriers and attitudes toward mental health help seeking (b = −.72, SE = 1.49, p < .001, 95% CI [-22.23, −16.35]). The direct effect of gender role conflict on attitudes toward mental health help seeking was no longer significant (b = −.08, SE = 1.16, p = .15, 95% CI [-3.95, −.62]). The indirect effects of gender role conflict on attitudes toward mental health help seeking (b = −.59, SE = 1.05, p < .001, 95% CI [-14.29, −10.17]) demonstrated full mediation through the perceived barriers to help seeking. Figure 1, 2 Standardised regression coefficients for the relationship between male role norms and men’s attitudes toward seeking supports for mental health services. The standardised regression coefficient between male role norms and men’s attitudes toward seeking supports for mental health services is in parentheses. **p < .001. Standardised regression coefficients for the relationship between gender role conflict and men’s attitudes toward seeking supports for mental health services. The standardised regression coefficient between gender role conflict and men’s attitudes toward seeking supports for mental health services is in parentheses. **p < .001.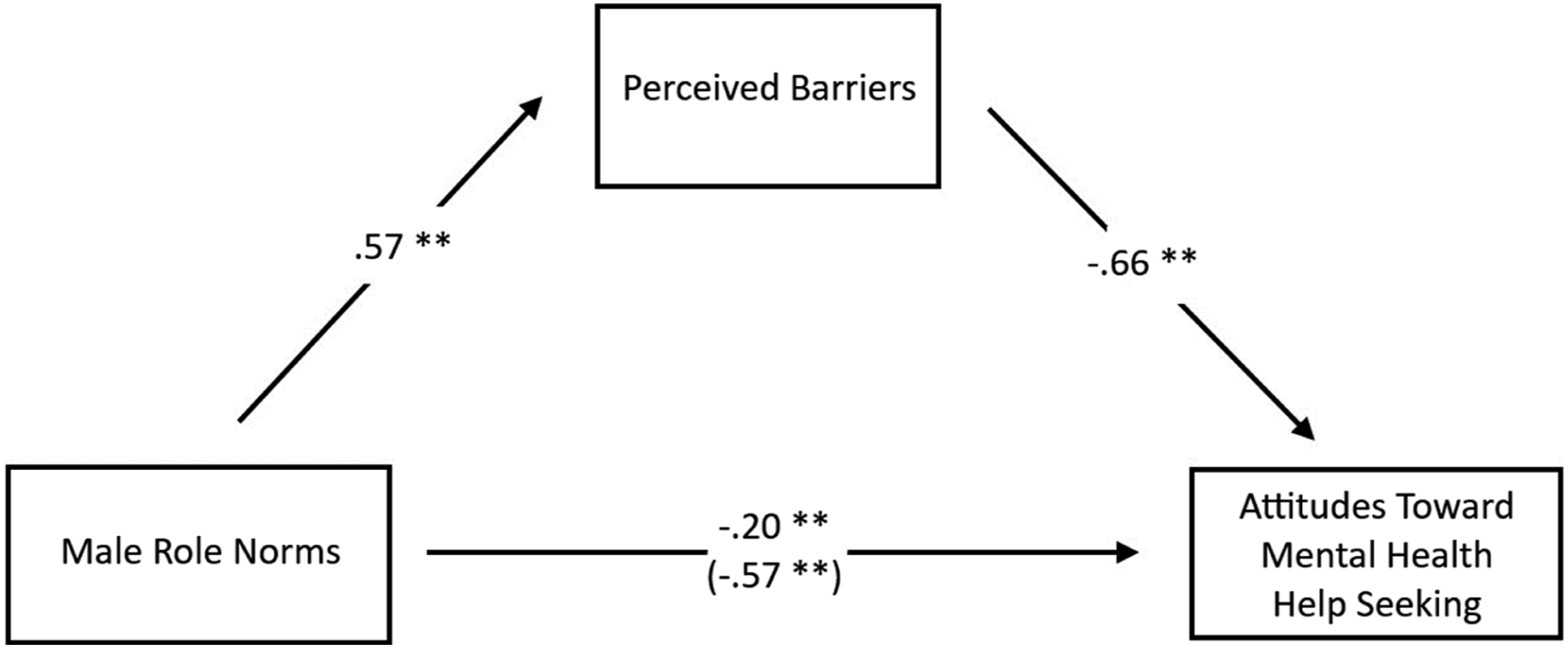
Discussion
This overarching aim of this study was to investigate whether traditional masculine norms impact attitudes toward mental health help seeking for men living in regional, rural, and remote Australia. In this study, four primary hypotheses were examined to understand the relationship between conformity to masculine norms, barriers to help-seeking, and attitudes toward seeking psychological help among men, particularly in non-urban settings. The first hypothesis posited a negative relationship between conformity to masculine norms and attitudes toward seeking psychological help. The results confirmed this hypothesis, demonstrating that adherence to traditional masculine norms significantly predicted negative attitudes toward help-seeking for mental health issues. This finding aligns with existing research highlighting how rigid adherence to traditional masculine norms can act as a deterrent to seeking psychological assistance (Mansfield et al., 2005; Seidler et al., 2018), reinforcing the importance of addressing these norms in mental health promotion efforts. The second hypothesis proposed a positive relationship between conformity to masculine norms and barriers to help-seeking. The findings partially confirmed this hypothesis, indicating that traditional masculine norms were associated with an increase in perceived barriers to help-seeking. However, this relationship was not as strong as expected, implying that while conformity to masculine norms does contribute to perceived barriers, other factors may also play a role in influencing these barriers. The third hypothesis suggested a negative relationship between barriers to help-seeking and attitudes toward seeking help. This hypothesis was confirmed as the study revealed that higher perceived barriers to seeking help were linked to more negative attitudes toward mental health help-seeking. This finding underscores the significance of addressing barriers individuals face in seeking mental health support to improve their attitudes and encourage help-seeking behaviour.
The implications of these relationships are important when delivering interventions intending to address intrinsic attitudinal barriers for men. In Australian cultural norms, particularly prevalent among men residing in non-urban areas, a rural mythology fosters values of self-sufficiency, resilience, and rugged determination (Wainer & Chesters, 2000). This ethos embodies the essence of a stoic and independent character, deeply ingrained in the collective identity of individuals within these settings. These negative intrinsic barriers and attitudes may contribute to men’s ambivalence to seek help for mental illness, drop out of services prematurely, or delay or defer help seeking altogether (Mansfield et al., 2005; Seidler et al., 2018). Importantly for non-urban cohorts, research examining intrinsic factors (e.g., rural stoicism and self-reliance) has provided support for these factors in contributing to decision making regarding seeking help for mental health concerns (Hull et al., 2017). Hull et al. (2017) operationalised stoicism through the facets of emotional control, self-reliance, and problem minimisation, traits often attributed to traditional masculinity (emotional restrictedness, toughness). Furthermore, men are more likely to express hesitation toward mental health help-seeking when compared to help-seeking for physical health (Fennell et al., 2018). Taken together, the research substantiates the current findings and aligns with perceptions that the therapeutic relationship requires men to violate masculine norms and relinquish control, discuss emotions, and embrace vulnerability (Berke et al., 2018; Seidler et al., 2018). These perceptions run counter to stereotypically masculine ideals of emotional restrictedness, stoicism, control, and the tendency to minimise problems. Therefore, while assumptions are that rural men are less likely to seek help for mental health concerns, the current data directs future research towards mechanisms being more closely linked to adequacy of services rather than the availability or attitudes toward help-seeking.
The fourth hypothesis posited that the association between conformity to masculine norms and attitudes toward seeking psychological help is mediated by barriers to help-seeking. The results affirmed this hypothesis, illustrating that perceived barriers to help-seeking acted as a mediator between adherence to masculine norms and negative attitudes toward seeking mental health assistance. These data suggest that the impact of traditional masculine norms on attitudes toward help-seeking is partially explained by the barriers perceived by individuals. These findings fit with extant work in this area, which found significant associations between masculine norms and help-seeking attitudes through path analyses, revealing indirect effects from other factors (e.g., emotionality) which may also have represented barriers. Notably, for gender role conflict, a full mediation was present, whereby barriers to help seeking mediated the relationship between gender role conflict and attitudes toward help seeking. Exploring these mediation concepts further suggests that, while masculine norms have a significant influence on attitudes, perceived barriers may play an equally crucial role. Comprehending the extent of mediation informs precise interventions, allowing targeted focus on normative and barrier-related facets for optimal outcomes. Tailored health messages should pinpoint perceived barriers related to mental health help-seeking arising from gender role conflict, rather than broadly addressing male role norms. Additionally, recognising the variable influence of these mediators underscores the necessity for customized approaches to enhance favourable attitudes towards mental health assistance, especially in non-urban contexts.
Regarding our fifth hypothesis, the findings of this study align with the established literature, confirming that higher levels of gender role conflict are significantly associated with more negative attitudes toward seeking support for mental health services among men (Lynch et al., 2018; Seidler et al., 2018; Smith et al., 2008; O'Neil, 2008; Rowbottom et al., 2012). Regarding the sixth hypothesis, the present data somewhat substantiates previous research, which has also demonstrated the mediating role of help seeking barriers between gender role conflict and willingness to seek help (Pederson & Vogel, 2007). Studies conducted both with Canadian men (Seidler et al., 2018) and within a mixed-sex Australian rural context (Fennell et al., 2018; Hull et al., 2017) point to both attitudinal and structural barriers influencing mental health help-seeking. While these studies were not designed to examine traditional masculinity, many of the attitudinal barriers share an overlap with how traditional conceptualisations of masculinity are measured. These include elements such as problem minimisation, need for self-reliance, and stoicism or the need for emotional control. Efforts to improve mental health of men living in non-urban communities may consider, more carefully, the way health messages could be targeted to optimise help seeking. Further research is required to test the feasibility of incorporating elements of traditional masculinity which may facilitate receptivity of health messages in non-urban communities of men, particularly those in non-urban areas of Australia.
Recent research has shed light on the nuanced role of masculinity within the framework of Social Identity Theory (Kantar & Yalçın, 2023a), offering a valuable foundation for exploring how elements of traditional masculinity could be strategically integrated into health messages. Drawing together the present data and recent research, future studies could rigorously examine the effectiveness of tailored health messages that incorporate aspects of traditional masculinity in resonating with men, especially in remote and regional areas. This approach aligns with the critical need to design interventions that consider the unique sociocultural contexts of non-urban communities, as highlighted by Galdas et al. (2005). By exploring how masculinity influences receptivity to health messages, future research can contribute to the development of targeted strategies to bridge the gap in healthcare accessibility and promote proactive health-seeking behaviours among men in these settings.
Limitations
There are some limitations worth noting for this study. Firstly, the low response rate by men living in more rural and remote areas of Australia justified the homogenisation of the present non-urban sample; however, the degree that these findings as a whole would hold across all individual regions of Australia is unclear. Future research may consider more targeted sampling of these specific areas for clarity. Furthermore, the study was underpowered, and ultimately, a larger sample of participants was required. A further limitation of this study pertains to the potential sampling bias, where despite data collection from 532 individuals, the analyses were conducted on a subset of 271 rural participants, potentially introducing sample bias. Secondly, the cross-sectional design of the study limits capacity for understanding how masculinity may be flexible, enacted, and contextual, and how traditional masculinity within this population changes over time. Given the trend to rejecting traditional masculine ideologies, in-depth qualitative research is required to understand how men in non-urban, particularly in regional, rural, and remote areas of Australia conceptualise, enact, and experience their own individual masculinities. An important consideration when examining masculinity in present research are the measurement limitations. It may be the case that the present findings are an artefact of the way traditionally masculinity is measured within populations. The current study’s scales were chosen for their robust evidence base; however, they rely on decontextualized endorsements of masculinity that may be overly reliant on stereotypes.
Implications and Future Directions
Understanding the barriers that exist for this cohort may assist in improving the mental health disparities for men living in non-urban areas of Australia. Extrinsic barriers such as service availability, affordability, and the appropriateness of services limit engagement with help-seeking (Baker et al., 2014; Salaheddin & Mason, 2016; Shea et al., 2019). The present research also demonstrates the role of traditional masculinity’s intersection with the perception of intrinsic barriers, which in turn shape attitudes toward mental health help-seeking. Our results suggest a role for targeted messaging and flexible service delivery that ameliorates barriers to help seeking, rather than stereotypical notions of masculinity or rural stoicism. Efforts to improve mental health in communities must be founded on a clear understanding of factors that influence help-seeking within the healthcare system (Hull, 2017).
Researchers and practitioners may consider a more comprehensive range of stakeholder engagement when designing programs and health interventions for men living in non-urban areas. For practitioners specifically, best practices for clinical intervention for men and, within the masculinities field, could be improved through diligent consideration given to stereotyped assumptions and examination of how current perceptions perpetuate disparities in men’s health. However, further investigations may yield more important insights. For example, by examining the indirect effects of traditional masculinity as a direct influence on behaviour. Traditional masculinity may not be the mechanism that creates negative attitudes toward mental health help seeking, but rather influences the beliefs that a barrier as a critical block to help-seeking. Researchers should consider the contextual nature of masculinity as an enacted, dynamic, and relational process, rather than a static concept.
Conclusion
This research examined how men living in regional, rural, or remote Australia endorse traditional norms associated with masculinity. The study also investigated how these norms affect attitudes toward mental health help seeking and whether the perceived barriers that exist for non-urban men mediate these relationships. Results underscored that traditional masculinity, while not a strongly held attitude in this population, still negatively impacted men’s attitudes toward mental health help seeking. The endorsement of traditional masculine norms was associated with perceived barriers, a factor which also mediated the relationship between masculinity and attitudes toward mental health help seeking. For gender role conflict specifically, a full mediation was present, whereby barriers to help seeking mediated the relationship between gender role conflict and attitudes toward help seeking. For Australian men living in non-urban areas more careful consideration is required regarding how health messages could be targeted to optimise help seeking. Further investigations which incorporate stakeholders, such as clinicians, community groups, government agencies, and mental health organisations more fully, may facilitate receptivity of health messages in non-urban communities of men, across regional, rural, and remote areas of Australia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.