
Abstract
The literature on African American (AA) men generally tends to focus on negative aspects of their health, but a more balanced approach is needed to understand positive factors that contribute to their overall well-being. This exploratory cross-sectional study examined the effect of different components of emotional wellness (happiness, self-esteem, and lack of stress) on AA men’s perceived overall health. The Wellness Self-Perception Questionnaire was administered among 115 AA men aged 18 to 45. Logistic regression analyses revealed that only happiness and self-esteem significantly increased the odds of better perceived overall health, with happiness being the strongest predictor. These findings suggest that broadening and strengthening the focus on positive aspects of AA men’s emotional health may improve their perceived overall well-being.
Overall health is affected by physical, mental/emotional, and social factors (World Health Organization, 1947). While the literature clearly demonstrates the important contribution of emotional wellness to overall health (see Diener & Chan, 2011 for a review), it is often overlooked, especially in the African American (AA) male population. Research on AA men’s mental health remains sparse (Sohail et al., 2014, Ward & Besson, 2013, Watkins et al., 2006, Watkins & Neighbors, 2007) despite more attention to this topic recently. Furthermore, the literature that does focus on AA men and emotional health generally centers on negative aspects and contributors. This limits a full understanding of the various elements of emotionality that might affect these men. Building on previous findings by the authors (McNeish et al., 2018), which highlighted that AA men perceived emotional wellness was just as important to their overall health as their physical wellness, this study aims to examine how different components of emotional wellness affect AA men’s perceived overall health.
Relevant Literature
“Research on the lives of AAs is almost irrevocably linked to concepts of distress and ‘risk.’ The field has not imagined AAs as people who experience joys, desires, passion, and growth or who make love or compassionate sacrifices for others” (Mattis et al., 2016, p. 85). There have been literature reviews and meta-analyses on the topic of AAs’ mental health, but they tend to emphasize the psychological distress that these individuals experience and the associated coping mechanisms (Clark et al., 1999, Lee & Ahn, 2013, Pieterse et al., 2012). Even when the meta-analyses focused on AA men’s well-being, the majority of the themes identified still revolved around the negative aspects of their mental health, including depression, fear of vulnerability, mistrust, racism/discrimination, substance abuse, and stress (Watkins et al., 2010).
AA men face many unique challenges that affect their health outcomes, therefore it is understandable that the literature primarily focuses on negative determinants and outcomes. One determinant that is often associated with negative health and other outcomes for AA men is their perceived hyper-masculinity. The unique intersection of being an AA and being male is a likely contributor to why AA men are seen as hyper-masculine (Wolfe, 2003). While most men conform to traditional masculine values to some extent, there is evidence to suggest that AA men are likely to endorse these values to a stronger degree than White men (Levant et al., 2003, 2007). Men who are more likely to embrace and conform to masculine norms are less likely to seek health services and therefore tend to have poorer health outcomes. Literature reviews and meta-analyses have shown that adherence to masculine norms is linked with a range of worse physical and mental health outcomes (Garfield et al., 2008, Wong et al., 2017). However, research also indicates that AA men’s definition of manhood comprises prosocial and positive characteristics (Griffith et al., 2015). These researchers also found that AA men’s constructions of manhood and health are intertwined, with a common emphasis on longevity, fulfillment of responsibilities, independence, and their legacy. A special series on AA men and their health acknowledged the overrepresentation of the negative outcomes and risk factors in AA men’s health literature and the need for a more positive focus on this topic area (Wade & Rochlen, 2013). Fortunately, in the last decade, there has been a movement to explore masculinity using a positive psychology positive masculinity paradigm and advocacy for studying masculinity through a more prosocial lens (McDermott et al., 2019).
The overemphasis on pathology neglects the personal strivings of these individuals as well as their strengths. As Snyder et al., (2011) warned, focusing solely on pathologies may lead to incomplete inquiry. Therefore, in addition to understanding the challenges that lead to suffering among AA men, it is equally important to explore the strengths and virtues that contribute to their emotional well-being. People can, in effect, flourish if certain conditions are met (Wong, 2007). Seligman and Csikszentmihalyi (2000) noted three foci that serve as indicators of optimal human flourishing. These are positive experiences, positive states, and positive institutions. Positive experiences are at a subjective level and include valued experiences such as well-being, happiness, contentment, and hope. Positive states and traits are at the individual level and include traits such as perseverance, courage, and spirituality. Positive institutions operate at the group level, concerned with virtues such as altruism, civility, and nurturance. People who experience high levels of happiness and are living a life that is meaningful in different areas (e.g., spirituality, family, and work) may experience greater well-being.
Emotional Wellness
In this study, emotional wellness was defined as “a person’s ability to cope with daily circumstances and to deal with personal feelings in a positive, optimistic, and constructive manner. A person with emotional wellness is generally characterized as happy, as opposed to depressed” (Corbin et al., 2014, p. 5). As the definition suggests, happiness is a significant component of emotional wellness. Happiness (or subjective well-being) is comprised of “more positive affect, less negative affect, and greater life satisfaction” (Ryan & Deci, 2001, p. 161). Positive affect is the extent to which a person feels joy or contentment, and negative affect is the extent to which a person feels sadness or fear. These emotions are brief and therefore unconscious; however, they are brought to awareness through physiological arousal of thoughts. Positive emotions may lead to activities that promote well-being like altruism, for example. They may also lead to improved psychological functioning, like problem-solving ability. Alternatively, negative emotions may lead to a downward spiral of depressive symptomology (Garland et al., 2010). According to the Broaden-and-Build Theory of positive emotions, the effects of positive emotions enhance psychological functioning by broadening thought-action repertoires to open one’s mind to alternative strategies to deal with problems, undoing negative emotions by returning the body to a normal physiological state, enhancing resilience, and increasing physical, intellectual, social, and psychological resources (Fredrickson, 2001).
Extensive literature has indicated that positive emotions are linked to more positive health outcomes, meaning that happier people, for example, may live healthier lives (Diener & Chan, 2011, Lyubomirsky et al., 2005, Veenhoven, 2008). Diener and Chan’s (2011) literature review revealed that although claims that increased happiness directly lengthens life expectancy cannot be assumed, there is sufficient evidence to conclude that positive feelings, such as happiness, predicts a healthier and longer life beyond negative feelings, such as stress. Veenhoven (2008) conducted a systematic analysis of 30 longitudinal studies on happiness and longevity and found that happiness predicted longevity among healthy populations, suggesting that although happiness does not cure illness, it may act as a protective factor against illness.
In addition to happiness, self-esteem has also been widely recognized as a construct that is important to mental well-being. Self-esteem refers to people’s global appraisals of their value in different contexts and life domains. How one evaluates oneself plays a large role in defining one’s psychological well-being (Ryff, 1989). The level of self-esteem can be a protective and/or risk factor in both mental health and physical health (Mann et al., 2004). Low self-esteem can lead to internalizing and externalizing symptoms, including depression, suicidal ideation, aggression, school dropouts, and other risky behaviors. On the other hand, high self-esteem correlates with many positive outcomes, including increased happiness, higher academic achievement, job satisfaction, and better coping mechanisms in the face of stress and physical illnesses (Mann et al., 2004).
While there have been several studies touting the positive effects of happiness and self-esteem on mental health, few studies have focused on the health of AA, and even less on AA men in particular. One study, using data from the National Survey of Black Americans, found that happiness is related to physical health, which mediated the effects of self-esteem on physical health (Christie-Mizell et al., 2010). It was suggested that happiness is beneficial to physical health because of its effect on an individual’s self-esteem among AAs. In another study, the association between happiness and self-rated physical health of AA men was assessed in a population-based cross-sectional study using data from the National Survey of American Life (Mwinnyaa et al., 2018). Researchers found that AA men who rated themselves high in terms of happiness were less likely to rate their physical health as poor or fair. The results suggested happiness may be related to positive perceptions of physical health among AA men.
The Current Study
As evidence suggests, dysphoric mood, low self-esteem/low optimism, and persistent stress may put an individual at risk for depression, while happiness, high self-esteem, and low stress may serve as protective factors that lead to higher emotional wellness (Grant et al., 2013, Pieterse & Carter, 2007, Pyszczynski et al., 2004). The literature on the positive effects of these emotional well-being components exists, but research on these components’ effects on AA men’s health is limited. To address this gap and build on previous research which established that emotional wellness is an important aspect that predicts AA men’s overall health (McNeish et al., 2018), further inquiry is needed to identify the specific aspects of emotional health that contribute to perceptions of better overall health in this population. Utilizing a measure that assesses each of these components of emotional wellness (happiness, high self-esteem, and low stress), the current study examines each emotional wellness component to assess its relationship to the men’s perceived overall wellness.
Method
Sample and Recruitment Procedures
The study recruited a nonrandom convenience sample of AA men residing in a large metropolitan area in a U.S. southern region. Participants were recruited via local churches, community-based organizations, a local college, posted announcements, existing wellness initiatives, and information materials and researcher presentations at community voluntary associations. All AA males 18 years or older were eligible to participate. Paper-based surveys were self-administered in a group setting; survey packets also contained the informed consent form and a $5 incentive for participation. Instructions and the purpose of the study were explained to participants by trained graduate students.
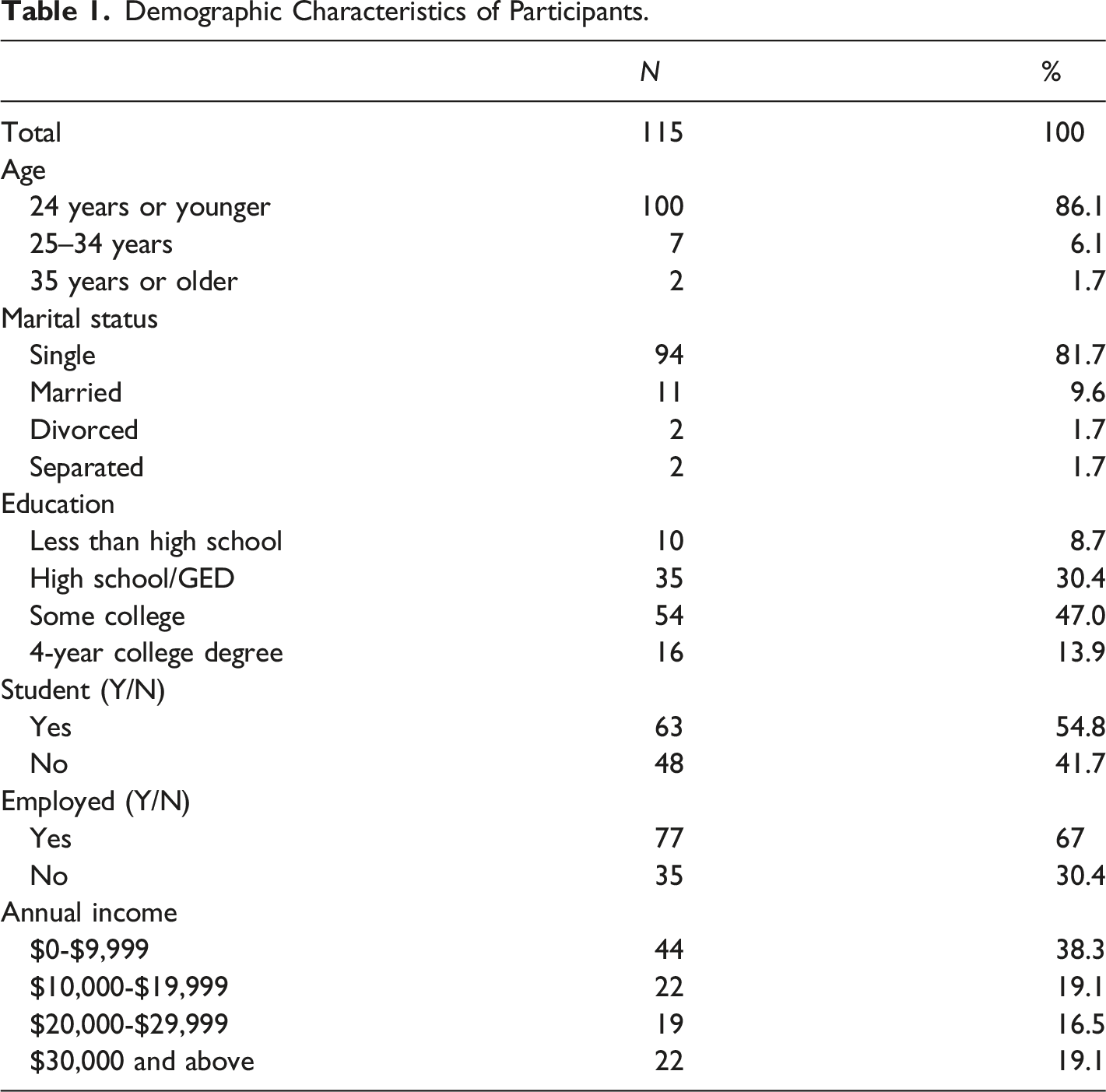
The total sample consisted of 122 AA males between 18 and 45 years old. However, seven had unusable and incomplete data, leaving 115 participants. Missing data were minimal for the study variables (i.e., only 3.4% for the emotional wellness dimension) and were assessed using the expectation-maximization (EM) algorithm (i.e., a two-step imputation process that replaces missing values with predicted values to complete the data) in SPSS Version 25 (IBM Corp, 2017).
Measures
The Wellness Self-Perception Questionnaire (WSPQ) is a 15-item scale used to assess perception of wellness on five dimensions: emotional, intellectual, physical, social, and spiritual (Corbin et al., 2014). The WSPQ was grounded on Corbin and Pangrazi’s (2001) conceptualization of wellness as a multidimensional component of positive health, which is possessed by the individuals, and often described as quality of life and well-being. Although the number of dimensions varies among researchers, the most commonly used dimensions are emotional, intellectual, physical, social, and spiritual. Each domain contains three statements for participants to rate their level of agreement on a 4-point Likert-type scale ranging from 1 (strongly disagree) to 4 (strongly agree). Because the independent variable of interest was emotional wellness, only that subscale was used in this study. It was important to understand the components of emotional wellness because they may be important personal factors in promoting behavioral health and overall health, in general. One study examined the validity and reliability of the WSPQ and revealed acceptable validity and reliability (>.70) (Odabas, 2017). The statements used in the WSPQ to assess emotional wellness were, 1) I am happy most of the time, 2) I have good self-esteem, and 3) I do not generally feel stressed. Higher ratings indicated higher levels of emotional wellness. In this study, Cronbach’s alpha for emotional wellness was .77. The dependent study variable, overall wellness, was assessed using a single item. Similarly, participants rated their overall wellness on a 4-point Likert-type scale ranging from 1 (poor) to 4 (excellent). A higher rating indicated better overall wellness.
Statistical Analysis
All emotional wellness factors (i.e., the independent variables) were treated as ordinal variables. The dependent variable, overall wellness, was dichotomized with responses of 3 (good) and above coded as “good overall wellness” and 2 (fair) and below as “bad overall wellness.” Logistic regression models were then used to predict the associations of aspects of emotional wellness with overall health. Two demographic factors (education and income) were included as covariates in the regression models due to the complex relationship between socioeconomic status and self-rated health in African Americans (Bell et al., 2020). For all analyses, SPSS version 27 was used (SAS Institute Inc, Cary, NC).
Results
Demographic Characteristics of Participants.
The link between the three aspects of emotional wellness and overall wellness was first analyzed separately in bivariate logistic regression models. Results indicated that only two components of emotional wellness independently and significantly predicted overall health. Happiness was the strongest predictor among the aspects of emotional wellness. Specifically, higher rating of happiness increased the odds of reporting better overall wellness by almost six times (OR = 5.99, 95% CI [2.15 – 16.68], p < .001). Similarly, higher rating of self-esteem was associated with 4.43 increased odds of better overall health (95% CI [1.88 – 10.44], p < .001).
The three emotional wellness components were then analyzed together in a logistic regression model (Model 1). Education level and income were added as covariates in Model 2. Model 1 was statistically significant, χ 2 (3, N = 115) = 20.46, p < .001. When examined together, the no-stress component was still not significantly associated with overall health, while happiness (OR = 6.75, 95% CI [1.47 – 30.92], p = .014) and self-esteem (OR = 2.97, 95% CI [1.09 – 8.11], p = .033) continued to predict better perceptions of overall health. Notably, the odds ratio of happiness increased while that of self-esteem decreased from the bivariate logistic regressions.
Logistic Regression of Overall Wellness (N = 115).
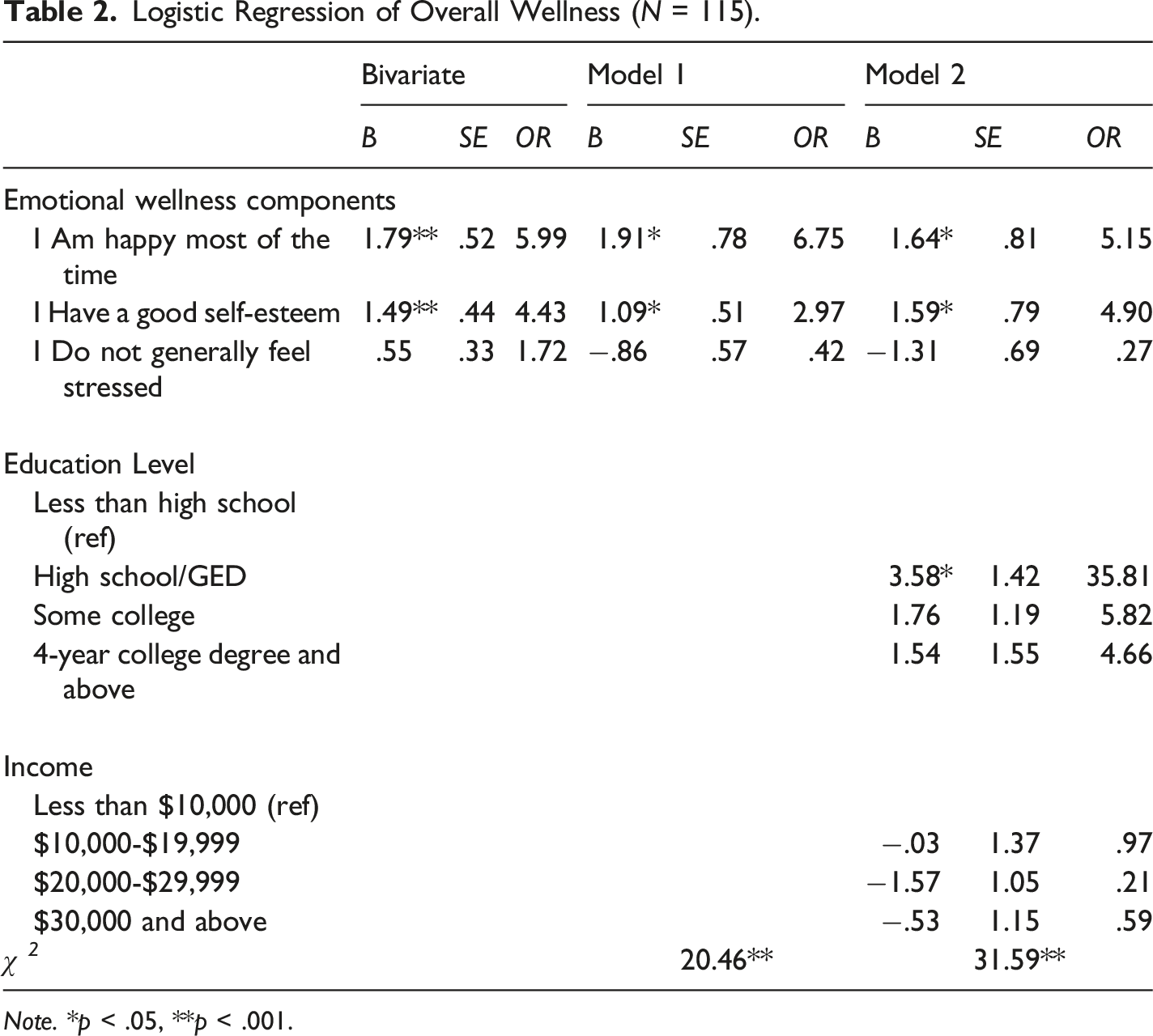
Note. *p < .05, **p < .001.
Discussion
AA males continue to have some of the worst health outcomes among all groups of males in the US. Efforts and research to improve their health have increased over time, but informational gaps remain. Addressing social determinants has been a primary focus of these efforts and research, leaving a chasm, though narrowing, in the area of emotional health research for this population. General and specific aspects of the emotional health of AA men remain an underexplored topic. This paper, therefore, further explores emotional health by expanding on previous research, which found it to be a significant predictor of better perceived overall health for AA men (McNeish et al., 2018). However, because little is known about which specific aspects of emotional health contribute to perceptions of better overall health among AA men, this study aimed to explore this gap in the literature by examining specific aspects of emotional health – namely happiness, self-esteem, and lack of stress - that contributed to positive perceptions of overall health in AA men. Research in this area is necessary to inform policy and practice to better serve this population, and disrupt the trajectory of negative health outcomes for this population.
As a large proportion of the extant literature on this population focuses on ameliorating negative conditions, the findings of this study also contribute to the overall limited knowledge on positive aspects of emotional wellness in AA men and their contributions to their perceptions of overall health. The results highlight that of the three aspects of emotional health assessed, happiness was found to be the strongest predictor of positive perceptions of overall health among the men in the study. These findings are consistent with previous studies that found a relationship between happiness and perceived health outcomes for AAs in general (Christie-Mizell et al., 2010), and AA men, in particular (Mwinnyaa et al., 2018). They also support the Broaden-and-Build Theory of Positive Emotions (Fredrickson, 2001), which states that positive emotions (i.e., happiness) are beneficial to positive outcomes (i.e., good health). Similarly, previous studies have found that happiness is positively correlated with health (Diener & Chan, 2011, Lyubomirsky et al., 2005, Veenhoven, 2008); while such studies were not specifically focused on AA men or minorities, there is some indication that this may be a universal outcome.
Self-esteem was found to positively predict overall health in the bivariate regression model, but that connection became weaker in the logistic regression model when happiness and no stress were added as covariates. Another study similarly found that happiness mediated the association of self-esteem and physical health in an AA sample (Christie-Mizell et al., 2010). The researchers found that when happiness was added to the model, there was no longer a relationship between self-esteem and physical health. Notably, in the current study, the contribution of self-esteem to overall health strengthened when demographic variables were introduced as covariates. Although there is not a clear cause for this phenomenon, it might be explained by an established connection between self-esteem and socioeconomic status (SES). Self-esteem is very closely associated with SES, and this relationship is substantially strong in young adulthood (Twenge & Campbell, 2002), which is the primary age of this sample. Therefore, SES variables might have moderated the relation between self-esteem and perceived overall health in the current study.
Somewhat unexpectedly, the absence of stress did not predict respondents reporting better overall health at all in this study. This is inconsistent with the literature indicating that stress is one of the most common factors related to emotional and physical health for AA men (Ellis et al., 2015, Watkins et al., 2010). While there is no definite explanation for why no stress was unrelated to overall health in this study, it is possibly due to how it was defined. Stress, in the instrument utilized in this study, was conceptualized as absence of stress (instead of the presence of measurable stress in other studies). The perceived absence of stress may have little association with perceived overall health, unlike the presence of actual stress, indicating an area for further research. Stress is also common among AA men and it is possible that stress has become normalized in this population (Chung et al., 2014, Butler, 2017). Butler (2017) found that Black college students have reported a high degree of normalizing their stress. This study’s sample corresponds to the current study’s sample in which most are college-aged and over half are current students. The absence of stress might be a non-existent factor in this population and therefore have little contribution to perceptions of their overall health. It is also possible that the effect of happiness is so strong it lessens perceptions of stress, as the findings of Diener and Chan’s (2011) review suggest.
Notably, the majority of the current sample consists of emerging adults, ages 18 to 24, and these findings highlighted some insights into this group’s emotional wellness. Previous research indicates that for AAs, emerging adulthood marks a developmental stage that is at a higher risk of depression (Assari et al., 2015). Specifically, AA young adults were found to have a higher lifetime prevalence of depression than older AAs (Williams et al., 2007). Inconsistent with the literature showing more negative adjustment in AA emerging adults, this study’s findings revealed that this population favorably rated their emotional wellness and overall health. This may be explained by the use of different population samples across studies and the fact that men in general tend to report more positive perceptions of their overall health (Olsen & Dahl, 2007). Additionally, educational attainment, particularly earning a high school diploma or GED, was positively correlated with health. This further emphasizes the importance of promoting positive emotions in AA men overall, particularly in populations that have limited access to education and other health-promoting opportunities.
Implications for Practice
In programs and treatment settings, service recipients are generally asked to report and rate negative moods, such as sadness or depressive symptoms, but professionals/practitioners often fail to elicit information about positive emotions or experiences. Assessing level of happiness is not usual practice and it may be assumed that lack of depression or other negative emotions equates to happiness, but this is not the case. Absence of a negative emotion does not necessarily mean that there is a positive emotion present (David et al., 2014); negative and positive emotions are not mutually exclusive or dichotomous concepts (Larsen et al., 2001). Positive emotions can help prevent and even undo some of the harmful effects of negative emotions (Cohn et al., 2009), however, both can co-exist (Larsen et al., 2001). Therefore, assessments should include questions about both, not assuming the presence of positive emotions if negative emotions are not reported.
Many programs involving AA men (and boys), tend to focus on reducing external negative conditions rather than improving or prompting positive internal states. Both approaches are important to overall well-being; however, the former often addresses social issues by viewing AA men as victims, while the latter focuses more on the strength and resilience of AA men (cf. Pedrotti & Edwards, 2010). While there has been some shift to the latter focus in recent years, there remains a need for programs promoting the enhancement of intrinsic positive factors such as emotional/mental well-being in AA males.
In promoting happiness and well-being among AA men, two components of well-being must be considered: hedonic well-being and eudaimonic well-being (for a review, see Ryan & Deci, 2001). The hedonic component of well-being is conceptualized as subjective well-being or happiness. It includes engaging in experiences that produce high levels of positive affect, low levels of negative affect, and high life satisfaction (Diener, 2000). Mattis et al. (2016) identified two concepts that are essential to positive affect: mattering (feeling cared for by others, important to others, and noticed by others) and love. However, hedonic well-being may not by itself be sufficient to bring about lasting fulfillment in one’s life; therefore, eudaimonic well-being must also be considered when aiming to promote happiness among AA men. Eudaimonic well-being is conceptualized as psychological well-being, which is achieved by engaging in activities that create meaning and purpose in one’s life (Ryff, 1989), such as racial identity development, civic engagement, altruism, religion, and spirituality (see Mattis et al., 2016 for a review). Therefore, both hedonic and eudaimonic experiences may enhance optimal emotional/mental well-being among AA men and should equally be incorporated into any programming that is designed with this outcome in mind. Further, there has been a general movement advocating for the positive psychology/positive masculinity paradigm to study men and masculinity through a more prosocial lens (McDermott et al., 2019). A shift to utilizing aspects of positive psychology in programming can help to increase the focus on positive states, positive experiences, and positive institutions (Pedrotti & Edwards, 2010).
Limitations and Future Research
Despite the study’s contributions to the literature, some limitations should be noted. First, the study sample may not be representative of AA men overall, so generalizations should be made with caution. Future studies should include a larger and more varied sample of AA men. Inclusion of a more diverse sample of men in the future will produce results with better external validity. Future research could sample Black males generally rather than just AA men to test if the results are impacted by ethnicity. This would expand the variability of participants as well as increase the sample size. Secondly, since all of the participants self-rated their emotional wellness and overall health, there is the possibility of mono-method bias. Future studies should utilize different informants or clinical measurements to obtain a more accurate depiction of well-being. Future research should further examine the intersection between education and mental health in AA men.
In addition, this study assessed individual items in a sub-scale instead of the entire scale or instrument. This was unconventional and appeared to make the design and analyses quite simplistic. However, research on positive aspects of mental health for men, and AA men in particular, is limited with scarce instruments measuring positive emotional wellness for this population. Hence, we had to scrutinize these positive aspects using single items. Though one might question the reliability and validity of single items, some research supports the sufficiency of using single-item measures to capture a construct (Wanous et al., 1997). Regardless, findings in this study should not be conclusive evidence of how positive emotional wellness components (happiness and self-esteem) contribute more to overall health, but rather jump-start a discussion of shifting focus from a pathological view to a more strengths-based view for AA men’s health and mental health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.