
Abstract
Muscle dysmorphic disorder (MDD) is a mental disorder characterized by men’s exaggerated self-perception as insufficiently muscular and lean and pathological preoccupation with achieving a muscular body. MDD has been recognized as a risk factor associated with negative mental health outcomes in men. However, previous studies did not sufficiently explore the link between MDD and masculine depression. Therefore, the present study examines the mediating role of social interaction anxiety and the moderating role of restrictive emotionality in the relationship between MDD and masculine depression. Structured questionnaires were distributed online among 849 Israeli men. The moderated mediation analysis indicated that a positive association between MDD and masculine depression was moderated by restrictive emotionality and partially mediated by social interaction anxiety. These findings have profound meaning in terms of the psychosocial aspects of men’s lives, underlining the risk factors inherent in the association between men’s dissatisfaction with their body and their mental health.
Keywords
Muscle dysmorphia (MDD) is a disabling condition characterized by a preoccupation with one’s body size as being not large enough, a fear of being too small and weak, and by the pathological pursuit of muscularity, even though one might actually be quite muscular and lean (Chandler et al., 2009; Cunningham et al., 2017; Pope et al., 1993; Zeeck et al., 2018). In the Diagnostic and Statistical Manual of Mental Disorders, fifth Edition (DSM-5; American Psychiatric Association, 2013), it is classified as a specifier for Body Dysmorphic Disorder. This mental disorder is prevalent mostly among men in Western cultures which internalize the unrealistic image of the ideal male sociocultural body as muscular and lean in a way that is difficult for most men to achieve (Campagna & Bowsher, 2016; Grieve, 2007; Murray et al., 2019).
MDD is associated with multiple pathological behaviors and severe psychological and social impairments (Compte et al., 2022; Nagata et al., 2021). On the psychological level, individuals with MDD show a pathological preoccupation with their appearance and muscularity and experience severe body image disturbance. They hold an unrealistic perception of themselves as less lean and muscular than other men and therefore they feel ashamed and embarrassed of showing their body (Hildebrandt et al., 2006; Maida & Lee Armstrong, 2005; Olivardia et al., 2000). Consequently, on the behavioral level, excessive preoccupation with a perceived flaw (Campagna & Bowsher, 2016) is frequently related to engaging in compulsive and detrimental activities aimed at hiding, improving, or controlling it (Hartmann et al., 2020; Phillips et al., 2005). As such, men with MDD are more likely to engage in excessive exercise, rigid diets, and disruptive eating patterns (Hildebrandt et al., 2006; Nagata et al., 2021) as well as to utilize appearance- and performance-enhancing drugs and substances (Hildebrandt et al., 2010; Zeeck et al., 2018). They commonly find it difficult to maintain control over these behaviors, keep exercising even when injured (Olivardia, 2001), and feel distressed when missing a workout session (Cooper et al., 2020; Zeeck et al., 2018). On the social level, a pathological and time-consuming preoccupation with one’s appearance and body image may result in severe avoidance of social interactions and social activities, considerable limiting of occupational activities, and withdrawal from social relationships (Olivardia et al., 2000; Pope et al., 2005).
Previous studies detected a significant association between MDD and adherence to some aspects of traditional masculine norms, such as heterosexual self-presentation, positive attitudes towards violence as a means of solving problems, and emotional restriction (Blashill et al., 2020), as well as personality traits such as perfectionism and neuroticism (Mitchell et al., 2017) and insecure attachment (Fabris, et al., 2018). MDD was also found positively linked to various forms of psychopathology such as obsessive-compulsive disorder (Chandler et al., 2009; Maida & Lee Armstrong, 2005), anxiety disorders (Cafri et al., 2008; Longobardi et al., 2017), loneliness (Chaney, 2008), a sense of decreased quality of life, psychological distress, suicide ideation (Cafri et al., 2008; Cunningham et al., 2017; Phillips & Menard, 2006; Pope et al., 2005), and depression (Compte et al., 2022; Mitchell et al., 2017).
At the same time, most studies on MDD do not address the psychosocial mechanisms through which MDD is associated with negative consequences for men’s mental health, and particularly masculine depression. Furthermore, studies on MDD are typically conducted among distinct social categories such as undergraduate students (e.g., Chandler et al., 2009; Tarsuslu & Durat, 2020), cisgender sexual minorities (Nagata et al., 2021), or weightlifters and bodybuilders (Longobardi et al., 2017; Olivardia et al., 2000), insufficiently representing the general male population. The disproportionate focus on such samples limits the ability to generalize findings to a broader and diverse male population that might be dealing with body image issues as well (Blashill et al., 2020).
Therefore, the aim of the current study was to explore the role of restrictive emotionality, which constitutes one manifestation of adherence to traditional masculine norms, and the role of social interaction anxiety, in the association between MDD and masculine depression in the general male population.
Masculine Depression
Men are diagnosed with depression less frequently than women, yet there is growing research evidence suggesting that the sex gap in depression diagnostics may not stem from actual differences in prevalence rates but rather from issues related to internalization of gender role norms (Magovcevic & Addis, 2008; Oliffe et al., 2011). According to Addis (2008), the differential effects of masculinity on depression can be understood from a perspective of the dysfunction strain paradigm and gender norm conformity paradigm. The dysfunction strain paradigm (Pleck, 1995) suggests that traditional masculine norms that reinforce social expectations of men to be self-sufficient, stoic, and avoid behaviors considered feminine, constrain their self and social legitimacy to express their emotions and to seek help for their mental health issues (Branney & White, 2008), thus impairing their mental health (Levant & Richmond, 2016), including depression (O’Neil, 2012; Pleck, 1995; Wong et al., 2017). According to the gender norm conformity paradigm, gendered socialization processes create restrictive norms regarding how men are supposed to think and behave. Therefore, the degree to which men adhere to dominant masculine norms might provide not only an explanation of their mental health outcomes (Mahalik et al., 2003) but also shape how men may respond to depression (Addis, 2008; Mahalik et al., 2003). Men who adhere more strongly to masculine norms may display depression in ways that are more congruent with those norms (Cochran & Rabinowitz, 2000). They may conceal their distress from others and try to suppress their emotional pain because they might perceive it as an unacceptable expression of weakness that is incongruent with their masculine identity. They might also engage in externalizing behaviors such as drinking (Angst et al., 2002) or using drugs, aggression, risk-taking, hyperactivity (Genuchi & Mitsunaga, 2015), and impulsivity (Addis, 2008; Winkler et al., 2004), and also withdraw from family and friends, report somatic complaints, and over focus on work (Magovcevic & Addis, 2008).
Masculine Depression and Social Interaction Anxiety
The DSM-5 (APA, 2013) criteria for social anxiety disorder refer to fear or anxiety that are specific to social situations and have been exhibited for at least six consecutive months, in which the individual feels noticed and observed and experiences fear of displaying the anxiety and of experiencing social rejection. The fear and anxiety are usually grossly disproportionate to the actual situation, but as social interactions consistently provoke distress they are either avoided or tolerated reluctantly (Summers & Cougle, 2018). Studies have documented that concerns about appearance are positively related to social anxiety symptoms, which in turn precede the onset of mental and behavioral disorders such as major depression (Bittner et al., 2004; Liao et al., 2010). Yet, although previous studies indicate a decline in social interactions among individuals with MDD, to the best of my knowledge they do not explore the link between MDD and social interaction anxiety, and its role in the association between MDD and masculine depression.
Masculine Depression and Restrictive Emotionality
Socialization to restrictive masculine norms may cause men to struggle to meet standards of masculinity such as demonstrating toughness, asserting independence, avoiding weakness, and exhibiting emotion regulation and emotional restrictiveness (Magovcevic & Addis, 2008; O’Neil, 2008; Pleck, 1995). There is growing scientific evidence that the relationship between masculine norms and mental health-related outcomes may depend on specific dimensions of masculinity rather than on the general concept of masculine identity as a whole (Levant et al., 2009, 2011; Wong et al., 2017). Therefore, the current study focuses on the role of restrictive emotionality in the association between MDD and masculine depression. Restrictive emotionality is defined as “having difficulty and fears about expressing one’s feelings and difficulty finding words to express basic emotions” (O’Neil et al., 1995, p. 176), and consistently found to be related to increased stress and negative affect in men (Rice et al., 2016; Wong et al., 2017).
Hypotheses
Social interaction anxiety will partially mediate the association between MDD and masculine depression, such that beside a positive direct effect of MDD on masculine depression, MDD will be positively correlated with social interaction anxiety, which in turn will be positively correlated with masculine depression.
Restrictive emotionality will moderate the association between MDD and masculine depression, such that the positive effect of MDD on masculine depression will be more pronounced at higher levels of restrictive emotionality.
Methods
Research Population and Sample
Inclusion criteria for participating in the study were being a man aged 18 or older and having command of the Hebrew language in order to respond to the questionnaire. The current study consisted of a sample of 849 Israeli men. The mean age of men in this study was 31.32 (SD = 13.01). The mean level of education was 13.54 years (SD = 2.23), 52.9% were married or in a committed intimate relationship, 67% were employed, and 56.5% identified themselves as religious to some degree.
Procedure
The current study was conducted after receiving the approval of the committee for non-clinical research in human beings at the university with which the researcher is affiliated. A link to a structured questionnaire was distributed to a convenience sample of men through an array of online means, such as in Facebook and WhatsApp groups. Respondents were asked to complete a questionnaire that did not ask for any details that might have disclosed their identities. Before completing the questionnaire, all respondents were asked to sign an informed consent form. Since the questionnaires were distributed online, there was no way of knowing how many respondents were exposed to them and decided not to access the link, so the response rate cannot be calculated.
Measurements
Muscle Dysmorphic Disorder was assessed by the 13-item Muscle Dysmorphic Disorder Inventory (Hildebrandt et al., 2004). Responses were given on a Likert-type scale from “1 (never) to 5 (always)”. The items form three subscales: drive for size, appearance intolerance, and functional impairment. A total MDD score was calculated by summing the responses to the subscales, where a higher score indicated a higher level of MDD. Cronbach’s alpha for this scale in the current study was 0.76.
Social Interaction Anxiety was assessed by the six-item Social Interaction Anxiety Scale short form (Fergus et al., 2012). Responses were given on a Likert-type scale from “1 (not at all) to 5 (extremely)”. A total social interaction anxiety score was computed by calculating the mean score of the six items, where a higher score indicated a higher level of social interaction anxiety. Cronbach’s alpha for this scale in the current study was .86.
Restrictive Emotionality was assessed by a three-item Restrictive Emotionality subscale, which is part of the 21-item Male Role Norms Inventory - Short Form (MRNI-SF; Levant et al., 2013). Responses were given on a Likert-type scale from “1 (strongly disagree) to 7 (strongly agree)”. The total score was computed by calculating the mean of the responses to the three items, where a higher score indicated more restrictive emotionality. Cronbach’s alpha for this scale in the current study was 0.82.
Masculine Depression was assessed by the 18-item Masculine Depression Scale (Tarsuslu & Durat, 2020). Responses were given on a Likert-type scale from “1 (none or some of the time) to 4 (all of the time)”. The scale was comprised of two subscales: internalizing symptoms and externalizing symptoms. A total masculine depression score was computed by calculating the sum of the responses to all items, where a higher score indicated a higher level of masculine depression. Cronbach’s alpha for this scale in the current study was .87.
Means, Standard Deviations, and Pearson Correlation of Research Variables (n = 849).
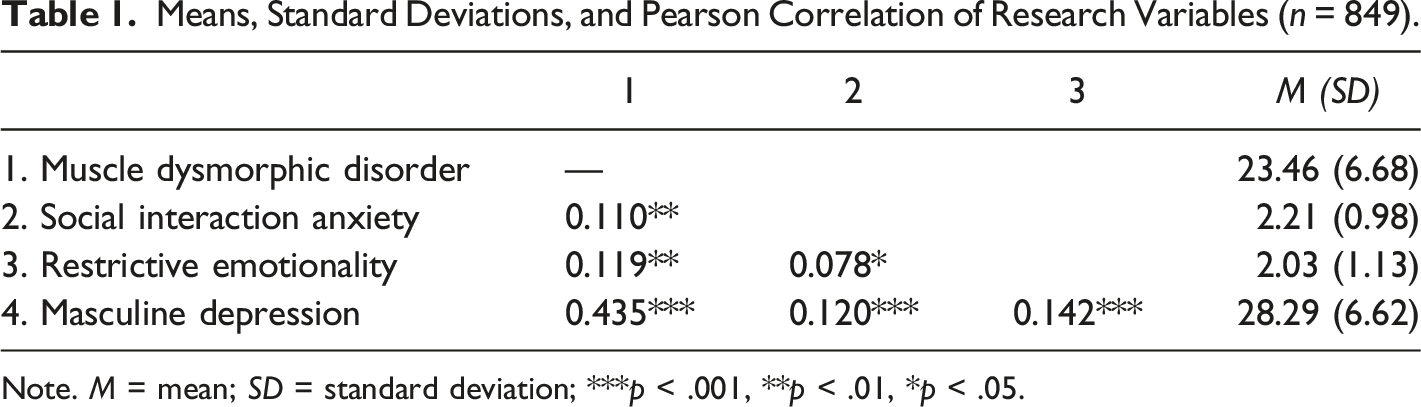
Note. M = mean; SD = standard deviation; ***p < .001, **p < .01, *p < .05.
Data Analysis
A moderated mediation model was tested using model 5 PROCESS v4.0 macro for SPSS (Hayes, 2018), with MDD as the independent variable, social interaction anxiety as a mediator, restrictive emotionality as a moderator, and masculine depression as the outcome variable (see Figure 1). In the present study, 5000 bootstrap samples were utilized and the mediating effect of the 95% confidence interval was determined. Moderation was probed by estimating the conditional direct and indirect effects at one standard deviation (SD) above the mean, at the mean, and at one SD below the mean. With the aim of avoiding a potential of high multicollinearity with the interaction term, the variables were first centered. Moderated mediation (PROCESS, 2018; Model 5).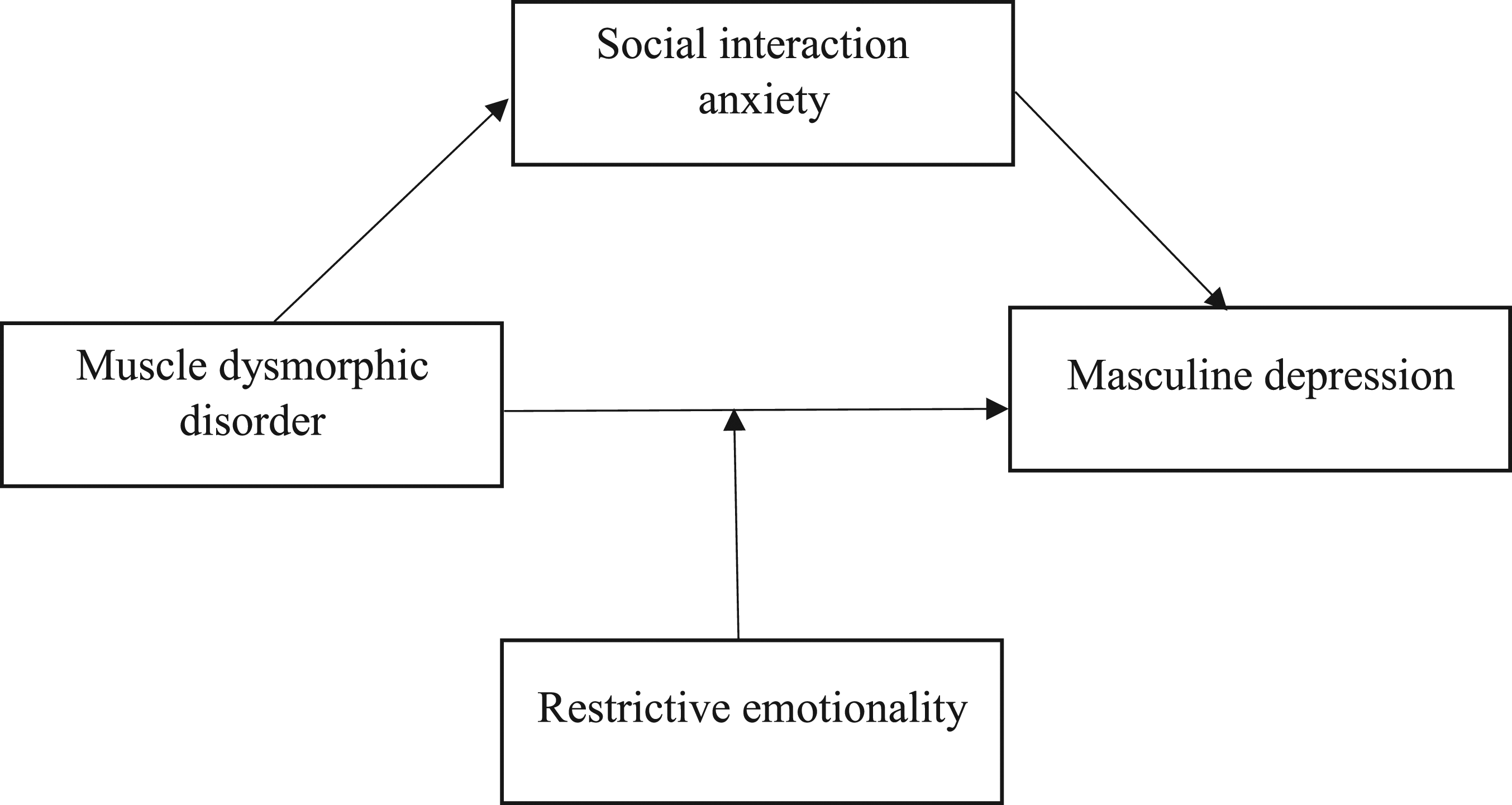
Results
In accordance with hypothesis H11, the results revealed a significant indirect effect of MDD on masculine depression, mediated by social interaction anxiety (b = 0.008, 95% CI = [.0003, .0203]). The regression analysis incorporated in model 5 PROCESS v4.0 macro for SPSS (Hayes, 2018) demonstrated that MDD was positively correlated with social interaction anxiety (b = 0.016, t = 3.23, p < .01), which in turn was found to have a positive correlation with masculine depression (b = 0.475, t = 2.308, p < .05). Also, a positive direct effect of MDD on masculine depression was detected (b = 0.397, t = 12.96, p < .001) (R2 = .223, F(4, 844) = 60.55, p < .001). Hence, social interaction anxiety partially mediated the relationship between MDD and masculine depression. Contrary to full mediation, which implies that the relationship between the independent variable and the dependent variable is not significant after introducing the mediating variable, in partial mediation the mediating variable accounts for only part of the relationship between the independent and dependent variables, while the direct relationship between the independent and dependent variables is reduced in absolute size but not nullified.
To test the hypothesis that restrictive emotionality moderates the association between MDD and masculine depression (H12), an interaction effect of restrictive emotionality and MDD was explored and found to be significant (ΔR2 = 0.021, F(1, 844) = 22.52, p < .001). In order to display the moderation effect, simple slopes for the association between MDD and masculine depression were explored at one SD above the mean (b = 0.516, p < .001), at the mean (b = 0.397, p < .001), and at one SD below the mean (b = 0.287, p < .001) of the restrictive emotionality values. The results support hypothesis H12, underlining that the positive effect of MDD on masculine depression is more pronounced at higher levels of restrictive emotionality (see Figure 2). The moderating effect of restrictive emotionality in the association between MDD and masculine depression.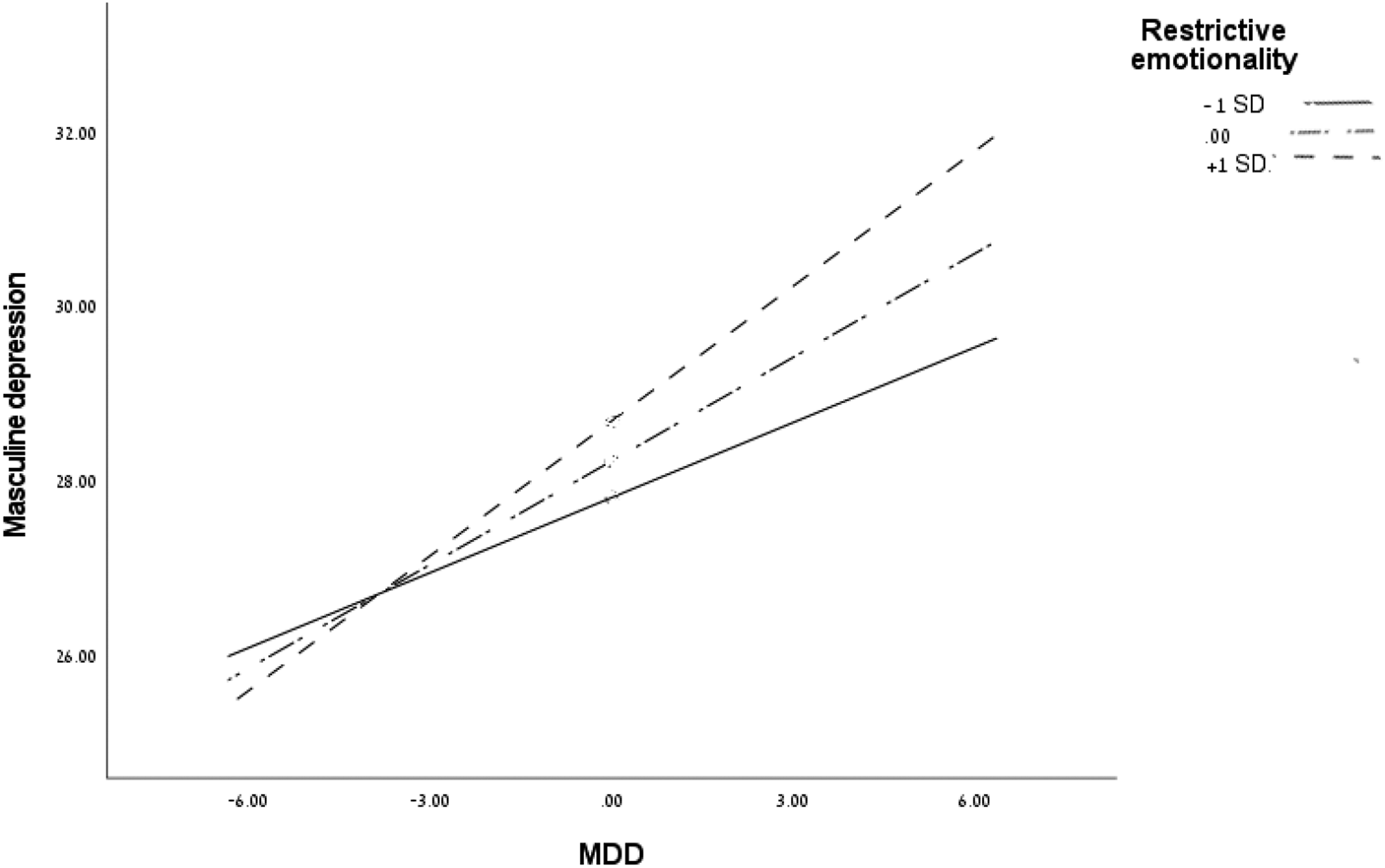
Discussion
Consistent with previous studies (Cafri et al., 2008; Cunningham et al., 2017; Mitchell et al., 2017; Phillips & Stout, 2006), which refer to the destructive consequences of body image disorders for men’s mental health, current findings demonstrate a positive association between MDD and masculine depression. An in-depth look at this association illustrates that internalizing traditional masculine norms and greater adherence to them, manifested in higher levels of restrictive emotionality, intensifies the harmful effect of MDD on masculine depression.
Men who comply to a large extent with traditional masculine norms that encourage them to demonstrate emotional control and emotional restrictiveness may find it difficult to express their emotions to others, form close and meaningful relationships, and seek and accept help. Therefore, their social support system may be lacking and they might have limited options at their disposal to relieve stress in a beneficial manner, accordingly aggravating symptoms of masculine depression (Magovcevic & Addis, 2008; Mahalik & Rochlen, 2006; Rice et al., 2016).
Identifying the schemas of masculine identity when addressing the mental health outcomes of masculine body image disturbance is of great clinical importance (Blashill et al., 2020). As such, therapists treating men with MDD should be aware of the issue of restrictive emotionality and its possible implications for their clients and for the intervention process. Traditional masculine norms, similar to many other social norms, are latently internalized social facts (Durkheim, 1982) that considerably affect the core aspects of masculine identity (Blashill et al., 2020). Awareness of the destructive effects of these norms may ameliorate men’s willingness to reconsider their perceptions of masculinity and to develop an alternative view of this construct. This may remove barriers to seeking and receiving help and support and to responding to treatment, and may accordingly reduce the negative mental health outcomes of masculine restrictive social norms, such as masculine depression (Emslie et al., 2006; Rice et al., 2016).
MDD has been described in previous studies as being significantly associated with avoidance of social interactions and social activities and with higher levels of mental distress among men (Cunningham et al., 2017; Olivardia et al., 2000; Pope et al., 2005). To the best of my knowledge, the current study is the first to provide evidence that MDD is associated with social interaction anxiety, recognized in the International Classification of Diseases (ICD-10) as a mental and behavioral disorder. This finding corresponds with studies that found an association between a preoccupation with one’s physical appearance and body dysmorphic disorder and social anxiety disorder (Bittner et al., 2004; Liao et al., 2010; Moscovitch et al., 2013), although MDD was not specifically addressed.
Social norms regarding the ideal masculine identity create a social expectation that men should be dominant and should conduct themselves confidently and assertively in social settings (Weinstock, 1999). However, men who experience social interaction anxiety might perceive themselves as failing to meet these social expectations and to conform to the ideal masculine identity. They may experience continual and extreme fear or anxiety of negative social events, such as receiving negative feedback, being victimized, or being rejected (Kim & Duval, 2022; Wong et al., 2006), and as result display distress or depression. The diagnosis of social interaction anxiety disorder in the context of MDD is of great importance in terms of clinical intervention with patients with MDD. Clinicians must gain a deep understanding of the factors associated with social interaction anxiety onset and progression in order to help their clients reduce the negative impact of these factors on their mental health outcomes.
The present study identified the important role of restrictive emotionality and social anxiety disorder in the association between MDD and masculine depression, highlighting the need for gender-adjusted treatment models focusing on these issues. Previous studies advise that cognitive behavioral therapy (Beck, 1979), family-based therapy (Murray & Griffiths, 2015), group therapy (Wilhelm et al., 1999), and mindfulness-based treatment approaches (Baer, 2015) can have positive outcomes in individuals with destructive thinking and behavioral patterns, helping them address and alleviate their symptoms. They may also be effective in treating men with MDD. Yet, to the best of my knowledge, comprehensive and in-depth research linking the clinical intervention method with the most efficient outcomes in men with MDD is still lacking and this should be subjected to further empirical investigation.
Limitations
The current study has several limitations. The data was collected online among a convenience sample of men in the Hebrew language only, meaning that this may not have included proper representation of male populations in Israel with limited access to online means (e.g., older people or the religious orthodox) or people whose level of literacy in Hebrew is low (e.g., immigrants). Furthermore, the study focused on a limited number of research variables. Since the psychosocial context of the relationship between MDD and masculine depression has only recently been recognized and is an understudied subject (Pope et al., 2005), it is important to expand the scope and focus on research of the moderating role of other traditional masculine norms such as toughness, dominance, avoidance of femininity, and self-reliance, as well as personality characteristics such as attachment style, self-efficacy, and locus of control, in the association between MDD and masculine depression. This has great significance in terms of intervention and treatment in men with MDD and masculine depression symptoms. Finally, data were collected within a single, unique national culture. At the same time, there is a great similarity between the Israeli culture and the culture of developed Western countries (Harel & Tzafrir, 1999). Therefore, Israel can provide researchers and practitioners with a legitimate field for studying and analyzing the psychosocial context of the relationship between various masculine body image disorders and mental health issues.
Conclusion
The current study constitutes an important theoretical contribution to the literature on the relationship between body image disorders and mental health among men, as it provides innovative empirical evidence for the psychosocial effects of traditional masculine norms and social interaction anxiety disorder on the relationship between MDD and masculine depression. These findings can be useful for therapists in the intervention process with men dealing with mental consequences of MDD.
Given the evidence of complex mental consequences of the pathological preoccupation with appearance and with the pursuit of a muscular body, manifested in MDD and of adherence to masculine social norms, manifested in emotional restriction, it is of great importance to raise social awareness of this issue. Bringing the issue to the social discourse may help men dealing with MDD recognize the problem and consider seeking help and support. It may also motivate a rethinking of traditional masculine norms among men with MDD and among a broader male population and thereby curb the progression of this phenomenon.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.