
Abstract
This analysis reported interest in exercise programs made for men survivors of sexual violence (SV), preferences for the structure and content of these programs, and comparisons by physical activity level and PTSD status. A cross-sectional survey was conducted among 198 men aged 18–65, with a history of SV, in the USA. Most respondents indicated interest in exercise programs for them. Men with PTSD were most interested. Men favored exercising at-home, alone, with a male instructor, 3–4 times per week, at moderate intensity, for 30 mins-1 h. No differences in preferences were found by activity status. Differences by PTSD status were found in location, social environment, instructor gender, intensity, duration, and program length. Top modes were walking, jogging, and biking. Results add new knowledge relevant for integrating exercise into trauma recovery programs.
Sexual Violence (SV) is a pervasive public health issue in the United States which has many wide-reaching negative impacts on its survivors (Breiding et al., 2014; 2015). Although the burden of SV (defined as a sexual act that is committed or attempted by another person without freely given consent of the victim or against someone who is unable to consent) is shouldered primarily by women, a significant number of men experience SV in their lifetime. Specifically, around 1.4% of men have experienced sexual assault in their lifetime, while 22.5% have experienced forms of SV other than assault, including being made to penetrate, sexual coercion, sexual contact, or non-contact sexual experiences (Barth et al., 2016; Black et al., 2010). Experiencing SV often contributes to the development of complex multimorbidity, with high rates of trauma-related mental health conditions like post-traumatic stress disorder (PTSD) and self-harm, coupled with cardiometabolic disorders and substance abuse (Choudhary et al., 2010; Haegerich & Hall, 2011; Murdoch et al., 2007). There is a large amount of social stigma and silence around men’s experiences with SV, which often results in a lack of awareness and understanding about the impact of SV on men, and how to best engage men in trauma recovery efforts. As a result, men rarely disclose SV and associated health concerns often go untreated (Sable et al., 2006).
Men survivors of SV face many gender-specific barriers to accessing care. These include stigma surrounding SV which often results in low levels of disclosure among men, as well as societal norms which emphasize self-reliance and dictate that help seeking signals weakness (Sable et al., 2006). As such, enrollment and engagement in gold standard treatments for SV-related mental health conditions are low (Tjaden & Thoennes, 2006). Among men who do enroll in these treatments, dropout rates are high and residual symptoms often remain following completion (Hoge et al., 2014; Sagar-Ouriaghli et al., 2019). Additionally, a limitation of these treatments is that they do not aim to treat physical health concerns. Recent and increasing work has begun to explore the use of physical activity (PA) as an adjuvant treatment for SV-related health conditions (Pebole et a., 2021). Several studies have identified that integrating physical activity into treatments for SV-related concerns (e.g., adding exercise sessions into cognitive behavioral therapy, adding yoga into group therapy sessions) may improve mental health (Clark et al., 2014; Smith et al., 2014). Additionally, preliminary evidence indicates that PA may improve physical and mental health independently of being enrolled in SV-related treatments (e.g., aerobic exercise without talk therapy; Nicotera & Connolly, 2020; Shors et al., 2018). More broadly, research among populations with PTSD has indicated that PA can independently improve physical and mental health, while also improving complementary factors not targeted by gold-standard mental health treatments (Björkman & Ekblom, 2021).
An essential part of implementing physical activity interventions among SV-exposed populations is integrating trauma-informed approaches (Darroch et al., 2020; Pebole et al., 2020). Trauma-informed practice integrates knowledge of trauma into all aspects of provided services, aims to avoid any possibility of re-traumatization, and reduces potential barriers to care (Substance Abuse and Mental Health Services Administration [SAMHSA], 2014). Broadly, trauma-informed practices follow several key pillars: safety, trustworthiness and transparency, peer support, collaboration and mutuality, empowerment, voice, and choice and cultural, historical, and gender issues (SAMHSA, 2014). Centering the voices and experiences of survivors of SV in healthcare services is an essential part of trauma-informed practice which aligns with these overarching principles. Examples of trauma-informed approaches which have been increasingly integrated into healthcare services include consensual touch and giving options about whether doors should be open or closed. Although significant strides have been made to improve in integrating these approaches into medical contexts, very little work has identified important trauma-informed considerations for exercise environments (Darroch et al., 2020; Pebole et al., 2020; Wheatley et al., 2022). This is concerning, given the increased recognition of widespread sexual abuse happening at all levels of sport and exercise involvement (Milroy et al., 2022).
Previous work aiming to identify best practices in exercise contexts for survivors of SV has emphasized that main considerations include enhancing safety in exercise environments, using consensual touch, limiting attention to physical appearance, and employing women exercise instructors (Pebole et al., 2021, 2022; Smith-Marek et al., 2018). However, this limited body of research draws from data collected exclusively from women survivors of SV, leaving no information as to how societal and gender-specific considerations may impact these considerations for men. As such, the voices of men survivors of SV have been excluded from this research base, leaving no formal guidance for how to actively include or target men survivors of SV in exercise. Understanding preferences for structure and content of exercise programs, and willingness to engage in these programs, is an essential first step to creating trauma-informed exercise interventions for this population. This information is especially relevant for exercise professionals wanting to create programs in partnership with organizations that provide services to men survivors of SV (e.g., mental health clinics, military sexual trauma clinics). Preferences for the structure and content of programs are especially relevant for subgroup of survivors who are less likely to engage in exercise, such as those with high trauma-related mental health symptoms and those not meeting public health PA guidelines.
To address these gaps in knowledge and practice, this study reported on willingness of men survivors of SV to engage in exercise interventions made for them, and preferences for their structure and content. It also compared preferences by current physical activity level and PTSD status. Data collection took place during August 2021 and as such reflects preferences which may have been impacted by the ongoing COVID-19 pandemic. Specific aims included reporting: 1) interest in exercise programs made for men survivors of SV; 2) preferences for the structure and content of exercise interventions among a sample of men survivors of SV; and 3) comparing exercise interest and preferences by activity and PTSD status.
Methods
Study procedures were approved by the IRB at The University of Illinois at Urbana Champaign (Protocol #21820). This study represents an analysis from a larger dataset aiming to assess exercise behaviors, perceptions, and preferences among survivors of SV. Due to ongoing concern for the risk of spreading COVID-19 associated with in-person data collection during study conceptualization and the data collection time-period, along with limited financial resources and time restrictions, this cross-sectional study was completed with Amazon Mechanical Turk (MTurk). MTurk is an online platform hosted by Amazon through which its users can opt to complete surveys or tasks for small incentives. Procedurally, MTurk allowed researchers to post tasks (e.g., online surveys) which become available to qualified participants (Engle et al., 2020). The parent study collected data on exercise behaviors, perceptions, and preferences, among men and women survivors of SV. Data collection was completed separately for males and females. Inclusion criteria for this male-specific sample were male sex, age between 18-65 years, self-reported history of SV, and living in the United States (U.S.).
The questionnaire was available during August 2021, based on recruitment for the parent study. Location within the U.S. and male sex were characteristics set by MTurk as prerequisites to accessing the survey. Eligibility requirements were masked from the participants at pre-screen to help avoid respondents misrepresenting themselves. Survey respondents were instructed to indicate their age, specify which gender they identified with (with the options man, woman, non-binary, or other available), and identify which stressful life experiences they have experienced from a list of possible events including recent unemployment, death of a loved one, moving into a new home, separation or divorce from a life partner, major chronic illness or injury, and/or SV. A respondent was considered a survivor of SV if he endorsed experiencing an “unwanted or uncomfortable sexual experience (including, but not limited to sexual harassment, unwanted sexual touch or experience, sexual assault, partner violence).” All men who met inclusion criteria were directed to the online consent form. Men were told that $3.00 would be credited to their MTurk account upon successful completion of the survey. All participants provided informed consent and were then directed to the online survey (hosted by Qualtrics). The research team used several methods to ensure data quality, including embedding a CAPTCHA question at survey start, checking IP address eligibility, using ballot-stuffing, screening open-ended responses and reverse-scored items, attention and logic checks, and monitoring speed of survey completion (Godinho et al., 2020; Stokozuk et al., 2020).
Instruments
Demographic Information
Single-item questions asked about age, race, ethnicity, education level, income level, marital status, number of children under the age of 18 living in the home, sexual orientation, location, and military affiliation.
Type of SV
A single question was used to assess which type of SV the respondent had experienced throughout their lifetime. Men could check multiple boxes, indicating they experienced more than one form of SV. Sexual violence classifications were consistent with categorizations per the Centers for Disease Control and Preventions (CDC) (Breiding et al., 2014; 2015). Responses included the following: sexual harassment (e.g., unwanted verbal comments, looks, or actions); sexual assault or rape (e.g., unwanted assault, forced penetration); unwanted sexual contact (e.g., intentional touching of private area under or through clothes); and non-contact unwanted sexual experiences (e.g., threats of violence, being forced to look at unwanted images, hostile environments).
Physical and Mental Health
The Patient-Reported Outcome Measurement System (PROMIS) Scale v1.2 for Global Health was used to gather information regarding physical and mental health (Cella et al., 2007; 2010). This measure uses 10 questions about physical and mental health, quality of life, physical function, fatigue, pain, emotional distress, and social health. Each item uses a Likert 1-5 scale, except for the pain item. This item is recoded into a 5 scale category based on NIH scoring criteria (Hays et al., 2009; 2015; 2017). The PROMIS Scale v1.2 Global Health measure produces two scores: Physical Health and Mental Health. Both physical and mental health scores were translated into a T-score per the scoring manual (Cella et al., 2007; Hays et al., 2009; 2017). T-scores were used to compare the score to the average for the general population in the U.S. (Hays et al., 2009; 2017).
Activity Status
Aerobic exercise levels were assessed with language consistent with questionnaires previously used by the CDC to assess activity among the general population (Centers for Disease Control and Prevention, 2020). Aerobic exercise was assessed with a question asking the respondent to recall how many weekly minutes they spend participating in moderate/vigorous intensity aerobic exercise. An explanation of the talk test was included to help respondents identify exercise intensity. For example, “How many minutes a week do you participate in moderate intensity aerobic exercise? In general, if you are doing moderate-intensity activity, you can talk but not sing during the activity. Examples include walking bristly, water aerobics, gardening, and tennis (doubles).” For vigorous exercise, the question read: “How many minutes a week do you participate in vigorous intensity aerobic exercise? In general, if you are doing vigorous intensity exercise, you cannot say more than a few words without pausing for a breath. Examples include jogging, tennis (singles), aerobic dancing, jumping rope, hiking uphill with a heavy backpack.” To assess strength training, participants were asked how many days a week they engaged in activities that strengthen the muscles, like weightlifting. Responses were used to categorize respondents into “active” and “not active” groups. Active participants met PA guidelines; not active participants did not. PA guidelines are defined as 150+ mins of moderate-intensity exercise, 75 mins of vigorous intensity exercise, or an equivalent combination, and at least 2 days a week of muscle strengthening activities (CDC, 2020).
PTSD Symptomology
Severity of PTSD symptoms was assessed using the PTSD Checklist for DSM-5 (PCL-5). The PCL-5 is a 20-item self-report instrument that uses a 5 point Likert-type scale ranging from 0 = “not at all” to 4 = “extremely.” Each item is used to assess the extent to which an individual is impacted by trauma-related mental health symptoms (range: 0–80). PTSD status was determined by using cutoffs based off the total PCL-5 score. A PCL-5 score of ≥31 was considered provisional PTSD, consistent with recommendations (Blevins et al., 2015; Bovin et al., 2016).
Willingness to Participate in an Exercise Program Targeting Men Survivors
Preference items were adapted from previous research (Abrantes et al., 2011; Busch et al., 2016). Participants were asked if they were interested in “an exercise program designed to improve the wellbeing of men who have experienced an unwanted sexual event.” Possible answers included “yes”, “maybe”, or “no.”
Preferences for Content and Structure of an Exercise Program for Survivors of SV
Participants were asked questions on preferred location (home using real-time video stream with an instructor, home using telephone coaching, home using an app or website, community gym, outdoors, local mental health facility, no preference), social environment (group format, alone, online in a group, online alone), supervision (with male instructors, with female instructors, no instructors, no preference), frequency (once a day, 3–4 days per week, 2–3 days per week, once per week), intensity (high intensity, moderate intensity, low intensity, no preference), duration of session (30 mins or less, 30 mins-1 hour, over 1 h, no preference) and duration of program (1–4 weeks, 4–8 weeks, longer than 8 weeks, ongoing). Exercise mode preferences were also assessed (men could indicate up to 3 preferred exercise types). Activity types were adapted from the Modifiable Activity Questionnaire (Kriska, 1997) with an open option to indicate any activity not listed.
Data Analysis
Analyses were performed using SAS (Version 9.3: SAS Institute, Cary, NC). Answers to the willingness to engage in an exercise program made for men survivors of SV were reported. Responses (frequency, percent) to questions about the preferences for the structure and content of exercise interventions were reported among men who indicated “yes” or “maybe” to the question assessing interest in an exercise program among men survivors of SV (n = 172). Differences in the interest in and content of the exercise programs by PTSD status and physical activity level were assessed using Chi-square comparisons and Fisher’s Exact tests. Missing PA data set the number of participants for comparison to 160 for PA levels. Preferred exercise modes are reported.
Results
Participants
Sociodemographic Characteristics of the Whole Sample and Men Interested in Exercise Programs by activity and PTSD status
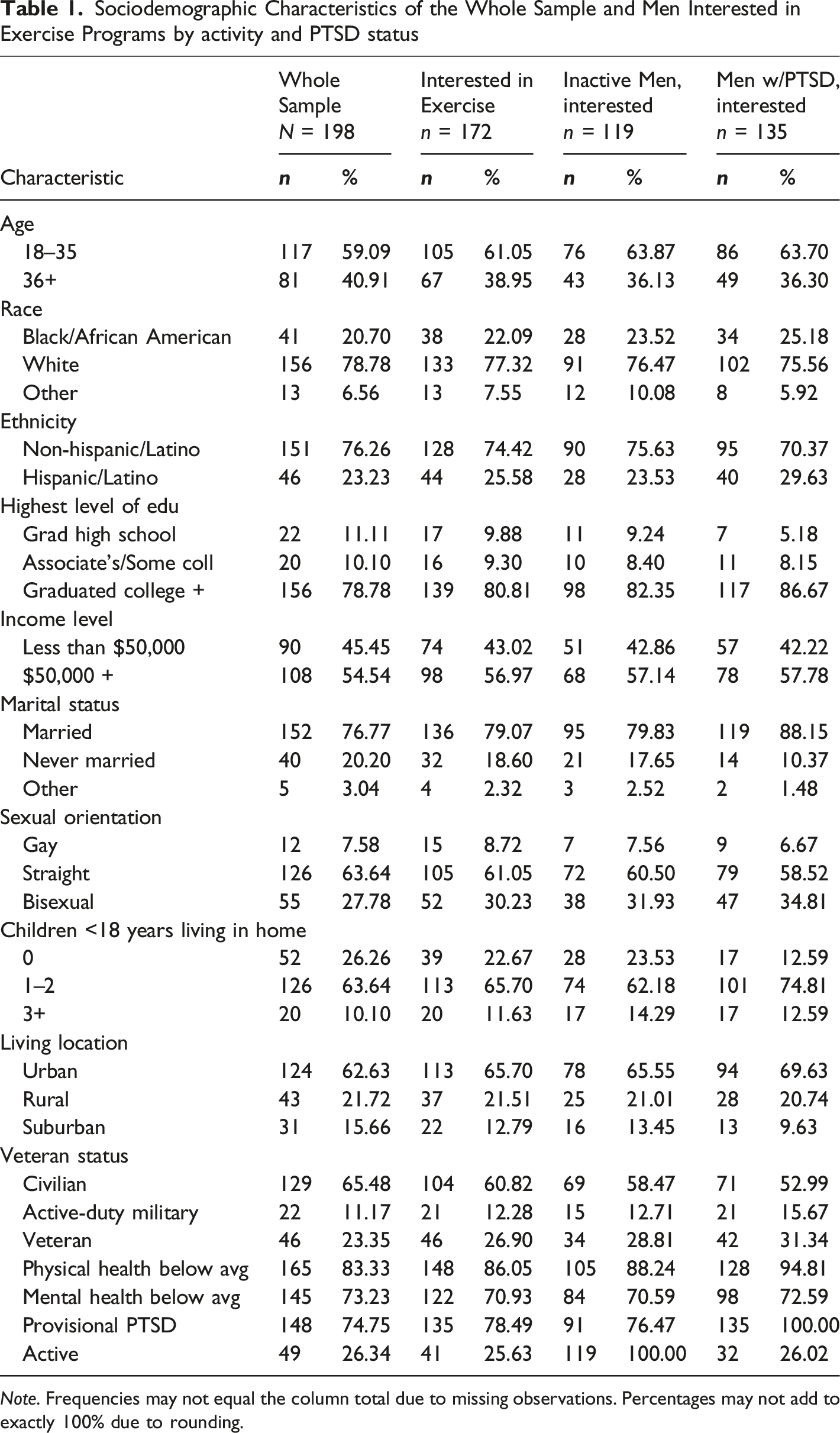
Note. Frequencies may not equal the column total due to missing observations. Percentages may not add to exactly 100% due to rounding.
Willingness to Engage in Exercise Program, Overall and by PTSD and Activity Status
When asked about desire to participate in “an exercise program designed to improve wellbeing among men who have experienced an unwanted sexual event,” 86.87% (n = 172) indicated potential interest in an exercise program made for men survivors of SV. Specifically, 47.9% of participants answered “yes” (n = 95), 38.8% responded “maybe” (n = 77), and 13.1% (n = 26) responded “no.” Significant differences were found by PTSD status. Men with provisional PTSD were more likely to report being willing to engage in these programs (n = 81, 54.7% yes; n = 54, 36.4% maybe; n = 13, 8.7% no) when compared to those without provisional PTSD (n = 14, 28.0% yes; n = 23, 46.0% maybe; n = 13, 26.0% no; p < 0.001; Cramer’s V = 0.27). There were no significant differences in willingness to engage in these programs between men who were active (n = 28, 57.1% yes; n = 13, 26.5% maybe; n = 8, 16.3% no) versus inactive (n = 58, 42.3% yes; n = 61, 44.5% maybe; n = 18, 13.24% no; p = 0.08; Cramer’s V = 0.16).
Preferences for Structure and Content of Exercise Program
Preferences for Structure and Content of Exercise for Men Survivors of SV Interested in Exercise Programs.
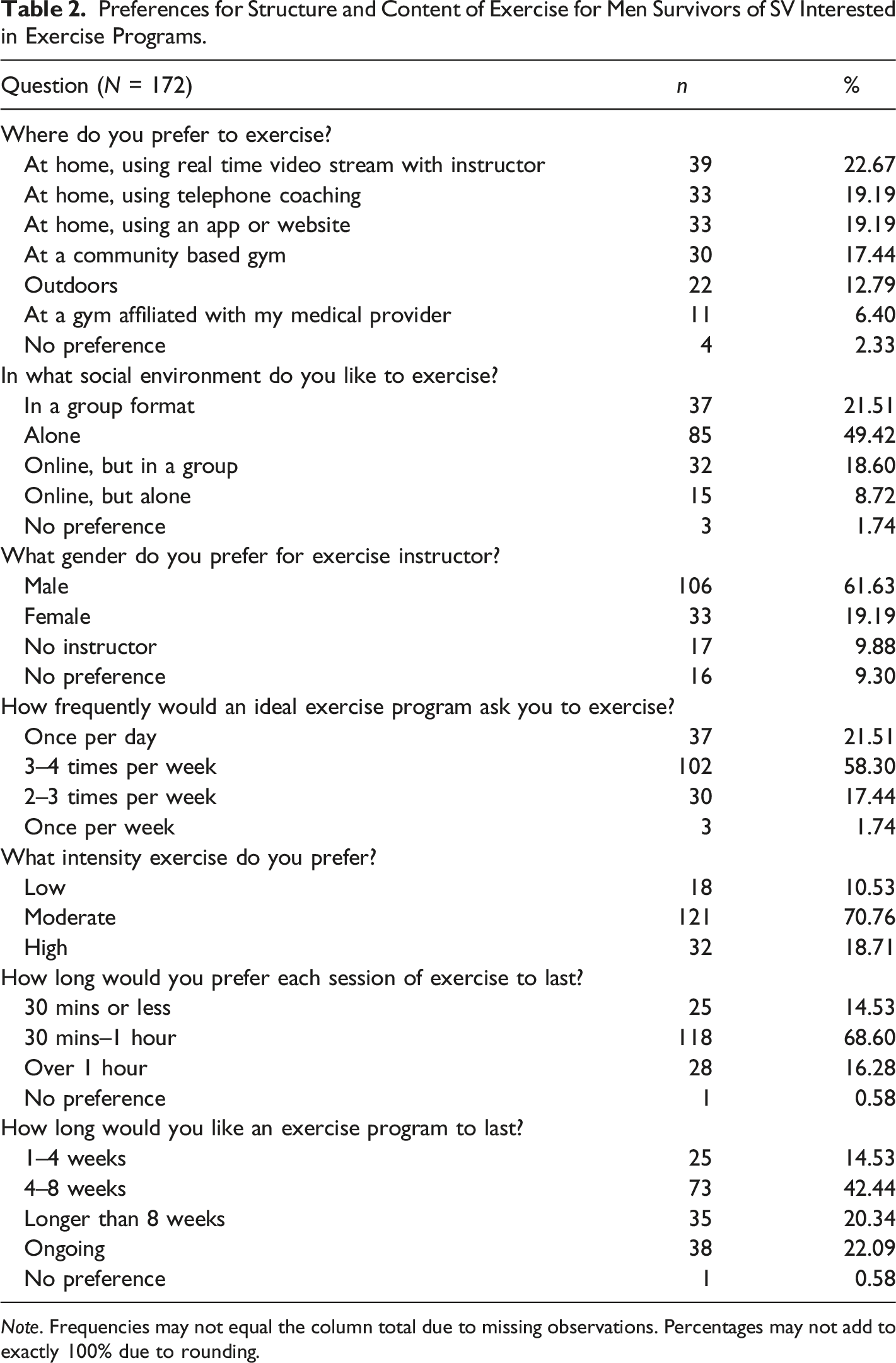
Note. Frequencies may not equal the column total due to missing observations. Percentages may not add to exactly 100% due to rounding.
Differences in Structure and Content Preferences by Activity Status
Preferences for Structure and Content of Exercise for Men Survivors of SV by Activity and PTSD Status.
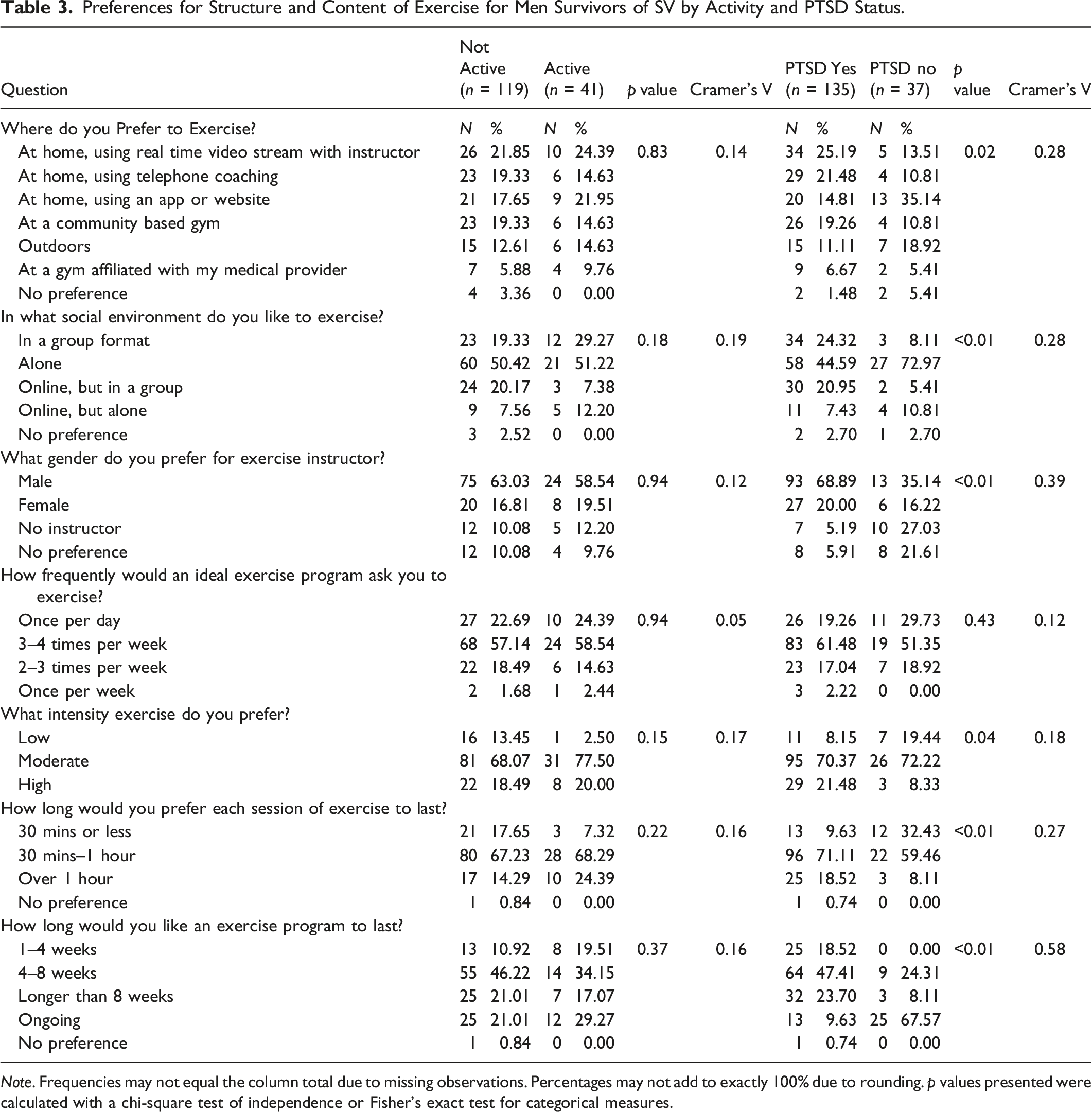
Note. Frequencies may not equal the column total due to missing observations. Percentages may not add to exactly 100% due to rounding. p values presented were calculated with a chi-square test of independence or Fisher’s exact test for categorical measures.
Differences in Structure and Content Preferences by PTSD Status
Significant differences were found by PTSD status in preferences for exercise location (p = 0.02; Cramer’s V = 0.28), social environment (p < 0.01; Cramer’s V = 0.28), instructor gender (p < 0.01; Cramer’s V = 0.39), exercise intensity (p = 0.04; Cramer’s V = 0.18), exercise duration (p < 0.01; Cramer’s V = 0.27), and program length (p < 0.01; Cramer’s V = 0.58). Specifically, respondents with provisional PTSD symptoms were more likely to prefer at home options with real time video stream and instructor or telephone coaching, or at a community-based gym (n = 34, 25.19%; n = 29, 21.48%; and n = 26, 19.26%, respectively), when compared to those without provisional PTSD (n = 5, 13.51%, n = 4, 10.81%, and n = 4, 10.81%). Those meeting PTSD cutoffs were also more likely to prefer exercising in a group format, or online but in a group (n = 34, 24.32%; n = 30, 20.95%, respectively), when compared to men without PTSD (n = 3, 8.11%; n = 2, 5.41%). Regarding exercise instructors, men with PTSD were significantly more likely to report preferring a male exercise instructor (n = 93, 68.89%) compared to men without PTSD (n = 13, 35.14%). Regarding exercise intensity, participants meeting PTSD cutoffs were more likely to endorse high intensity exercise (n = 29, 21.48%), when compared to men not meeting these cutoffs (n = 3, 8.33%). Additionally, men with PTSD were more likely to endorse longer exercise sessions (n = 25, 18.52%, over 1 h; n = 96, 71.11%, 30 mins to hour) compared to those without PTSD (n = 3, 8.11%; n = 22, 59.46%). Lastly, men with PTSD preferred shorter exercise program duration (n = 64, 47.41% 4–8 weeks; n = 25, 18.52% 1–4 weeks; n = 13, 9.62% ongoing), compared to those without PTSD (n = 9, 24.31%; n = 0, 0.00%; n = 25, 67.57% ongoing).
Exercise Modes
Of the men reporting interest in exercise programs made for men survivors of SV, the three most frequently endorsed exercise modes were walking (n = 126), jogging (n = 116), and biking (n = 63). The three least frequently endorsed exercise modes were dance/Zumba (n = 18), self-defense/boxing (n = 12), and organized sports (n = 6). Open ended responses also included: kick scooter riding, rock climbing, gardening, Pilates, rowing, virtual reality workouts, and push-ups/pull ups.
Discussion
This study provides essential new information and initial guidance relevant for engaging men survivors of SV in exercise programs. There is ample opportunity for exercise professionals to partner with organizations that serve men survivors of SV to provide exercise-based programs aimed at improving physical and mental health among men survivors of SV. This study provides targeted information on men survivors of SV experiencing PTSD symptoms and who are physically inactive, two sub-groups that would benefit greatly from physical activity and targeted health promotion efforts.
Interest in Exercise Program for Men Survivors
Most men indicated that they were interested, or might be interested, in gender-specific exercise programs for men who had experienced an unwanted sexual event. Men survivors with provisional PTSD were more likely to be interested in these programs than those without provisional PTSD. No differences were found by physical activity status. This finding is significant, considering the high levels of shame following victimization and low levels of disclosure of SV among men (Sable et al., 2006). Interest in exercise programs indicates that men would consider joining a group with other men with shared experiences of SV. Men survivors may be more open to engaging in exercise than other trauma-focused therapies, given that exercise aligns with several societal-defined constructs of masculinity like physical strength, leadership, and autonomy (Connell & Messerschmidt, 2005; Hurd et al., 2018). PA contexts therefore seem to have the potential to provide a low-stigma social environment where men with shared stigmatized experiences could seek out informal social support without being forced to discuss past traumas. This may be especially relevant for men survivors with PTSD, who often experience increased levels of social isolation, but who also who indicated high interest in these programs. Previous exercise programs among male-dominated samples with PTSD have demonstrated high levels of social support, even in individualized exercise programs (Browne et al., 2021; Wilkins et al., 2020), further emphasizing the potential social benefits of exercise in this group. Another significant consideration in this group is the high number of men who responded “maybe” to being interested. These responses likely indicate that men might be interested in these programs, but more information about the structure and content should be communicated. Providing information at the start of programs per these findings aligns with the trauma-informed principle of transparency and would help build trust between organizations and participants (SAMHSA, 2014).
Preferences for the Structure and Content of Exercise Interventions
Results indicated that men preferred programs with at-home options, exercising alone, with male instructors, 3–4 times a week, at moderate intensities, between 30 mins-1 h, and programs lasting 4–8 weeks. These results provide practical guidance for implementing exercise programs. For example, this sample highly endorsed home-based options, indicating that exercise professionals working with this population likely need to include flexible/hybrid programs with both in-person and remote options. This is especially relevant in the aftermath of the COVID-19 pandemic, which may be impacting preferences for exercise in private facilities/at home (Dwyer et al., 2020). Moreover, increased shame and stigma surrounding SV experiences may make in person exercise meetings (which could identify them as a survivor of SV) challenging at the start of these programs. Future research should examine the reasons underlying men SV survivors’ preferences for home-based exercise.
Previous work demonstrates the social benefits of exercise among trauma-exposed men, and peer support can be integrated even into individualized exercise programs (e.g., working out independently but in the same gym space). Peer support is a significant trauma-informed principle that deserves further research attention among men SV survivors in exercise contexts as it can help establish safety and hope, build trust, and promote recovery and healing (SAMHSA, 2014). As such, future research should explore men survivors’ willingness to engage in men-survivor focused social environments in exercise contexts and identify best practices for creating such programs. One option supported by these data is the creation of hybrid programs that allow men to engage at a time and speed of their choosing, further emphasizing participant autonomy, and aligning with the trauma-informed principles of collaboration and mutuality and empowerment, voice, and choice (SAMHSA, 2014).
Men in this study preferred male exercise instructors. Previous research with women survivors of SV also shows a preference for same-gendered exercise instructors (Pebole et al., 2021). Most research hypothesizes women’s preference for same-gendered exercise instructors is due, in part, to men being the main perpetrators of SV against women (Black et al., 2010), and as such women instructors enhance feelings of safety by removing threatening presences. However, men are also most often perpetrators of SV-related crimes against men, yet this did not drive preferences towards women exercise instructors. Interestingly, men survivors of SV often prefer woman-identifying mental health providers (Turchik et al., 2013). It therefore seems that exercise instructor preference may be most strongly impacted by social context among men survivors of SV. For instance, although women providers may be seen as more understanding in mental healthcare contexts, this is unlikely to be seen as relevant for men during exercise. Instead, men survivors may seek out male instructors to subconsciously align themselves with masculine societal constructs which focus on strength, power, and dominance (Mahalik et al., 2003). Masculine norms within patriarchal power structures often emphasize physical power over women specifically, which may be underlying this desire to train with other men and further driving this preference (Mahalik et al., 2003). This emphasizes the importance of clinical alliances between exercise and mental health professionals in these contexts, which can help men survivors of SV unpack harmful societal constructs of masculinity, like power over women. Other endorsed exercise preferences indicate that men survivors likely value consistency, moderate intensity, and time efficiency. Importantly, individualization and flexibility in all aspects of exercise programs can enhance feelings of safety and autonomy among exercise participants (also key trauma-informed principles; SAMHSA, 2014), and should be emphasized.
Differences in Preferences by Physical Activity Status
There were no significant differences in exercise preferences by physical activity status within this sample. This finding was surprising, given that active participants are generally open to more exercise sessions and increased exercise intensities. Although differences were not found here, individualization using baseline fitness levels has been essential among populations with PTSD and is widely recommended among diverse trauma-exposed populations and across mental health diagnoses (Lederman et al., 2017; Pebole et al., 2019; 2021; Teychenne et al., 2020; Vancampfort et al., 2016). As such, individualization should be continued in exercise programs structured for this population.
Differences in Preferences by PTSD Status
Men with provisional PTSD symptoms were more likely to prefer home-based exercise with coaching, group formats (online or in person), male exercise instructors, high intensity exercise, longer session durations (30 mins–1 h, over 1 h), and longer exercise program lengths than those without provisional PTSD. These findings provide considerations for designing and implementing exercise programs which aim to incorporate men with high trauma-related symptoms, a population which has traditionally been hard to target and engage. Several considerations may have increased preferences for at-home options among this sample with provisional PTSD. These include high rates of social avoidance in general, along with exaggerated social avoidance associated with COVID-19 hypervigilance. Moreover, men with provisional PTSD may also face increased levels of SV-related shame/stigma, further driving their desire to exercise at-home. Again, this finding emphasizes the need for hybrid options which allow men to choose when and how best to engage in these programs. Men with provisional PTSD strongly preferred men instructors, further supporting that trauma-informed practice among this group necessitates available male exercise instructors. Reasons behind preferences for higher-intensity and longer bouts of exercise and program duration among individuals with provisional PTSD are more unclear, although previous work has linked higher intensity exercise with lower PTSD symptoms (Whitworth et al., 2017). Individuals experiencing PTSD may therefore recognize higher intensity exercise as a temporary escape, inspiring increased willingness to participate for longer periods of time. Altogether, these differences in preferences by provisional PTSD status emphasize the importance of centering the voice of the individual in developing exercise programs for those impacted by trauma-related mental health symptoms. Building programs alongside survivors of SV with PTSD highlights mutuality, collaboration, and empowerment, therefore aligning with trauma-informed principles and practice (SAMHSA, 2014).
Exercise Mode Preferences
Altogether, there was high variability in preferred exercise modes, indicating that individualized exercise programs where men can choose their exercise plans would be beneficial for this group. Previous interventions have used individualized and multi-modal exercise programs in other populations exhibiting trauma-related symptoms (Hall et al., 2020), and are also likely feasible and important for this population.
Recommendations for Trauma-Informed Practice among Men
Given the relevance of these findings to the trauma-informed framework, and the current dearth of information available focused on men survivors of SV, we emphasize several recommendations. First, given these data which suggest men survivors are willing to engage in these programs and may reap myriad benefits, we support increased integration of PA into trauma recovery programs and specifically emphasize the importance of future work identifying ways to make these programs accessible to men. Other trauma-informed considerations for this group based on these data include providing as much information as possible before exercise interventions begin, and implementing exercise programs which meet consistently, have an option of using male instructors, use moderate-vigorous intensity exercise, and time efficiency. Flexibility in these programs based of individual preferences should be emphasized to enhance feelings of safety and autonomy. Clinical alliances between exercise and mental health professionals would be extremely advantageous in recovery programs for men survivors of SV. Morevoer, while understanding exercise preferences among men survivors of SV is significant, it represents only part of essential trauma-informed considerations when working with this group. Future work should identify additional exercise-specific trauma-informed considerations and gauge interest and preferences from local communities of survivors.
Limitations
First, data were collected using a non-random convenience sample where participants self-selected to participate, limiting the generalizability of the findings. While online data collection via MTurk has several strengths (e.g., helping maintain privacy of the respondents, individuals being more open to disclosing violence online, workers being less susceptible to socially desirable reporting, cost- and time-efficiency; Engle et al., 2020), MTurk utilizes a non-random sampling scheme in which individuals self-selected to participate, limiting the generalizability of this study. Trauma exposed MTurk users have previously been shown to report lower mean scores of PTSD, depression, and anxiety symptoms when compared to other populations with PTSD, which may have impacted these results and further limited the generalizability (Engle et al., 2020). Additionally, men with marginalized identities (e.g., racial/ethnic, gender, minorities, LGBTQIA+, low socioeconomic status, incarcerated persons) were underrepresented in this sample, despite each of these marginalized groups being disproportionately impacted by SV. Thus, more work should be done to identify exercise preferences among these men who experience myriad additional barriers to engaging in PA (e.g., less financial resources for accessing gyms or activity-related technology, lack of feeling safe in gym spaces for gender minorities). Additionally, research which focuses on men survivors of SV in the military would be beneficial, given their high risk for experiencing SV and lower levels of PA upon exiting military service (Littman et al., 2009; Wilson, 2016). The study design was cross-sectional and self-report. Therefore, causal inferences cannot be made, and personal differences may have impacted self-report accuracy.
Conclusions
This study provides new information which can aide exercise professionals in designing and implementing exercise programs which aim to target or include men survivors of SV. Findings emphasize that men survivors of SV are generally interested in exercise programs which are structured specifically for them and highlights considerations for exercise interventions within this group. Results emphasize the importance of creating exercise interventions that are individualized to the participant and may need to include remote and at-home options. More research should be done to expand our understanding of exercise among men survivors of SV and identify additional and salient trauma-informed considerations for this group.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Ferber Survey Dissertation Award at the Graduate College of the University of Illinois at Urbana Champaign (PI: Pebole, M).
Ethical Approval
Informed Consent
Informed consent was obtained from all individual participants included in the study.