
Abstract
Men are reluctant to seek psychological help as doing so may label them as weak and vulnerable. Thus, we tested whether a first-person storytelling video could buffer men’s self-stigma of seeking help associated with traditional masculinity ideology. Adult men (N = 396; Mage = 35.62) were randomly assigned and exposed to one of three conditions: (1) control (nothing), (2) male-sensitive brochure, (3) male-sensitive first-person storytelling video. Controlling for pre-existing depressive symptoms, multi-group path analyses with bootstrapping revealed that greater traditional masculinity ideology was associated with lower psychological help-seeking attitudes via increased self-stigma of seeking help, but this indirect effect was not significant for the video group. The direct effect was significantly lower in the video group compared to the brochure and control groups. The findings suggest that brief male-sensitive storytelling videos may be useful clinical and psychoeducational tools to help men re-examine their resistance toward seeking psychological help for depression.
Although effective treatments for depression are available, studies indicate that men are significantly less likely than women to access such services and suffer from untreated depression (Coleman et al., 2020; Seidler et al., 2016). Untreated depression among men is particularly concerning given the risk of suicide. National statistics on suicide indicate that, compared to women, men are 4 times more likely to complete suicide (Centers for Disease Control and Prevention, 2019). In understanding men’s psychological help-seeking for depression, stigma has been an important variable (Vogel et al., 2006). The stigma associated with mental illness has been discussed as a leading cause of underutilization of treatment (Corrigan, 2004). In 2019, about 20% of the U.S. population experienced mental health issues but less than half of these individuals sought care, and men were represented in this group more than women (Substance Abuse and Mental Health Services Administration, 2020).
Literature suggests that men do not seek help due to the belief that doing so would label them as “weak,” “vulnerable,” and “unmanly” (Addis & Mahalik, 2003; Levant, Stefanov et al., 2013). These self-stigmatizing beliefs are rooted in men’s socialization around traditional masculinity ideology (TMI), or the need to internalize and endorse physical toughness, self-reliance, and restrictive emotionality as core concepts of how a man should appear and think to conform to societal expectations (Levant, Hall et al., 2013). As such, greater internalization of TMI has been found to evoke greater self-stigma of seeking help among men, which in turn reduces their propensity for seeking help for mental health issues (Levant, Stefanov et al., 2013; Vogel et al., 2011). Thus, the current study tested whether an empirically-informed first-person storytelling video exposure could help men work through their help-seeking resistance associated with TMI and self-stigma of seeking help, and improve their psychological help-seeking attitudes.
Research has shown that men who internalize TMI view psychological help as a threat to masculine norms (Vandello & Bosson, 2013) and develop negative attitudes toward seeking psychological help (Addis & Mahalik, 2003). In understanding the link between TMI and psychological help-seeking, studies have examined the mediating role of self-stigma of seeking-help (Covello, 2020). Self-stigma of seeking help is defined as the labeling and devaluing of one’s sense of self due to needing psychological help (Vogel et al., 2006). Self-stigma of seeking help is posited to stem from the public stigma associated with seeking mental health services, referred to as “the stigmatizing perception, endorsed by the general population, that a person who seeks mental health services is undesirable or socially unacceptable” (Vogel et al., 2006). For instance, Vally et al. (2018) found that public stigma on seeking help indirectly predicted attitudes toward seeking psychological help through self-stigma of seeking help.
For men who internalize TMI, self-stigma of seeking help may be salient as the thought that men will not be able to solve their depression or other mental health issues on their own is discrepant against the norms of TMI. Indeed, greater internalization of TMI was found to be indirectly related to lower help-seeking attitudes through self-stigma of seeking help among young adult men in the U.S. (Levant, Stefanov et al., 2013). Similarly, Wasylkiw and Clairo (2018) found that conformity to masculine norms was related to greater self-stigma of seeking help, which in turn was related to lower help-seeking attitudes. Given this mediating link, self-stigma of seeking help has received empirical attention as a malleable factor for interventions to target in helping men improve their help-seeking attitudes (Mittal et al., 2012).
Studies are limited on effective strategies to reduce the self-stigma of seeking help and approaches, a common element is psychoeducation, which involves delivering health information through didactic materials (e.g., brochures) and workshops. The effectiveness of psychoeducation strategies, however, has been mixed (Mittal et al., 2012), with some studies finding significant results (e.g., Hammer & Vogel, 2010) while other studies finding no effects (e.g., Alvidrez et al., 2009).
The mixed findings may be due to materials being impersonal to the audience (Janoušková et al., 2017). For example, print materials (e.g., brochures) on health information are often too general and created without regard for specific relevance to the readers’ background (Janoušková et al., 2017). In support of this limitation, Hammer and Vogel (2010) found that a male-sensitive brochure improved men’s attitudes and reduced their self-stigma of seeking counseling to a greater extent than an information-oriented brochure developed by the National Institute of Mental Health and a gender-neutral brochure developed by Rochlen et al. (2006). Compared to the other two brochures, the male-sensitive brochure incorporated language more compatible with masculine beliefs, such as replacing words like “therapist” with “consultant,” describing the client’s ownership and control in the counseling process, normalizing depressive symptoms within the context of masculinity, and explaining the value of associated costs and time for devoting attention to their mental health.
However, the impact of educational brochures may still be limited in their influence in comparison to other contemporary approaches such as the use of multimedia materials (Lusardi et al., 2017). Indeed, short-term interventions using didactic and print materials have been shown to have less effect in reducing mental health-related stigma than contact or video-based interventions (Janoušková et al., 2017). Video-based anti-stigma interventions have been on the rise to align with people’s increasing reliance on social media and digital media communication (Demyan & Anderson, 2012; Janoušková et al., 2017). Videos may be a promising strategy for facilitating a personally- and digitally-relevant medium for individuals to experience a more immersive influence on their beliefs and attitudes toward mental health (Janoušková et al., 2017). For example, Hackler et al. (2016) found that participants who viewed people discussing personal experiences with mental illness and experiences of having family or friends with mental illness resulted in significantly lower mental illness stigma than those who viewed a control video irrelevant to mental health issues. It appears that the videos provided positive experiences with people who have a mental illness, which likely fostered a more favorable view toward mental illness that detach from the pervasive stigmatizing norms in the public (Keum, Hill et al., 2018).
Yet, most of the studies on video-based interventions have focused on general stigma related to mental illness (e.g., negatively stereotyping people with mental illness as crazy or dangerous) rather than stigma toward psychological help-seeking (Janoušková et al., 2017; Morgan et al., 2018). Only one study (Demyan & Anderson, 2012) examined stigma toward psychological services, in which mass-media video intervention was helpful in improving positive attitudes toward psychological help-seeking but not effective in reducing stigma. It is possible that the generalized approach of using a commercial-type mass-media video intervention toward a broader college-aged population lacked personal relevance and specificity in conjunction with the viewers’ experiences with mental health issues and attitudes on mental health services. As noted in Hammer and Vogel’s (2010) study, although video materials may provide a more immersive and interactive medium, the efficaciousness of video-based interventions also likely requires the use of content that is tailored and sensitive to the context and unique experiences of the population and mental health issues being examined.
Building upon this lead and current evidence on video-based interventions, we sought to test a male-sensitive video intervention specifically for depression among men for potential improvements in help-seeking attitudes. One aspect that we incorporated to maximize the potential effects of the intervention was to use a video based on a man’s first-person narrative storytelling of experiences with depression. Storytelling is a powerful medium through which the storyteller’s personal narrative can stimulate the viewers to deeply engage with the intended message of the story (Heo, 2009). Narrative theory (Fisher, 1984) suggests that stories are a natural part of human experiences and a significant medium through which people can share and connect on various life experiences. The storytellers convey their life experiences through stories, and the listeners and viewers can develop interpretations and meaning from the narratives of the stories. Often, the stories contain powerful meaning-making and reflective elements that persuade and motivate people in certain ways (Kreuter et al., 2007). Specific to health-related stories, Harter and Bochner (2009) note that narrative storytelling can help the viewers and listeners to engage in meaning-making around the process of healing, which provides hope and agency for individuals to work through their health issues and seek support. For this reason, narrative storytelling is often used in health communication interventions and persuasive marketing to promote cost-effective attitude and behavior changes, including health-related outcomes such as quitting smoking (Lipsey et al., 2020; Pulizi, 2012), promotion of advocacy against gender-based violence (Mannell et al., 2018), and informing the public about health disparities (Lee et al., 2016).
Three factors of the narrative theory guide how narrative storytelling may promote men’s help-seeking attitudes for depression: transportation, identification, and realism. Green and Brock (2000) suggest that transportation occurs when viewers are absorbed into the narrative flow of the story and are aroused both cognitively and emotionally (Krause & Rucker, 2020). In essence, they are “transported” into the storyteller’s world. Identification also plays a significant factor as it allows the listener and the viewer to engage in perspective taking and visualizing of the storyteller’s positions (Bussell & Bilandzic, 2009). Finally, realism, or how authentic and plausible the story is for the listener and the viewer, helps to connect with the story in a realistic way (Murphy et al., 2013). These three elements help explain how storytelling can persuade listeners and viewers to re-examine their beliefs and encourage them to consider changes in attitudes and behaviors. Based on these mechanisms, it is possible that a man’s narrative storytelling regarding depression and help-seeking efforts may persuade other men to re-examine their core beliefs of TMI and self-stigma of seeking help, and ultimately consider seeking help for depression.
Applying this framework, we theorized that men who view a video of another man telling a real story about their depression and help-seeking experiences may connect with the storyteller at a deeper emotional and cognitive level, thereby being persuaded to form a more positive attitude toward psychological help-seeking. Specifically, we examined whether exposure to such video would be able to buffer the higher self-stigma of seeking help associated with higher TMI among men, which would otherwise result in more negative attitudes toward psychological help-seeking (see Figure 1; Levant, Stefanov et al., 2013). The effect of the video was tested with a controlled design in which the results for the video group were compared to (a) the brochure group, who were exposed to a male-sensitive depression resource brochure (Hammer and Vogel, 2010); and (b) the control group, who were not exposed to any material. We hypothesized that the indirect relations of TMI on psychological help-seeking attitudes via self-stigma of seeking help would be non-significant or significantly lower for the video group compared to the brochure and control groups. In examining the models, we controlled for depressive symptoms as pre-existing levels of depression may be associated with attitudes toward psychological help-seeking (Call & Shafer, 2018). Indirect relation of traditional masculinity ideology on attitudes toward seeking psychological help via self-stigma. Note. C = Control; B = Brochure, V = Video. *p < .05, **p < .01, ***p < .001.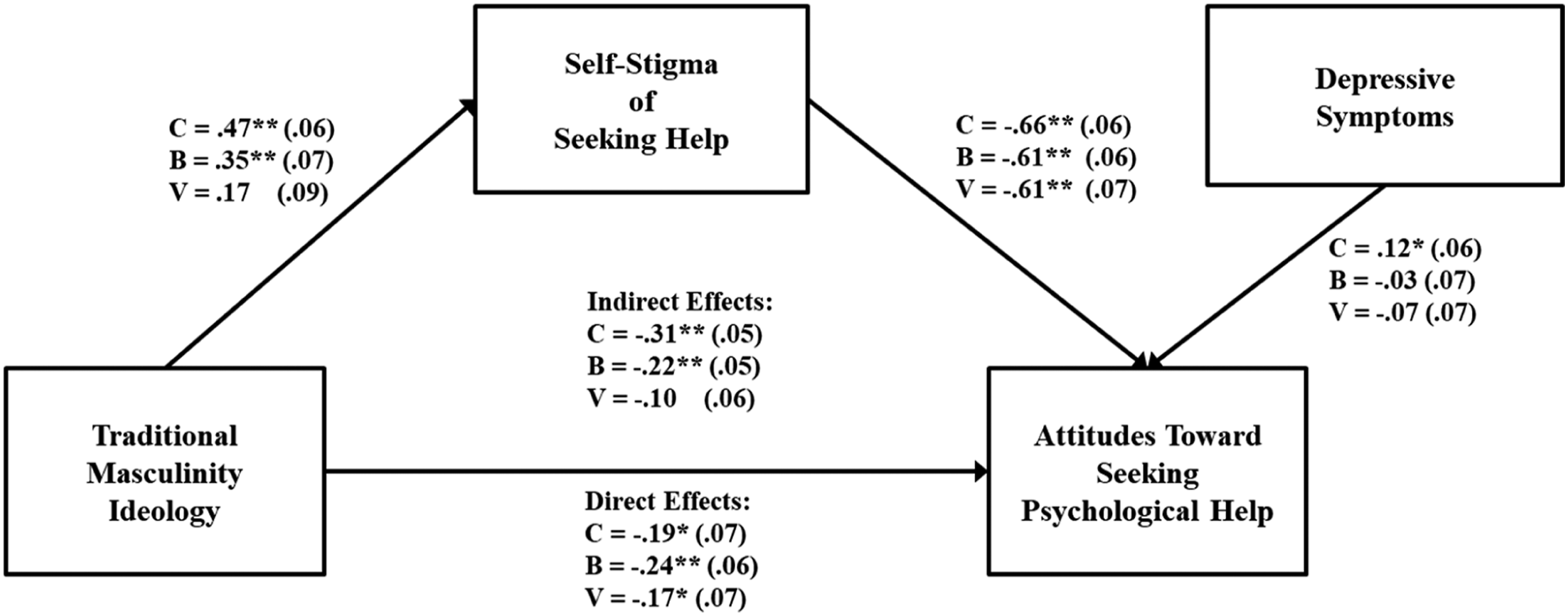
Methods
Participants
Participants were 396 adult men currently residing in the United States. Participants’ ages ranged from 15 to 80 years old (M = 35.62, SD = 12.92, Mdn = 32). Most of the participants were White (n = 270; 68%), 10% Hispanic American/Latinx (n = 41), 8% Asian/Asian American (n = 33), 7% African American/Black (n = 29), 4% Multiracial (n = 14), 2% (n = 9) Native American/Alaskan Native, and 1% other (n = 4). About 83% were heterosexual (n = 319), 9% bisexual (n = 37), 4% gay (n = 15), 1% uncertain (n = 3), 1% asexual (n = 3), and 2% other (n = 6). In terms of religion, 51% were Christian (n = 201), 18% Agnostic (n = 73), 16% Atheist (n = 62), 3% Buddhist (n = 10), 2% Earth Religion (n = 7), 2% Hindu (n = 7), 1% Jewish (n = 5), 1% Muslim (n = 3), and 6% Other (n = 28). About 90% (n = 358) indicated that English was their first language.
Male-Sensitive Brochure
We used the evidence-based male-sensitive brochure (MSB) developed by Hammer and Vogel (2010). The MSB incorporated current knowledge from the psychology of men and masculinity and mental health marketing (Hammer & Vogel, 2010) and was developed to be sensitive to unique stigma and attitudes toward seeking counseling among men. The 6-page MSB included the following information: (1) information differentiating the “blues” from depression, (2) pictures of four men and their short accounts of depression experiences, (3) facts about men and depression, (4) a frequently asked questions section, (5) promotion of courage to seek help, and (6) pictures of the four men presented again with a note saying they took the courage to seek help. 1
Real Story Video
The real story videos hosted on HeadsUpGuys (Ogrodniczuk et al., 2018) were shown to the participants. The men in these videos told brief first-person stories about their depression and help-seeking experiences. The videos were 3–4 min long. Videos were racially matched as character identification likely plays a significant role in the impact of the contents (Bussell & Bilandzic, 2009). We used Mitchell’s video for White men and Rich’s video for men of color. These videos were selected as they provided a male-sensitive discussion on difficulties in seeking help for depression. The two stories also contained shared components and seemed particularly relevant to the general experiences of the younger adult men who may not have considered seeking psychological help. Rich talks about the impact of his father’s health tragedy on Rich’s own health, struggling with emotions and feeling alone, struggling at university, isolation, attempting suicide, reaching out, building support, and surrounding himself in positive environments. Mitchell talks about stress at school, feeling helpless from not being able to help an ill family member, not wanting to be a burden on his family, keeping his pain hidden, talk therapy, managing stress, and building a team of supports. 2
Measures
Psychological Help-Seeking Attitudes
The Attitudes Toward Seeking Professional Psychological Help Scale-Short Form (ATSPPHS-SF; Fischer & Farina, 1995) was used to assess psychological help-seeking attitudes. The measure contains 10 items using a Likert scale ranging from 1 (disagree) to 4 (agree). Five items are reverse scored; higher scores indicate a more favorable attitude toward seeking psychological help. Validity has been evidenced by positive relationships with U.S. college students’ prior help seeking behavior (Fischer & Farina, 1995), intentions to seek counseling (Garriott et al., 2017), and negative relationships with self-stigma of seeking help (Garriott et al., 2017; Vogel et al., 2006). Internal consistency for the current study was .82.
Self-Stigma
The Self-Stigma of Seeking Help scale (SSOSH; Vogel et al., 2006) was used to assess self-stigma on seeking psychological help. The measure contains 10 items using a Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Five items are reverse scored; higher scores indicate stronger self-stigma for seeking psychological help. Validity has been established by negative relationships with attitudes toward seeking professional psychological help and intentions to seek counseling, and positive relationships with public stigma for seeking psychological help (Garriot et al., 2017; Vogel et al., 2006). Internal consistency for the current study was .86.
Depressive Symptoms
Patient Health Questionnaire-9 (PHQ-9; Kroenke & Spitzer, 2002) was used to assess depressive symptom severity. Participants rate nine items on a 4-point Likert-type scale (0 = not at all to 3 = nearly every day). Scores range from 0 to 27 with higher scores indicating more severe symptomatology. Validity and measurement invariance of PHQ-9 with racially-diverse adults in the U.S. has been established (Keum, Miller et al., 2018). Internal consistency for the total scale score in our sample was .92.
Traditional Masculinity Ideology
We used the Male Role Norms Inventory-Short Form total score (MRNI-SF; Levant, Hall et al., 2013) to assess participants’ adherence to traditional masculinity ideology. MRNI-SF is a 21-item self-report measure of total traditional masculinity score and seven subscale scores: Restrictive Emotionality, Self-Reliance Through Mechanical Skills, Negativity Toward Sexual Minorities, Avoidance of Femininity, Importance of Sex, Dominance, and Toughness. Participants are asked to rate their agreement with each item on a 7-point Likert scale from 1 (strongly disagree) to 7 (strongly agree). Higher scores indicate a greater endorsement of traditional masculinity. Validity of the general traditional masculinity factor has been established with positive relationships with other masculinity-related constructs (e.g., Conformity to Masculine Norms Inventory-46; Levant et al., 2015). Internal consistency for the current study was .95.
Exposure Check and Perceived Persuasiveness
To check that participants actually viewed the brochure or the video, we included several exposure check items. For the video, participants were asked (4 choices) what precipitated the depression of the man telling his story in the video. Given that the men talk about the precipitation at length throughout the two videos, we expected participants to be able to adequately answer this question if they had watched the video. For the brochure, we included three attention check true or false items which were all true: (1) There were pictures of men in the brochure, (2) The brochure contained brief stories from men, and (3) The brochure had a frequently asked questions section.
To assess whether the brochure and the video had an intended persuasive impact on the participants (O’Keefe, 2018), we developed four items on a 6-point scale (Not at all to Very Much) that asked participants about their perceived persuasiveness after viewing the brochure/video. Sample items read: “The brochure/video was designed to persuade,” “The brochure/video was trying to advance a particular point of view.”
Procedures
The study was approved by the Institutional Review Board. Participants were invited to take an online survey hosted by Qualtrics. Recruitment messages were advertised through e-mail (e.g., listserves), discussion forums, and online social networks for men residing in the U.S. (e.g., Facebook pages, Yahoo groups, Google groups). Participants were told that they would be reviewing materials for mental health related materials. The survey contained the measures assessing pre- and post-intervention variables, demographic questions, and attention check items (e.g., “Please choose always”). The inclusion criteria for the study were: (a) 18 years or older, (b) identify as a man, (c) currently reside in the U.S, and (d) no previous counseling experiences. Upon consent, participants clicked on an external Qualtrics link and completed a 30-minute survey. Participants had a chance to enter a raffle to win a $50 gift card. At the end of the survey, all participants were provided with debriefing information and resources for depression. Those who endorsed clinically high PHQ-9 scores (>14) or endorsed the suicidality item were contacted to provide additional resources.
Following the pre-intervention measures (in the order of MRNI-SF, SSOSH, PHQ9), participants were randomly assigned to either a control (nothing), brochure, or video condition by the randomize functionality in Qualtrics survey. After viewing the brochure or the video, they completed post-intervention measures (in the order of ATSPPHS-SF, exposure check items of brochure/video, perceived persuasiveness of brochure/video). Participants in the control condition proceeded straight to post-intervention measures (only ATSPPHS-SF).
Analyses and Results
Data Inspection and Preliminary Analyses
Of the 580 participants who completed the survey, we removed 3 cases for not meeting the study consent/inclusion criteria, 69 cases for failing the attention/validity check items, and 112 cases due to missing more than 20% of the data and incorrectly answering exposure check items for the brochure/video. The final sample size was 396, among which 27 cases were missing up to 20% of the data. First, we examined the existence and pattern of missing values in the data set. Little’s missing completely at random (MCAR) test was significant, suggesting that missing data in our sample were not completely random, χ2 (1660) = 1901.85, p < .001. Correspondingly, we used the expectation maximization estimates for multiple imputation of the missing values in SPSS, and calculated the mean or total scores for the corresponding scales, which were used in subsequent analysis. Sample sizes were 149, 137, and 110, for control, brochure, and video conditions, respectively, which were adequate or close to the minimum sample size of 120 to detect at least a small effect based on the message persuasion literature.
Descriptives and Bivariate Correlations of Study Variables.
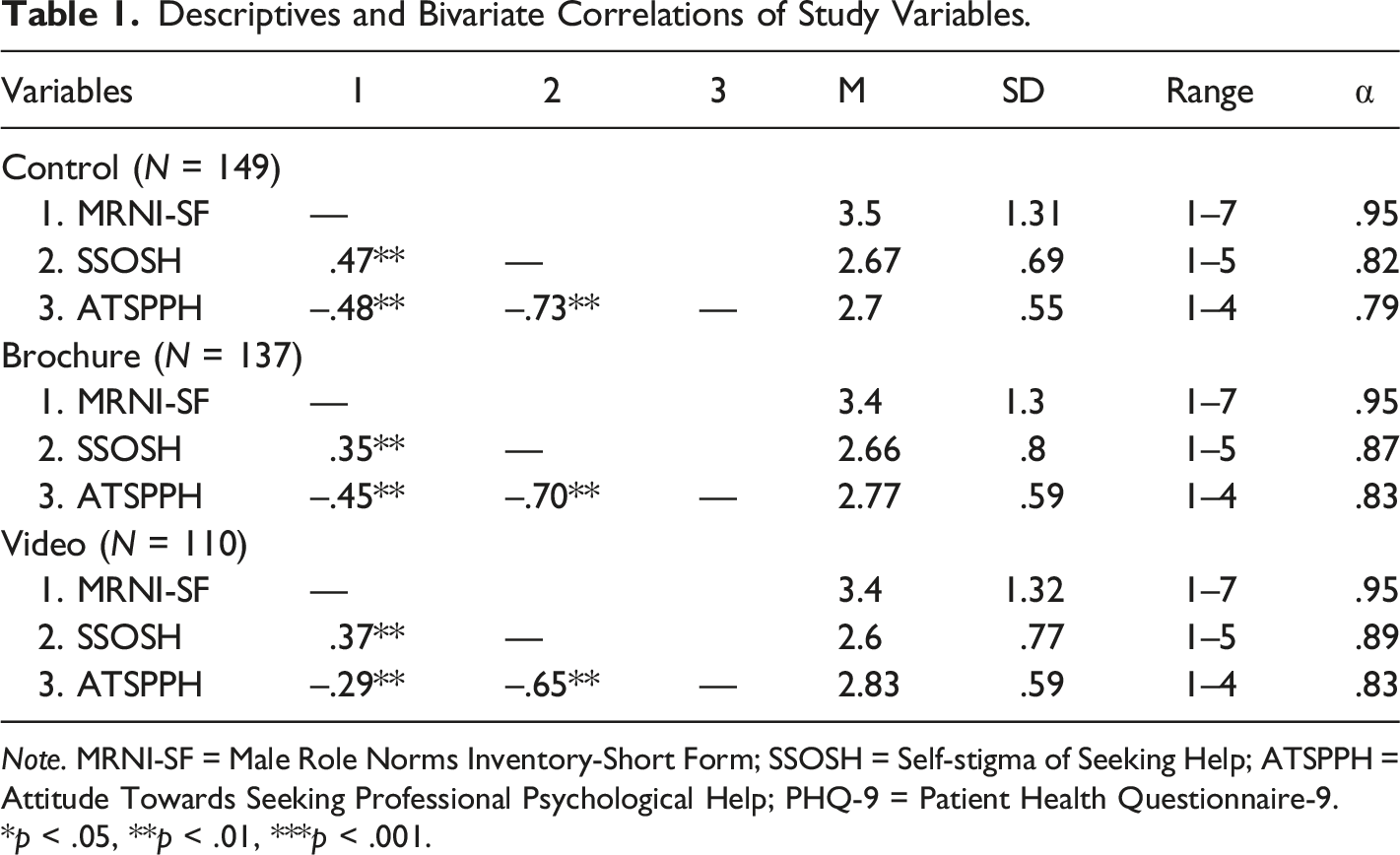
Note. MRNI-SF = Male Role Norms Inventory-Short Form; SSOSH = Self-stigma of Seeking Help; ATSPPH = Attitude Towards Seeking Professional Psychological Help; PHQ-9 = Patient Health Questionnaire-9. *p < .05, **p < .01, ***p < .001.
Base Model with Full Sample
We used Mplus 8.0 (Muthen & Muthen, 2017) to first establish our base model of the hypothesized paths with the full sample using maximum likelihood estimation (Figure 1). Overall model fit indices suggested that our hypothesized model fit with the data adequately per the recommended thresholds (Hu & Bentler, 1999): χ2 = 4.644, df = 1, p = .031; RMSEA = .096 (CI = [.023, .191]); CFI = .987; TLI = .936; SRMR = .036. We proceeded to examine the specific path coefficients and the specific indirect (i.e., mediation) effect. To calculate the indirect effect, we adopted the bootstrap method with 5000 random samples, which has the advantage of not assuming a normal distribution and using randomly generated samples to more accurately determine the standard errors, confidence intervals (CI), and the significance of the indirect effect (Hayes & Scharkow, 2013). We used the 95% CI to assess the significance levels: if the 95% CI did not include zero, the estimates were considered significant at the p < .05 level.
The direct path from MRNI-SF to ATSPPH was negative and significant (β = −.21, p < .05), and the path from MRNI-SF to SSOSH was positive and significant (β = .34, p < .05). The path from SSOSH to ATSPPH was negative and significant (β = −.63, p < .05). The path from PHQ9 to ATSPPH was not significant (β = .02, p = .61). Overall, we found a significant negative direct effect of MRNI-SF on ATSPPH (β = −.206, 95% bootstrapped CI = [−.270, −.142]) that accounted for 49.2% of the total effect, and a significant negative indirect effect via SSOSH (standardized indirect effect β = −.213, 95% bootstrapped CI = [−.265, −.161]) that accounted for the remaining 50.8% of the total effect. Results suggested a partial mediation pattern for the overall sample.
Multi-Group Analysis Across the Conditions
Estimate of Indirect Effects from Bootstrap Analysis.
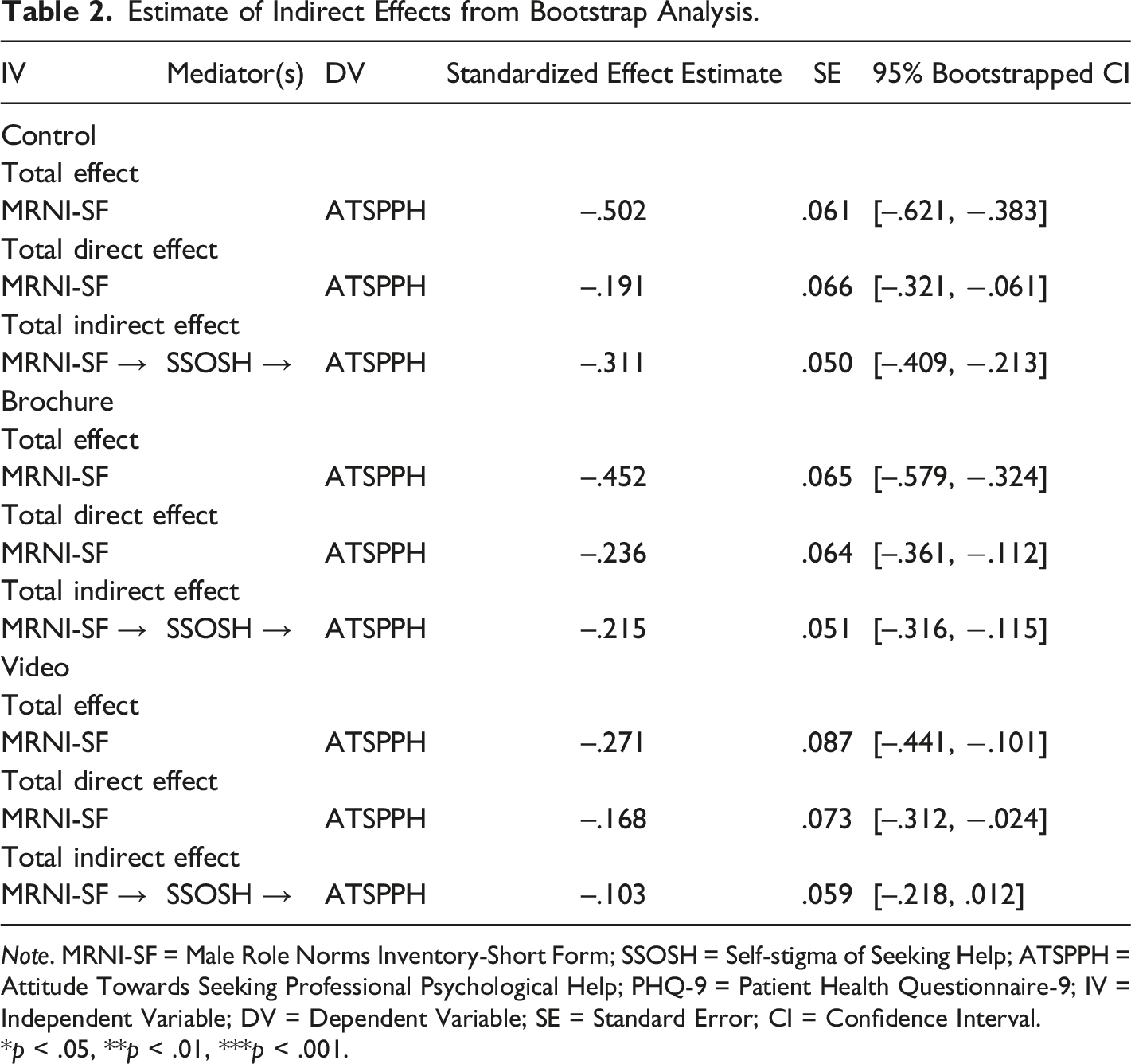
Note. MRNI-SF = Male Role Norms Inventory-Short Form; SSOSH = Self-stigma of Seeking Help; ATSPPH = Attitude Towards Seeking Professional Psychological Help; PHQ-9 = Patient Health Questionnaire-9; IV = Independent Variable; DV = Dependent Variable; SE = Standard Error; CI = Confidence Interval. *p < .05, **p < .01, ***p < .001.
For the control group, the direct effect was significant (standardized effect = −.191, SE = .066, 95% bootstrapped CI = [−.321, −.061]) and accounted for 38% of the total effect. The indirect effect was significant (standardized effect = −.311, SE = .050 95% bootstrapped CI = [–.409, −.213]) and accounted for the remaining 62% of the total effect. These results suggested a partial mediation pattern (see Table 2).
For the brochure group, the direct effect was significant (standardized effect = −.236, SE = .064, 95% bootstrapped CI = [−.361, −.112]) and accounted for 52.2% of the total effect. The indirect effect was significant (standardized effect = −.215, SE = .051, 95% bootstrapped CI = [−.316, −.115]) and accounted for the remaining 47.8% of the total effect. These results suggested a partial mediation pattern (see Table 2). The Wald test of parameter constraints suggested that the indirect effect on ATSPPH for the brochure group was not significantly different than the indirect effect on ATSPPH for the control group, χ2 (1) = .817, p = .37. Between the control and brochure group, the direct path was not significantly different, χ2 (1) = .463, p = .496.
For the video group, the direct effect was significant (standardized effect = −.168, SE = .073, 95% bootstrapped CI = [−.312, −.024]) and accounted for 62% of the total effect. The indirect effect was nonsignificant (standardized effect = −.103, SE = .059, 95% bootstrapped CI = [−.218, .012]) and accounted for the remaining 38% of the total effect. Hence, as hypothesized, with the video group, the nonsignificant indirect effect suggested that the video had a buffering role on the indirect relations of MRNI-SF and SSOSH on ATSPPH (see Table 2). Of note, the direct effect was approaching non-significance as the upper 95% CI was reaching 0. Compared to the brochure and control group, the Wald test of parameter constraints suggested that the direct path from MRNI-SF to ATSPPH was significantly lower for the video group compared to the brochure group, χ2 (1) = 11.282, p = < .001, and the control group, χ2 (1) = 8.745, p = .003.
Discussion
This is the first study to examine the role of online video-based narrative storytelling in improving men’s psychological help-seeking for depression. The findings suggest that exposure to a brief first-person storytelling video significantly buffered the negative impact of self-stigma of seeking help associated with TMI. In fact, self-stigma of seeking help was a non-significant mediator only in the video group, whereas both the control and brochure groups yielded significant partial indirect relation of TMI on psychological help-seeking attitudes via self-stigma of seeking help. The significance of the direct link between TMI and attitudes was also significantly lower in the video group compared to the brochure and control groups. Thus, in line with the framework of narrative storytelling (Fisher, 1984; Kreuter et al., 2007), the intended persuasive and immersive influence of a first-person storytelling nature of the video (Lipsey et al., 2020) may have been effective in encouraging men to be transported into the story, identify with the storyteller, and be aroused emotionally and cognitively. This experience may have ultimately allowed men to re-examine and reshape their self-stigmatizing beliefs in seeking help associated with TMI and become more open to considering psychological help-seeking (Levant, Stefanov et al., 2013).
As we speculated about content sensitivity and specificity, the use of male-sensitive and depression-specific video content may have been the major driver behind the findings. Whereas a generalized mass-media intervention had no effect in reducing the self-stigma of seeking help (Demyan & Anderson, 2012), the men in the current study were exposed to a more personally- and masculinity-relevant video that might have augmented the process of realism (Murphy et al., 2013) and identification (Bussell & Bilandzic, 2009). As we reviewed, perceiving the story and the storyteller to be authentic and identification with the storyteller are key requirements for effective persuasive storytelling (Bussell & Bilandzic, 2009). In the current study, to augment identification, racial matching was also conducted given the disparities in depression experiences between White men and men of color (Griffith et al., 2012; Vogel et al., 2011). Ideally, more specific racial matching among men of color would have been preferred, but the male-sensitive approach and racial matching, coupled with exposure to a powerful medium of storytelling, likely maximized the men’s identification with the storyteller and the favorable message toward psychological help-seeking.
One interesting finding is that while the video had a buffering role, the video and brochure groups did not significantly differ in the perceived persuasiveness. This is especially notable since the indirect effect in the brochure group was significant, and not significantly different than the condition group, even though the perceived persuasiveness of the brochure was similar to that of the video. This discrepancy may be reflecting the transportation mechanisms of the storytelling framework that was not assessed in the current study. For instance, exposure to immersive storytelling has been shown to increase empathy toward particular characters or issues presented in the story (Bang & Yildirim, 2018). In our case, it is possible that men in the video group may have developed greater empathy toward men experiencing depression.
Harnessing the intersection of online media and the power of persuasive narrative storytelling, our findings show potential for storytelling videos such as the ones tested in the current study for shifting the culture and narrative around men’s help-seeking for depression. This implication is particularly timely given the prevalence of untreated depression and completed suicides among men (Centers for Disease Control and Prevention, 2019). In addition to the role of untreated depression, studies suggest that impulsive and aggressive beliefs and behaviors associated with TMI may also contribute to completed suicides among men (Dumais et al., 2005). Against this concerning health disparities trend, online storytelling videos may be scaled up to drive national campaigns (Lefebvre et al., 2020) to encourage men to seek help for their depression and suicide risk. Doing so may also spread messages of hope and healing (Harter & Bochner, 2009) for men suffering from depression and validation for men to share their distress with others (Keum et al., 2021). This is particularly important as robust intrapersonal norms such as TMI and self-stigma of seeking help require group level interventions for more effective attitude and behavioral change rather than individual level interventions Keum, Hill et al., 2018). The narrative storytelling framework fits naturally as a potential group level intervention as it emphasizes community and relationship building through the power of shared stories (Kreuter et al., 2007). Furthermore, Online media is a promising and efficient avenue for disseminating stories and creating a reflective medium to change men’s beliefs, attitudes, and behaviors, given the cost-effectiveness of the method and the breadth of reachable population.
Despite the contributions of the current study, limitations call for further research for intervention application. First, although we tested an empirically established link between TMI, self-stigma of seeking help, and attitudes, we are not able to assess directionality given the cross-sectional design of the current study. In addition to examining causality, a longitudinal study would be needed to examine whether men who viewed the video actually sought help, and if so, what their outcomes were. Second, a longitudinal approach would also be important to delineate between the roles of self-stigma of seeking help and attitudes toward psychological help-seeking as the two constructs retain conceptual similarities and may influence the order of the variables in the model. Third, a longitudinal study would be able to better test the efficacy of the video by increasing the time between pre-test and post-test measures. In our study, the pre-test and post-test measures were given immediately before and after the brochure and video conditions. This may have affected how participants responded to the post-test measures, as the recency of the video may have persuaded participants to feel more improvements in their help-seeking. Future studies would need to test whether such a response would still hold if greater time has passed after viewing the video. Fourth, even though we theorized mechanisms associated with exposure to storytelling, other than perceived persuasiveness and exposure check, we did not assess for other indicators such as emotional and cognitive arousal, or state empathy. For instance, men with increased empathic reactions to other men experiencing depression reported greater intentions to seek psychological help (Keum et al., 2021). These variables would need to be examined given that they are linked to how people are affected by media messages and can be additional intervention points (Bang & Yildirim, 2018). Fifth, although the sample sizes were adequate or close to the minimum required to detect a small effect, the findings are limited in generalizability. Specifically, we assessed men’s general experiences with TMI, depression, and self-stigma of seeking help even though disparities are observed in men of color, and across specific racial/ethnic groups among men of color (Griffith et al., 2012; Levant et al., 2022). Furthermore, other demographic factors such as education and relationship status could play a role in men’s help-seeking attitudes. Thus, future studies with larger samples would need to test culture-specific and sensitive video content and variables to examine culturally-informed stigma and help-seeking attitudes. A larger sample would also provide more power to detect additional findings, such as a potential non-significant direct effect in the video group as the estimate was reaching non-significance. Last, we are not able to discuss whether the male-sensitive aspects of the video contributed to our findings as we did not include a general video group (e.g., gender neutral) to tease out the differences. It would be important for future studies to refine the effects of male-sensitivity and -relevance in video interventions.
In conclusion, findings suggest initial and promising evidence on brief male-sensitive first-person storytelling videos for reducing the self-stigma of seeking help among men who have not previously sought psychological help. Male-sensitive storytelling videos, such as the ones used in the current study, may be useful clinical and educational tools to help men reconsider their options for seeking psychological help for depression. It may be especially helpful to employ these videos for men who are experiencing depression but are unwilling to consider mental health services due to their belief that doing so would undermine their masculine self-concept. Given that these videos can be watched at their own leisure and privacy, the videos may be a gentle and non-invasive way to get men started on changing their attitude toward seeking psychological help.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bruce C. Abrams Emerging Scholars Grant from Active Minds.
Ethics Approval
Ethics approval for the study was granted by the Institutional Review Board.