
Abstract
Objective:
The purpose of this review is to evaluate the efficacy and safety of plozasiran, a novel agent recently approved by the US Food and Drug Administration for familial chylomicronemia syndrome (FCS).
Data Sources:
A comprehensive literature search was conducted in PubMed and the National Institutes of Health Clinical Trials Registry (http://www.clinicaltrials.gov) from April 2014 to April 2026 using the keyword “plozasiran.” Trials that were phase 1 trials, review papers, pooled analyses of trials, or ongoing studies without complete results were excluded.
Study Selection and Data Extraction:
Phase 2 and 3 trials assessing plozasiran’s safety and efficacy were included. Initially, 57 articles were yielded, and 3 studies were included after application of inclusion criteria.
Data Synthesis:
The findings from this review indicate that plozasiran is overall a safe and effective medication to significantly lower triglycerides and acute pancreatitis in patients with FCS.
Relevance to Patient Care and Clinical Practice in Comparison to Existing Drugs:
Plozasiran is a novel agent that targets a similar pathway as olezarsen but requires less frequent administration (4 times a year for plozasiran vs 12 times a year for olezarsen). While this may help with patient adherence compared to olezarsen, plozasiran’s higher annual cost (approximately $72 000/year) compared to olezarsen ($40 000/year) may limit use for FCS management.
Conclusions:
Plozasiran offers an alternative pharmacological agent to olezarsen for management of FCS in the United States. Currently, there are limited data evaluating the long-term outcomes of plozasiran use in patients with FCS.
Introduction
Familial chylomicronemia syndrome (FCS) is a disease that can be challenging to diagnose, and has historically had limited approaches to management outside of dietary restriction strategies, significantly impacting quality of life. 1 This autosomal recessive disorder is caused by biallelic loss-of-function variants within the lipoprotein lipase (LPL) gene or other genes that code for necessary components of LPL activity. 2 This reduction in LPL function results in elevated triglyceride (TG) levels due to reduced chylomicron degradation. This can cause patients to experience symptoms such as nausea, vomiting, eruptive xanthomas, and acute pancreatitis, requiring frequent hospitalizations and medical care. 2
Importantly, FCS should be differentiated from multifactorial chylomicronemia syndrome (MCS), both of which result in elevated TGs. Two scores are available (FCS Score and North American Familial Chylomicronemia Score) to help with differentiation and avoid misdiagnosis.3,4 Patients with FCS have decreased or normal levels of very-low-density lipoproteins (VLDL), whereas patients with MCS have elevated VLDL levels. 5 In addition, acute pancreatitis has been found to occur at a higher incidence in patients with FCS compared to MCS (81.8% and 35.2%, respectively). 6
Management of FCS has been centered on dietary restriction strategies that include a reduction in dietary fat, avoiding alcohol, consuming complex carbohydrates, and meeting physical activity goals. 2 In addition, medium-chain TGs, which are metabolized through a chylomicron-independent pathway, can be taken as a supplement to provide additional calories and fat. Pharmacologic agents such as fibrates and omega-3 fatty acids have not been found to significantly lower TGs in patients with FCS, or decrease the incidence of acute pancreatitis. 5
Recently, newer medications that target apolipoprotein have demonstrated significant reductions in both TGs and the incidence of acute pancreatitis via decreased synthesis of apolipoprotein CIII (apo-CIII). Apo-CIII, a 79 amino acid glycoprotein, is synthesized in the liver and intestine. 7 It is found on chylomicrons, VLDL, intermediate-density lipoprotein (IDL), and low-density lipoprotein (LDL) particles. This glycoprotein inhibits LPL activity to decrease chylomicron lipolysis, and also decreases hepatic reuptake of chylomicron remnants. 7 Apo-CIII inhibits breakdown of chylomicrons via LPL-dependent and independent pathways, which allows apo-CIII inhibitors in patients with FCS to (1) prevent inhibition of LPL activity and (2) prevent inhibition of LPL-independent pathway catabolism of TGs.1,2,5
Volanesorsen, an antisense oligonucleotide (ASO) that targets apo-CIII production, was approved in Europe for patients with FCS. 1 The APPROACH trial (2019) found a 77% reduction in TG levels at 3 months in patients randomized to volanesorsen 300 mg subcutaneously (SQ) given once weekly vs an 18% TG reduction seen in the placebo group. 8 In addition, acute pancreatitis occurred in fewer patients receiving volanesorsen compared to placebo (1 patient and 3 patients). 8 The COMPASS trial (2021) evaluated volanesorsen in patients with MCS, but 7 of 114 patients did have FCS. 9 Volanesorsen was found to decrease TG levels in the 7 patients with FCS by 73% and 69% at 3 and 6 months, respectively. 9 The Food and Drug Administration (FDA) ultimately did not grant approval to volanesorsen due to concerns of adverse effects, most notably thrombocytopenia.
In December 2024, the FDA approved olezarsen (Tryngolza) as an adjunct to diet to decrease TGs in adults with FCS. 10 Similar to volanesorsen, olezarsen is an ASO that inhibits apo-CIII production. In the BALANCE trial (2024), olezarsen was found to significantly reduce TG levels in patients with FCS at 6 months by 43.5% in the 80 mg group and 22.4% in the 50 mg group (dosed SQ every 4 weeks). 11 Two episodes of acute pancreatitis occurred in patients randomized to olezarsen (1 in the 80 mg group and 1 in the 50 mg group) and 11 episodes were reported in the placebo group (occurred in 7 patients). 11 Importantly, the thrombocytopenia observed with volanesorsen use was not reported in the BALANCE trial. 11 This FDA approval provided a long-awaited effective pharmacological option for FCS patients in the United States.
In November 2025, the FDA approved the newest apo-CIII targeting medication, plozasiran (Redemplo), as an adjunct to diet in patients with FCS to decrease TGs.12 -14 This is a novel agent that adds an additional option for FCS patients to manage TGs and prevent the ramifications of unopposed, elevated TGs. The purpose of this article is to review the pharmacology, pharmacokinetics, efficacy, and safety of plozasiran.
Data Selection
We performed a literature search from April 2014 to April 2026, using the keyword “plozasiran” in the PubMed database and the National Institutes of Health Clinical Trials Registry (http://www.clinicaltrials.gov). Phase 2 or 3 trials, in English, evaluating the efficacy and safety of plozasiran were included. A total of 57 articles were identified. After applying inclusion criteria, 3 studies were included in the review. Articles that were phase 1 trials, review papers, pooled analyses of trials, or ongoing studies without complete results were excluded.
Pharmacology
Mechanism of Action
Plozasiran differs from volanesorsen and olezarsen in that it is a small interfering ribonucleic acid (siRNA) conjugated with N-acetylgalactosamine (GalNAc) rather than an ASO (of note, olezarsen does have a GalNac3 moiety).7,13 -15 Plozasiran targets the apo-CIII messenger ribonucleic acid (mRNA), which ultimately results in mRNA degradation to prevent apo-CIII production. 15 All 3 agents target posttranscriptional apo-CIII gene silencing, but there are pertinent differences between ASO and siRNA therapy to note. 16 Plozasiran, an siRNA therapy, has an antisense and sense strand. When in the hepatic cell nucleus, the sense strand guides the antisense strand to the RNA-induced silencing complex (RISC). 16 When attached to the RISC, the antisense strand targets the apo-CIII mRNA and the complex of the antisense and RISC degrade the target mRNA. This complex can inactivate multiple mRNA molecules, which allows for less frequent dosing. Agents that are ASOs bind directly to the target mRNA as deoxyribonucleic acid (DNA) in the cell nucleus and cause RNase H mRNA degradation. 16 The DNA is available to bind to subsequent targets, but the dosing frequency is more frequent than siRNA therapy. Newer generation ASOs are conjugated to GalNAc (ie, olezarsen) for more targeted delivery of the agent to the liver. 16 Volanesorsen is not conjugated to GalNAc and thus not as selective for its target. This may contribute to the thrombocytopenia observed with volanesorsen use in clinical trials. 16
Pharmacokinetics
In healthy adults who received plozasiran 25 mg the Cmax and Tmax was 68.5 ng/mL and 6 hours, respectively. 15 The majority of plozasiran (78%) is protein bound in vitro and the volume of distribution is approximately 146 L, with distribution occurring in plasma and extracellular body water prior to hepatocellular uptake. Plozasiran’s half-life is 3 to 4 hours and the medication is metabolized by nucleases with 16% to 19% excreted in urine. It is not impacted by CYP450 enzymes in a clinically meaningful manner. 15 The impact of antidrug antibodies on plozasiran effects is also unknown. 15
Dosing and Administration
Plozasiran sodium is only available in a 25 mg/0.5 mL single-dose prefilled syringe, intended for SQ injection. 15 For treatment of FCS when used in combination with a low-fat diet (<20 g of fat per day), plozasiran is given as a 25 mg SQ injection once every 3 months, administered into the abdomen, front of the thigh, or the upper arm. The medication should not be injected into damaged skin, or areas with scars or stretch marks. Plozasiran can be injected by a health care provider, or by the patient and/or caregiver if they have been trained in appropriate administration. Syringes should be stored in the original packaging in the refrigerator prior to use. Intact syringes may alternatively be stored at room temperature (68-77°F) for up to 30 days prior to use but then should be discarded. Missed doses should be taken as soon as possible, with subsequent doses resumed every 3 months from the most recently administered dose.
There are no dose titrations or escalations of therapy with plozasiran. 15 There are no renal dose adjustments when used in patients with an estimated glomerular filtration rate (eGFR) between 30 and 90 mL/min. Use in patients with renal disease and an eGFR of <30 mL/min has not been studied. There is no dosage adjustment recommended for mild hepatic impairment, and patients with moderate to severe hepatic impairment were not included in clinical trials.
Clinical Trials
Of the 3 trials included, 2 were phase 2 trials, conducted in patients with mixed hyperlipidemia and severe hypertriglyceridemia, and 1 was a phase 3 trial conducted in patients with persistent chylomicronemia. Plozasiran received its FDA approval based on the PALISADE trial (2025) in patients with persistent chylomicronemia. A summary of the clinical trials discussed can be found in Table 1.
Summary of Plozasiran Clinical Trials.
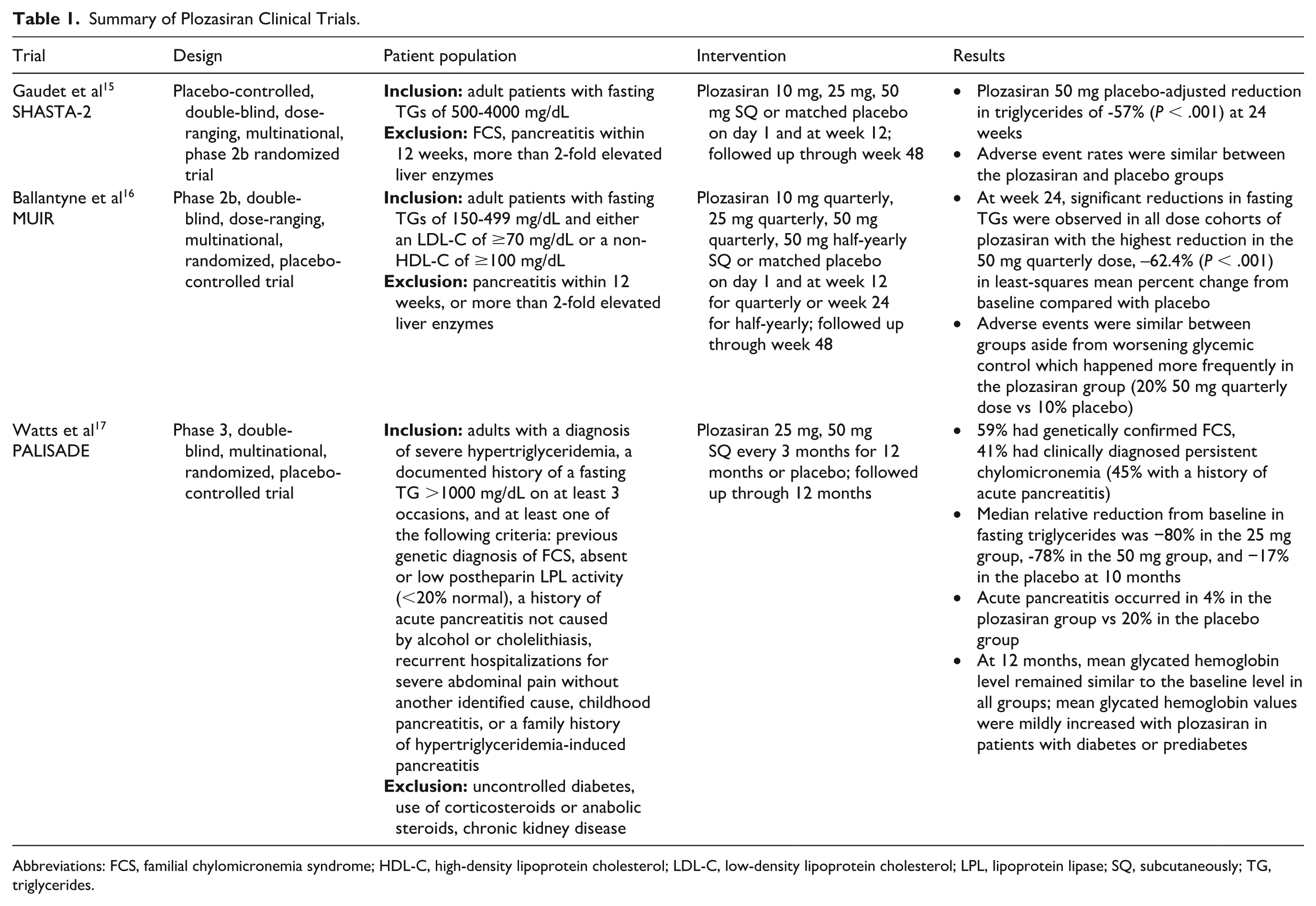
Abbreviations: FCS, familial chylomicronemia syndrome; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; LPL, lipoprotein lipase; SQ, subcutaneously; TG, triglycerides.
The SHASTA-2 Trial
The SHASTA-2 trial was a placebo-controlled, double-blind, dose-ranging, multinational, phase 2b randomized trial. 17 Prior to randomization, participants underwent a 6-week screening and diet run-in period, and then were randomized in a 3:1 ratio to plozasiran (10, 25, or 50 mg) or placebo, stratified by screening TGs. Plozasiran or placebo were administered SQ at weeks 0 and 12 and patients were followed through week 48. 17 All other care, including concomitant medications and diet, was per local standard of care. Adult patients with fasting TG levels of 500 to 4000 mg/dL were included. Patients with FCS, pancreatitis within 12 weeks, plasma apheresis within 4 weeks, >2-fold elevated liver enzymes, and hemoglobin A1c >9% were excluded. 17 The primary end point was the mean difference of percentage TG change between each dose group and pooled placebo groups from baseline to week 24. Secondary endpoints included changes in other lipoproteins, all adjusted for changes observed in the placebo group. 17
A total of 226 patients were included in the primary analysis. The baseline characteristics were similar across the groups with a mean age of 55 years, 78% male, 90% white, mean body mass index (BMI) 32 kg/m2, and mean apo-CIII of 32 mg/dL. 17 Baseline mean TG and low-density lipoprotein cholesterol (LDL-C) levels were 897 and 72 mg/dL, respectively. A total of 64% of patients had diabetes, and 17% had a history of acute pancreatitis, with a majority of patients receiving statins (68%). 17
Plozasiran use resulted in significant dose-dependent least-squares mean reductions in TG levels of −57% (95% confidence interval [CI], –71.9% to −42.1%; P < .001) in the 50 mg dosing arm and in placebo-adjusted reductions in apo-CIII of −77% (95% CI −89.1% to −65.8%; P < .001) at week 24. 17 Both the 10 mg and 25 mg doses were found to significantly reduce TG levels and apo-CIII compared to placebo at week 24. Overall, TG reductions were sustained to week 48. 17 Plozasiran use led to 90.6% of patients reaching a TG level of less than 500 mg/dL at week 24 and 76.5% sustained TGs below this threshold at week 48. Significant reductions in non-high-density lipoprotein cholesterol (HDL-C), remnant cholesterol, and ApoB48 (main apolipoprotein component in TG-rich lipoproteins synthesized in the intestine and helps with dietary lipids transport from the small intestine) were observed at 24 weeks.17-19 No meaningful reduction in lipoprotein(a) was found at 24 weeks. 17
The adverse event profile was similar across treatment groups. 17 The most common adverse events reported with plozasiran use included coronavirus disease 2019 (COVID-19) infection (16%), worsening glycemic control (19%), diarrhea (3%), urinary tract infection (4%), and headache (9%). Three episodes of acute pancreatitis occurred with 2 episodes in the placebo group, and 1 episode in the plozasiran group. 17 All 3 of these patients had a history of acute pancreatitis, with 1 patient in the plozasiran group experiencing pancreatitis 9 months after the final dose of medication during the safety observation period. 17
Overall, the study demonstrated that plozasiran led to dose-dependent substantial decreases in TG levels in patients with severe hypertriglyceridemia with a generally favorable safety and tolerability profile. 17 It should be noted that patients with FCS were excluded from this trial.
The MUIR Trial
The MUIR trial was a phase 2b, double-blind, dose-ranging, multinational, randomized, placebo-controlled trial. 20 Patients were assigned in a 3:1 ratio to receive plozasiran or placebo within 4 cohorts. Patients were randomized to plozasiran 10, 25, or 50 mg SQ on day 1 and at week 12 (quarterly dose), or 50 mg of plozasiran on day 1 and at week 24 (half-early dose), or placebo. 20 Adult nonpregnant patients with a fasting TG level of 150 to 499 mg/dL and either an LDL-C ≥70 mg/dL or a non-HDL-C of ≥100 mg/dL were included. Patients with recent pancreatitis within the last 12 weeks, more than 2-fold elevated liver enzymes, or hemoglobin A1c >9% were excluded. Participants had to have been on a stable diet for at least 2 weeks, had received a stable maximally tolerated dose of a statin for at least 4 weeks, and had been receiving background medications at stable doses. 20 The primary end point was the least-squares mean percent change in the fasting plasma TGs from baseline to week 24. Secondary end points included changes in other lipoproteins (apo-CIII, non-HDL-C, HDL-C, ApoB, LDL-C) at week 24 and through week 48. 20
Of the 353 patients randomized, the baseline characteristics were similar across groups with 1 exception. 20 One difference noted was that a lower percentage of included patients were female in the plozasiran 50 mg half-yearly group (35%) vs the placebo and plozasiran 10, 25, and 50 mg quarterly groups (44%-47%). 20 The mean age was 61 years, 56% were male, and mean BMI was 32 kg/m2. 20 Baseline mean TG and LDL-C levels were 244 and 103 mg/dL, respectively. A total of 61% of patients had diabetes, and 12% were determined to be at high risk for cardiovascular disease. 20
Plozasiran induced significant dose-dependent placebo-adjusted least-squares mean reductions in TG levels of −49.8% (95% CI −59.0% to −40.6%) with the 10 mg quarterly dose, –56.0% (95% CI −65.1% to −46.8%) with the 25 mg quarterly dose, –62.4% (95% CI −71.5% to −53.2%) with the 50 mg quarterly dose, and −44.2% (95% CI −53.4% to −35.0%) with the 50 mg half-yearly dose (P < .001 for all comparisons). 20 TG level reductions began as early as week 4 and persisted to week 48. Among patients treated with plozasiran, 77% to 92%, depending on the dose of plozasiran received, achieved a TG level of less than 150 mg/dL at week 24. 20 Reductions in apo-CIII, non-HDL-C, remnant cholesterol, and ApoB, and increases in HDL-C were observed at 24 weeks. 20
Adverse events that occurred in 5 or more participants were COVID-19 infection, worsening glycemic control, upper respiratory tract infection, urinary tract infection, headache, and bronchitis. 20 No meaningful changes in the mean platelet count or aminotransferase levels were observed. Worsening glycemic control occurred in 10% in the placebo group vs 20% in the 50 mg quarterly group, and 21% in the 50 mg half-yearly group. Participants with diabetes at baseline generally showed more variability in glycemic control. 20
The study investigators concluded that in patients with mixed hyperlipidemia, plozasiran led to dose-dependent substantial decrease in TG levels. Worsening glycemic control seemed to be more significant in the higher dose plozasiran groups. 20
The PALISADE Trial
The PALISADE trial was a phase 3, double-blind, multinational, randomized, placebo-controlled trial. 21 Patients were randomly assigned in a 2:1:2:1 ratio to receive plozasiran 25 mg, placebo, or plozasiran 50 mg, or placebo SQ every 3 months for a total of 12 months. 21 Randomization was stratified according to the baseline TG level. Inclusion criteria included adults with genetically confirmed FCS or clinically diagnosed persistent chylomicronemia. 21 Exclusion criteria included uncontrolled diabetes, use of corticosteroids or anabolic steroids, and chronic kidney disease. 21 The primary end point was the median percent change from baseline in fasting TGs at 10 months. Secondary end points included the primary end point evaluated at 12 months, the percent change in apo-CIII, and incidence of acute pancreatitis. 21
Of 123 patients evaluated, 75 patients were included in the primary analysis. The baseline characteristics were similar across the groups. 21 The mean age was 46 years, 51% female, 73% white, and median BMI was 25 kg/m2. The baseline median TG level was 2044 mg/dL. 21 Fifty-nine percent of patients had genetically confirmed FCS while 41% had clinically diagnosed persistent chylomicronemia, with 45% qualifying based on a history of acute pancreatitis (76% of which was recurrent). 21 A total of 37% of patients had diabetes, and 89% had a previous episode of pancreatitis. A total of 45% of patients were receiving statins, 67% of patients receiving fibrates, and 29% of patients receiving omega-3 fatty acids. 21
Patients in the plozasiran 25 and 50 mg group had a −80% and −78% median relative reduction from baseline in their fasting TG levels, respectively, compared to a −17% median reduction in the placebo group at 10 months. 21 The median percent change in fasting TG levels in the plozasiran group as compared with placebo was −59% (95% CI −90% to −28%; P < .001) in the 25 mg group, and −53% (95% CI, –83% to −22%; P < .001) in the 50 mg group at 10 months. TG level reductions began as early as week 4 and persisted throughout the 12-month treatment period. Apo-CIII changed minimally with placebo but was substantially reduced in both plozasiran arms at 10 and 12 months. 21 There was a total of 2 cases of pancreatitis (4%) in the plozasiran arm vs 7 (20%) in the placebo arm (odds ratio, 0.17; 95% CI 0.03-0.94; P = .03). Levels of non-HDL-C were lower than baseline in the plozasiran groups while HDL-C and LDL-C were higher than baseline. 21
The most common adverse events were abdominal pain, COVID-19, nasopharyngitis, headache, nausea, upper respiratory tract infection, and diarrhea. 21 Adverse events were similar in the placebo group compared to the treatment group apart from COVID-19 infection, which was higher in the treatment group. 21 At 12 months, the mean glycated hemoglobin level remained similar to baseline in all groups; however, mean glycated hemoglobin levels were mildly increased with plozasiran in patients with diabetes or prediabetes. 21 Plozasiran treatment was associated with a nonprogressive mean increase in alanine aminotransferase (ALT) and aspartate aminotransferase (AST) but no increases of more than 3 times the upper limit of normal was noted. Platelet levels remained unchanged between both groups. 21
The authors concluded that in patients with persistent chylomicronemia, defined as genetically confirmed FCS or clinically diagnosed, plozasiran significantly lowered TG levels and reduced the incidence of pancreatitis compared to placebo. 21
Ongoing Studies
A search was conducted on ClinicalTrials.gov and 6 ongoing studies evaluating plozasiran were found.22-27 Five studies are phase 3 studies of the SHASTA and MUIR trials, looking at plozasiran in patients with either hypertriglyceridemia (150-499 mg/dL) or severe hypertriglyceridemia (≥ 500 mg/dL).22-26 The MUIR-3, SHASTA-3, and SHASTA-4 trials examine the surrogate end point of percent change in fasting serum TG levels at 12 months as the primary end point while SHASTA-5 examines a clinical end point looking at time to first occurrence of positively adjudicated acute pancreatitis event.22-25 The SHASTA-10 trial is an open-label extension study focusing on treatment-emergent adverse events. 26 One study enrolled patients with FCS; however, this study is specific to the Chinese patient population. The study’s preliminary results reported that plozasiran significantly decreased TG levels compared to baseline at both 10 and 12 months compared to placebo at the 25 and 50 mg dose given SQ every 3 months. 27 All studies were funded by Arrowhead Pharmaceuticals.
Adverse Events/Precautions
The most reported adverse events from clinical trials include COVID-19 infection (11%-25%), worsening glycemic control (15%-19%; 2 patients in the PALISADE trial had new antidiabetic agents added), nasopharyngitis (14% in the PALISADE trial), headache (5%-16%), nausea (14% in the PALISADE trial), upper respiratory tract infection (8%-10% in the MUIR and PALISADE trials), urinary tract infection (4% in the SHASTA-2 and MUIR trials), diarrhea (3%-10% in the SHASTA-2 and PALISADE trials), and injection site reaction (0.6%-10% in the SHASTA-2 and PALISADE trials).17,20,21
Worsening glycemic control was an adverse event reported in all 3 trials. Events were more likely reported in the 50 mg dose group.17,20,21 In the SHASTA-2 trial, the least-squares mean of hemoglobin A1c difference vs placebo at 24 weeks was 0.1%, 0%, and 0.5%, respectively, for the 10, 25, and 50 mg doses. Worsening glycemic control only occurred in patients with diabetes at baseline. 17 In the MUIR trial, worsening glycemic control occurred in 10% of the patients in the placebo group vs 12% in the 10 mg quarterly group, 7% in the 25 mg quarterly group, 20% in the 50 mg quarterly group, and 21% in the 50 mg half-yearly group. In a post hoc analysis, it was found that patients in the placebo group and those in the 10 and 25 mg quarterly groups had similar findings regarding adverse glycemic events vs those in the 50 mg groups. Patients in the 50 mg groups had more adverse events related to glycemic control, excursions into the diabetic range, and receipt of additional antidiabetic therapy. 20 In the PALISADE trial, an increased glycated hemoglobin level occurred in 3 patients in each plozasiran group and in no patients in the placebo group. The mean increase in hemoglobin A1c from baseline was 0.3% for the 25 mg group. Treatment emergent adverse events indicating worsening of diabetes happened in 23.1% of patients in the 25 mg group vs 8% in the placebo group, with it affecting 1 patient (6.3%) without diabetes at baseline in the 25 mg group. 21 A potential mechanism proposed for the hyperglycemia observed with plozasiran use is an increase in hepatic gluconeogenesis due to TG hydrolysis and a subsequent increase in lipid substrates delivered to the liver. 21
In patients with persistent chylomicronemia, plozasiran treatment was associated with a nonprogressive mean increase in ALT and AST, with at least 1 ALT value surpassing the upper limit of normal in 23% of patients in the 25 mg group and in 46% of patients in the 50 mg group vs 4% of those in the placebo group. 21 However, there were no increases more than 3 times the upper limit of normal. The AST and ALT were also monitored in the MUIR and SHASTA-2 trials but no significant changes were reported.17,20
Increases in LDL-C were also seen in 2 of the 3 trials. In the SHASTA-2 trial, in those receiving the plozasiran 25 mg, the placebo-adjusted increase in LDL-C was 25.8%, but there were no accompanied changes in ApoB. 17 In the PALISADE trial, the placebo group had mean LDL-C increase from 28.4 mg/dL at baseline to 35.7 mg/dL vs an increase from 23.8 mg/dL at baseline to 49.0 mg/dL in the plozasiran 25 mg group at month 12. 21 This was also accompanied by a change in ApoB with a mean ApoB increase from 78.9 mg/dL at baseline to 85.5 mg/dL in the placebo group vs an increase from 72.5 mg/dL at baseline to 90.6 mg/dL in the plozasiran 25 mg group at month 12. However, ApoB levels generally remained within normal range.17,21
Of note, thrombocytopenia, which was observed with volanesorsen use, was not a concern in any of the included trials that evaluated plozasiran.17,20,21
Cost
The average wholesale price of plozasiran is $18 000 per 25 mg prefilled syringe, which equates to approximately $72 000/year for treatment of MCS. Currently, plozasiran is only available to patients via a single specialty pharmacy, Vanscoy Rare Pharmacy. The Rely on Redemplo copay card program is a financial assistance program available through the drug manufacturer that provides financial assistance to commercially insured patients who qualify. 28 (https://redemplohcp.com/access-and-support#support-services)
Relevance to Patient Care and Clinical Practice in Comparison to Existing Drugs
FCS has historically had limited treatment options outside of lifestyle management with dietary restriction of fat intake and physical activity.1,2 The advent of volanesorsen and olezarsen have been exciting new options to reduce TGs in patients with FCS. Major limitations with volanesorsen use include the risk of profound thrombocytopenia and that it is not approved for use in the United States.
Olezarsen is another option for FCS management but requires more frequent administration than plozasiran (monthly vs every 3 months). As noted in the pharmacology section, plozasiran’s less frequent administration is likely due to it being siRNA therapy vs olezarsen being an ASO. Only needing 4 doses/year of plozasiran vs 12 doses/year of olezarsen may help patients with adherence.15,29 Plozasiran would be estimated to cost about $72 000/year based on its wholesale price ($18 000/dose). Olezarsen was previously estimated to cost ~$600 000/year, but as of April 1, 2026, Ionis lowered the annual wholesale cost to $40 000/year.30,31 Cost will be a key factor in patients and providers deciding between these 2 agents as the cost difference is approximately $32 000/year.
Plozasiran is the first FDA-approved siRNA for FCS in adult patients. The TG reduction and decreased acute pancreatitis events with plozasiran use observed in studies will allow patients to better manage their FCS and provides another option for therapy in addition to olezarsen. It is important to highlight that of the studies reviewed, SHASTA-2 excluded patients with FCS and the MUIR trial included patients with TGs between 150 and 499 mg/dL (unlikely to have included patients with FCS). It is also paramount to highlight that only 44 (59%) of the 75 patients in the PALISADE trial had genetically confirmed FCS and the other 31 patients had persistent chylomicronemia, but did not have genetically confirmed FCS. 21 This is important to juxtaposition with the BALANCE trial, where olezarsen was evaluated in patients who had genetically confirmed FCS. 11 This also may be a potential factor clinicians consider when choosing between these 2 agents. While the TG lowering with plozasiran is promising, additional data in patients with FCS and long-term outcomes are still needed.
Conclusion
Plozasiran is a novel, siRNA medication that offers an additional pharmacological treatment option for management of FCS. This medication significantly reduces TG levels and may help with patient adherence as it only requires a total of 4 doses/year, though its higher cost compared to olezarsen may be a limitation for use. The availability of this medication has the potential to significantly and positively impact the quality of life and outcomes in patients with FCS. Additional studies are needed to assess the long-term impact of plozasiran.
Footnotes
Ethical Considerations
This article does not contain any studies with human or animal participants.
Consent to Participate
This article does not contain any studies with human participants.
Author Contributions
Ellen Yin contributed to writing—review and editing, writing—original draft, visualization, and conceptualization. Matthew A. Wanat contributed to writing—review and editing and writing—original draft. Elisabeth M. Wang contributed to writing—review and editing, writing—original draft, visualization, supervision, and conceptualization.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.