
Abstract
Background:
Intravenous (IV) iron supplementation is an important strategy for correcting iron deficiency in patients with heart failure with reduced ejection fraction (HFrEF). Despite guideline recommendations, real-world implementation remains inconsistent.
Objective:
This study aimed to evaluate the real-world impact of IV iron therapy on clinical outcomes in patients with HFrEF and iron deficiency.
Methods:
This retrospective cohort study included adult patients with HFrEF and iron deficiency, who were admitted between January 2022 and May 2024 and received IV iron during hospitalization. Clinical outcomes included all-cause mortality and rehospitalization within 12 months of discharge and were analyzed using Kaplan-Meier survival curves. Changes in laboratory values from baseline to 12 months were compared using paired t-tests or Wilcoxon signed-rank tests.
Results:
Among 124 patients, death or rehospitalization occurred in 81 (65%), including 14 (11%) deaths, and among 119 discharged alive, 75 (63%) were rehospitalized within 12 months. Mean hemoglobin increased by 1.1 g/dL (95% confidence interval [CI] = 0.5 to 1.7; n = 46), median ferritin by 44 ng/mL (interquartile range [IQR] = 8.4-372; n = 23), transferrin saturation by 4% (IQR = 0-13; n = 22), and left ventricular ejection fraction (LVEF) by 3% (95% CI = −2 to 7; n = 33).
Conclusion and Relevance:
Among patients with HFrEF and iron deficiency who received IV iron during hospitalization, improvements in anemia and iron parameters and modest increases in LVEF were observed, while rehospitalization remained common. Real-world practice was characterized by lower cumulative dosing and barriers to outpatient continuation of IV iron therapy, which may have attenuated clinical benefit. Further research should define optimal dosing, improve outpatient delivery, and clarify the role of oral iron when IV iron is unavailable or not tolerated.
Keywords
Background
Heart failure (HF) remains a leading cause of morbidity and mortality worldwide, and its prevalence continues to rise, particularly among older patients, placing a substantial burden on patients and health care systems.1,2 Among patients with heart failure with reduced ejection fraction (HFrEF), defined as a left ventricular ejection fraction (LVEF) of ≤40%, iron deficiency is a common and clinically significant comorbidity, affecting up to 50% of this population. 3 Iron deficiency may result from insufficient intake, impaired gastrointestinal absorption, or increased losses and is more prevalent in individuals of advanced age, females, those with kidney disease, and those with more severe HF. 4 Iron deficiency, even in the absence of anemia, is associated with worsening HF symptoms such as fatigue, reduced exercise capacity, impaired functional status, and decreased quality of life, contributing to increased morbidity and mortality. 5
Intravenous (IV) iron supplementation has emerged as an important therapeutic strategy for correcting iron deficiency in patients with HFrEF. Previous randomized controlled trials demonstrated that IV iron therapy improved patient-reported outcomes, exercise capacity, quality of life, and HF-related hospitalizations.6-10 Accordingly, current European Society of Cardiology (ESC) guidelines for the diagnosis and treatment of acute and chronic HF, as well as the American College of Cardiology (ACC)/American Heart Association (AHA)/Heart Failure Society of America (HFSA) guideline for the management of HF, recommend IV iron supplementation for patients with HFrEF and iron deficiency with or without anemia.11-13
Despite these guideline recommendations, real-world implementation of IV iron therapy remains inconsistent, partly due to variability in study designs, iron formulations, and dosing strategies, as well as limited data on clinical outcomes in routine practice. To optimize the management of iron deficiency in patients with HFrEF, evaluation of IV iron use and associated outcomes, including hospital readmissions or mortality, in routine clinical practice is needed. Therefore, this study aimed to evaluate the real-world impact of IV iron therapy on clinical outcomes in patients with HFrEF and iron deficiency, with a focus on hospital readmissions and mortality. We hypothesized that administration of IV iron prior to hospital discharge would be associated with reduced rehospitalization and mortality in this population, given that improvements in functional status and reductions in heart failure–related decompensation may contribute to potential downstream mortality benefit.
Methods
Study Design and Setting
This retrospective observational cohort study included adult patients with HFrEF and iron deficiency, with or without anemia, who were admitted to an academic medical center or affiliated community hospitals between January 1, 2022, and May 31, 2024, and received IV iron during hospitalization. The diagnosis of HFrEF was confirmed with an LVEF of ≤40%, and iron deficiency was defined as ferritin <100 ng/mL, or ferritin 100 to 299 ng/mL with transferrin saturation < 20% prior to IV iron administration. 11 Patients were excluded if they received a blood transfusion within 1 month prior to admission, had hematologic disorders such as hemochromatosis, hemophilia, or hematologic malignancy, or had documented iron overload during hospitalization. Baseline heart failure status was classified according to the ACC/AHA stage and the New York Heart Association (NYHA) functional class, based on documentation in the electronic health record. 11 This study was approved by the health system’s institutional review board with a waiver of informed consent. This article adhered to the Strengthening the Reporting of OBservational studies in Epidemiology (STROBE) reporting guidelines. 14
Outcomes
The clinical outcomes were all-cause mortality and all-cause rehospitalization within 12 months of hospital discharge. Surrogate outcomes included changes in hemoglobin, ferritin, transferrin saturation, and LVEF, as well as the number of patients who received oral iron therapy. Changes in laboratory values were calculated between baseline, defined as the measurement obtained prior to and closest to IV iron administration, and 12 months. All outcomes were assessed at baseline, at hospital discharge, and at 3, 6, and 12 months after hospital discharge.
Data Analysis
Data were summarized using descriptive statistics. Continuous variables were reported as mean ± standard deviation (SD) or median (interquartile range [IQR]), as appropriate based on distribution. Cumulative incidence of clinical outcomes was analyzed using Kaplan-Meier survival curves. Clinical outcomes were also compared between patients who did and did not receive oral iron therapy after discharge using chi-square test. Changes in laboratory values between baseline and 12 months were compared using paired t-tests or Wilcoxon signed-rank tests, as appropriate. All analyses were conducted using Stata version 19.5 (StataCorp LLC, College Station, TX, USA).
Results
Baseline Characteristics
Among 163 patients who met the inclusion criteria, 39 were excluded due to receipt of a blood transfusion within 1 month prior to admission, resulting in 124 patients included in the analysis. Most patients (n = 90, 73%) were admitted for heart failure–related causes. The cohort had a high burden of comorbidities, most frequently hypertension (n = 82, 66%) and other cardiovascular diseases (n = 69, 56%), including pulmonary hypertension, myocardial infarction, or coronary artery disease (Table 1). Among patients with chronic kidney disease, 11 (9%) were receiving kidney replacement therapy. At baseline, although most patients were classified as ACC/AHA Stage C (Symptomatic HF) or D (Advanced HF), only 5 (4%) patients were receiving all 4 guideline-directed medical therapy classes prior to hospitalization, and 8 (6%) were receiving them at the time of IV iron administration.
Baseline Characteristics.
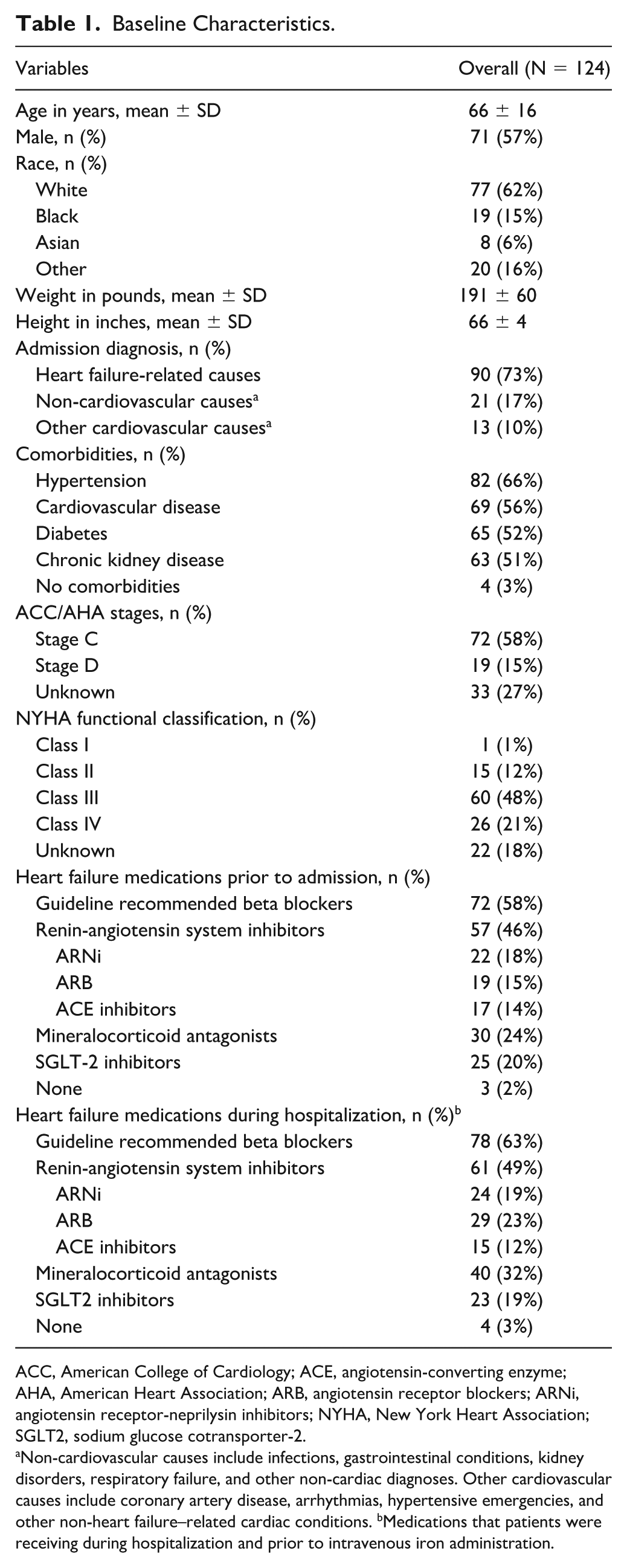
ACC, American College of Cardiology; ACE, angiotensin-converting enzyme; AHA, American Heart Association; ARB, angiotensin receptor blockers; ARNi, angiotensin receptor-neprilysin inhibitors; NYHA, New York Heart Association; SGLT2, sodium glucose cotransporter-2.
Non-cardiovascular causes include infections, gastrointestinal conditions, kidney disorders, respiratory failure, and other non-cardiac diagnoses. Other cardiovascular causes include coronary artery disease, arrhythmias, hypertensive emergencies, and other non-heart failure–related cardiac conditions. bMedications that patients were receiving during hospitalization and prior to intravenous iron administration.
Iron Therapy During Hospitalization
During hospitalization, 74 patients (60%) received iron sucrose, 50 (40%) received ferric gluconate, and none received iron dextran. The mean total IV iron dose was 554 ± 306 mg overall; specifically, the mean total dose of iron sucrose was 521 ± 270 mg and ferric gluconate was 602 ± 349 mg. A subset of patients required repeat IV iron therapy after discharge. At 3 months, 6 of 119 patients (5%) required repeat therapy with a mean total dose of 563 ± 360 mg. At 6 months, 1 of 116 patients (1%) received 324 mg. At 12 months, 4 of 114 patients (4%) required repeat therapy with a mean total dose of 538 ± 403 mg, and the mean cumulative dose within 1 year was 601 ± 343 mg. The median time to first post-discharge IV iron administration was 33 days (IQR = 7-205). No adverse events were reported after IV iron administration.
Clinical Outcomes
Among 124 patients, either death or rehospitalization occurred in 81 patients (65%) (Figure 1). A total of 14 patients (11%) died between the first IV iron administration and within 12 months of discharge, including 5 (4%) in-hospital deaths (Table 2). The median time from IV iron administration to death was 74 (IQR = 6-256) days. Among 119 patients who were discharged alive, 75 patients (63%) had ≥1 rehospitalization within 12 months of discharge, accounting for a total of 240 rehospitalization events. The median time from IV iron administration to rehospitalization within 12 months of discharge was 63 (IQR = 29-151) days.
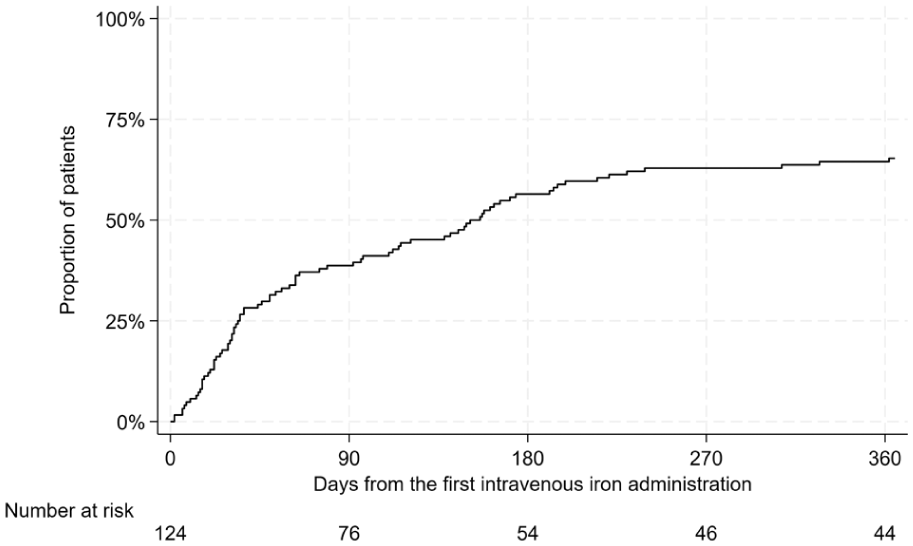
Cumulative incidence of death or rehospitalization within 12 months after discharge following first IV iron administration.
Clinical Outcomes Over 12 Months Following IV Iron Administration.
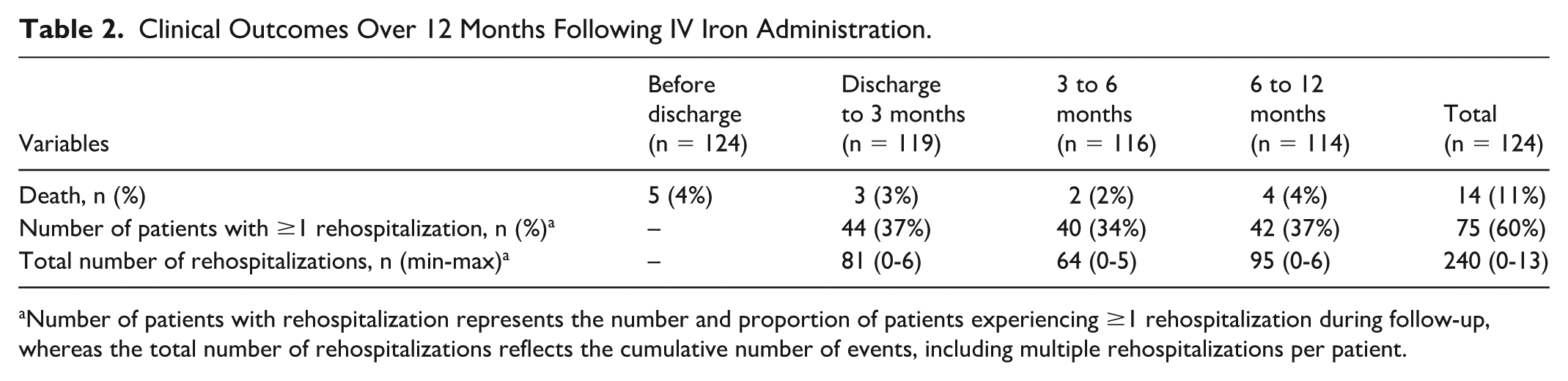
Number of patients with rehospitalization represents the number and proportion of patients experiencing ≥1 rehospitalization during follow-up, whereas the total number of rehospitalizations reflects the cumulative number of events, including multiple rehospitalizations per patient.
Surrogate Outcomes
At baseline, anemia was present in 52 of 53 females (hemoglobin <12 g/dL) and 70 of 71 males (hemoglobin <13 g/dL). Paired comparisons between baseline and 12 months showed that mean hemoglobin increased by 1.1 g/dL (95% confidence interval [CI] = 0.5 to 1.7; P = 0.0009; n = 46), median ferritin increased by 44 ng/mL (IQR = 8.4, 372; P = 0.0002; n = 23), median transferrin saturation increased by 4% (IQR = 0-13; P = 0.004; n = 22), and LVEF increased by 3% (95% CI = −2 to 7; P = 0.2461; n = 33) (Figure 2). The decreasing sample size over time reflects loss to follow-up and incomplete availability of laboratory and echocardiographic data in routine clinical practice.
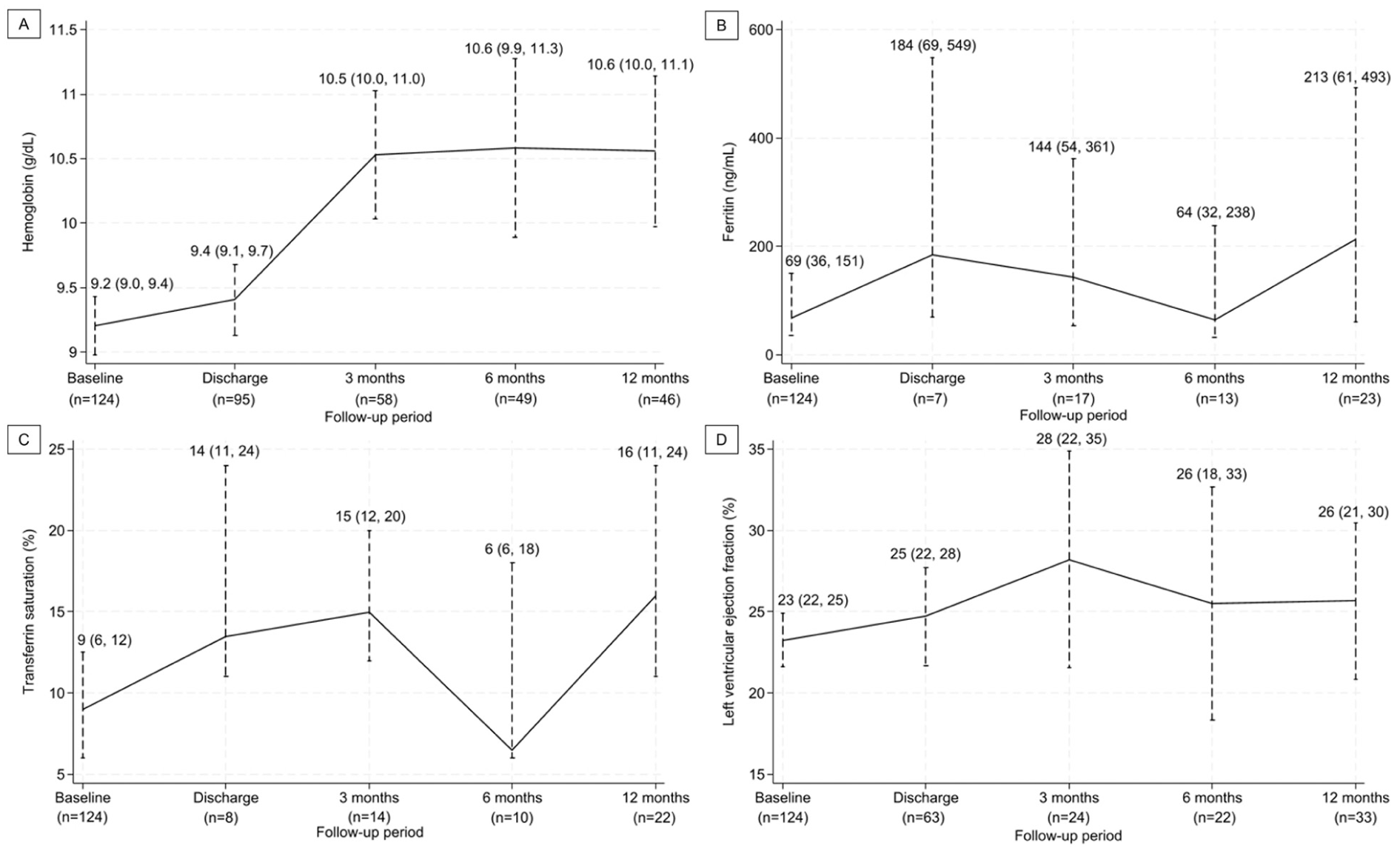
Changes in hemoglobin, iron status, and cardiac function over 12 months after IV iron administration. Temporal trends in hemoglobin (a), ferritin (b), transferrin saturation (c), and left ventricular ejection fraction (d) following IV iron administration.
Subgroup of Patients Received Oral Iron Therapy
In addition to IV iron therapy, oral iron therapy, exclusively as ferrous sulfate 324/325 mg (65 mg elemental iron), was administered to 12 patients (10%) prior to hospitalization, 16 (13%) during hospitalization, and 28 patients (23%) after discharge. Among patients who received oral iron therapy after discharge, death or rehospitalization occurred in 23 of 28 patients (82%), compared with 58 of 96 patients (60%) who did not receive oral iron therapy (P = 0.034). Among these patients, mean hemoglobin increased by 1.3 ± 1.9 g/dL (n = 17), median ferritin increased by 152 ng/mL (IQR = 24-292; n = 8), median transferrin saturation increased by 4% (IQR = 0-19; n = 8), and mean LVEF increased by 2 ± 13% (n = 10).
Discussion
This study evaluated the use of IV iron therapy during hospitalization in patients with HFrEF and iron deficiency, with or without anemia. Complementing prior randomized trials, this study uniquely captures real-world inpatient use of IV iron across varied formulations and dosing strategies. These findings provide important insight into how iron supplementation is administered and its potential impact on routine hospital practice.
The baseline characteristics of our cohort showed a high burden of comorbidities, with most patients presenting in ACC/AHA Stage C and NYHA Class III heart failure. Although this study did not restrict inclusion to patients with anemia, 98% were anemic at baseline, and iron replacement was administered exclusively using iron sucrose or ferric gluconate. The selection of IV iron products reflected our academic institution’s formulary, where ferric carboxymaltose (FCM) was not available, unlike prior clinical trials evaluating IV iron use in patients with heart failure.6-9,15 The mean inpatient IV iron dose in our study was 554 mg, and the mean cumulative dose within 1 year was 600 mg, which was lower than doses reported in prior studies using FCM, which ranged from 1352 to 2040 mg within 1 year. This study demonstrated that inpatient IV iron dosing in routine practice differed from regimens used in previous trials that established its efficacy in this population. Despite access to IV iron during hospitalization, patients often received lower cumulative doses than those used in clinical trials. This may be due to deferral of IV iron administration during hospitalization because of other clinical factors such as active infection or shorter length of stay, which may limit cumulative dosing. Furthermore, therapy was rarely continued after discharge, potentially resulting in suboptimal iron repletion and diminished clinical benefit. This may reflect real-world barriers to optimal dosing, including limited access to outpatient infusion services, cost and insurance constraints, variability in provider familiarity, and challenges in coordinating follow-up care.
While mortality was comparatively low overall, with a total of 14 deaths (11%) including 5 in-hospital deaths, rehospitalization occurred in 75 patients (60%), accounting for 240 rehospitalizations within 1 year of hospital discharge. This was higher than that reported in a previous trial of hospitalized patients, in which a total of 217 heart failure hospitalizations occurred within 1 year. 9 This difference may be partially explained by the inclusion of all-cause rehospitalizations in the present study, whereas prior trials have typically reported heart failure–specific hospitalizations.
Surrogate outcomes demonstrated statistically significant improvements in hemoglobin, ferritin, and transferrin saturation at 12 months after discharge. In this study, mean hemoglobin increased by 1.1 g/dL at 12 months, comparable to increases of approximately 0.7 to 1.0 g/dL reported in previous trials over 6 to 12 months.6,7 In contrast, median ferritin increased by 44 ng/mL at 12 months, whereas previous trials reported a mean increase of approximately 250 to 400 ng/mL, and transferrin saturation increased by a median of 4%, compared with a mean increase of approximately 11% to 12%.6,7 Overall, this study showed a smaller magnitude of improvement in iron parameters compared with prior trials. However, the reduction in sample size over time may limit the interpretation of these longitudinal findings.
Subgroup analysis of patients who received both IV and oral iron therapy showed no difference in the incidence of clinical outcomes compared to patients who did not receive oral iron therapy. This result was consistent with a previous trial evaluating the oral iron therapy, which found no reduction in hospitalizations or improvement in functional capacity despite increases in iron stores. 16 These findings support IV administration as the preferred therapeutic approach while also highlighting persistent unmet needs in reducing clinical relapse.
Several limitations must be acknowledged. First, due to the retrospective design, this study relied on secondary use of clinical documentation, which may be incomplete, inaccurate, or missing key information. Follow-up laboratory measurements were often unavailable, resulting in a smaller subset of patients eligible for paired pre- and post-IV iron analyses. This may introduce selection bias, as patients with available follow-up data may differ from those without, thereby limiting the interpretation of longitudinal changes. In addition, exposure to oral iron therapy was determined from medication orders in the medical record; adherence could not be assessed. Second, the retrospective and descriptive nature of the analysis precludes causal inference regarding clinical outcomes. Finally, as this study reflects practice within a single health system, generalizability may be limited, particularly where local formulary restrictions and practice patterns differ.
Conclusion and Relevance
Among patients with HFrEF and iron deficiency who received IV iron during hospitalization, improvements in anemia and iron parameters, along with modest increases in LVEF, were observed over 12 months; however, rehospitalization remained common during 1-year follow-up. Real-world practice was characterized by lower cumulative iron doses, variability in dosing strategies, and barriers to continuation of IV iron therapy in the outpatient setting. These factors may have attenuated clinical benefit. Additional oral iron therapy after discharge did not show improvement in outcomes; however, this observation was limited by the small sample size and possible non-adherence. Further research is needed to define optimal IV iron dosing strategies, address logistical and access barriers to outpatient IV iron delivery, and clarify the role of oral iron when IV iron is unavailable or not tolerated.
Footnotes
Ethical Considerations
This study was approved by the health system’s institutional review board with a waiver of informed consent.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on request.