
Abstract

To the Editor:
The pharmacokinetics of many drugs while using extracorporeal membrane oxygenation (ECMO) are poorly understood. Several factors may lead to suboptimal medication exposure, such as ECMO tubing, oxygenator, priming fluid, drug lipophilicity, and drug protein binding, which directly impact drug sequestration and elimination.1,2 There have been previous attempts to characterize the degree of drug loss in ECMO circuits for some medications, particularly analgesics, sedatives, and antimicrobial agents. 3 Fentanyl is a commonly used lipophilic drug with a large volume of distribution (3.2-5.6 L/kg) and high protein binding. 4 Fentanyl has been shown to undergo drug loss in simulation ECMO circuits, 5 but there are currently no in vivo studies describing the magnitude of sequestration. Retrospective analyses of patients on ECMO have found that patients receiving fentanyl infusions require greater morphine milligram equivalents than those receiving hydromorphone, which may allude to the clinical impact of fentanyl sequestration.6,7 We sought to determine the effects of ECMO on fentanyl concentration in human blood samples.
In five participants, we measured fentanyl levels 30 minutes prior to veno-venous ECMO initiation, immediately after ECMO initiation, then 15, 30, and 60 minutes after ECMO initiation. All participants were placed on a CardioHelp ECMO system (HLS 7.0 oxygenator) (Getinge, Sweden). The average age was 48.5 ± 23.3 years, with an average body mass index (BMI) of 29.4 ± 3.7 kg/m2. One participant had renal dysfunction (CrCL < 60 mL/min), and none had liver dysfunction. All participants were on continuous intravenous fentanyl infusions at stable rates (ranging 125-200 mcg/hr) for over 30 hours prior to and throughout the study period. Participants did not receive additional fentanyl boluses at any point during the study period apart from participant 1 who received 25 mcg IV once immediately after cannulation. We performed a Kruskal-Wallis test and found no statistical difference (P = 0.68) between any of the 5 time points (see Figure 1).
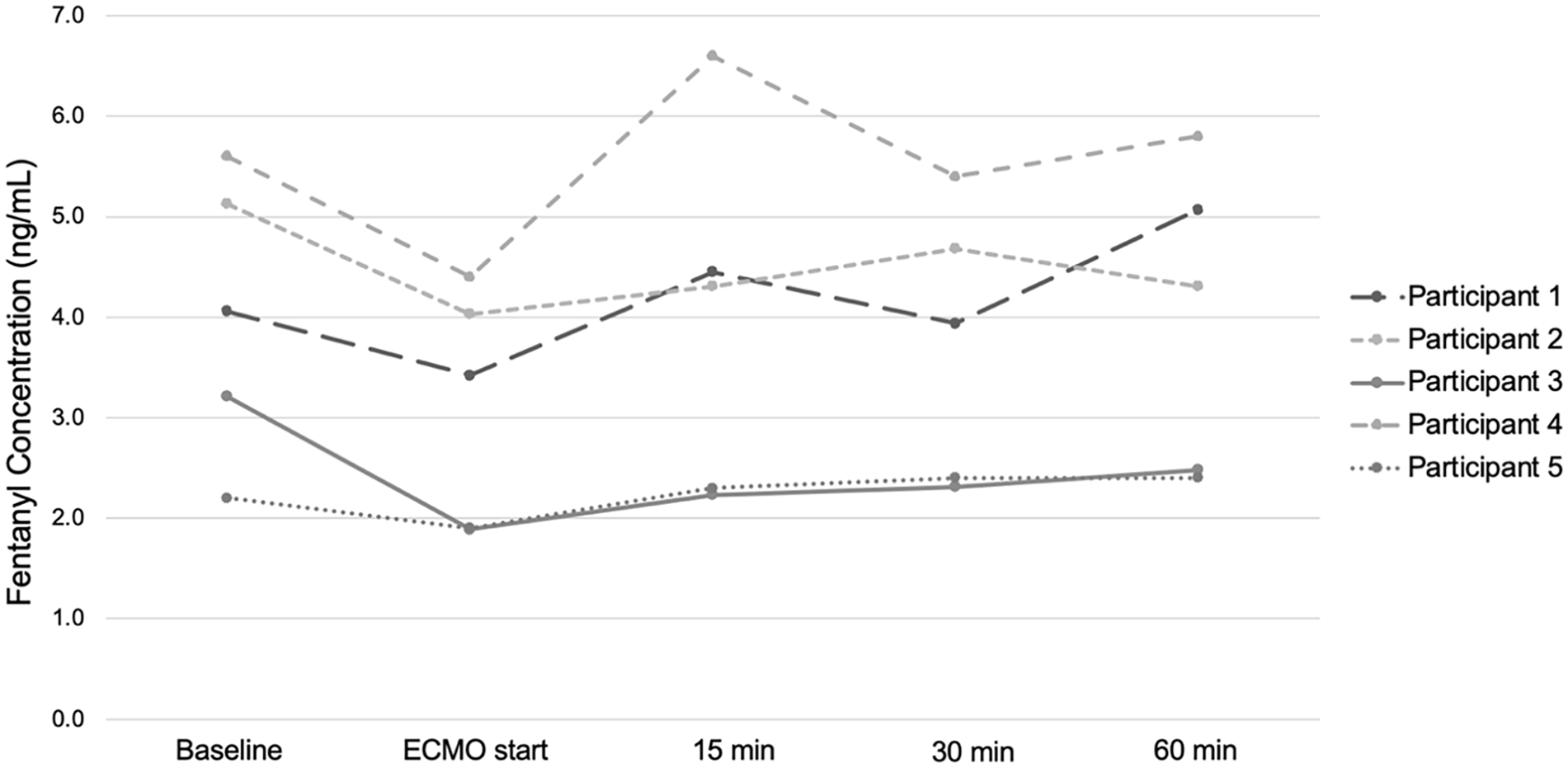
Fentanyl concentrations prior to ECMO initiation, then immediately, 15 minutes, 30 minutes, and 60 minutes after cannulation.
Our small case series suggests there are no significant changes in fentanyl concentrations at 60 minutes after ECMO initiation. While there appears to be an initial decrease in drug concentration, likely due to the increase in volume of distribution as the extracorporeal circuit is added to the patient’s circulation, drug concentrations recover within 15 to 30 minutes after ECMO initiation (Figure 1). It is possible that fentanyl levels could vary in other circuits with different oxygenators as their surface area and drug binding may differ, although all now utilize polymethylpentene hollow fiber oxygenators. While this is a small case series evaluating fentanyl levels over a short duration, there are few data on the in vivo changes of fentanyl in adult patients placed on ECMO and it would not have been clinically feasible to continue fixed fentanyl rates in dynamic patients requiring constant reassessment of therapy. Larger studies may further characterize the pharmacokinetics of intravenous fentanyl in patients on ECMO over longer periods of time, and further research on other analgesics and sedatives are necessary to elucidate the impact of ECMO on circulating drug concentrations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the National Institutes of Health, Grant 2UL1TR001442-06 of CTSA. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.