
Abstract
Background:
Stenotrophomonas maltophilia is a multidrug-resistant organism with limited antibiotic treatment options. Minocycline and doxycycline may be appropriate, but clinical data are limited.
Objective:
To compare tetracyclines (minocycline and doxycycline [TCN]) with standard of care, sulfamethoxazole-trimethoprim (TMP-SMZ), in S. maltophilia pneumonia treatment.
Methods:
This retrospective, 2-center study evaluated patients treated for S. maltophilia pneumonia with TCN or TMP-SMZ for clinical success, defined as resolution of leukocytosis, fever, and tachypnea. Patients were classified as treatment with TCN or TMP-SMZ based on definitive agent used for ≥50% of the treatment course and ≥4 days. Inclusion criteria were age ≥18 years, S. maltophilia confirmed on respiratory culture from January 2013 to November 2020, and appropriate definitive antibiotic dosing. Pregnancy, incarceration, S. maltophilia–resistant or intermediate to definitive therapy, and combination therapy for treatment of S. maltophilia pneumonia were exclusion criteria. Secondary outcomes were microbiologic success and recurrence or reinfection within 30 days requiring treatment.
Results:
A total of 80 patients were included (21 TCN [15 minocycline, 6 doxycycline], 59 TMP-SMZ). There was no difference in clinical success (28.6% vs 25.4%; P = 0.994), microbiologic success (n = 28, 55.6% vs 66.4%; P = 0.677), or recurrence or reinfection (n = 24, 66.7% vs 26.7%; P = 0.092) between TCN and TMP-SMZ, respectively.
Conclusion and Relevance:
Clinical and microbiologic success rates were similar in patients treated with TCN compared with TMP-SMZ for S. maltophilia pneumonia. These data suggest minocycline and doxycycline may be options to treat S. maltophilia pneumonia, but conclusive clinical data continue to be lacking.
Introduction
Stenotrophomonas maltophilia is an opportunistic, aerobic, gram-negative bacillus associated with monomicrobial and polymicrobial infections, including pneumonia, bacteremia, and central venous catheter–related infections.1-3 It is a multidrug-resistant organism (MDRO) intrinsically resistant to several antibiotic classes including β-lactams through the production of extended-spectrum β-lactamases (ESBLs), zinc-dependent metallo β-lactamase, efflux pumps, and decreased permeability of antibiotics into the cell. Collectively, these varied mechanisms of resistance result in limited antibiotic treatment options. 4 Sulfamethoxazole-trimethoprim (TMP-SMZ) is considered the treatment of choice based on clinical experience and in vitro studies that demonstrated high susceptibility of S. maltophilia to TMP-SMZ. 5
Emergence of bacterial resistance to TMP-SMZ and patient allergy to sulfa moieties have prompted exploration of alternative agents such as levofloxacin, minocycline, and ceftazidime for definitive management of S. maltophilia infection.5,6 Fluroquinolones have been shown to have clinical utility for S. maltophilia in retrospective studies, but exposure is associated with increased resistance due to a combination of Smqnr genes and overexpression of efflux pumps during therapy.7-9 Ceftazidime has been used for S. maltophilia treatment, but the Infectious Diseases Society of America (IDSA) guidance on the treatment of Antimicrobial-Resistant Gram-Negative Infections suggests against use because of inducible metallo β-lactamase and concern for lower cure rates.9,10 Tetracyclines (TCN) demonstrate reliable in vitro activity against S. maltophilia, particularly minocycline and doxycycline. Clinical data for minocycline are limited to retrospective studies and case reports, and a single case report describes doxycycline treatment in combination with colistin.10-14 However, TCN can play a significant role in S. maltophilia pneumonia given increasing resistance and intolerances to other agents. The purpose of this study is to compare S. maltophilia pneumonia treatment success with TCN (doxycycline or minocycline) compared with TMP-SMZ.
Methods
This retrospective, multicenter, single health system study included hospitalized adult patients aged ≥18 years admitted to UC Health acute care hospitals—University of Cincinnati Medical Center (UCMC) and West Chester Hospital—from January 2013 to November 2020. All patients were treated for culture-positive S. maltophilia pneumonia with a tetracycline (minocycline or doxycycline) or TMP-SMZ. Institutional Review Board approval was obtained.
An electronic medical record report identified patients with a respiratory culture (sputum, bronchiolar alveolar lavage, or tracheal aspirate) positive for S. maltophilia and concomitant medication order for minocycline, doxycycline, or TMP-SMZ within 2 days prior to or 7 days after respiratory culture. Patients were classified into TCN or TMP-SMZ treatment groups based on the definitive agent used for ≥50% of the overall antibiotic treatment course and administered for at least 4 days. For TMP-SMZ patients, only the first documented S. maltophilia pneumonia culture within UC Health system was included. Pregnant patients, prisoners, those who underwent S. maltophilia–resistant or intermediate to definitive therapy, those who underwent treatment with combination therapy, and those who received inappropriate TMP-SMZ dosing (eg, < 15 mg/kg/day for patients with creatinine clearance >30 mL/min) based on institutional guideline for S. maltophilia were excluded (Table 1).
Baseline Characteristics.
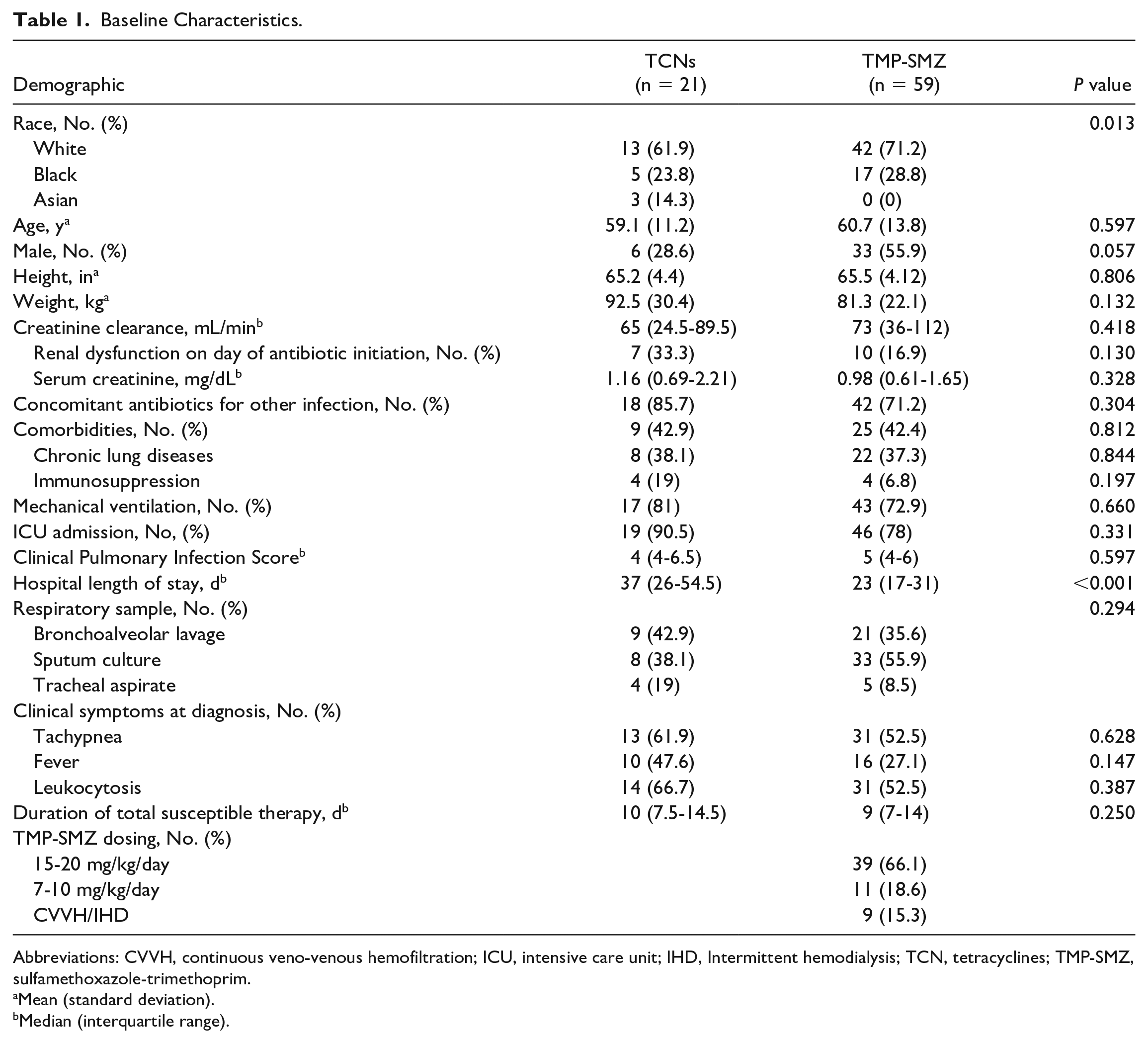
Abbreviations: CVVH, continuous veno-venous hemofiltration; ICU, intensive care unit; IHD, Intermittent hemodialysis; TCN, tetracyclines; TMP-SMZ, sulfamethoxazole-trimethoprim.
Mean (standard deviation).
Median (interquartile range).
The primary outcome was the rate of clinical success between TCN and TMP-SMZ groups. Clinical success was defined as a composite resolution of leukocytosis (white blood cell ≤12 × 109/L or ≥50% reduction from day of culture), tachypnea (≤1 episode of respiratory rate ≤22 breaths per minute within 24 hours), and fever (temperature ≤100.4 °F) within 48 hours of definitive treatment completion. Secondary outcomes included microbiologic success and incidence of infection recurrence or reinfection requiring treatment within 30 days of the original culture. Microbiologic success was defined as documented clearance of S. maltophilia from culture or 1-grade reduction in S. maltophilia colony-forming units in a lab-calibrated loop within 48 hours of treatment completion. Additional secondary outcomes compared doxycycline with minocycline for clinical success in the treatment of S. maltophilia with susceptible minocycline minimum inhibitory concentration (MIC) and identified independent factors for clinical success. A subgroup analysis was performed to compare doxycycline, minocycline, and TMP-SMZ for clinical success, microbiologic success, and reinfection or recurrence.
A convenience sample was used for patients treated with TCN due to the pilot nature of this study and based on previous data. 11 Sulfamethoxazole-trimethoprim patients were screened for candidacy, and then enrollment was prioritized to enroll more TMP-SMZ patients than TCN patients in an intended ratio of 2-3:1. A random number generator was used to guide TMP-SMZ patient inclusion. Categorical data were assessed with χ2 or Fisher exact test, and continuous data were analyzed with Student t test or Wilcoxon rank sum, as appropriate. For the clinical success factor analysis, a univariate analysis compared independent variables between patients with and without clinical success (dependent variable). Variables with a P value <0.2 were included in a multivariate logistic regression analysis (MVLR). Antibiotic selection was included a priori in the model. SigmaPlot version 14 (Systat Software, San Jose, California) was used for statistical analysis.
Results
A total of 80 patients were included, with 21 patients in the TCN group (doxycycline n = 6, minocycline, n = 15) and 59 patients in the TMP-SMZ group. Patients were similar in age, height, weight, creatinine clearance, concomitant antibiotics for other infections, comorbidities including chronic lung diseases and immunosuppression, mechanical ventilation, intensive care unit (ICU) admission, Clinical Pulmonary Infection Score, type of pulmonary culture, clinical symptoms at diagnosis, and duration of total susceptible therapy. Sulfamethoxazole-trimethoprim patients were more likely to be white, men, and have a shorter hospital length of stay (Table 1). Sulfamethoxazole-trimethoprim dosing was appropriate per institutional guidance based on renal function in all patients, with most patients receiving 15 to 20 mg/kg/day of trimethoprim (66.1%) and 55.9% of TMP-SMZ patients initiating oral TMP-SMZ. Eleven (52.4%) TCN patients had a previous S. maltophilia respiratory culture in the system within 6 months. Two patients in the TMP-SMZ group (3.4%) had a previous S. maltophilia respiratory culture but no documented treatment. Thirteen (61.9%) patients in the TCN cohort had S. maltophilia cultures that were resistant to TMP-SMZ. There were 18 patients with a reported minocycline MIC of 0.75 (interquartile range [IQR], 0.348-1.625). All 18 isolates were susceptible to minocycline. Definitive therapy was the same as initial therapy for 15 (71.4%) TCN patients compared with 58 (98.3%) TMP-SMZ patients (P = 0.001). Three patients were switched from initial TMP-SMZ therapy to definitive TCN therapy due to resistance to TMP-SMZ on final culture, 2 were switched due to intolerances to TMP-SMZ therapy (hyperkalemia), and 1 patient was switched from doxycycline to minocycline by the treating clinician because of the lack of doxycycline MIC on the tracheal aspirate culture.
No significant difference was found in clinical success between TCN and TMP-SMZ (28.6% vs 25.4%; P = 0.994). Microbiologic success was assessed in 28 patients with no statistically significant difference between groups (55.6% TCN vs 66.4% TMP-SMZ; P = 0.677). Recurrence or reinfection at 30 days was evaluable in 24 patients (TCN, n = 9; TMP-SMZ, n = 15). Six (66.7%) TCN patients compared with 4 (26.7%) TMP-SMZ patients had recurrence or reinfection (P = 0.092) (Table 2). Seventeen TCN patients (minocycline n = 12, doxycycline n = 5) with susceptible minocycline MIC were compared for clinical success. In patients with susceptible minocycline MIC, the rate of clinical success of doxycycline was similar to minocycline in S. maltophilia pneumonia (33.3% vs 20%, P = 1.00). Incidences of clinical success, microbiologic success, and recurrence or reinfection were not different between doxycycline, minocycline, and TMP-SMZ (Table 3).
Clinical Outcomes.
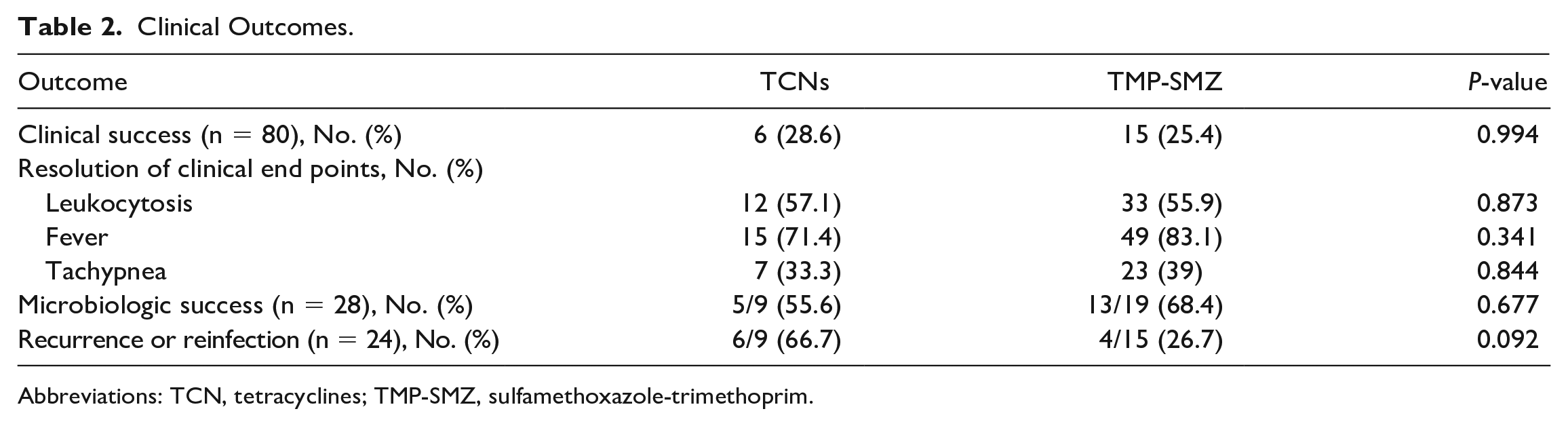
Abbreviations: TCN, tetracyclines; TMP-SMZ, sulfamethoxazole-trimethoprim.
Antibiotic Subgroup Analysis.
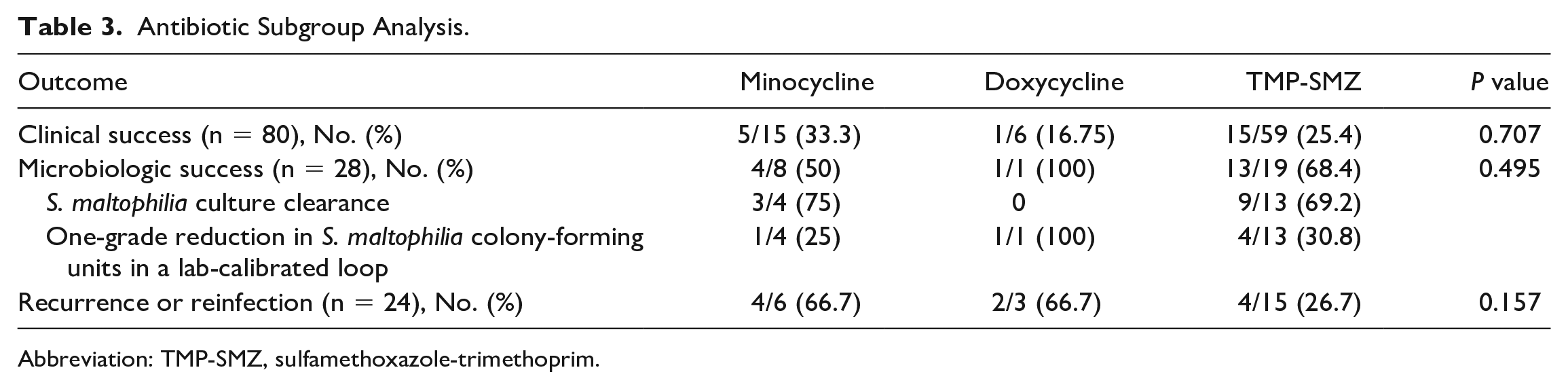
Abbreviation: TMP-SMZ, sulfamethoxazole-trimethoprim.
Univariate analysis identified antibiotic selection, renal dysfunction, mechanical ventilation, ICU admission, and duration of treatment for MVLR inclusion. No risk factors were independently associated with clinical success (Table 4).
Independent Risk Factors for Clinical Success.
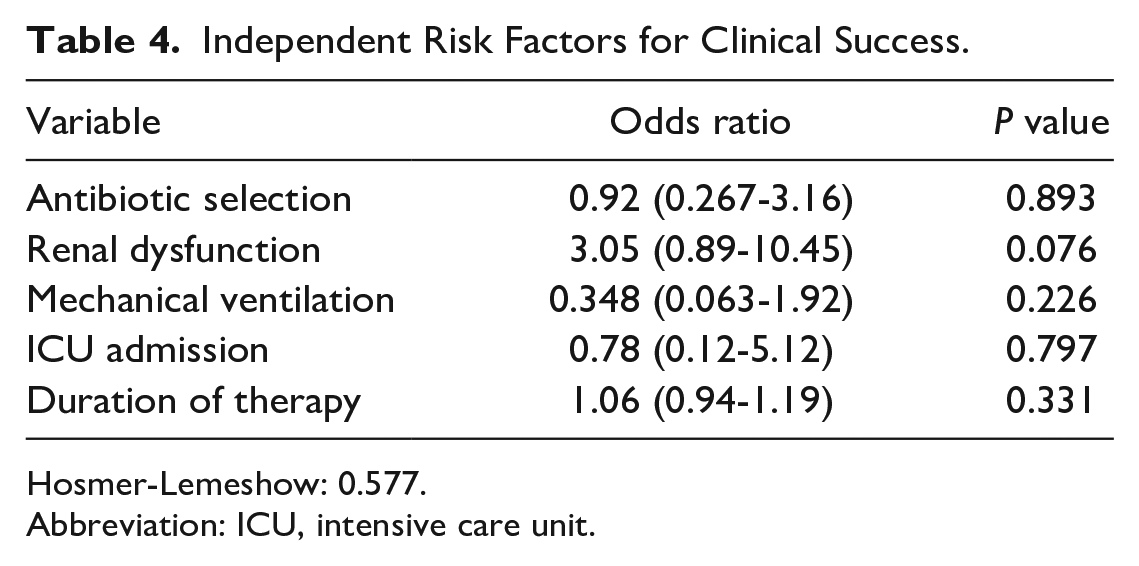
Hosmer-Lemeshow: 0.577.
Abbreviation: ICU, intensive care unit.
Discussion
Stenotrophomonas maltophilia possesses numerous virulence factors that enable resistance to antibiotics and aid in the pathogenesis of colonization, making antibiotic selection challenging. 15 Clinicians continue to face obstacles despite the recent IDSA AMR Guidance 2.0 on the treatment of S. maltophilia infections, due to limited susceptibility data and paucity of robust evidence. Historically, TMP-SMZ has been the agent of choice. AMR Guidance 2.0 suggests the use of TMP-SMZ as monotherapy for mild infections, or combination therapy with other active agents in moderate to severe infections.9 The utilization of TMP-SMZ in practice has been associated with increased resistance and adverse events such as hypersensitivity reactions, hyperkalemia, renal insufficiency and volume overload with the intravenous (IV) formulation.16,17 Agents such as minocycline, doxycycline, and levofloxacin have been utilized more frequently in practice. AMR Guidance 2.0 suggests the use of levofloxacin as monotherapy for mild infections. However, caution should be taken when utilizing levofloaxcin as monotherapy due to development of resistance during treatment and adverse effect profile.7-9 Minocycline and doxycycline have been suggested as alternatives due to their high susceptibility rates and favorable adverse effect profiles.10,18,19 AMR Guidance 2.0 suggests the use of minocycline as monotherapy for mild infections, or combination therapy in moderate to severe infections. Oral or IV high dose minocycline (200 mg twice daily) is suggested over standard dosing. No suggestion was made for doxycycline; however, it has been historically utilized as alternative due to minocycline shortages. Given this information, AMR Guidance 2.0 has suggested TMP-SMZ and minocycline as preferred therapy for S. maltophilia infections. 9 Nonetheless, existing data on clinical outcomes for treatment of S. maltophilia infections with minocycline or doxycycline monotherapy is limited.
This study found no difference in clinical success with TCN (doxycycline or minocycline) compared with appropriately dosed TMP-SMZ for the treatment of S. maltophilia pneumonia. Further analysis demonstrated no difference in microbiologic success and recurrence or reinfection between groups. Hand and colleagues 11 showed similar treatment failure rates with minocycline (30%) and TMP-SMZ (41%). Jacobson and colleagues 12 described a 58% complete clinical success rate with minocycline, but a majority of patients received combination therapy. Junco and colleagues 14 demonstrated similar clinical failure rates between TMP-SMZ (35.5%), fluoroquinolone (28.6%), and minocycline (30.8%). This study compared 21 doxycycline or minocycline patients with 59 patients receiving TMP-SMZ and found no difference in outcomes with similar duration of total susceptible therapy between cohorts.
Clinical success in both groups was lower than other studies describing outcomes with minocycline treatment in S. maltophilia infections, likely due to different definitions of clinical success.11,12,14 Jacobson et al had a clinical success rate of 58% for S. maltophilia treatment with minocycline, defined as survival within 30 days of initial positive culture, no further positive S. maltophilia culture, no receipt of additional antibiotics for S. maltophilia, and no clinical worsening. In Hand et al, minocycline monotherapy had a treatment failure of 30%, but had a primary outcome similar to the study by Jacobson et al.11,12 This study classified clinical success comprehensively as resolution of leukocytosis, fever, and tachypnea. Patients had a 56.2% resolution of leukocytosis, 80% resolution of fever, but only 37.5% resolution of tachypnea. The low rates of tachypnea resolution led to a potential decrease in clinical success rates in both groups. A majority (81%) of patients in this study were admitted to ICU, while 75% were mechanically ventilated which may be indicative of moderate to severe infection. The IDSA AMR Guidance 2.0 suggests combination of TMP-SMZ and minocycline for moderate to severe S. maltophilia infections. However, this study only included patients on monotherapy which may have contributed to lower clinical success rates amongst treatment groups. The AMR Guidance 2.0 were released after the completion of this study. 9 In addition, S. maltophilia can present as a polymicrobial infection which may have led to lower rates of clinical success in both groups. Additionally, hospital length of stay was notably longer than duration of therapy for S. maltophilia. This may be attributed to 75% of patient on concomitant antibiotics for other infections which may have prolonged their ICU and hospital length of stay. The rate of recurrence requiring treatment in the TCN group was higher but not statistically significant compared with TMP-SMZ. This is likely due to TCN patients having a higher incidence of treatment with TMP-SMZ in the past, as well as development of resistance to TMP-SMZ. Three of 6 patients in the TCN group had a previously positive S. maltophilia pneumonia culture compared with no patients in the TMP-SMZ group. In addition, 4 of 6 patients in the TCN cohort had resistant S. maltophilia cultures to TMP-SMZ. Only 2 historic cultures had reported minocycline MIC, and both were susceptible. The higher rates of recurrence are possibly indicative of colonization in the TCN group.
The Clinical Laboratory Standards Institute (CLSI) reports MIC breakpoints for minocycline but not doxycycline, which limits the exploration of doxycycline in S. maltophilia treatment. 20 Doxycycline has not been studied as monotherapy for treatment of S. maltophilia pneumonia, and data for clinical use are sparse. A single case report demonstrated successful use of doxycycline alongside inhaled colistin for a patient who had treatment failure with TMP-SMZ and ciprofloxacin. 13 However, in vitro data support high susceptibility of S. maltophilia to doxycycline, suggesting it is a potentially viable agent.9,17 To our knowledge, this is the first study to explore doxycycline in the treatment of S. maltophilia pneumonia. Six patients received doxycycline monotherapy as the definitive treatment course, and the subgroup analysis for clinical success demonstrated no statistically significant difference between antibiotics. Nonetheless, the doxycycline sample size is small with one patient achieving the primary outcome. Treatment success was assessed in patients receiving doxycycline with susceptible minocycline MIC in the absence of a doxycycline CLSI breakpoint to determine association. Correlation was unable to be identified between doxycycline clinical success and susceptible minocycline MIC due to the low number of patients on doxycycline. More conclusive data are needed to determine the utility of doxycycline in S. maltophilia pneumonia treatment and utility of surrogate minocycline MIC.
This study was limited by its retrospective design and small convenience sample, especially in the TCN group, which may limit extrapolation to clinical practice. Sulfamethoxazole-trimethoprim patients must be receiving their first treatment course for S. maltophilia pneumonia culture; however, patients externally treated for S. maltophilia pneumonia were potentially included. The TCN group included patients with S. maltophilia resistant to TMP-SMZ and/or previously treated with TMP-SMZ, which may indicate more resistant and harder to treat infection or potential colonization in that cohort. Tetracyclines patients had a lengthier hospital stay compared to TMP-SMZ patients which may be associated with higher acuity of care. Tetracyclines patients also had a higher number of patients in the ICU, but it was not statistically significant. AMR Guidance 2.0 suggests high dose minocycline for S. maltophilia. In this study, only 40% of patients on minocycline were initiated on this dose. This potentially may have affected the rates of clinical success in the TCN group. No dosage suggestion has been provided for doxycycline. 9 Additionally, 75% of patients were on a concomitant antibiotic for other infections, potentially confounding assessment of the primary outcome related solely to S. maltophilia treatment. Also, transitioning between parenteral and oral formulations for both groups was not recorded in this study. Nonetheless, sequential parenteral to oral conversion for TCN and TMP-SMZ is commonly practice due to their excellent bioavailability. Although this study had 80 patients, only 28 patients were identified for microbiologic success and 24 for recurrence or reinfection. Five patients in the TCN group were initially started on TMP-SMZ but were later switched to a TCN which was likely prior to return of positive culture results.
Conclusion and Relevance
Increasing resistance and intolerance toward TMP-SMZ has led to the exploration of alternative agents such as minocycline and doxycycline. This study demonstrated similar rates of clinical success with TCN and TMP-SMZ for the treatment of S. maltophilia pneumonia. This study provides additional support for the use of minocycline as a preferred agent alongside TMP-SMZ. However, conclusive data continue to be lacking for doxycycline given the low number of patients and the absence of MIC breakpoints. Although microbiologic success was similar in patients treated with TCN, recurrence/reinfection rates appeared higher but not statistically significant compared with TMP-SMZ in the small subset of evaluable patients. The choice of therapy should be based on microbiological data, clinical presentation, and adverse effect profile of the selected agent. More studies are needed to explore doxycycline as an agent for S. maltophilia pneumonia and other infections.
Footnotes
Authors’ Note
Prior presentation: An abstract was presented at ID Week in September 2021 virtually.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Anthony J. Gentene served on a joint advisory board for Theravance Biopharma US, Inc, and Mylan Specialty LP.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.