
Abstract
Introduction
Older people often have increasingly complex medication regimens. In the United States, the proportion of people ≥65 years old who took 5 or more medications tripled from 12.8% to 39.0% between 1988 and 2010. 1 The number of prescribed medications have also increased in Europe, with the proportion of people ≥65 years old who take 10 or more medications in the United Kingdom also tripling from 4.9% to 17.2% between 1995 and 2010. 2
Clinical practice guidelines increasingly advocate the use of multiple medications to achieve therapeutic targets. 3 This can result in older people having complex medication regimens. Complexity may arise as a result of number of medications, different types of dose forms, and multiple daily dosing. Complex medication regimens may lead to errors with dosing and administration. These errors may have serious consequences, particularly in people who take high-risk medications (eg, warfarin, opioids, insulin).
The complexity of a medication regimen may be an independent risk factor for poor outcomes. Regimen complexity has been associated with adverse drug events (ADEs), 4 nonadherence, 5 hospital discharge to an aged care facility, 6 and hospital readmission.4,7 Furthermore, vulnerable population groups such as older people 8 and those with cognitive impairment may be at greater risk of experiencing these errors. To our knowledge, no previous study has investigated the association between medication regimen complexity and mortality in older people.
Multiple medication use is only one component of complexity. However, there is a strong correlation between polypharmacy and medication regimen complexity. 9 Polypharmacy can be defined as either a continuous or dichotomous variable. It has been associated with a range of ADEs, including hospitalization and mortality. 10 However, there is conflicting evidence regarding the association between polypharmacy and mortality. 10 One study reported that the association between polypharmacy and mortality was higher in women than in men. 11
The objectives of this study were to investigate whether medication regimen complexity and/or polypharmacy are associated with all-cause mortality in older people.
Methods
Design, Setting, and Participants
This population-based cohort study analyzed data from the Swedish National Study on Aging and Care in Kungsholmen (SNAC-K). This is an ongoing study on aging and care of people 60 years and older residing in central Stockholm. 12 People were sampled according to their age in 11 age cohorts; the oldest and youngest age groups were intentionally oversampled. 13 Potential participants were excluded if they could not be interviewed because of a hearing impairment or a language barrier. 12 This study analyzed data from participants who completed the SNAC-K baseline assessment between 2001 and 2004.
Medication Assessment
Participants brought all their medications and medication lists to the clinical examination, at which time a physician conducted the medication assessment. For participants residing in a nonhome setting (eg, nursing home, group dwelling or residential home), medical records were used to compile the medication list. Both prescription and nonprescription medications were recorded. 12
Medication regimen complexity was computed by using the Medication Regimen Complexity Index (MRCI). 9 This 65-item validated tool considers dosage form, dosing frequencies, and additional directions for medication use (eg, intake times in relation to food, need to split tablets). Higher MRCI scores reflect more complex medication regimens. The MRCI assesses both prescription and nonprescription medications and takes into consideration scheduled and as-needed medications. Specific instructions for medication dosing were not recorded at the time of data collection (eg, take on an empty stomach). For this reason, it was assumed that all participants took their medications in accordance with standard dosing instructions in the Australian Pharmaceutical Formulary and Handbook, the British National Formulary, and the electronic Medicines Compendium.14-16 MRCI was analyzed as a continuous variable divided by 10 because a 1-unit increase in complexity index was judged not to be clinically relevant. 17 Polypharmacy was analyzed as the total medication count considering scheduled and as-needed medications and prescription and nonprescription medications. 12 We analyzed polypharmacy as a continuous variable rather than as a dichotomous variable because the common polypharmacy cutpoint of ≥5 medications implies a threshold effect and assumes that there is no difference between 1 and 4 medications or between 5 or more medications.
Primary Outcome
The primary outcome measure was all-cause mortality over a 3-year follow-up period (1095 days). Time to death was calculated individually for each participant from the date of baseline clinical examination. Dates of death were obtained from the Swedish National Cause of Death Register. The register is managed by the National Board of Health and Welfare and includes all deaths in Sweden since 1952. 18
Covariates
Age was analyzed as a continuous variable. Activities of daily living (ADLs) were assessed using the Katz ADL scale. 19 The scale measured independence in 6 ADLs (bathing, dressing, toileting, continence, transferring, and feeding) and was analyzed as a continuous variable. Comorbidity was assessed using a modified Charlson’s Comorbidity Index (CCI).20,21 It was computed using the list of diseases recorded at the baseline examination and was analyzed as a continuous variable. Educational level was defined as the highest level completed and was categorized as elementary school, high school, and university. Cognitive status was assessed by the Mini-Mental State Examination (MMSE) and was analyzed as a continuous variable. 22 MMSE assessments were conducted as part of the SNAC-K study in the same way for participants living in home and nonhome settings. Residential setting was categorized as living at home (eg, owner or tenant of an apartment or detached house) and living in a nonhome setting (eg, nursing home, residential home, or group dwelling). 12
Statistical Analyses
Baseline characteristics were presented as numbers and proportions or as medians and interquartile ranges (IQRs). χ2 Tests and Wilcoxon rank-sum tests were used to compare the characteristics of participants meeting the primary end point during the follow-up. A Kruskal-Wallis test was used to analyze differences between the 3 groups of ordinal variables. Variables associated with all-cause mortality in bivariate analyses (P < 0.05) or those associated with unplanned hospitalization in previous research were included in the multivariate models.10,11,20 Variables were checked for multicollinearity. The analyses were weighted by age group and sex to reflect the population of Kungsholmen. Weighting by age group was important because people in the highest and lowest age cohorts were oversampled. 23
Two sets of main analyses were conducted. In the first set Cox proportional hazards regression analyses were conducted to compute unadjusted and adjusted hazard ratios (HRs) with 95% CIs for the association between MRCI and all-cause mortality over a 3-year follow-up period. In the second set, Cox proportional hazards regression analyses were conducted to compute unadjusted and adjusted HRs with 95% CIs for the association between polypharmacy and all-cause mortality over a 3-year follow-up period.
To investigate whether age, sex, and cognition were effect modifiers, 3 sets of subanalyses were conducted, with participants stratified by age (≤80 years and >80 years), sex, and MMSE (<26 and ≥26). Each set was conducted individually for MRCI and for polypharmacy. In the first set of subanalyses, participants were stratified by sex. These subanalyses were conducted because women have previously been reported to have a different pattern of medication use and corresponding association with mortality. 11 In the second set of subanalyses, participants were stratified by age (≤80 years and >80 years). These analyses were conducted because older people with complex medication regimens may, at the same level of medication complexity, be at higher risk of medication errors and adverse events than younger people. We chose a cut-point of ≤80 years because age 80 years is considered an age when SNAC-K participants experience major health changes. 13 In the third set of subgroup analyses, participants were stratified by cognitive status (MMSE<26 and MMSE ≥26). 24 This was done because people with cognitive impairment may have particular difficultly managing complex medication regimens. The MRCI and polypharmacy models were adjusted using the same parameters. Analyses were performed using the Statistical Package for Social Sciences (SPSS) version 21 (IBM Corporation, Armonk, NY) and STATA version 13 (Stata Corp LP, College Station, TX).
Ethical Considerations
All potential participants were provided with written information about the study, and written informed consent was obtained from each participant. If the participant was unable to provide informed written consent to participate, proxy consent was obtained. The study was approved by the regional ethical review board in Stockholm.
Results
Overall, 5111 people were invited to participate in the SNAC-K study. Of these, 1227 refused and 521 were not eligible (262 could not be contacted, 200 died before examination, 32 had moved, 23 did not speak Swedish, and 4 had hearing impairments that prevented them from completing the study assessments). 12 In total, 3363 people agreed to participate in the study. Participation rates were 73% among women and 74% among men. 13 Baseline clinical and medical data were available for 3348 participants. In the final study sample, there were 64.8% women (n = 2170) and 35.2% men (n = 1178). Overall, 14% of the participants (n = 470) died during the 3-year follow-up period (Table 1). Participants who met the primary end point had significantly higher regimen complexity (median MRCI of 15.0 vs 8.0, P < 0.01), were older (median age of 90 vs 72 years, P < 0.01), were less likely to live at home (61.9% vs 96.0% of participants, P < 0.01), had more comorbidities (median CCI of 1 vs 0, P < 0.01), and had lower cognitive status (median MMSE of 25 vs 29, P < 0.01).
Baseline Characteristics of the Participants.
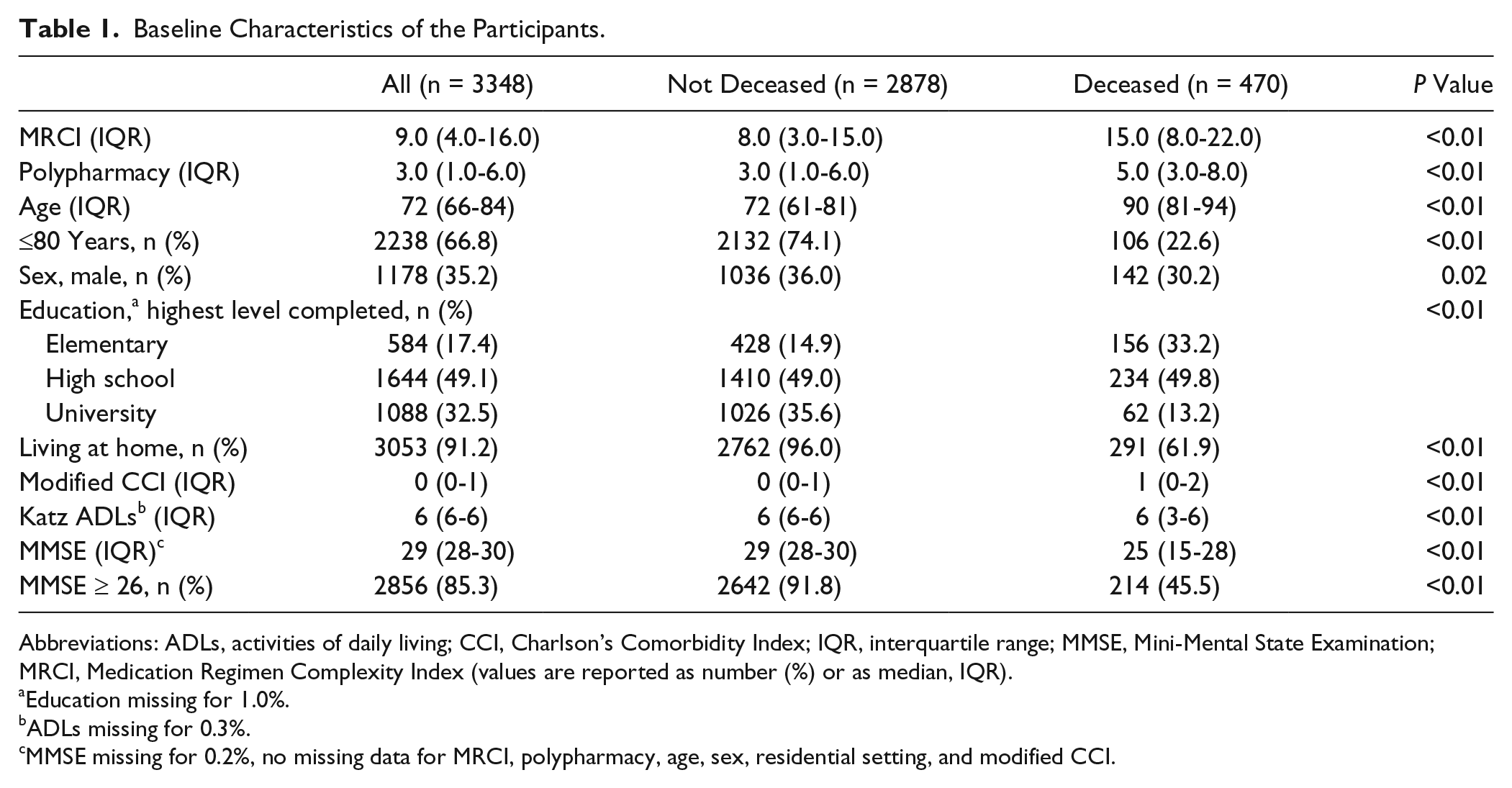
Abbreviations: ADLs, activities of daily living; CCI, Charlson’s Comorbidity Index; IQR, interquartile range; MMSE, Mini-Mental State Examination; MRCI, Medication Regimen Complexity Index (values are reported as number (%) or as median, IQR).
Education missing for 1.0%.
ADLs missing for 0.3%.
MMSE missing for 0.2%, no missing data for MRCI, polypharmacy, age, sex, residential setting, and modified CCI.
Medication regimen complexity was associated with mortality in the unadjusted (HR = 1.61; 95% CI 1.51-1.72) and adjusted analyses (HR = 1.12; 95% CI = 1.01-1.25). Polypharmacy was associated with mortality in the unadjusted (HR = 1.15; 95% CI = 1.13-1.17) but not in the adjusted analyses (HR = 1.03; 95% CI = 0.99-1.06; Figure 1).
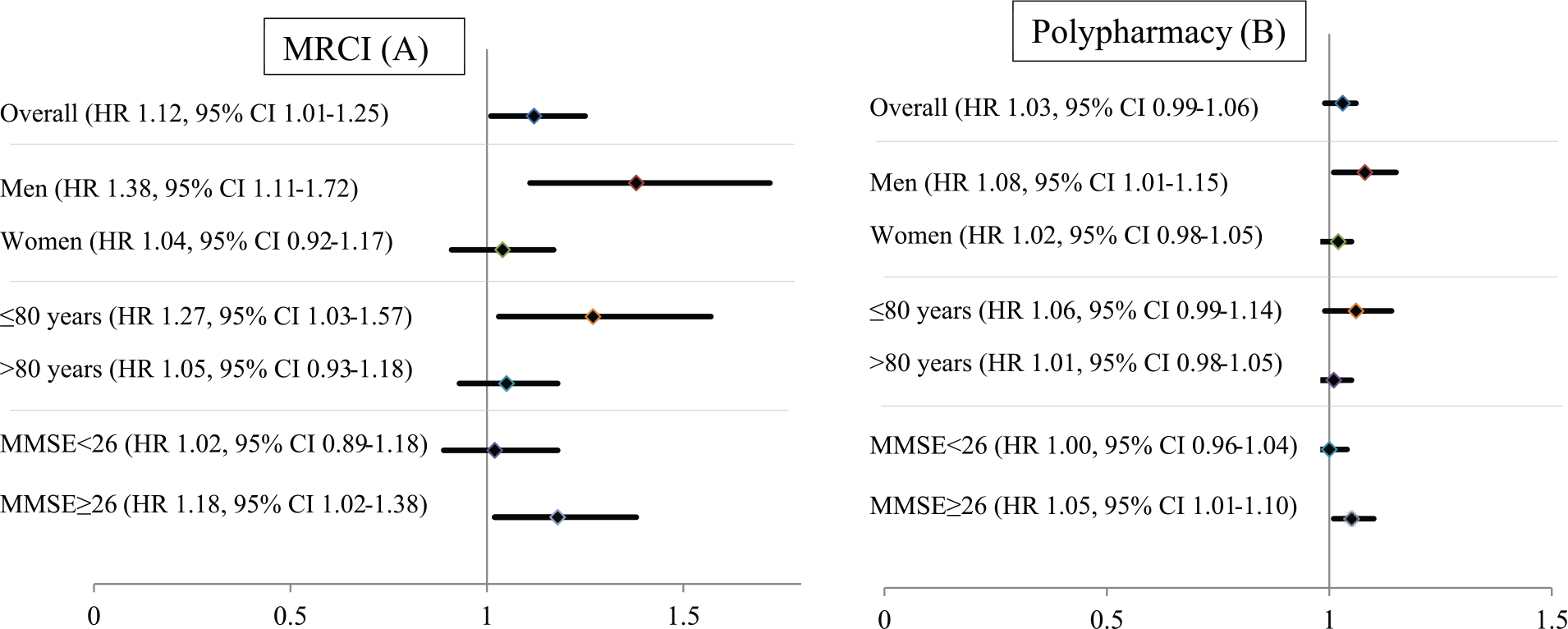
Cox proportional hazards regression analyses for overall associations between MRCI (A) and polypharmacy (B), with all-cause mortality adjusted for age, sex, modified CCI, Katz ADLs, educational level, MMSE, and residential setting. Participants were stratified by sex, age group (≤80 years and >80 years), and MMSE (<26 and ≥26).
In the subanalyses when the study sample was stratified by sex, there was an adjusted association between MRCI and all-cause mortality for men (HR = 1.38; 95% CI = 1.11-1.72) but not women (HR = 1.04; 95% CI = 0.92-1.17). Similarly, in adjusted analyses, polypharmacy was associated with mortality in men (HR = 1.08; 95% CI = 1.01-1.15) but not women (HR = 1.02; 95% CI = 0.98-1.05; Figure 1). When the study sample was stratified by age, adjusted analyses showed an association between regimen complexity and mortality for participants ≤80 years old (HR = 1.27; 95% CI = 1.03-1.57) but not for participants older than 80 years (HR = 1.05; 95% CI = 0.93-1.18). When the study sample was stratified by cognitive status, there was an association between regimen complexity and polypharmacy with mortality in participants with MMSE ≥26 (HR = 1.18; 95% CI = 1.02-1.38) but not in participants with MMSE <26 (HR = 1.02; 95% CI = 0.89-1.18; Figure 1).
Discussion
This was the first study to investigate and compare the association between medication regimen complexity and polypharmacy with all-cause mortality. The main finding of the study was that medication regimen complexity was a better overall predictor of all-cause mortality than polypharmacy. However, medication regimen complexity and polypharmacy were only associated with mortality among men and in all participants with MMSE ≥26 regardless of sex. In participants ≤80 years old, regimen complexity but not polypharmacy was associated with mortality.
There are several reasons why medication regimen complexity may be a better overall predictor of mortality than polypharmacy. First, the complexity of the administration instructions may have an effect over and above that of the crude number of medications in increasing the likelihood of medication errors. Higher regimen complexity has also been associated with nonadherence, 5 which in turn is a risk factor for poor treatment outcomes, including mortality. 25 Second, medications that are complex to administer may be associated with a high risk of fatal ADEs. Warfarin, insulin, and opioids may be complex to administer because of potentially variable dosing, the need for injection, and possible transdermal delivery. These medications are also associated with potentially fatal ADEs such as bleeding, hypoglycemia, falls, and fractures. Warfarin and insulin were 2 of the top 4 medications implicated in emergency department visits for ADEs in the United States. 26 Finally, severe medical conditions that require complex medication regimens (eg, chronic obstructive pulmonary disease) may be associated with a higher risk of death. 27 To account for this, we adjusted our analyses for comorbidities using the modified CCI. However, there remains the possibility of residual confounding.
Medication regimen complexity was associated with higher mortality in people <80 years old but not in people ≥80 years old. This may be because people who were ≥80 years old may have had other non–medication-related risk factors for death. Furthermore, clinicians may have “deprescribed” medications and simplified medication regimens in people ≥80 years old with limited life expectancy. 28 This may result in participants with less-complex medication regimens having a higher risk of death. Less-aggressive treatment regimens in participants with limited life expectancy may have contributed to the lack of association between medication regimen complexity and polypharmacy with mortality in people ≥80 years old. The lack of a significant association between both regimen complexity and polypharmacy with mortality in participants >80 years old could also be attributable to survival bias.
Regimen complexity and polypharmacy were associated with mortality in men but not in women. This may be partly attributable to differences in disease-specific mortality, especially for ischemic heart disease, other heart disease, and diabetes. 29 In Sweden, between 2000 and 2004, age-standardized mortality rates for diabetes were around twice as high in men compared with women. 29 This may explain the sex difference in the association with mortality because cardiovascular and diabetes medication regimens may be particularly complex, and these conditions are associated with higher mortality in men. Our results are in accordance with those of a previous study, which reported that the association between polypharmacy and mortality was stronger for men than for women over a 2- to 5-year follow-up. 11 Another possible reason for complexity being associated with mortality in men but not women may be sex differences in pharmacodynamics and pharmacokinetics. 30 Women have a lower blood volume than men but also more lipid mass and, therefore, a higher volume of distribution of lipophilic psychotropics.31, 32 Therefore, lipophilic psychotropics may accumulate over time in women, which can lead to ADEs. However, we did not investigate whether men and women took different types of medications, and this may have contributed to the different pattern of association with all-cause mortality.
In our study, regimen complexity and polypharmacy were both associated with mortality in participants who had an MMSE ≥26 but not in participants with an MMSE below 26. This appeared counterintuitive because we hypothesized that people with cognitive impairment may be at greater risk of adverse events secondary to complex regimens. However, the finding was consistent with previous researchthat found that people without Alzheimer’s disease (AD) had a higher risk of death associated with sedatives and anticholinergics than those with AD. 33 This may be because people with dementia are at increased risk of death from a range of non–medication-related factors. The relative contribution of medications may be greater in those without cognitive impairment. Moreover, the lack of association between regimen complexity and mortality in people with MMSE <26 may be because clinicians minimized or discontinued prescribing complex and high-risk medications to participants with cognitive impairment (eg, warfarin, insulin, and oral hypoglycemics). Another potential explanation for the lack of association between regimen complexity and mortality in participants with MMSE <26 could be that these participants received assistance to administer their medications.
Our study has a number of clinical implications. The numbers of prescribed medications are increasing among older people. 1 Our study suggests that the complexity of a medication regimen may be an additional independent risk factor for mortality. Evidence is accumulating about the benefits of medication cessation or deprescribing in patients with limited life expectancy.28,34 Deprescribing complex or unnecessary medications may confer benefits to patients. It is not known whether targeted interventions to reduce regimen complexity improve survival. However, deprescribing has been associated with lower mortality in geriatric nursing departments, 35 and in institutional settings, it has been associated with reduced hospitalization and maintenance of quality of life. 36
Strengths and Limitations
The strengths of this study include the population-based sample, which included people living in home and nonhome settings. If a participant was unable to self-report information (eg, as a result of cognitive impairment), a proxy provided this information instead. This permitted data collection for participants with cognitive impairment. The data used for this study were likely to be accurate because they were collected by trained staff using validated scales,9,19 and the dates of death were obtained from the Swedish National Cause of Death Register. Furthermore, we considered both prescription and nonprescription medications when computing complexity. This would not have been possible if data were obtained from a prescription database. Although we had data on medication dose, form, and dose frequency, it was a limitation that we did not have access to data on specific instructions for medication use (eg, take medication on an empty stomach). We overcame this by using standard dosing instructions published in recognized key reference texts to compute the MRCI. This may have over- or underestimated participants’ true regimen complexity. However, the assumption that participants took their medications in accordance with standard dosing instructions in key reference texts had a small impact on overall complexity. Assumptions related to additional directions contributed no additional complexity for 50% of participants; 1 to 2 units of MRCI based on assumptions contributed for 42% of participants; and between 3 and 7 units of MRCI contributed for the remaining 8% of participants. Given that MRCI scores ranged from 1.5 to 76, the contribution of these assumptions was minimal.
Our results may not be generalizable to other populations outside of Sweden and Europe because of differences in the structure and availability of health and social services. As with all observational studies, there is the possibility of confounding. The HRs were small after adjusting for confounders. The HRs for MRCI and polypharmacy were 1.12 and 1.03, with a lower 95% CI of 1.01 and 0.99, respectively. These results were very close to the null. It is possible that MRCI and polypharmacy were markers of multimorbidity. Although we adjusted our analyses for comorbidity, ADLs, and a range of other clinically important parameters, the possibility of residual confounding cannot be excluded.
Conclusion
Regimen complexity was a better overall predictor of mortality than polypharmacy. However, regimen complexity was not predictive of mortality in women, in participants >80 years old, or in those with MMSE<26. The age and sex differences in the association with mortality deserve further investigation.
Footnotes
Acknowledgements
We thank all participants and the members of the SNAC-K Project Study Group for data collection and collaboration. Our special thanks go to Dr Kris Jamsen for statistical support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Swedish National study on Aging and Care, SNAC (![]() ), was funded by the Ministry of Health and Social Affairs, Sweden; the participating county councils and municipalities; and the Swedish Research Council. BCW received a Monash Graduate Scholarship to undertake the research reported in this manuscript.
), was funded by the Ministry of Health and Social Affairs, Sweden; the participating county councils and municipalities; and the Swedish Research Council. BCW received a Monash Graduate Scholarship to undertake the research reported in this manuscript.