
Abstract
Asthma exacerbations are preventable, costly, and a common cause of school absenteeism. Using Group Concept Mapping, we interviewed school nurses, staff, school-based providers, and families/caregivers (N = 31). We elicited feedback regarding social circumstances relevant to asthma exacerbations in schools and then participants prioritized those circumstances. Perspectives of our 31 participants produced 84 statements, grouped into 10 clusters and rated separately on the impact and feasibility of preventing asthma exacerbations in schools. The highest rated clusters were Exposure to smoking / vaping and Caregiver / Child lack of asthma education. Stakeholders identified a variety of factors, with some rated as highly impactful yet less feasible to address. Important circumstances are recognized by multiple stakeholders, yet are underresearched, especially to guide collaborative school-based interventions. Our findings can be used to prioritize feasible and impactful interventions in collaboration between school nurses, staff, school-based providers, and families, ultimately decreasing the suffering of children with asthma.
Keywords
Introduction
Affecting more than 4.9 million children and costing more than $10 billion per year in the United States (Asthma and Allergy Foundation of America, 2024; Imanak et al., 2025), asthma is common and problematic. While the prevalence and cost have decreased over the last few years, childhood asthma exacerbations still result in over 270,000 emergency department visits and 27,000 hospitalizations each year (Centers for Disease Control and Prevention (CDC), 2024b). In schools, asthma is one of the most common chronic conditions and a frequent cause of school absenteeism (CDC, 2024a; Thomas et al., 2020). Given its significant prevalence, preventable poor outcomes, and extreme costs, asthma in children noticeably needs further inquiry, especially through collaboration with the school nurse (SN) and school-based health centers (SBHCs).
School nurses provide direct care to all students and are often the first to identify urgent medical concerns, address chronic conditions, and coordinate the variety of care services, including referral to SBHCs (National Association of School Nurses (NASN), 2022). If available, SNs can work together with SBHCs in a unique model providing services jointly in or near a school, typically more accessible than outside providers (Borkowski et al., 2023), critical for those experiencing an acute asthma exacerbation. Harnessing SN leadership and collaboration with SBHCs, school staff, and families, these key stakeholders can promote policy changes within schools, especially given the SN's established relationships and an SBHC's proximity to school-age patients (Martin et al., 2020).
Risk for asthma exacerbations is associated with social factors, including socioeconomic status, health inequities, crime or violence exposure, food insecurity, and unemployment (Simoneau & Gaffin, 2023). School-based asthma programs, often led by SNs, improve asthma outcomes via components such as asthma health literacy, mitigation of air quality or pest reduction, and self-management (Perry et al., 2024). However, these asthma programs vary widely, as it may be difficult to prioritize school interventions to address harmful social risk factors without knowing the perspectives of SNs, SBHCs, school staff/administration, and family/caregivers. Perspectives of these stakeholders can help identify what factors are most relevant and actionable within the context of schools.
Aims
The purpose of this study was to obtain stakeholder feedback from SNs, SBHC providers, school staff/administration, and families/caregivers about the social circumstances of children with asthma, to provide a foundation for actionable interventions in schools. To our knowledge, there are no studies that collect and synthesize information based on the experiences of these four groups, particularly focusing on asthma exacerbations. Using the innovative, research-supported method of Group Concept Mapping (GCM), we pursued the following two aims:
Explore and describe the social circumstances relevant to the management of childhood asthma exacerbations from the perspectives of key stakeholders; and Prioritize concepts as impactful and/or feasible to prevent asthma exacerbations in schools.
Methods
We used GCM to identify concepts at the intersection of the perspectives of SNs, SBHC providers, school staff/administration, and families/caregivers. Group Concept Mapping is a mixed methods approach designed to elicit, synthesize, and make actionable information from diverse stakeholders (groupwisdom™, 2022). The Vanderbilt University Medical Center Institutional Review Board determined our study was Exempt from review under submission number 230199. For consent, participants completed an online voluntary participation form and confirmed verbal consent at the start of brainstorming sessions.
Setting and Participants
For sufficient content coverage and depth, we conducted four groups in 2024, each with five to eight participants, segregated by participant type (SNs, SBHC providers, school staff/administration, and families/caregivers). We used purposive sampling via email contacts through the National School-based Health Alliance, a national group of members connected to SNs and SBHCs. Next, we asked SBHC providers to distribute flyers/emails through their personal and professional networks to reach the remaining three groups. We initiated recruitment in December 2023 using inclusion criteria as follows:
School nurses: Elementary/ secondary school, experience with patients with asthma; SBHC Providers: Advanced providers in schools within the last two years; School staff/administration: Adult school staff member interacting with students with asthma, aware of asthma through parental or SN report; and Families/Caregivers: Adult living with a school-age (5–18 years old) patient with asthma symptoms in the last two years. Families/Caregivers served as proxy, as we felt caregivers tend to be more aware of social conditions, particularly for elementary patients with asthma.
Design: GCM Method
Group Concept Mapping engages stakeholder experts to elicit, in a structured way, firsthand perspectives on a topic, with the assumption that the people with lived experience are the best informants (LaNoue et al., 2019; Trochim, 1989). Group Concept Mapping uses a sequential mixed methods design that combines qualitative and quantitative data (Begert, 2022) and consists of the following steps as depicted in Figure 1: (1) Brainstorming: Develop a ‘focus prompt’ to which participants will respond to during synchronous brainstorming sessions; (2) Statement Analysis: Review statements to synthesize ideas, avoid redundancy, and ensure consistency and reliability; (3) Sorting: Participants sort statements in an online virtual tabletop, and name each pile for its theme; and (4) Rating: Participants rate each statement according to predefined dimensions. (5) Statistical Analysis: Hierarchical cluster analysis and rating analysis; and finally (6) Visualization and Interpretation: Summarize findings and present in useful visualizations. Details are further expanded upon below.

Steps of group concept mapping. Group Concept Mapping (GCM) uses a sequential mixed methods design with multiple steps.
Data Collection
Data collected in this study was reported according to the evidence-based guideline for reporting concept mapping research (Pantha et al., 2023). We collected and managed data using the software groupwisdom™ (2022) and the Research Electronic Data Capture (REDCap) tool (Harris et al., 2009; Harris et al., 2019). Developed by Concept Systems, Inc., a leading expert in GCM, groupwisdom™ is a user-friendly web-based application that integrates the methods for collecting, analyzing, and visualizing GCM data. The groupwisdom™ support team offers training courses, help modules, and on-call consultations to assist researchers with GCM studies.
Brainstorming Sessions and Idea Synthesis
We developed and pilot-tested our brainstorming prompt in a Community Engagement Studio through The Meharry-Vanderbilt Community Engaged Research Core (Vanderbilt Institute for Clinical and Translational Research, 2024). Our prompt was:
Sorting and Rating Tasks
During May 2024, participants sorted response statements online into virtual piles and named each pile for its theme. Participants were provided with instructions explaining the use of a 5-point Likert scale, and asked to rate each statement, answering two questions separately: (1) How much of an impact would screening for this social condition in schools have on a child's asthma? and (2) How feasible is screening for and addressing this social condition in schools? Ratings were from 1 (no impact at all; not feasible at all) to 5 (a very high impact; very feasible). Participants were able to save their work and return later as needed to complete both activities.
Data Analysis
For analysis, we used groupwisdom™ for data quality review, aggregating the sorted results, and applying multidimensional scaling to produce a point map as a visual representation of the data. Each point is a concept from brainstorming, and the distances between points (bridging values) serve as an index of their relatedness (Dunlop et al., 2020; groupwisdom™, 2022; LaNoue et al., 2019). Next, we used unsupervised hierarchical cluster analysis of the distances of the points to produce a visual map of clusters of the data. Lastly, we analyzed sorting and rating data at the level of the individual statements and cluster level. We validated groupwisdom™ results by exporting our datasets and analyzing them using Python in Jupyter Notebook.
Results
Description of Sample
A total of 39 participants completed the demographic survey, of which 16 (41%) were available to attend a brainstorming session. An additional 15 participants completed the sorting and rating tasks, for a total number of participants N = 31 (31 of the 39 participants who volunteered (80%)). The eight remaining volunteers were either unavailable for online brainstorming session times or did not respond to email or text follow-up. Descriptive statistics are summarized in Table 1. Our participants were mostly over the age of 35 (93%), White (74%), not Hispanic (90%), and female (84%).
Demographics of Study Participants.
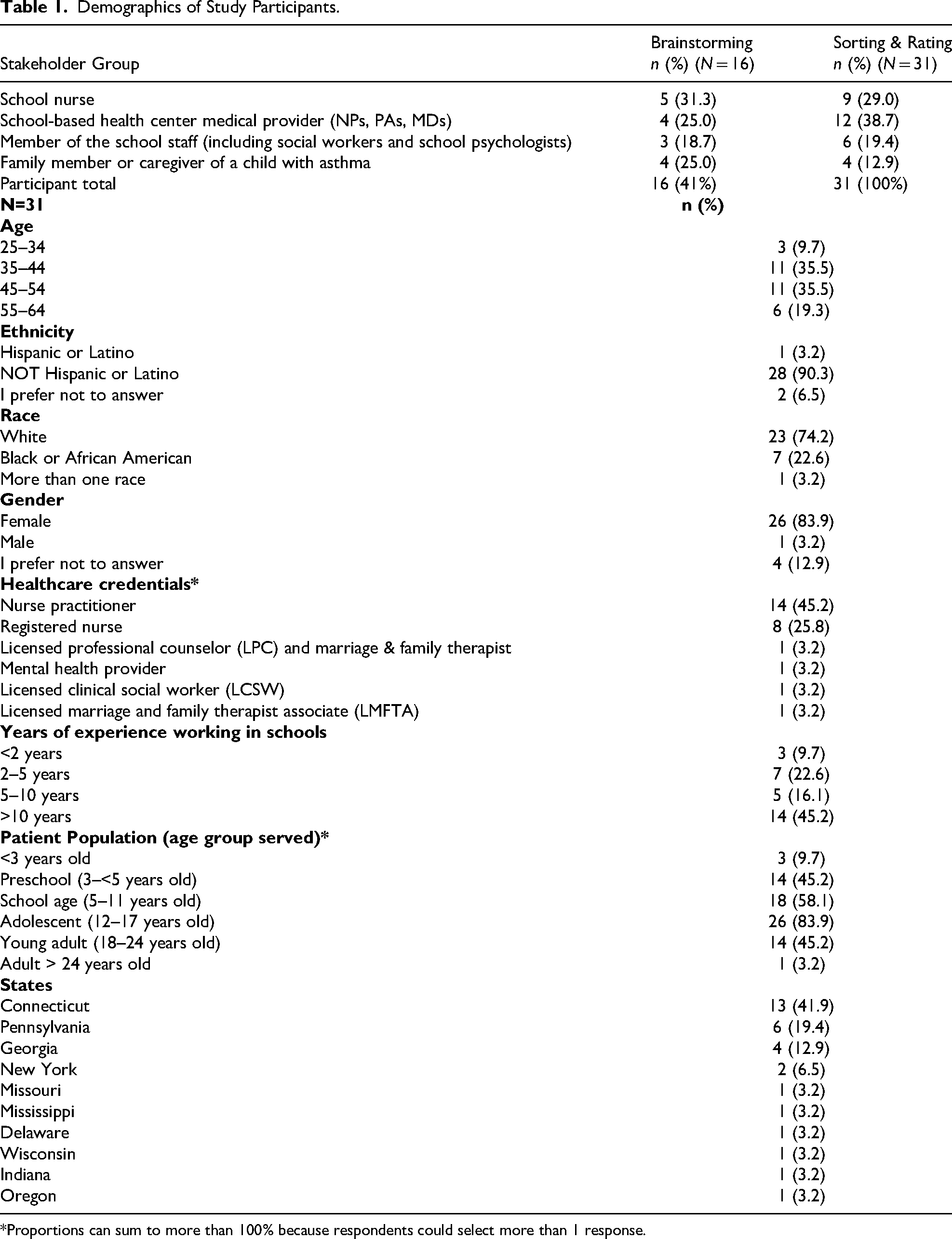
*Proportions can sum to more than 100% because respondents could select more than 1 response.
Sorting
Participants were given 84 statements for sorting into piles based on concepts. The average number of piles was 7.23, with a median of 8. The lowest number of piles was 4, while the highest number was 11.
Point Map
The groupwisdom™ software calculates a stress value for the point map, which measures goodness of fit. Lower stress values have a better fit and less variability in participant's sorted data. A reliable average stress value is 0.285 (range 0.155–0.352) (Brennan et al., 2012). Our stress value was calculated at 0.2773, which suggests an adequate fit.
Cluster Map
Conducted within the groupwisdom™ software, we reviewed the range of cluster solutions and reached consensus on the cluster map presented in Figure 2. Using Python for agglomerative hierarchical clustering, we validated the choice of 10 clusters using a dendrogram. Table 2 provides definitions of the clusters and examples of highly rated statements. The variety of clusters represents the concepts identified and labeled by our participants as social circumstances affecting children with asthma. The clusters are complex, with compounded factors such as Unhealthy school environments and Specific school rules / policies that likely interact, or Healthcare system challenges and Post-immigration challenges that highlight the difficulty of navigating the healthcare system, especially if newly immigrated. An example of a statement within the Caregiver / Child lack of asthma education is “Children do not understand how to use inhalers” rated as highly impactful (4.07) and feasible to address (4.26). Within Strained family resources, “Multiple social risks such as homelessness or caregiver mental health make it difficult for caregivers to manage a child's asthma” was rated highly impactful (4.20), yet not as feasible to address (3.52). A full list of statements is available in Supplemental Material.

Cluster map of statements. The cluster map displays how participants grouped and named groups of statements (groupwisdom™, 2022). I = Impactful average rating on scale 1–5. F = Feasible average rating on scale 1–5.
Clusters with Definitions & Example Statements with Average Ratings.

Impact and Feasibility Rating
The average ratings of the clusters (also produced within the software) are depicted in Figure 2. The clusters rated most impactful to prevent asthma exacerbations were Exposure to smoking / vaping and Caregiver / Child lack of asthma education, with average ratings of 3.95 and 3.85, respectively. The clusters rated most feasible were Caregiver / Child lack of asthma education, Exposure to smoking / vaping, and Specific school rules / policies, with average ratings of 3.79, 3.50, and 3.50. Overall, participants rated most clusters as more impactful than feasible.
Group Comparisons
We compared cluster ratings for impact and feasibility for all participants and by the separate stakeholder groups. There was very low agreement in relative cluster ratings for Specific school rules /policies and Unhealthy environmental factors, while Caregiver/Child Lack of Asthma Education and Financial barriers had moderate agreement. All groups rated Exposure to smoking / vaping as their most impactful cluster, except for school staff, who rated Strained Family Resources as most impactful. All groups rated Caregiver/Child Lack of Asthma Education as their most feasible cluster, except school staff who rated Financial barriers as most feasible.
Discussion
We gathered input from SNs, SBHC providers, school staff/administration, and families/caregivers, who produced 84 independent statements, grouped these concepts into 10 clusters, and rated statements for impact and feasibility to prevent asthma exacerbations. Our major findings include: (1) Exposure to smoking / vaping and Caregiver/Child lack of asthma education were rated as the most impactful and feasible concepts to address in schools. (2) Our participant groups tended to agree on concepts that are impactful but differ on whether these same concepts are feasible. (3) There are complex and compounding factors that may be impactful; however, they may not be feasible to address.
Relatively, all groups rated Exposure to smoking / vaping and Caregiver/Child lack of asthma education as highly impactful to address. There is strong representation in prior research regarding the association of smoking, secondhand exposure, and vaping to negative asthma outcomes, related to harmful chemicals and nicotine in these products (Beznos et al., 2021; Roh et al., 2023). However, smoking and vaping discussed with asthma patients and families remains low (Beznos et al., 2021). We need innovative ways to approach adolescents and families about smoking and vaping cessation and prevention, for example, screening, text-based reminders, mobile health applications, and peer-to-peer prevention (Jensen et al., 2024; Müssener et al., 2020), which are feasible at schools. Further research can incorporate feedback from middle school-age and adolescents to increase the potential success of stakeholder efforts and prevention programs within school systems.
All groups except school staff rated Caregiver/Child lack of asthma education as their most feasible cluster. Expansive literature notes that asthma education is associated with better outcomes, less missed school days, and empowered patients and families (Culmer et al., 2020; Perry et al., 2024). Our study is consistent with this prior research, highlighting the need for further research and implementation and program evaluation of tailored education not only for family/caregivers and patients with asthma but importantly, for staff/administration who interact with these students in school. As nonhealthcare providers, school staff/administration may be unaware of the potential of asthma education to improve asthma outcomes or perhaps the critical role of SNs in providing that education. Prior evidence is clear: SNs can be leaders in research and implementation of school interventions, providing education, increasing awareness, and collaborating with additional stakeholders to ultimately improve asthma outcomes in schools (Kindi et al., 2022).
Our findings also demonstrate the complexity of factors contributing to asthma exacerbations, and therefore, solutions will not be simple. We need innovative approaches in schools to address all the clusters, with increased involvement of all four groups in planning and testing future interventions, particularly in addressing home and school environments. In 2024, 26 different nursing organizations met with the White House Council on Environmental Quality, including the National Association of School Nurses and the National Association of Pediatric Nurse Practitioners, recommending continued advocacy for environments that equitably ensure students can breathe and learn (Alliance of Nurses for Healthy Environments, 2024). Community-based participatory action research, which includes involvement of community members, community health workers, pharmacists, and use of home visits and/or telehealth, is a promising component to address the topics of our clusters, especially unhealthy school and home environments (Culmer et al., 2020; Gilkey et al., 2023; Kennedy et al., 2024).
Strengths and Limitations
Group Concept Mapping allows for brainstorming to capture experiences of a variety of stakeholders, obtaining deeper insights regarding asthma exacerbations in schools and the factors most impactful and feasible. We acknowledge the missing voice of school-age youth with asthma, as while families/caregivers served as proxy, combining both the voices of caregivers and youth may influence our findings. As with convenience and snowball sampling, there is the potential for selection bias and generalizability is limited, even with attempts to recruit nationally. Small group sizes limited our ability to meet statistical assumptions for pairwise comparisons between groups. While there is a risk for self-report bias, we feel this was minimal due to our engagement during brainstorming, validated methods, and a rigorous data analysis and visualizations. Finally, groupwisdom™ allows participants to log in individually and save their work for sorting and rating, allowing for reflection time and avoiding social desirability bias.
Implications for School Nursing
Our findings highlight a starting place and urgent need for SN-led research that tests and evaluates interventions addressing social circumstances that stakeholders identified as impactful and feasible. School nurses can select evidence-based asthma education for implementation within their schools, assigning pre and posttest evaluations, collaborating with SBHC providers or local universities to support data collection and analysis. Utilizing the existing youth educational resources, or community liaisons, SNs can coordinate smoking/vaping prevention awareness, such as social media posts geared for asthma patients and families. Finally, this study provides an example of the innovative method of GCM to elicit the perspectives of key stakeholders. School nurses and SBHCs can use GCM to investigate many topics presented in school healthcare, such as diabetes, obesity, and others. A combination of perspectives on topics and interventions that leverage SNs, SBHCs, and school staff can have synergistic impact, and future research should be led, implemented, and evaluated by SNs and SBHCs.
Conclusion
Evidence from this study gives insight into the social circumstances considered impactful to school-age children with asthma, with potential for feasible interventions in schools. These perspectives can inform SN-led asthma education and collaborative community resources, particularly increasing the awareness and knowledge of school staff/administration and families/caregivers. By prioritizing interventions that are viewed as highly feasible, future research can harness the unique collaborative delivery model of care by SNs and SBHCs in schools. By focusing on social circumstances that our stakeholders prioritized as impactful and feasible, SNs and SBHCs can raise awareness, improve community partnerships, and increase practical interventions in schools that decrease asthma exacerbations, thereby ultimately decreasing medical costs and the suffering of children and adolescents with asthma.
Supplemental Material
sj-docx-1-jsn-10.1177_10598405261447899 - Supplemental material for Social Circumstances Affecting Asthma: A Group Concept Mapping Study of School Stakeholders
Supplemental material, sj-docx-1-jsn-10.1177_10598405261447899 for Social Circumstances Affecting Asthma: A Group Concept Mapping Study of School Stakeholders by Vera Borkowski, Alvin D. Jeffery and Marianna (Marnie) LaNoue in The Journal of School Nursing
Footnotes
Acknowledgments
Sincere thanks to all participants for their time and contribution to make this research possible. Research reported in this publication was supported by a National Association of Pediatric Nurse Practitioners (NAPNAP) Foundation Research Grant. Editing and finalization of the manuscript were supported by the National Institute of Nursing Research of the National Institutes of Health under Award Number T32 NR008857, during Dr. Borkowski's postdoctoral fellowship at the University of Pittsburgh. The content is solely the responsibility of the authors and does not necessarily represent the official views of NAPNAP or the National Institutes of Health. This work was funded in part by the Gordon and Betty Moore Foundation through Grant GBMF9048 to Alvin D. Jeffery. This work was also supported by a 2024 Vanderbilt University School of Nursing Student Achievement Research Award and the 2023–24 Nurses’ Educational Funds Evelyn J. Barclay Scholarship. REDCap is supported in part by the National Institutes of Health National Center for Advancing Translational Sciences under Award number UL1 TR000445.
Ethical Statement
The Vanderbilt University Medical Center Institutional Review Board determined the study was Exempt from review under submission number 230199.
Author Contribution(s)
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Association of Pediatric Nurse Practitioners (NAPNAP), National Institute of Nursing Research, Gordon and Betty Moore Foundation, Vanderbilt University School of Nursing, Nurses’ Educational Funds, (grant number Foundation Research Grant, T32 NR008857, GBMF9048, Student Achievement Research Award, Evelyn J. Barclay Scholarship).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.