
Abstract
School nurses lead efforts to assess and respond to individual and community health needs by implementing and evaluating policies, procedures, and actions that impact student health, safety and achievement. Despite the importance of developing school nurse leadership, few reports are available to evaluate evidence-based programs designed to increase school nurse leadership practice. This report describes the development and evaluation of a school nurse leadership program implemented from 2016 to 2024 in the United States. Sixty-three school nurses and administrators who participated in the program evaluation demonstrated increased leadership knowledge, confidence, skills, and behaviors with evidence of positive impacts on school communities—outcomes that align with the Kirkpatrick Model for evaluating training programs. As the leadership program aligned with national standards and frameworks and was delivered in both virtual and in person formats, a future goal is to implement the program at the local, state, and national levels with adequate resources provided.
Keywords
Nurses working in schools are often the sole healthcare professionals in the educational setting. They are in a unique position to influence the health and safety of all students, teachers, administrators, and the larger school community. School nurses lead efforts to assess and respond to individual and school community health needs and implement and evaluate policies, procedures, and actions that positively impact student health, safety and achievement at school (NASN, 2024a). For the specialty of school nursing, leadership is identified by the National Association of School Nurses (NASN) as one of the five principles of the School Nursing Practice Framework™ (Framework; NASN, 2024b). Despite the importance of developing school nurse leadership for both school nurses providing direct clinical services as well as school nurse administrators, no peer-reviewed reports are available on recently implemented evidence-based school nurse leadership programs (Mazimpaka et al., 2025). The goal of this report is to describe the evaluation of a national school nurse leadership continuing education program (Program) guided by the Kirkpatrick Model (Kirkpatrick & Kirkpatrick, 2010).
Program Development
Developed by experienced university school nurse educators, the Program goal was to increase school nurse leadership knowledge, confidence, skills, and behaviors. The Program was guided by prior school nurse leadership programs operated by the Healthy Schools Campaign (2006–2011) and Johnson and Johnson/Rutgers University (1988–2016; Cogan, 2018; Gibbons et al., 2012; M. Bergren & D. Fishman, personal communication, August 19, 2025). The Scope and Standards of School Nursing Practice was an essential resource for developing the curriculum (NASN, 2022). Participant learning outcomes were aligned with identified competencies within the Leadership standard, including those related to accountability, conflict, culture, evaluation, policy, and professionalism. Based on participants’ needs assessments, competencies within other school nursing practice standards, such as Advocacy, Communication, Ethics, Quality of Practice and Resource Stewardship, were also used to inform content and instruction. Additional resources included guidelines for the educational design process for continuing nurse education from the American Nurses Credentialing Center (ANCC), Specific, Measurable, Attainable, Relevant, Time-bound, Inclusive, Equitable goal setting from the Institute on Community Integration, and the backward design process from the Association for Supervision and Curriculum Development (ANCC, 2023; ICI, N.D.; McTighe & Wiggins, 2012).
The Program included topics of self-assessment and goal setting, advocacy, budget and grants, conflict management, data and technology, evaluation, legal considerations, networking, policy development, professionalism, and team building. Instructional strategies chosen were guided by adult learning best practices (Chugai et al., 2017; Kurt, 2020). Program components included: live workshops led by experts; pre/post workshop instructional assignments; and participant engagement in cohort virtual activities. Each participant was guided to identify, plan, implement and evaluate a year-long project based on their individual self-assessment and individual consultation with Program educators. Although project completion was not required to obtain nursing contact hours, participant presentation of project progress demonstrated knowledge and skills attained and the opportunity for earning a School Nurse Leadership digital badge from the Program's University, a potential indicator to the school district of leadership skills attained (Graebe et al., 2025). A maximum of 40 nursing contact hours for educational activities were offered by an ANCC accredited nursing continuing professional development provider.
Program Delivery
From 2016 to 2024, 10 cohorts of school nurse professionals participated in the Program (ranging from 11 to 27 participants within each cohort). One hundred seventy-five Program participants (128 school nurses; 28 school nurse administrators; 19 combined) represented 20 states in the United States with most working in Massachusetts (MA; n = 101), Vermont (n = 22), Arizona (n = 10), Maine (n = 10), and Kentucky (n = 6). Monthly in-person workshops were held for MA nurses (2016–2018) and in 2019, workshops were offered both in-person and virtually. Beginning 2020, the 90-to-120-min workshops were delivered exclusively virtually with participants also completing assignments individually on their own time. One non-U.S. nurse working internationally participated in 2020.
The Kirkpatrick Model
Program evaluation was guided by the Kirkpatrick Model. This model was first introduced in the 1950s to measure the impact of training for workers and organizations. The Kirkpatrick Model has been used more recently to evaluate leadership programs for nurses working in hospital settings (Dwyer et al., 2025; Huang et al., 2025) and has been recommended for use in evaluating leadership training for school nurses (Mazimpaka et al., 2025). The Kirkpatrick Model has four levels—Reaction, Learning, Behavior, and Results. Level 1, Reaction, refers to the “degree to which participants find the training favorable, engaging and relevant to their jobs” (Kirkpatrick & Kirkpatrick, 2010, p. 9). Level 2, Learning, examines how the training impacted participants’ knowledge, skills, attitude, confidence, and commitment. Level 3, Behavior, identifies how participants apply the learning in their workplace. Level 4, Results, is “the degree to which targeted outcomes occur as a result of the learning event(s) and subsequent reinforcement … in a not-for-profit, government, or military organization [and] it means accomplishing the mission within the resources allocated” (Kirkpatrick & Kirkpatrick, 2010, pp. 5–6). Within Level 4 are leading indicators, which are “short-term observations and measurements that suggest that critical behaviors are on track to create a positive impact on the desired results” (Kirkpatrick & Kirkpatrick, 2010, p. 6).
Method
Survey Development
An anonymous survey developed by the Program educators, and hosted by Qualtrics software, was used to evaluate the Program. A panel of two internationally recognized content experts (a university nurse researcher and an external school nurse specialist) collectively scrutinized the items for appropriate item construction, clarity, representativeness of concepts, and redundancies in measurement. Decisions to retain or delete items were based on the expert panel's consensus on the contribution of each item to the measurement domains. The survey was pilot tested before dissemination and evaluated for clarity, ease of completion, and relevance to practice.
Consistent with the Kirkpatrick Model, the survey questions were categorized into (a) Reaction to education/training (engagement, relevance, satisfaction), (b) Learning (knowledge, skills, attitude, confidence, commitment), (c) Behavior (applying learning in work environment), and (d) Results (targeted organization outcomes occur) according to the Kirkpatrick Model. The final survey consisted of 54 questions, including 12 questions for demographics, 30 multiple-choice questions with 4-point Likert scales (not at all, a little, somewhat, a lot), eight questions with dichotomous responses (Yes/No), and four open-ended questions. The study was approved by Northeastern University Institutional Review Board (#24-08-40).
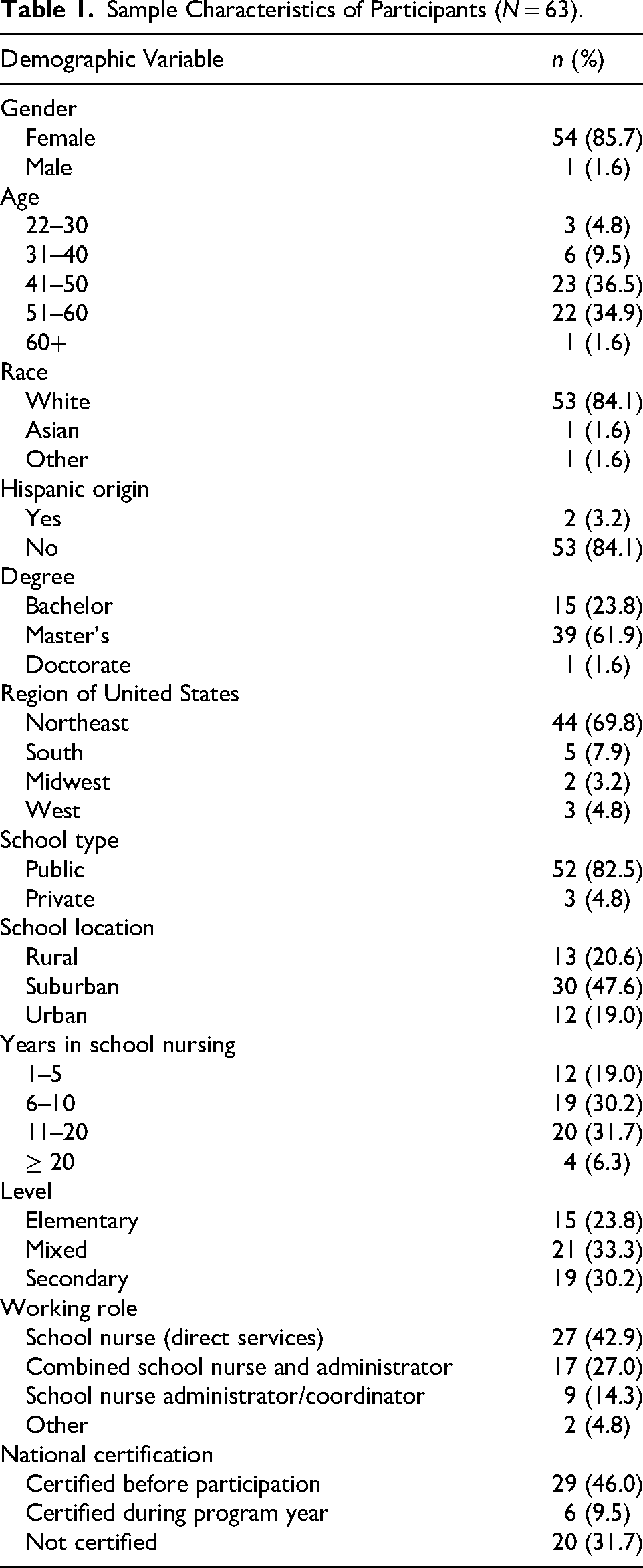
Sample Characteristics of Participants (N = 63).
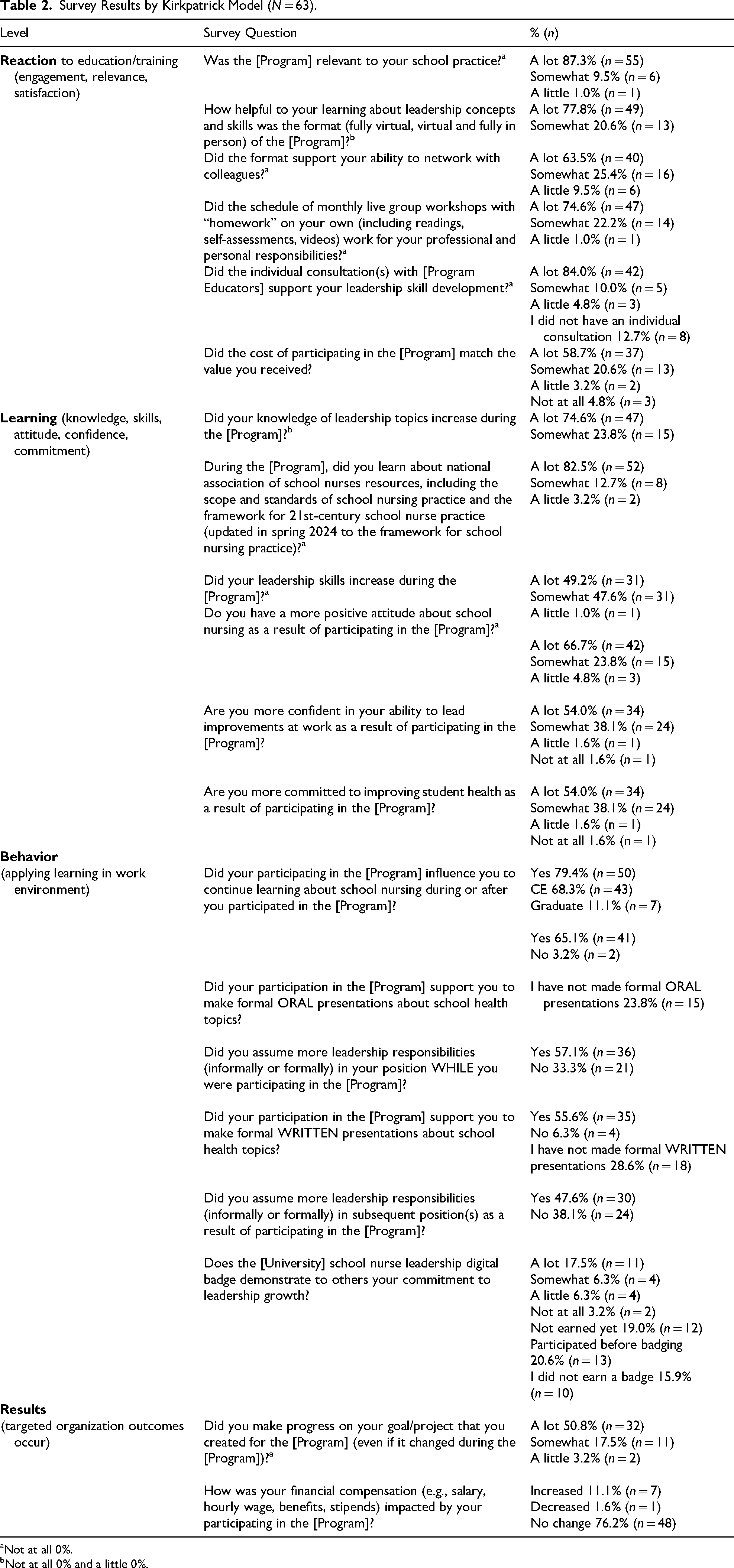
Survey Results by Kirkpatrick Model (N = 63).
Not at all 0%.
Not at all 0% and a little 0%.
Survey Administration
In mid-November 2024, an email invitation was distributed to 175 school nurses and school nurse administrators who participated in the Program from 2016 to 2024, inviting them to complete the survey with one reminder email. Data collection occurred over three weeks. Fifteen emails were returned as undeliverable. A total of 63 participants responded and completed the survey, yielding a 39.4% response rate. The median time of survey completion by participation was 14 min.
Survey Analysis
Descriptive statistics were used to describe sample demographics and responses to survey questions. Frequencies were calculated for all qualitative variables to characterize participant responses across key program domains. Statistical analysis was conducted using the Statistical Package for the Social Sciences version 29.0 software (SPSS, Chicago, Illinois). Qualitative analyses of open-ended questions were conducted using the Braun and Clarke (2006) thematic analysis method to identify patterns across responses. Consistent with the exploratory nature of the study, reporting was limited to the most commonly occurring themes, illustrated with representative quotations.
Results
Sample Demographic Characteristics and Program Participation
As indicated in Table 1, most respondents were female (85.7%, n = 54), white and Non-Hispanic (84.1%, n = 54). Most were middle-aged, with 71.4% (n = 55) between the ages of 41–60 years old. Most respondents held a master's degree (61.9%, n = 39), were employed in public school settings (82.5%, n = 52), and practiced in the Northeast region of the United States (69.8%, n = 44). A majority of participants (69.8%, n = 44) reported completing the full Program. Participants came into the Program with diverse work roles, but the largest proportion of participants reported a direct clinical service role (42.9%, n = 27), compared to those who had school nurse administrator roles (14.3%, n = 9) or combined administrator and direct service roles (27.0%, n = 17). The majority of participants (60.3%, n = 31) received funding from school districts and/or state grants to participate in the Program; however, 23.8% (n = 15) paid for the program themselves.
Prior to enrolling in the Program, slightly less than half (46.0%, n = 55) were nationally certified as school nurses and more than three-quarters (77.8%, n = 49) had not participated in a leadership program for school nurses. Program delivery format varied, but the majority of respondents (74.6%, n = 47) participated virtually between 2020 and 2024, while 15.9% (n = 10) participated fully in person between 2016 and 2018, and 7.9% (n = 5) experienced a hybrid format with both virtual and in-person components during 2019.
Reaction to Education/Training (Kirkpatrick Level 1)
Survey responses were organized by Kirkpatrick Levels, along with corresponding frequencies. For clarity, the results table (Table 2) included only the most frequently selected options. Participants’ reactions to the Program were positive across multiple measures of educational outcomes and relevance. Almost all respondents reacted favorably to the Program's design, with the majority reporting “a lot” when asked the degree to which their experience in the Program was relevant to their practice (87%, n = 55). The vast majority of respondents shared that the schedule of monthly live group workshops with homework on their own was effective “a lot/somewhat” for their professional and personal responsibilities (96.8%, n = 61).
Learning (Kirkpatrick Level 2)
Participants reported substantial gains in leadership knowledge and competencies because of Program participation. For example, almost all respondents indicated “a lot/somewhat” increase in knowledge of leadership topics (98.4%, n = 62) and leadership skills (98.4%, n = 62). Participants also reported an increase in skill areas across several domains, with the most frequently cited being an increase in advocacy (74.2%, n = 46), data use (69.4%, n = 43), sharing professional expertise (69.4%, n = 43), networking (64.5%, n = 40), goal setting (56.5%, n = 35), and budget/finance/grants (54.8%, n = 34). As a result of participating in the Program, almost all reported they were “a lot/somewhat” more confident in their ability to lead improvements at work (92.1%, n = 58), greater commitment to improving student health (92.1%, n = 58), and more positive attitude about school nursing (90.5%, n = 57).
Behavior (Kirkpatrick Level 3)
The majority of respondents (89%, n = 50) reported an increase in responsibilities as a result of participating in the Program, including accepting new positions in a current or new district and joining boards of professional organizations. A large proportion indicated enhanced ability to share professional knowledge, with nearly two-thirds citing that the Program supported them to present orally (65.1%, n = 41) and in writing (55.6%, n = 35). The most common audience members for participants’ presentations were Nurses (oral: 76.2%, n = 32; written: 88.9%, n = 24), Teachers (oral: 73.8%, n = 31; written: 66.7%, n = 18), Principals/Directors/Superintendents (oral: 69.0%, n = 29; written 85.2%, n = 23), and School Boards/Committees (oral 52.4.%, n = 22; written 51.9%, n = 14). Sustained engagement with professional networks was demonstrated with more than half (55%, n = 33) sharing that they continued to network with cohort members in-person at meetings and conferences and via email and phone/video calls after the Program.
At the time of the survey, 72.1% (n = 31) of eligible participants earned the school nurse leadership digital badge from the Program's university with nearly half (48.4%, n = 15) of these nurses reporting that the badge demonstrated “a lot/somewhat” to others their commitment to leadership growth. Respondents who provided detail on how they use their digital badges (54.8%, n = 17) reported using it with their email signature (64.7%, n = 11), on their resume/CV (47.1%, n = 8), sharing it with supervisors/administrators (23.5%, n = 4), disclosing it in a interviewing/hiring process (17.4, n = 3), social media (11.8%, n = 2), and/or on a district webpage (5.9%, n = 1).
Results (Kirkpatrick Level 4)
Many participants (68.3%, n = 38) made progress on their projects, representing leading indicators for this level, even if their goals changed during their Program participation. Projects undertaken by participants covered many topic areas including: advocacy to increase school health services staffing; communication and education about health topics, insurance, and community resources with families; and nursing staff support with orientation, onboarding, and team building. A small number of participants (11.1%, n = 7) reported a salary increase with increased job responsibilities and/or change in position as a result of participating in the Program.
Thematic Analyses
When asked, “If you had a specific outcome as a result of your participation in the Leadership Academy that was not captured in this survey, please share briefly,” 15 nurses responded. The most common theme that emerged was Professional Growth related to advocacy and confidence. Highlighting the theme of professional development, one nurse wrote, I appreciated the “modeling” from school health experts as this practice has much autonomy and offers little time spent with models for newer nurse leaders. During and after the program, I prioritized working closely with the nursing staff to develop their practice, to identify their own professional goals and create career growth.
Discussion
This research is the first known to report school nurse specific leadership educational program outcomes based on the Kirkpatrick model for evaluating professional training. This study demonstrates the success of this leadership program in increasing school nurses’ and school nurse administrators’ knowledge, confidence, skills, behaviors, and results—outcomes that align with the Kirkpatrick model (Figure 1). Findings indicate that participants applied what they were learning, especially about professional growth, advocacy, and communication to improving school health services. This evaluation provides school nurses and administrators with a framework for considering how nursing continuing education can support the demonstration of professional growth on initiatives that seek to improve the health and safety of students and school communities.
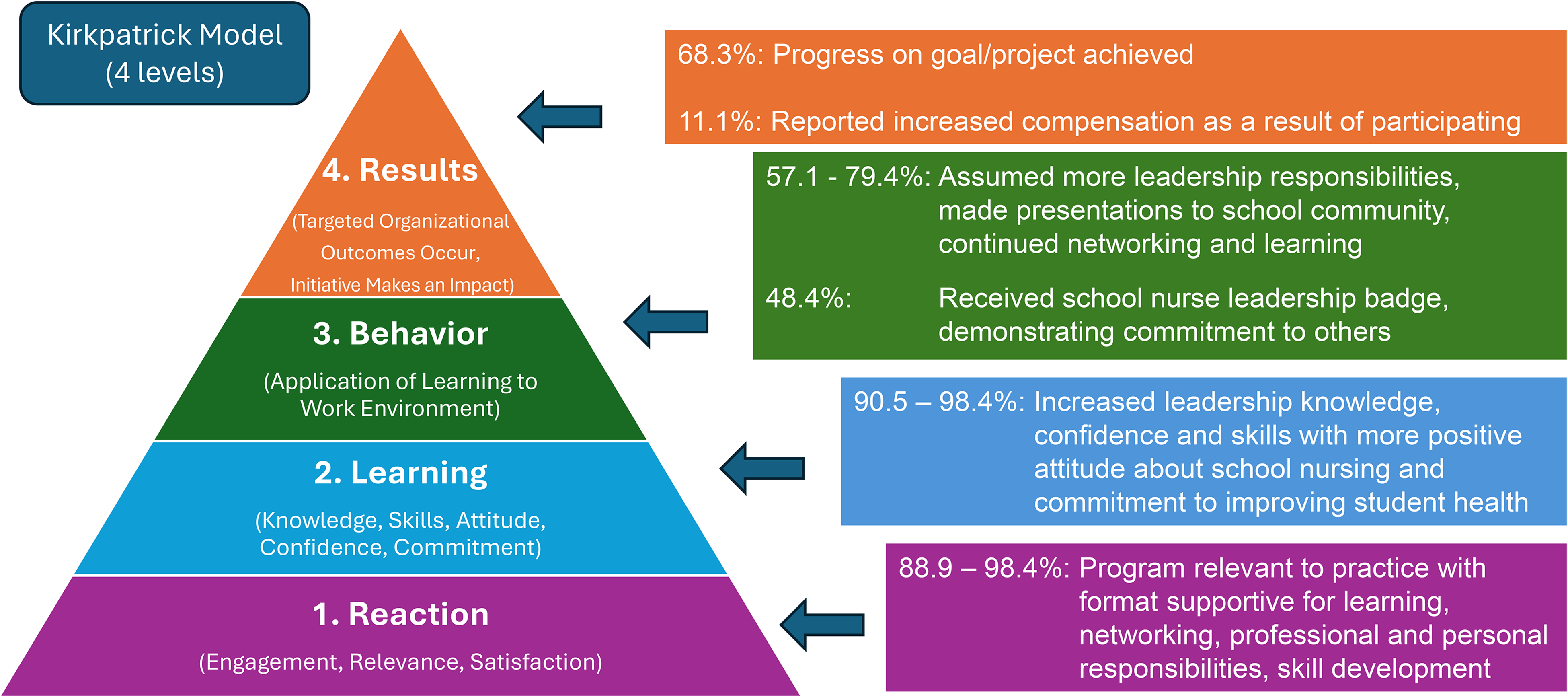
School nurse leadership program outcomes aligned with Kirkpatrick model.
In their scoping review of school nurse leadership training programs, Mazimpaka et al. (2025) identified the need for sharing program outcomes in peer-reviewed literature and suggested using the Kirkpatrick Model to evaluate program effectiveness. While researchers have noted that the first three levels in the Model are relatively easy to measure with tests, demonstrations, and self-report, the fourth level, Results, is more challenging to assess (Cahapay, 2021). Huang et al. (2025) acknowledge the lack of objective measurements of Kirkpatrick Level 4 Results. Dwyer et al. (2025) did not report on Kirkpatrick's Level 4, noting that hospital nurses who participated in their study represented a fraction of the organization's workforce and cautioned against making connections between their leadership program and changes in the hospital's performance, such as reduced costs and improved quality.
The fact that fewer participants reported or demonstrated higher Kirkpatrick Model level outcomes confirms assessment challenges and the fact that school nurses and school nurse administrators are a small fraction of the educational workforce. As a leading indicator in Level 4 of Kirkpatrick's model, progress on goals and projects was reported by more than two-thirds of participants. Nevertheless, some experienced difficulty implementing health policy and procedure improvements in school communities where educational achievement, not health, is its primary mission. Progress may be slow or even thwarted during times of public health emergencies (like the COVID pandemic), cuts in federal, state and local budgets for pre-K-12 education, and when school families and staff have polarizing opinions on how to keep students healthy, safe, and learning in school.
In this study, digital badging was categorized at the Kirkpatrick Behavior level as it demonstrated the participants’ commitment to school nurse leadership within the school community. Although digital badging has been used in other industries for many years, this concept and practice is newer to nursing: “Within nursing academia and clinical practice, [digital badging] credentials are being used to address novel needs, enhance specialized knowledge, and provide visible, shareable markers of achievement” (Graebe et al., 2025, p. 353). The Kirkpatrick Model was a useful tool for categorizing all levels of outcomes reported by participants in this novel school nurse leadership program.
Limitations
This study used a convenience sample of nurses who volunteered to participate in the school nurse leadership program and complete the survey. Although gender and race distribution in the study sample were similar to that of the U.S. school nursing workforce, differing demographics of age and geography limit the generalizability of the results (Willgerodt et al., 2024). Self-report has limitations in accuracy, especially for those who completed the Program years earlier. Other evaluation methods beyond self-report or self-evaluation should be explored for future evaluations.
Implications for Practice
Measuring Kirkpatrick Model lower levels of Reaction and Learning is very feasible with the use of pre–post assessments and evaluations for nurse educators who implement school nurse leadership continuing education programs. However, due to the nature of leadership and the dispersed settings where school nurses work, it is more challenging to measure higher Kirkpatrick Model levels of Behavior and Results. In the future, school nurse educators implementing leadership programs can seek more tangible evidence of Kirkpatrick Level 4 outcomes that align with school community educational missions, such as reports of reduced student absenteeism and increased time in classroom learning due to school nurse interventions for health challenges. Additional leading indicators for Level 4 outcomes could include increased student access to food, clothing, and health care as well as increased school health services staffing that can support student educational achievement. The focus on Kirkpatrick Model higher level outcomes would also align with the new outcomes-based continuing education (OB-CE©) Model, developed by the ANCC for nurse planners to evaluate nursing continuing professional development (ANCC, 2021).
As this leadership program draws on national standards and frameworks and has been delivered in both virtual and in person formats, it can be replicated at the local, state, and national levels with adequate resources for educators and participants provided. During a time of increased stress on school nurses and school nurse administrators, learning about this type of professional growth activity—especially if more widely available—could support engagement in the specialty and renewed excitement about the role. In turn, school community members would have new evidence of the value of school nursing leadership for supporting student health, safety and achievement.
Footnotes
Author contribution(s)
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by a donation from School Health Corporation.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Partial support for this research was provided by School Health Corporation.