
Abstract
This study explores how school nurses in Norway plan and conduct health dialogues with first graders and their caregivers. Using an exploratory qualitative design, data were generated through six focus group discussions and 10 individual interviews with school nurses from diverse contexts, including rural and urban areas, small and large communities, and varying socioeconomic and cultural backgrounds. Reflexive thematic analysis by Braun and Clarke constructed three intersecting themes: strategies for trust-based relationships, conflict between quality and quantity, and striving for consistency and professional autonomy. Results highlight the complexities of translating National Guidelines into real-world practice, emphasizing the demanding nature of school nurses’ work. The study underscores the need for clearer guidelines to support school nurses in delivering meaningful, health-promoting dialogues tailored to the diverse needs of children and their caregivers.
Keywords
Background
Schools are vital settings for promoting health and well-being, serving as a cornerstone of public health initiatives worldwide (Jourdan et al., 2021; Pulimeno et al., 2020). As environments where children spend a significant portion of their time, schools provide an opportunity to address health inequalities, foster healthy behaviors, and support children's physical and mental development. Recognizing this, the World Health Organization (WHO) started the Global School Health Initiative in 1995 to improve health in schools using a “whole-school approach,” provided by health workers within schools or through affiliated facilities (WHO, 2021). In Norway, school health services are a mandatory part of the municipal health services, provided free to pupils aged 5–20 years, offering low-threshold care with a focus on health promotion (Norwegian Directorate of Health, 2019; Norwegian Ministry of Health and Care Services, 2018). This study focuses on the first-grade health dialogue, a central feature of Norway's school health services, which fosters collaboration among school nurses, children, and caregivers to promote early intervention and well-being.
A global review found that 102 countries offer school health services; however, the content varies (Baltag et al., 2015). In Norway, school health services are easily accessible services that aim to reduce social health inequalities by addressing issues such as violence, abuse, and neglect (Norwegian Ministry of Health and Care Services, 2018). School nurses play a central role in delivering these services in Norway and other countries, such as the United States, Denmark, the United Kingdom, Sweden, Australia, and Finland (Alhammadi et al., 2024). In Norway, school nurses are registered nurses with postgraduate training in public health, qualified to deliver preventive care and strengthen connections between schools, families, and communities (Dahl et al., 2014; Glavin & Kvarme, 2024, pp. 20–59; Norwegian Ministry of Education and Research, 2021). Working independently, they are integral to the delivery of public health nursing services (Glavin et al., 2019).
A key pillar of Norway's school health services is the first-grade health dialogue, a universal, voluntary initiative conducted in the child's first year of school. This dialogue involves the school nurse, the child, and their caregivers, and includes a medical examination. Its primary goal is to establish early contact and collaboration to address the child's needs (Norwegian Directorate of Health, 2019). School nurses and doctors are advised to prepare for these dialogues by reviewing the child's medical records in advance, as outlined in the Guidelines. To ensure children with greater needs are prioritized, the scheduling of these dialogues is based on individual needs rather than alphabetical order of pupils (Norwegian Directorate of Health, 2019). Families are formally invited by school nurses, who emphasize the purpose of the dialogue. This dialogue is guided by recommendations from the Guidelines, which include suggested topics that school nurses should address. When no specific concerns are raised, nurses are advised to use the recommended topics as a framework to explore any challenges identified during the conversation and offer follow-up discussions, including referrals to other health professionals if needed. By providing a platform to address lifestyle, psychosocial, and health-related concerns, health dialogues play a crucial role in promoting the well-being of children and their families (Norwegian Directorate of Health, 2019). Early interventions like these have demonstrated long-term benefits for health, education, and lifelong outcomes (García et al., 2017).
The health dialogue is instrumental in fostering trust, which helps strengthen relationships between school nurses, children, and caregivers (Norwegian Directorate of Health, 2019). In a Swedish qualitative study, Kostenius (2023) emphasized its value in building relationships that lower barriers to seeking help. By linking trust to the health dialogue, her findings underscore its importance in creating a supportive environment for both children and families. Our study builds on these findings by exploring the practical aspects of the health dialogue in Norway, focusing on how school nurses plan and conduct these dialogues to meet children's needs. Similarly, in a Danish study, Borup (2002) described health dialogue as a “communicative room” that empowers students to make health-promoting changes. “Communicative room” refers to a dynamic and supportive space, both physical and relational, where genuine dialogue, trust-building, and health learning process can occur. Norwegian studies within school health settings also highlight the role of trust, built through sincerity, honesty, and supportive communication, especially when addressing sensitive topics (Clancy & Svensson, 2010; Laholt et al., 2017).
Health dialogues are most commonly practiced in Nordic countries, with variations in implementation, particularly regarding caregiver involvement (Borup, 2000, 2002; Borup & Holstein, 2004, 2006, 2007; Golsäter et al., 2012; Mäenpää & Åstedt-Kurki, 2008). Studies consistently underscore their value as a health promotion tool from both pupil and nurse perspectives (Harder et al., 2017; Kostenius, 2023; Laholt et al., 2017).
In Norway, these dialogues address lifestyle and psychosocial health factors, guided by the Norwegian Directorate of Health's recommendations. While the National Guidelines suggest topics like coping (handling challenges or stress effectively), relationships, sleep, nutrition, physical activity, oral health, and exposure to violence, the focus is primarily shaped by the concerns of the child and caregivers (Norwegian Directorate of Health, 2019). The recommended duration is 60 min per pupil for school nurses, and 40 min for doctors, including preparation and documentation (Norwegian Directorate of Health, 2010).
Although legally mandated, the Guidelines for School Health Services offer limited practical guidance on how health dialogues should be conducted. While the Guidelines are comprehensive, combining recommendations, best-practice documents, and regulatory requirements, their dual function as both advisory and prescriptive places considerable pressure on school nurses (Hustad et al., 2025a). Reports highlight unclear expectations and variation in practice, both in Norway (Waldum-Grevbo, 2018) and in Sweden (Golsäter et al., 2012). This ambiguity suggests a need for further research, making this study both relevant and timely.
This study aims to explore how school nurses in Norway plan and conduct health dialogues with first graders and their caregivers. By exploring the practical aspects of these dialogues in depth, the study aims to enhance understanding of their implementation and contribute to quality assurance in health-promoting efforts within School Health Services.
Methodology
Study Design
We employed an exploratory qualitative design to investigate the perspectives of school nurses in planning and conducting health dialogues with first-grade pupils and their caregivers. Data were generated through six focus group discussions and 10 individual interviews. To ensure methodological transparency and rigor, the study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Tong et al., 2007).
Participants and Recruitment
A total of 46 participants were included in the study: 36 school nurses participated in focus group interviews, and 10 took part in individual, in-depth interviews. To recruit participants, the research team (the authors of this study) identified 10 relevant regions and assigned responsibilities for contacting the heads of school health services in each municipality via phone or email. They were provided with both oral and written information about the study, including the desired number of participants for focus group interviews. These leaders then distributed the invitation and information letter to school nurses in their teams. Interested school nurses could either contact the first author directly or notify their leaders of their willingness to participate. Purposive sampling ensured information power by selecting participants with experience in health dialogues to illuminate the study's aim (Malterud et al., 2016; Patton, 2015, p. 265). Inclusion criteria required only prior experience in conducting health dialogues with first graders and their caregivers in school settings. Initially, all invited municipalities and districts agreed to participate; two later withdrew due to heavy workloads, leaving four municipalities participating in the study. Participants represented diverse professional contexts, including varying levels of professional experience and work environments across urban, rural, and suburban municipalities. Participants worked in schools with a range of population sizes and socioeconomic conditions, including those with high proportions of ethnically diverse pupils, as well as in more homogeneous school settings.
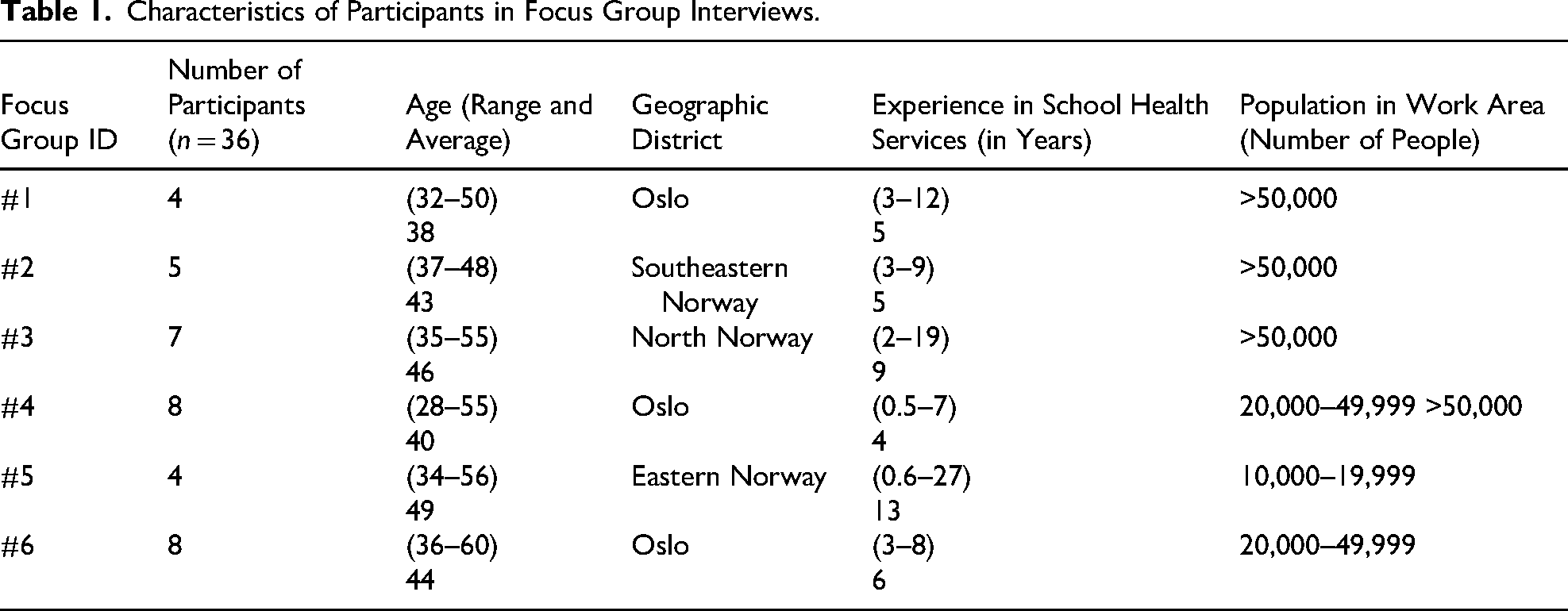
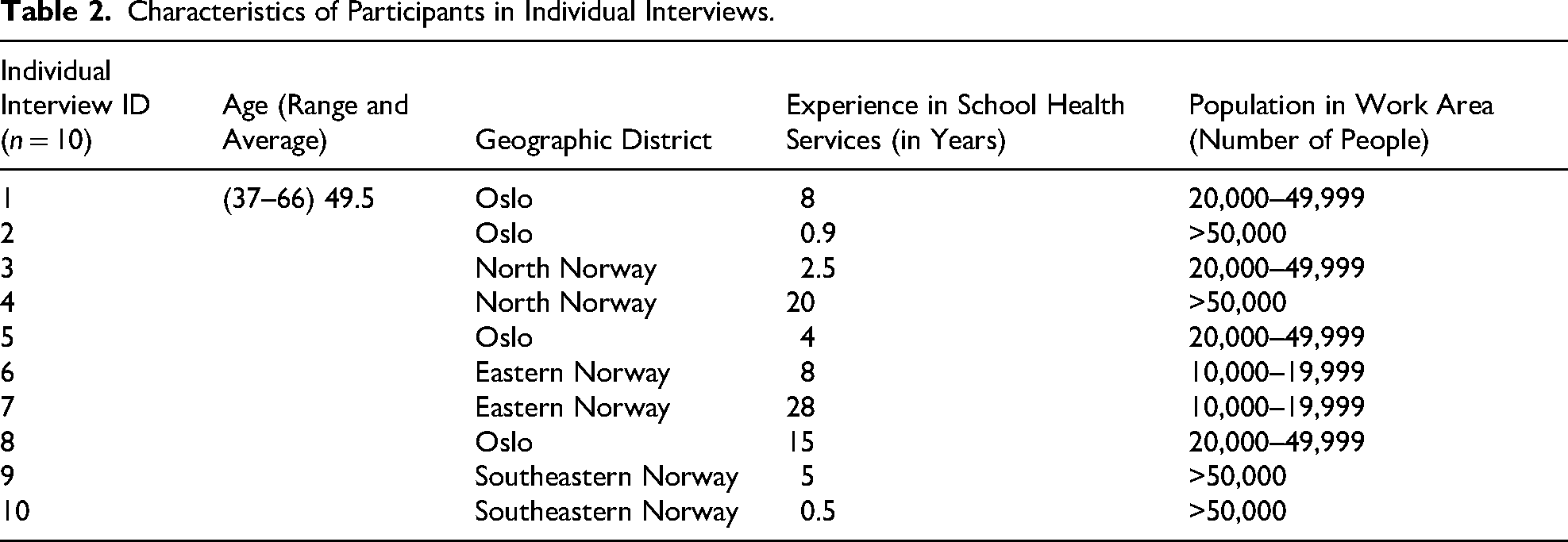
Following the completion of six focus groups, an additional invitation was sent to school health service leaders, requesting participation in individual interviews. Respondents to this invitation contacted the first author directly. Two focus group participants identified as “key knowledgeables” (Patton, 2015), were invited for individual interviews due to their extensive experience and particular relevant perspectives. All participants were school nurses, with two focus group participants in similar roles. Gender was not reported to maintain anonymity, as school nurses in Norway are predominantly women. Participants’ characteristics are detailed in Tables 1 and 2.
Characteristics of Participants in Focus Group Interviews.
Characteristics of Participants in Individual Interviews.
Recruitment was concluded when the dataset possessed sufficient information power, ensuring richness and relevance to address the study's research questions (Malterud et al., 2016). Data generation ended when new participants provided consistent accounts without introducing novel perspectives, indicating adequacy for reflexive thematic analysis (Braun & Clarke, 2006, 2019).
Setting
The study was conducted across eight municipalities and districts in Norway, representing diverse geographic, demographic, and socioeconomic contexts. Recruitment included five districts within Oslo, Norway's capital (which serves as both a county and a municipality), and three municipalities in the northern, eastern, and southeastern regions, with high ethnic diversity and differing income and education levels. To minimize disruption and encourage reflections rooted in their real-world professional contexts, focus group and individual interviews were conducted at or near participants’ workplaces during work hours. In Oslo, participants from two districts (western and southeastern) were combined into one group for convenience, and scheduling was adjusted to accommodate participants’ availability.
Data Generation
Focus Group Interviews
Six focus groups were conducted between November 2023 and January 2024, following a pilot session in September 2023 that tested the semi-structured interview guide and audio recording tool (Nettskjema Diktafon) (University of Oslo, 2025a). As the pilot provided valuable data, it was included in the study as part of the focus group results. While no changes were made to the content of the interview guide, practical adjustments were implemented, such as having participants state their participant number at the beginning of the recording to streamline the transcription process. Each session lasted 55–90 min. Discussions were moderated by the first author, while some co-authors observed group dynamics and noted non-verbal cues such as participant interactions and emotional expressions. The moderator would only step in to clarify points, move to the next topic, or steer the discussion back on track if it strayed to irrelevant topics. The semi-structured interview guide ensured that key research topics were addressed while giving participants the flexibility to shape the discussions. It featured open-ended questions exploring how school nurses plan and conduct health dialogues in their daily practice. Instances where participants introduced new ideas, expanded on each other's points, and highlighted variations in practice, both within and between districts and municipalities, were included. Focus groups were treated as analytic units where participants co-produced knowledge offering insights into organizational dynamics and collective practices. Through sharing experiences, building on each other's perspectives, and co-constructing new understandings, participants collaboratively explored challenges and practices.
Individual Interviews
Ten in-depth interviews were conducted between April and May 2024, each lasting 38–70 min. Using the same semi-structured guide, the interviews encouraged participants to reflect on specific challenges and practices and share deeper insights by including additional prompts. During these interviews, the first author actively summarized and reflected on the process, which often provided richer, co-constructed insights, such as reflections on specific dilemmas or approaches to health dialogues. All participants were encouraged to provide follow-up reflections or additional information after the interviews. Although only one participant followed up via email to share further reflections and details about their follow-up procedures this information was incorporated into the dataset to enrich the analysis.
Combined Approach
The combination of focus groups and individual interviews provided complementary perspectives. Focus groups facilitated interactive and dynamic exchanges, illuminating collective practices, while individual interviews provided personalized, in-depth accounts. This multi-dimensional approach enabled a richer understanding of the phenomenon under study.
Data Recording and Transcription
All interviews (focus groups and individual interviews) were audio recorded securely using the Nettskjema Diktafon app, which is approved by OsloMet for ethical data collection (University of Oslo, 2025a). Transcriptions captured participants’ spoken words verbatim, including hesitations and pauses, while contextual notes documented tone and emotions. Focus group transcriptions also described group dynamics, such as interactions, moments of agreement, and shifts in energy, where both the moderator and the observer were taking notes during group discussions. These contextual elements enriched the data's depth and nuance.
Ethical Considerations
The study was approved by the Norwegian Agency for Shared Services in Education and Research (Sikt) (reference number 309211) and deemed outside the scope of the Health Research Act by the Regional Committee for Medical and Health Research Ethics (REK) (reference number 2023/634692). It complied with the Personal Data Act, adhered to the Declaration of Helsinki (World Medical Association, 2025).
Participants provided informed consent after receiving detailed study information via email and in written form during interviews. Consent forms and background information were securely stored separately in a fireproof safe at OsloMet University, ensuring an additional layer of security. While interview recordings were stored in the Service for Sensitive Data (TSD) provided by the University of Oslo (University of Oslo, 2025b), ensuring data security and confidentiality.
Analytical Approach
A reflexive thematic analysis (RTA) was conducted in line with Braun and Clarke's (2022) approach, emphasizing the interpretative and iterative nature of qualitative analysis. Grounded in constructionist epistemology, the analysis explored how school nurses understand health dialogues with first-graders and caregivers. An inductive approach, grounded in the data (Braun & Clarke, 2024) was employed to actively construct patterns of meaning through a reflexive and interpretive process (Byrne, 2022), rather than relying on pre-existing theoretical frameworks.
Preliminary analysis began during data generation, with reflective memos capturing observations of interactional dynamics, data patterns, and areas for further exploration. These reflections from the focus groups informed refinements to the interview guide, ensuring greater relevance and depth in subsequent individual interviews. For example, new questions about the aims and ideal practices of health dialogues were introduced. A co-researcher member of the research team assisted with clarifying idiomatic expressions to ensure accurate transcription, as the primary analyst was not a native Norwegian speaker.
Focus Groups
Focus group discussions were analyzed first to understand collective meaning-making. Familiarization (Phase 1) involved repeated listening to recordings and reviewing transcripts. While the first author served as the primary coder, some research team members independently coded one transcription each to ensure quality. The team then met to collaboratively discuss and verify the coding process, noting group dynamics, emotional responses, and patterns of agreement and disagreement. Systematic coding (Phase 2) was conducted manually in Microsoft Word, capturing both content and interactional patterns. Codes were refined iteratively and transferred to a spreadsheet to facilitate the development of subthemes and candidate themes. Codes served as heuristic tools, fostering deeper interpretation and reflection (Table 3) (Braun & Clarke, 2022, p. 288).
Examples of Sentence-by-Sentence Manual Coding Using Inductive Descriptive Codes.
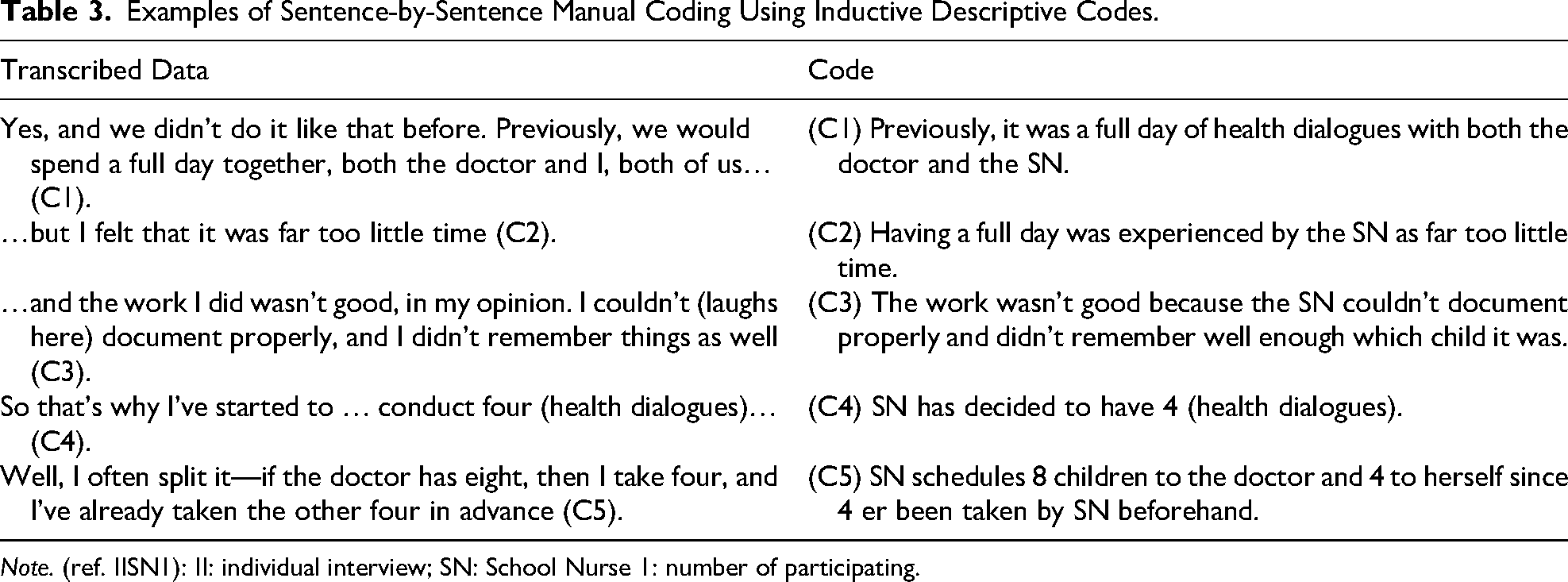
Note. (ref. IISN1): II: individual interview; SN: School Nurse 1: number of participating.
Individual Interview
Individual interviews were analyzed to provide detailed, personal insights. Familiarization (Phase 1) focused on tone, emotional expressions, and reflections on specific challenges in health dialogues. Memo-writing and note-taking captured the depth and nuance of individual accounts. Systematic coding (Phase 2) followed the same approach as for focus groups but emphasized individual experiences and context-specific nuances, ensuring alignment with the broader patterns across the dataset.
Theme Construction and Refinement
Codes from both focus groups and individual interviews were grouped into candidate themes using visual tools such as tables and mind maps (Phase 3). Themes were reviewed against the dataset to ensure coherence and consistency (Phase 4). Eight initial themes were consolidated into three overarching themes, capturing both individual and collective dimensions of school nurses’ work. Themes were defined and refined (Phase 5) through collaborative discussions within the research team. When differences emerged, such as disagreement about the boundaries or scope of certain themes, the team revisited the raw data together and engaged in reflexive dialogue to consider alternative perspectives. Final theme names and definitions were agreed upon by consensus.
The final phase (Phase 6) involved iterative writing and revision to ensure the thematic narrative was coherent, grounded in the data, and aligned with the study's aim. Terms like “almost all,” “a majority of,” or “most” indicated themes mentioned in 20–30 instances; “many,” or “often,” referred to 15–22 mentions, while “some” or “several” indicated fewer than half of the participants mentioned the theme.
Results
As shown in Tables 1 and 2, the focus group participants had an average age of 43.5 years (range: 28–60), while participants in individual interviews had an average age of 49.5 years (range: 37–66). The years of professional experience among focus group participants ranged from 0.5 to 27 years (average: 7), while those in individual interviews reported between 0.5 and 28 years (average: 9). The analysis constructed three intersecting themes: two with two sub-themes each, and one with one sub-theme. Importantly, the themes are interconnected, existing in continuous interplay where they influence and are influenced by one another in a dynamic, circular manner (Figure 1).
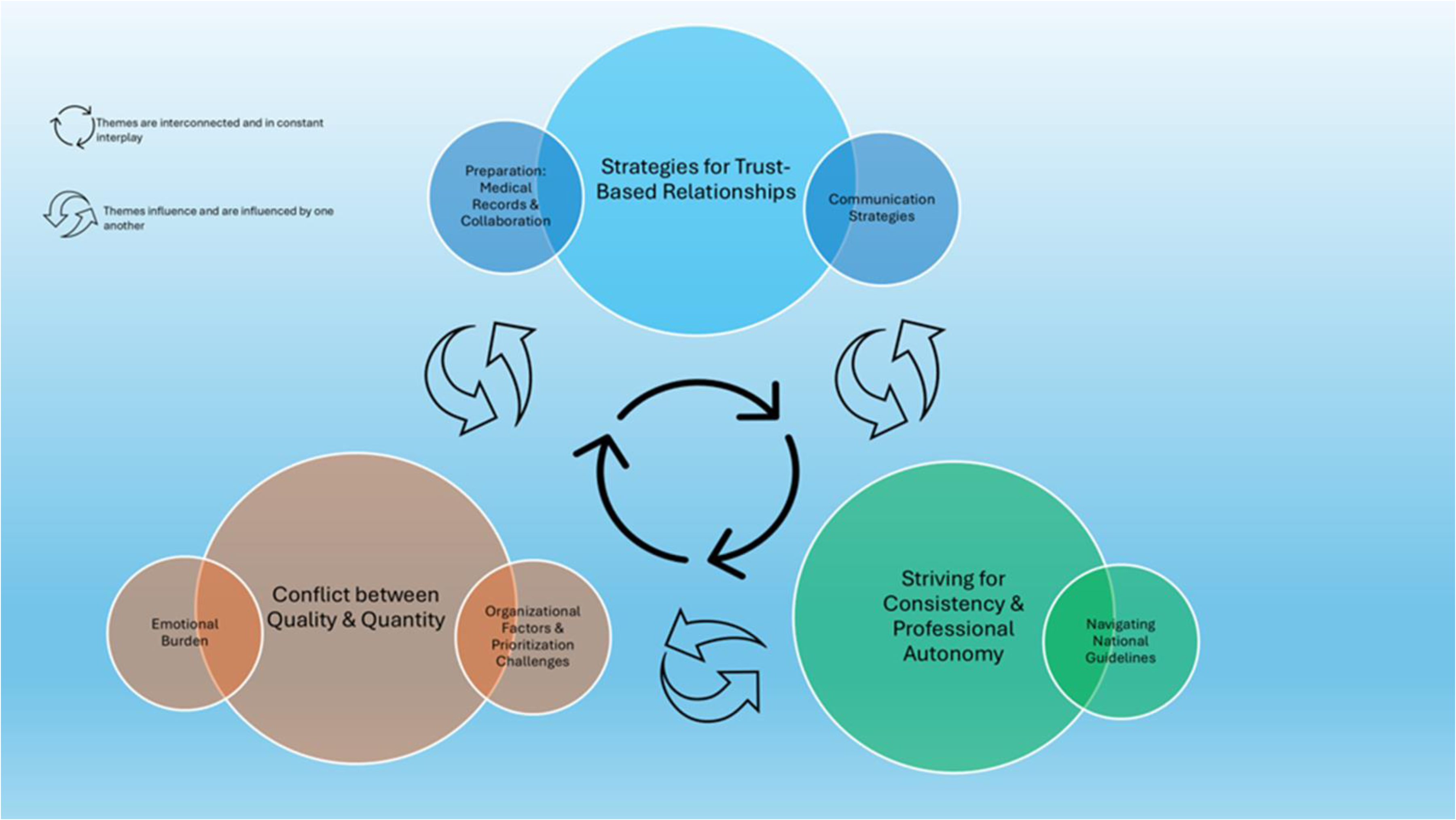
Finalized artfully interpretative constructed themes and their corresponding sub-themes.
Strategies for Trust-Based Relationships
This theme highlights how school nurses foster trust-based relationships with first-graders and their caregivers to create a supportive environment for meaningful health dialogues. It consists of two interconnected sub-themes: (1) communication strategies and (2) preparation through medical records and collaboration.
Communication Strategies
Communication strategies encompass the diverse channels, tools, and approaches school nurses use to engage with children and caregivers. These strategies include verbal and non-verbal communication, the use of digital and physical tools, fostering a welcoming environment, and maintaining a visible presence in schools to facilitate meaningful health dialogues. Almost all participants emphasized that building trust with children and caregivers is the foundation of health dialogues. A school nurse explained: I think of it as the beginning of a relationship we’ll have for the next seven years…. (Focus Group 5 Participant 1)
To achieve this, nurses employed various strategies to create a welcoming and supportive atmosphere. For example, they used visual aids, tactile tools, and child-friendly spaces to engage children during health dialogues. One nurse shared: I’ve used bear cards showing different emotions, and the children have also been allowed to draw during the health dialogue. (Focus Group 2 Participant 5)
In addition to using creative tools, many also stressed the importance of adapting communication methods to each family's context, using tools like health information forms or “backpack mail” (paper notices sent home with children) to balance standardization with flexibility. These tools ensured families were informed while creating space for individualized health dialogues. One nurse noted: I still send out what we call “backpack mail,” so they [the family] receive more comprehensive information about what the health dialogue is. I also send out a health information form for them to check off the topics they wish to discuss. (Individual Interview Participant 1)
A warm and attentive demeanor was seen as essential. One nurse explained: It’s all about welcoming, being sensitive toward the child … and demonstrating that we have plenty of time…. (Individual Interview Participant 3)
The physical environment of health dialogues was another key factor highlighted by participants. One nurse noted: The room we sit in should be inviting, tidy, and pleasant, not too close and confrontational, but not too far apart either. (Focus Group 2 Participant 1)
A majority of participants emphasized that visibility and accessibility were important prerequisites for the first-grade health dialogue. School nurses participated in key arenas, such as introduction days, the first day of school, and parent–teacher meetings, where they met children and their families, and maintained regular contact with both children and caregivers. This presence helped children experience a sense of safety and comfort during the health dialogue itself and simultaneously lowered the threshold for contacting the school nurse at a later stage. As one participant reflected: The goal is for the child to associate a face with the school nurse, feel safe, and know who they can turn to if needed. (Individual Interview Participant 2)
Building on this trust, several participants highlighted the unique role of school nurses in uncovering sensitive information not readily accessible to other professionals. As one shared: We have a pretty unique role as school nurses because there is a high level of trust in us as a professional group…. (Focus Group 4 Participant 8)
These communication strategies appeared to reinforce the role of school nurses as approachable, reliable professionals, while facilitating low-threshold access to health services for both children and caregivers.
Preparation Through Medical Records and Collaboration
Preparation was seen as a critical foundation for fostering trust and ensuring meaningful dialogues. By being well-informed, school nurses were better equipped to address the unique needs of children and families. This often involved reviewing medical records and health information forms in advance, frequently collaborating with teachers, kindergartens, and child and family health centers to better understand the child's needs. One nurse stated: I read the medical records … and then the health information forms a few days in advance, and make notes so that we’re prepared. (Individual Interview Participant 9)
Collaborating with kindergartens and schools was also described as invaluable in identifying children needing extra support, with one nurse explaining: Kindergarten has informed us in advance about which pupils have additional challenges … and we also receive that information through the school…. (Focus Group 1 Participant 3)
By combining medical records with input from stakeholders, school nurses felt better equipped to meet families’ specific needs.
The Conflict Between Quality and Quantity
This theme captures the challenges school nurses face in balancing heavy workloads with the need to provide high-quality health dialogues. It highlights how external organizational constraints influence their work, often in ways beyond their control. Two sub-themes were developed: (1) organizational factors and the challenges of prioritization and (2) emotional burden.
Organizational Factors and the Challenges of Prioritization
School nurses described how time constraints, scheduling pressures, and inconsistencies across schools and districts affected their ability to deliver high-quality health dialogues. Many expressed how conducting multiple dialogues in one day left them feeling rushed, which compromised the depth of interactions. One nurse reflected: If you have five or six of these conversations in one day, the quality starts to drop toward the end…. (Individual Interview Participant 3)
Delays in scheduling health dialogues, especially when pushed later in the school year, often exacerbate challenges for families. A participant explained: Challenges may have become even more difficult, bigger, because we’ve had to wait so long to be allowed to “enter” the family. (Focus Group 2 Participant 3)
Additionally, deviations from Guidelines and inconsistent practices between schools created frustration, as one nurse noted: Having the health dialogue around Easter or in May-June, deviates from the Directorate of Health’s Guidelines. (Focus Group 2 Participant 5)
Prioritization also posed dilemmas, as nurses had to focus on the most critical issues for each family within limited timeframes. One participant shared: You can’t cover all topics (recommended), so you have to consider what’s most important for this family…. (Individual Interview Participant 8)
Despite structured topics, many school nurses emphasized the need for follow-up conversations to address the specific needs of individual families.
Emotional Burden
Several participants described the emotional and cognitive burden of conducting multiple health dialogues under tight time constraints. Heavy workloads and time constraints left them mentally and physically exhausted, particularly on days with up to 10 or 11 back-to-back sessions. One nurse shared: You’re expected to show up fully present for each one, but you don’t even have five minutes in between. (Individual Interview Participant 2)
Another participant admitted: By the 7th or 8th conversation in a day, you start to feel a bit strange in your head. (Focus Group 5 Participant 1)
The inability to adequately prepare for dialogues due to time pressures added to the emotional strain. Nurses expressed frustration about entering conversations without reviewing medical records, as one said: Sometimes there simply isn’t time [to read medical records] … and it leaves a bit of a bad feeling … like a poor starting point. (Focus Group 6 Participant 7)
Often, school nurses noted that factors like tired or unprepared children further hindered the quality of health dialogues. Combined with high workloads, these challenges contributed to emotional burden and frustration. Still, most participants emphasized the need to balance organizational demands with individual needs, highlighting flexibility and professional judgment as essential.
Striving for Consistency and Professional Autonomy
This theme explores how school nurses navigate the tension between adhering to Guidelines and exercising professional autonomy to deliver meaningful health dialogues. While the Guidelines provide structure, nurses often find themselves adapting these frameworks to meet the practical realities of their work. The sub-theme, navigating National Guidelines illustrates how nurses actively balance these demands, often blending formal procedures with informal and flexible approaches to meet the diverse needs of children and families.
Navigating National Guidelines
Most school nurses emphasized the challenge of delivering meaningful health dialogues within the constraints of Guidelines, which they described as comprehensive yet lacking practical tools for implementation. One participant reflected: There are Guidelines that say we must cover this [violence and sexual abuse] … but nothing about how we’re supposed to do it. It’s a lot, but we’ve developed tools locally … But … I miss a national framework…. (Individual Interview Participant 3)
This lack of guidance often left nurses relying on their professional autonomy and local adaptations, which required significant effort and creativity. Another nurse shared: We’re constantly getting new tasks … these Guidelines are pretty packed [pointing the National Guidelines]…. (Individual Interview Participant 8)
While many appreciated the autonomy to adapt their practice, some expressed frustration at the lack of evidence-based tools to guide their work. As one nurse explained: We have an enormous amount of freedom to just work as we want … but I want things to be more evidence-based. (Individual Interview Participant 3)
Professional autonomy allowed nurses to prioritize the needs of individual children and families over rigid adherence to standardized topics. One participant shared: I don’t stress about covering all the recommended topics. If I notice the child is no longer engaged, I don’t drag out the conversation. (Focus Group 1 Participant 4)
This autonomy was seen as essential for fostering trust and ensuring that dialogues remained meaningful and relevant to each family's context.
To manage high workloads, many school nurses relied on formal tools, such as checklists, topic guides, and visual aids, to ensure consistency and alignment with Guidelines. At the same time, they valued informal collaboration with colleagues to share ideas and adapt tools to fit the unique needs of children and families. One participant explained: We have formal procedures, but we also share informal tools, like pictures and conversation cards, among colleagues…. (Focus Group 2 Participant 1).
However, the volume of forms and the time required to adapt them to specific contexts were sources of frustration. As one nurse remarked: There are so many forms … I’m constantly developing forms and adjusting them to fit…. (Individual Interview Participant 8)
Most participants emphasized the need to balance structure with adaptability. Standardized tools ensured consistency, while informal sharing and personalized adaptations enhanced practice. This blend enabled school nurses to deliver efficient, meaningful health dialogues tailored to each child and family.
General Discussion
The analytical approach constructed three main intersecting themes: strategies for trust-based relationships, the conflict between quality and quantity, and striving for consistency and professional autonomy. This study included participants from diverse geographical, socio-economic, and professional contexts, which provided a comprehensive perspective on how school nurses adapt to various social and cultural environments.
Strategies for Trust-Based Relationships
The study found that school nurses prioritized building trust-based relationships during health dialogues with first graders and their caregivers. They used various strategies, both in preparation and during the conduct of health dialogues, to foster trust. This focus aligns with previous research emphasizing the importance of caring relationships in public health nursing (Glavin et al., 2014) and the role of meaningful relationships over rigid systems in driving school improvement (Bragg, 2007, pp. 659–680). A key finding was the importance of creating a supportive and interactive environment that encourages openness and engagement during health dialogues. This can be understood in light of the model of a “communicative room” (Borup, 2002), which emphasizes the need for reflective openness, authenticity, competencies, and environmental support to build trust and facilitate meaningful communication. School nurses in our study demonstrated these elements by tailoring their communication strategies to each family's needs. In a Norwegian qualitative study, Nygård et al. (2024) similarly emphasized the value of close collaboration within schools as a key factor for effective public health nursing. In our study, school nurses actively informed pupils and parents about available services, such as the health dialogue, often through classroom visits and parent–teacher meetings. These practices supported communication by fostering familiarity and approachability, which were important for building trust. A quantitative study from Switzerland (Pfiffner et al., 2023) also highlighted trust as a key facilitator in help-seeking behaviors among pupils. Their findings suggest that trust, positive prior experiences, and accessibility are critical for encouraging younger children to seek support, underscoring the importance of established relationships between professionals and pupils. However, findings from Clancy and Svensson (2009), a Norwegian qualitative study, and Mäenpää and Åstedt-Kurki(2008), in a qualitative Finnish study, highlighted that greater efforts may be needed to ensure school nurses remain visible and accessible to all pupils and families. Preparation and collaboration were also highlighted as essential components of building trust. Reviewing medical records and providing caregivers with health information forms helped nurses tailor conversations to families’ needs. In their mixed-methods study, Sagatun et al. (2021) found that web-based tools effectively supported personalized health dialogues in similar contexts. Swedish studies (Golsäter et al., 2014; Harder et al., 2017) emphasized the balance between directive approaches (providing information) and child-centered strategies that encourage active participation.
School nurses in this study also used visual tools, such as cards, pictures, toys, and drawings, to engage children and encourage dialogue. Visualization techniques have been shown to foster relationships, identify at-risk groups, and create space for participation by both children and parents (Håkansson et al., 2019; Laholt et al., 2017). Finally, our findings align with Kostenius (2023), who emphasized that health dialogues build strong relationships and reduce barriers to seeking help. Participants in our study likewise stressed the importance of creating a welcoming environment where children and families feel comfortable returning if needed.
The Conflict Between Quality and Quantity
Our findings revealed that organizational factors significantly affected the quality of health dialogues, with school nurses reporting challenges such as rigid scheduling and conducting multiple sessions daily. These constraints often lead to a focus on quantity over quality. Similarly, Kostenius (2023) highlighted the impact of limited time, administrative tasks, and large caseloads on the quality of school nurses’ interactions. Waldum-Grevbo (2018) reported that only 48.7% of school nurses provided both a school nurse and a doctor during the health dialogue, and just 11.4% included a doctor's examination, reflecting inconsistencies across municipalities. Our findings align with these results, illustrating how structural constraints shape school health services. Participants described conducting up to 10–11 health dialogues daily for consecutive weeks, which left them physically and emotionally drained, limiting their ability to focus on individual needs. This finding echoes Borup (2000), in a Danish qualitative study, who identified sufficient time as critical for successful health dialogues, and Kostenius (2023), who reported that overwhelming workloads undermined the quality of nursing practice. The emotional burden was a prominent theme, as school nurses expressed feelings of inadequacy when time constraints hindered preparation. In a qualitative Norwegian study, Dahl et al. (2014) found that public health nurses faced ethical dilemmas in balancing institutional demands with prioritizing children's well-being. Practical barriers, such as noise and interruptions, further exacerbated these challenges. Kostenius (2023) noted that such disruptions negatively affected communication, while Jameson and Bowen (2020) observed that high workloads placed American school nurses at risk of emotional exhaustion and burnout. The high demand for school health services is further reflected in Norwegian studies. Nygård et al. (2024) discussed how school nurses’ flexibility complicates balancing competing demands in high-pressure environments, while Hustad et al. (2025b), in a quantitative study, found that administrative duties consumed significant time, reducing opportunities for direct interaction with students and families. Together, these studies highlight the demanding nature of school health services and the strain they place on nurses. Despite these challenges, participants demonstrated remarkable adaptability in managing competing demands. Ultimately, our findings emphasize that the tension between quality and quantity is not a binary issue of “good” versus “bad” practice; rather, it is a spectrum that requires careful navigation. While structural constraints often hinder the delivery of ideal care, school nurses consistently prioritize trust-based relationships and the well-being of children and their families.
Striving for Consistency and Professional Autonomy
Our findings underscore the tension school nurses face between adhering to Guidelines and exercising professional autonomy to tailor health dialogues to the specific needs of children and families. While Guidelines provide structure and consistency, participants emphasized the importance of autonomy to address real-world complexities. This challenge is echoed by Reuterswärd and Lagerström (2010), who found in a Swedish qualitative study that experienced school nurses often moved beyond protocol-driven practices to adopt student- and family-centered approaches. Similarly, Reuterswärd and Hylander (2017), in another qualitative study, argued that professional autonomy allows school nurses to interpret Guidelines in ways that prioritize the individual needs of children and families, rather than rigidly adhering to prescribed protocols. Our findings underscore the need for clear but adaptable Guidelines to support meaningful, tailored care.
Autonomy was a central theme in our results, with participants describing their efforts to balance independence with the need to align their work with the national standards. However, participants reported a disconnect between the recommendations in the Guidelines and their practical implementation. Hustad et al. (2025a) found that 53% of school nurses considered the Guidelines unclear, with nearly half reporting being unable to meet their outlined responsibilities. Another study by Hustad et al. (2025b) revealed that the school nurses’ prioritization of tasks varied significantly, shaped by individual and contextual factors. These findings raise questions about whether the Guidelines themselves create barriers or if the inherent flexibility of school nursing leads to inconsistencies in practice.
The challenge of balancing mandatory tasks with individualized care is well-documented in the literature. Golsäter et al. (2014) described health visits within national health programs as complex and challenging, while Midtsund et al. (2023), in a qualitative study, found that time constraints often force public health nurses to prioritize mandatory tasks over family concerns. Harder et al. (2017) emphasized that nurses frequently act flexibly to meet program demands, which may limit focus on individual needs. Similarly, in an English qualitative study, Hoekstra et al. (2016) noted that school nurses often struggled to manage their responsibilities within tight schedules. In our study, participants developed individualized tools and procedures to navigate these challenges, reflecting their resourcefulness in balancing competing demands. Hoekstra et al. (2016) observed school nurses balancing immediate concerns with limited resources, often collaborating with colleagues or developing informal tools to streamline health dialogues. Similarly, our participants adapted their approaches by tailoring health dialogues to individual needs, using forms for caregivers to highlight concerns or prioritize topics. These strategies reflect school nurses’ ability to navigate systemic constraints while addressing both formal expectations and the unique needs of children and families. This duality between Guidelines and autonomy is a defining characteristic of school nursing in our study. While Guidelines ensure consistency, professional autonomy is essential for adapting health dialogues to the unique needs of children and families. Autonomy is a valued aspect of public health nursing, as highlighted by Foley et al. (2004), in an American study, and Federici et al. (2021) in a Norwegian report, who identified it as a key element of school nurses’ professional identity and job satisfaction. Dahl et al. (2014) similarly emphasized the pride public health nurses take in advocating for the well-being of children and families. Participants in our study echoed these sentiments, prioritizing the most pressing concerns of families over rigidly adhering to every guideline. Experience played a key role in enabling school nurses to move beyond protocols, fostering meaningful, family-centered care.
Implications for School Nursing and Future Research
The findings of this study have implications for school nursing practice, policy, and future research. When trust is established, as emphasized in our study, children and caregivers are more likely to feel safe, express themselves openly, and seek support when needed (Pfiffner et al., 2023). School nurses can strengthen trust by actively creating a welcoming and safe environment by fostering sensitivity, sincerity, and open communication (Kostenius, 2023; Laholt et al., 2017). Short-term actions, such as ensuring a visible presence in schools and using child-friendly tools like drawings and toys, can enhance engagement and reduce barriers to seeking help.
At the policy level, the findings highlight the need to address systemic constraints that limit school nurses’ capacity to conduct effective health dialogues. Time pressure and resource shortages, identified in both the present study and by Hustad et al. (2025c), influence the quality of care. This underscores the need for increased investment in school health services to reduce workloads, enhance collaboration, and provide resources that enable school nurses to balance quality and quantity. Without addressing these systemic challenges, the conflict between organizational demands and meaningful care will persist, limiting the potential of school health services to deliver lifelong outcomes. Policymakers should revise the National Guidelines to include clear, evidence-based, and practical tools that guide nurses in delivering consistent and effective care. Standardizing tools, particularly for addressing sensitive topics like violence and abuse, while allowing for flexibility in local adaptation, will reduce disparities and support school nurses in balancing professional autonomy with consistency.
Future research should focus on evaluating which tools and methods are most effective in facilitating meaningful health dialogues. Additionally, studies should prioritize amplifying the voices of caregivers and children to gain deeper insight into their experiences and ensure that health dialogues are adapted to meet their specific needs. These efforts will ensure school health services are evidence-based, equitable, and responsive to the diverse needs of children and families.
Limitations
This study provides valuable insights into how school nurses plan and conduct health dialogues with first graders and their caregivers. While the inclusion of participants from diverse geographical, socioeconomic, and professional contexts enhances the transferability of findings, the relatively small sample size and focus group dynamics may have limited the range of perspectives and the sharing of sensitive experiences. Additionally, the findings are specific to the Norwegian school health system, which may limit their applicability to other countries. While reflexivity was maintained, participants’ responses may have been influenced by the researchers’ professional background or perceived power dynamics.
Conclusion
This study constructed three key themes: strategies for trust-based relationships, the conflict between quality and quantity, and striving for consistency and professional autonomy, which highlight the complexities of school nursing. The findings highlight trust as a necessary condition for health dialogues, fostered through school nurses’ communication and supportive environments. However, organizational challenges, such as time constraints and administrative demands, often force nurses to balance competing priorities, which may influence the quality of care. Despite these challenges, nurses demonstrated remarkable adaptability by developing individualized approaches to meet both systemic expectations and the needs of children and families.
The findings also underscore the tension between adhering to Guidelines and exercising professional autonomy, with nurses emphasizing the importance of flexibility to address real-world complexities. While Guidelines provide structure and consistency, professional autonomy allows nurses to prioritize individualized care, which is essential for meaningful health dialogues. These results highlight the need for clear yet adaptable Guidelines, increased investment in school health services, and systemic changes to reduce workloads and support both quality and quantity in care delivery. Addressing these structural barriers is essential to ensure that school nurses can continue to enhance health outcomes and promote the well-being of children and their families.
Footnotes
Acknowledgments
The authors wish to express their sincere gratitude to all the participating school nurses for making this study possible and for their invaluable contributions during the interviews. Without your input, this study would not have been possible. The authors also extend their gratitude to Merete Waage Hanssen-Bauer, head of the Child and Health Center and School Health Services in the Grünerløkka district, for her support with recruitment and her significant contributions to the research project.
Author Contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Grünerløkka District and the Norwegian Research Council.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.