
Abstract
A mixed methods design drawing on Bioecological Systems Theory was used to explore primary school-aged children, parents, teachers, and school nurses’ experiences and understanding of school nurses’ mental health work. Phase One involved administration of a national cross-sectional online survey of nurses working in the school health service in Scotland (N = 83). Phase Two employed a Single Qualitative Case Study in one Scottish health board area. Online semi-structured interviews were conducted with school nurses, primary school-aged children (9–11 years), parents and teachers (N = 23). Creative, participatory methods were used in the interviews with children. The findings identified that despite a refocus of the school nurse role in Scotland to maximize their contribution, their role lacks visibility, and their mental health work is reactive rather than proactive and preventive. This research suggests that their role and remit should be included and clearly articulated in whole-school approaches to mental health.
Keywords
Mental health problems in children and young people (CYP) are a global public health issue and national priority across the United Kingdom (UK). Globally, it is estimated that 10–20% of children and young people will experience a mental health problem with half of these developing before the age of 14 (World Health Organisation, 2022). In Scotland, within an average classroom of 30 children, about three will have experienced a mental health problem by the time they reach the age of 16 (Scottish Children's Service Coalition, 2023). Despite this, CYP experiencing mental health problems are not receiving support early enough and there are long waiting lists for Child and Adolescent Mental Health Services (Public Health Scotland (PHS), 2023). While there is some evidence suggesting that school nurses (SNs) could make a significant contribution to supporting children's mental health (Jonsson et al., 2019; Pryjmachuk et al., 2012), few empirical studies have focused on their contribution to supporting primary-school-aged children's mental health. This research adds an original understanding from the perspective of school nurses, primary-school-aged children themselves, parents and teachers in Scotland. The findings are significant because they point to the need for school nurses to be working in schools and communities as part of a whole school approach to promote good mental health.
Background
Globally, the educational qualifications required to practice as a school nurse vary with some countries requiring an additional postgraduate qualification (Skundberg-Kletthagen & Moen, 2017). Within the UK, school nurses are Nursing and Midwifery Council (NMC) registered nurses or midwives who have completed additional post-registration qualifications, usually at Master's level to register as a Specialist Community Public Health Nurse-School Nurse (SCPHN-SN). They work in partnership with CYP aged 5–19, their families and professionals in education, health and other agencies to identify and address health and wellbeing needs and uphold their rights. In Scotland, school nurses work in integrated community nursing teams to deliver the School Nursing Service Pathway, which comprises 10 public health priority areas. The priority areas include emotional/mental health and wellbeing, substance misuse, child protection, domestic abuse, looked-after children, homelessness, sexual health and wellbeing, pregnancy and parenthood, youth justice, young carers and transitions (Scottish Government, 2018). The school nurse role was refocused to facilitate early intervention and support for vulnerable CYP identified at primary school entry with health and wellbeing needs.
According to PHS (2022), the most common mental health issues affecting CYP in Scotland are anxiety, depression, self-harm and conduct disorders. The Mental Health of Children and Young People in England 2022 survey (Newlove-Delgado et al., 2022) revealed that the rates of probable mental health disorders in children aged 8–16 years had increased from 12.1% (one in nine) in 2017 to 16.7% (one in six) in 2020, and in 2023 the rate had increased to 20.3% (one in five) (National Health Service (NHS) England, 2023). Although there is no comparable data for Scotland, Wales or Northern Ireland, the national statistics for Scotland have highlighted significant increases in the number of referrals of children and young people to the Child and Adolescent Mental Health Service (CAMHS) since December 2021 (PHS, 2023). These statistics suggest that, in common with England, the prevalence of mental health disorders in children aged 8–16 years has increased which is concerning, given the implications of poor mental health on the outcomes for CYP across the life course.
The aim of this study was to explore primary-school-aged children's, parents’, teachers’, and school nurses’ experiences and understanding of the mental health work of the school nurse; and to identify their contribution to supporting and improving children's mental health. The research questions were:
How do children, parents, teachers and school nurses currently experience and understand the work of the school nurse in supporting primary-school-aged children's mental health? What factors influence their experiences and understanding? How do their experiences and understanding inform the future work of the school nurse in supporting primary-school-aged children's mental health from an ecological and strengths-based perspective?
Research Design
An explanatory sequential mixed methods design comprising of two phases was used to address the study aim and research questions (Creswell & Creswell, 2018). The theoretical basis drew on Bioecological Systems Theory, in particular the Person-Process-Context-Time (PPCT) Model (Bronfenbrenner, 1995), which provided a lens to view school nurse practice. Gaining an understanding of the influence of social relationships and support networks, particularly in relation to the mental health work of the school nurse, were key to addressing the research aim and questions. The principles and four key elements of Bioecological Systems Theory informed each stage of the research process. For this study, the elements were defined as: Person refers to the school child aged 9–11 years and their parents, and the school nurses delivering school nursing services in their area. Process refers to the quality of the interactions between the school-aged child and the school nurse, their parents, and the teacher and how they can support the child's mental health in school, home and community. Context refers to the child's wider world, which includes school, home and community. Time refers to the socio-historic time period, and at the time of Phase Two, Scotland was in the midst of a global pandemic.
Methods
Phase One involved administration of a national cross-sectional online questionnaire to registered nurses and midwives, herein referred to as registrants, working in the Scottish NHS school health service. The purpose of this phase was to scope out their current work in supporting primary school-aged children's mental health and inform selection of case for the qualitative phase. Phase Two was a single qualitative case study which was embedded within the core explanatory sequential mixed methods design in a complex adaptation for Mixed Methods-Case Study Design (MM-CS) (Guetterman & Fetters, 2018). This phase enabled the phase one results to be explained and to provide a more in-depth, nuanced understanding of school nurse's work supporting primary school children's mental health. To assure the quality and robustness of the research, the four criteria suggested by Bryman (2008) and a reflexive approach were employed.
Ethical Approval
Ethical approval was granted from the University of Stirling Ethics Committee (NICR 17/18—Paper No 053 and NICR 18/19—Paper No. 039) and the relevant access permissions from Executive Nurse Directors and Education Departments. NHS Research Ethics Committee approval was not required as the study was deemed to be Service Evaluation.
Settings
The study was conducted in Scotland. Phase Two was conducted in one NHS health board in central Scotland where the school nursing team (the case) delivered their service to schools in three Local Authority Education Departments. This case was selected for two reasons. First, the results from Phase One, highlighted that in this health board area, only registered SCPHN-SNs were using the title—“School Nurse,” which contrasted with some other board areas. Second, this health board had implemented the Emotional/Mental Health and Wellbeing priority area and pathway (Scottish Government, 2018). These were especially relevant to address the research aim and questions.
Study Population
Phase One
The whole population of registrants working in the Scottish School Health Service in September 2018 were invited to participate (n = 281.4 whole-time equivalents) (NHS Scotland, 2018). Registrants working in independent schools were excluded as their role and remit varies from those working in the NHS School Health Service. Recruitment to the study was via email, information pack and a link through a lead person in each board area. Respondents were required to provide informed consent at the beginning and end of the questionnaire.
Phase Two
Participants were purposefully selected. They included school nurses, primary-school-aged children, parents and teachers who met the inclusion criteria: registered SCPHN-SN working in the Scottish School Health Service; Primary School Teacher working in a Scottish local authority primary school; Parent of a child aged 9–11 years enrolled in a Scottish local authority primary school; Child aged 9–11 years enrolled in a Scottish local authority primary school. This age range was selected in response to feedback from the Teacher's Advisory Group who suggested the children would be more comfortable and capable being interviewed. To ensure diversity, a sample matrix was developed to ensure representation from different genders and ethnicities. The final sample included six school nurses, five women and one man, all were white; two teachers, one woman and one man, both white; three girls and five boys, seven were white and one was Asian; six mothers and one father, six were white and one was Asian. School Nurses were recruited via email invitation and information pack through the Lead for School Nursing. Permission to recruit children, parents and teachers through the Head Teacher in one local authority primary school was obtained and fieldwork planned for March 2020. However, due to COVID-19, access to schools was not permitted. To ensure the views of children, parents and teachers were included, ethical permission was obtained to use university networks for recruitment. The recruitment email and announcement clearly identified the case boundary and inclusion criteria. Information packs and consent forms were emailed to teachers and parents to share with their child. Written voluntary informed consent to participate was sought from teachers and both child and their parent and reconfirmed prior to commencing the interviews. To safeguard children, they were offered the opportunity to have a parent or trusted adult present during the online interviews. The researcher was a registered nurse and trained in Advanced Interviewing Skills with Children and had completed the Talking Mats™ Foundation training. The Talking Mats Consulting Children and Young People Resource was used with permission from Talking Mats Ltd.
Data Collection
Phase One
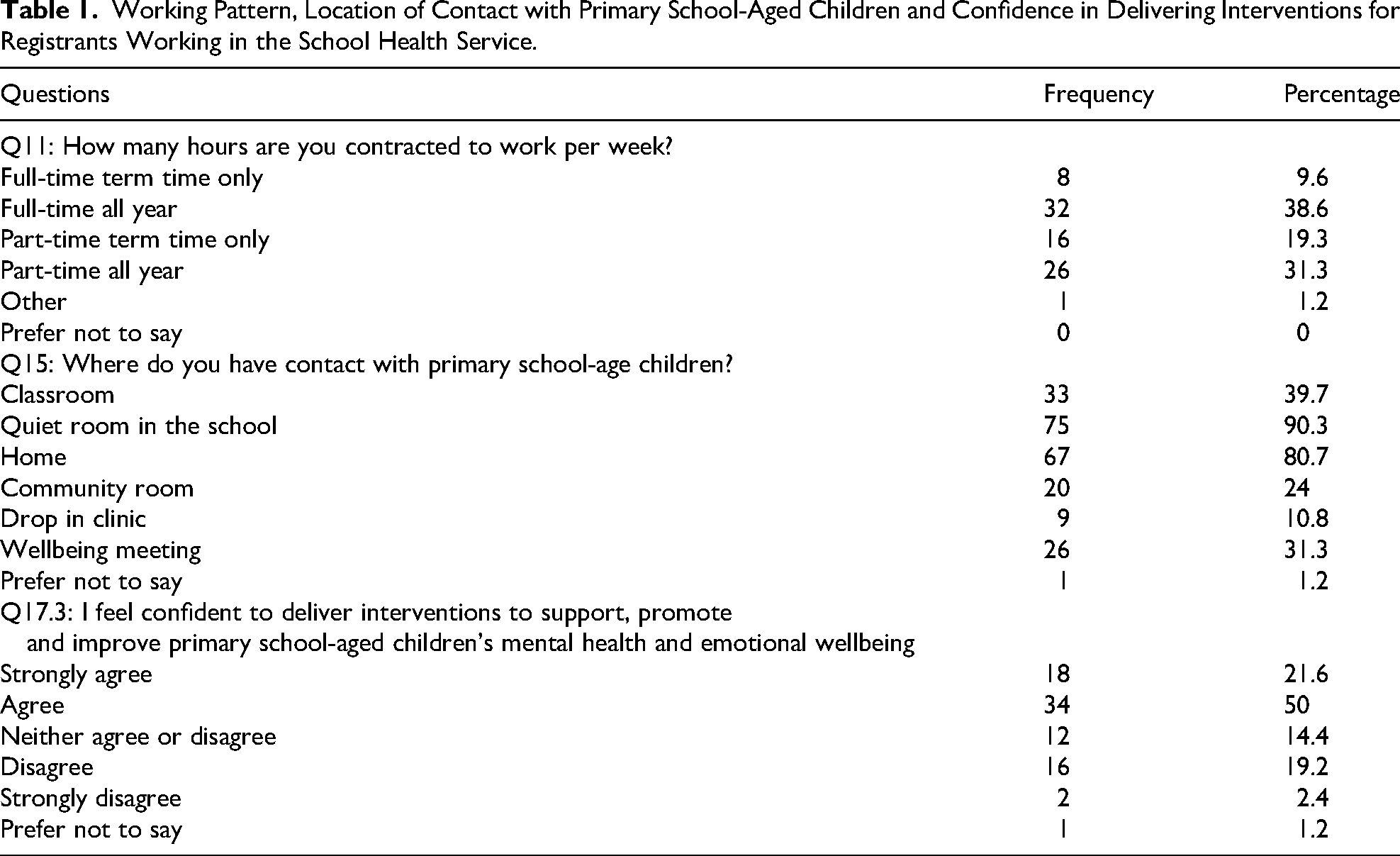
Data were collected between September and November 2018 using an online questionnaire that was designed using the online survey tool, Online Surveys (Jisc, 2024). This tool is fully compliant with the UK General Data Protection Regulations (2018). The questionnaire was distributed via an anonymous web-based link via a lead person in each board area. It comprised 26 questions grouped under five sections which were informed by the scoping review of the literature which sought to identify what is known about the school nurses’ role in supporting primary-school-aged children's mental health, and the research questions. Sections 1 and 2 were designed to obtain demographic data and comprised closed questions. There was also the option to tick “other” for Questions 3, 5, and 7 should respondents identify with a different gender, have a different professional qualification, or different level of qualification. Sections 3, 4, and 5 were designed to obtain data exploring respondent's experiences and understanding of their role and mental health work and comprised a variety of types of questions, for example, a Likert Scale, multiple choice with multiple answers, and multi-line free text (see Table 1). The questionnaire was piloted by a SCPHN-SN educator and three students on a SCPHN program who had previously worked in the school health service for several years.
Working Pattern, Location of Contact with Primary School-Aged Children and Confidence in Delivering Interventions for Registrants Working in the School Health Service.
Phase Two
Semi-structured interviews were used to collect data from school nurses (n = 6), primary-school-aged children (9–11 years) (n = 8), parents (n = 7), and teachers (n = 2) between August 2020 and July 2021. A total of 23 interviews were conducted online using MS Teams, apart from one with a school nurse that took place over the telephone due to internet issues. Interviews were conducted, digitally audio recorded and transcribed verbatim by the first author, an academic nurse and doctoral student holding registration as a SCPHN
Data Analysis
Phase One
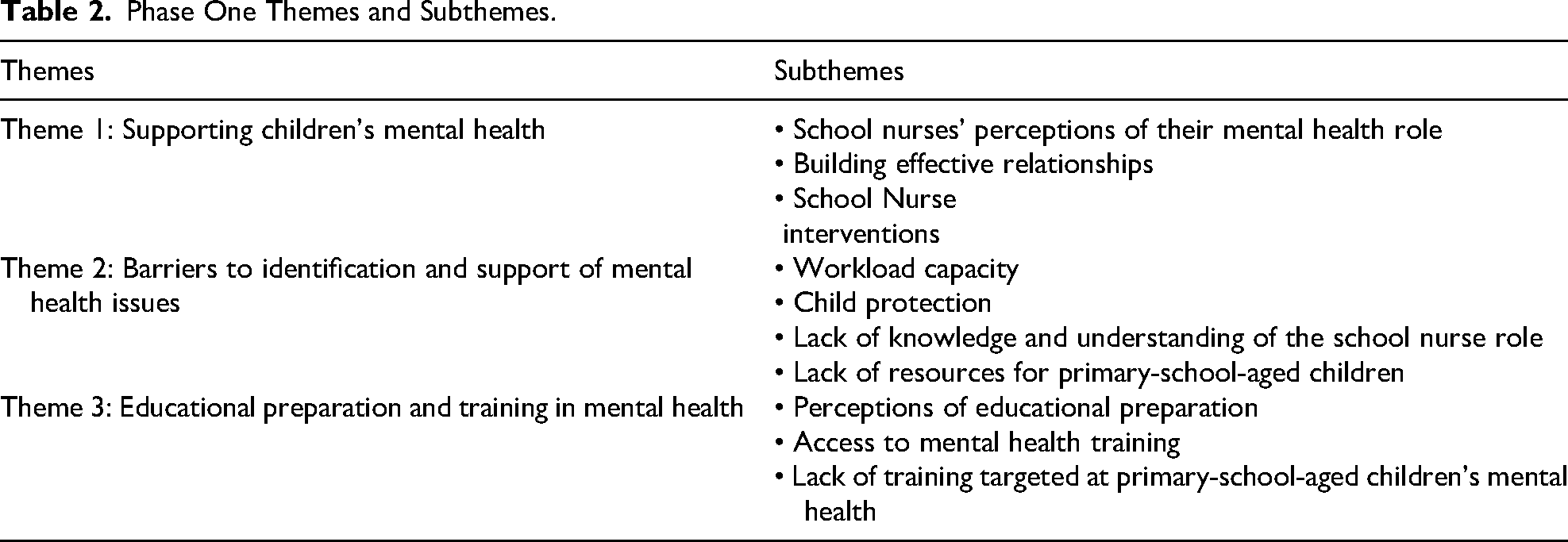
Results were exported from Online Surveys to MS Excel for descriptive analysis and presented as frequency and percentage. Free text data was managed and analyzed thematically following the five-stage process of framework analysis as outlined by Spencer et al. (2014). Stage one involved familiarization of data by reading and re-reading the responses and noting down key comments made by respondents. Stage two involved constructing a thematic framework, informed by emergent themes and questionnaire topics to aid with stage three, indexing and sorting. This stage involved reading individual responses, deciding what label(s) were relevant and applying them to segments of free text. Stage four involved developing charts and summarizing the data. The framework matrices in NVivo 12 were used to aid this. The final stage involved mapping and interpretation and development of themes and subthemes (see Table 2).
Phase One Themes and Subthemes.
Phase Two
Data was managed and analyzed thematically following the process described above. A thematic framework was constructed for each dataset to address emergent themes and interview topics. Due to intermittent issues accessing NVivo-12 when working remotely, Word was used with Tracked Changes to index and sort the transcripts and to create charts to summarize data.
Results/Findings
Phase One
The results are reported in line with the Consensus-Based Checklist for Reporting of Survey Studies (CROSS) results (Sharma et al., 2021). The four components of the PPCT Model (Bronfenbrenner, 1995) are used to situate the results.
Respondent Characteristics
Person
Most respondents were women (n = 82; 98.8%), and one (1.2%) was a man, and all described their ethnicity as white. The average age range was 45–54 years (n = 40; 48.1%). All respondents were registered nurses or midwives, but most were Registered Nurses-Adult (65%). Thirty-one (37.3%) were also Specialist Community Public Health Nurses (SCPHN), but of this number only 14 (16.8%) were registered SCPHN-SNs. Almost half had a bachelor's degree and the highest level of qualification was a master's degree. Four (4.81%) had achieved this award and 30 (36.1%) were studying at this level. Sixty-four (77.1%) had attended training in mental health, 17 (20.5%) had not and two (2.4%) did not know.
Descriptive Statistics
Context
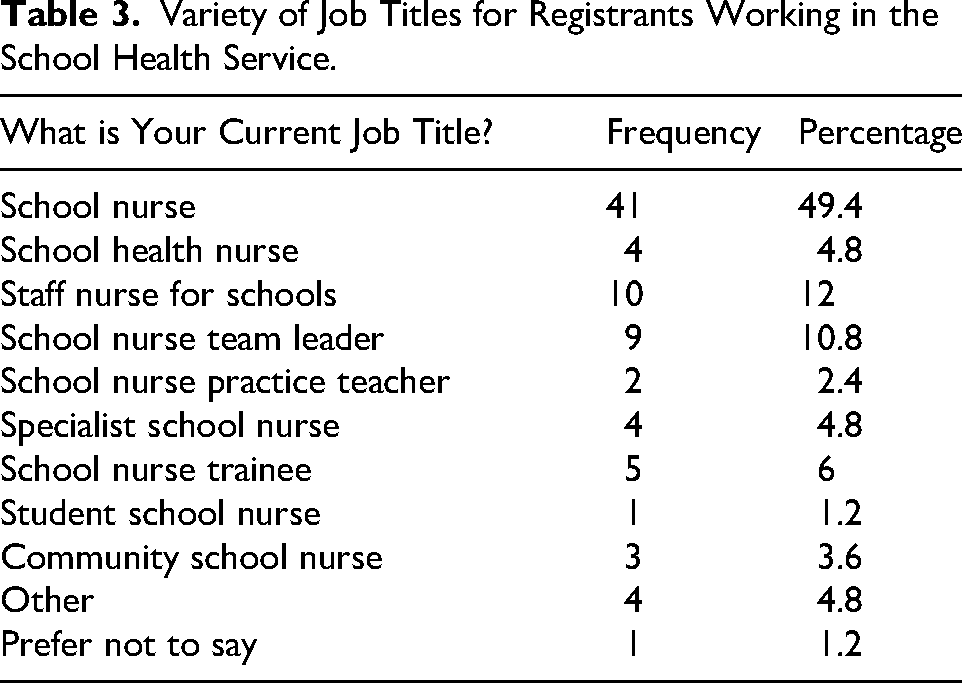
Respondents were represented from all 14 Scottish NHS Health Board areas. There were a total of 83 responses, representing a response rate of 29.5%. The largest number of responses (n = 11) was from NHS Greater Glasgow and Clyde which is the largest health board in Scotland. Respondents comprised an experienced workforce with 47 (56.6%) reporting they had worked in the school nursing service for 5 years or more. Notably, the length of experience with the largest number of responses (27.7%) was between 1 and 4 years, indicating investment in increasing the numbers of school nurses in Scotland. Respondents had a range of job titles (see Table 3), however, though only 16.8% indicated that they were registered SCPHN-SN, nearly half (49.4%) described their job title as a “School Nurse.” This served to highlight that in some Boards, the title school nurse was not confined to those who had completed a SCPHN-SN program.
Variety of Job Titles for Registrants Working in the School Health Service.
Time
In 2018, the Scottish Government were planning to implement the refocused school nurse role and priority areas and pathways (Scottish Government, 2018), and more than half of respondents (64.7%) indicated that they had been implemented in their area. Ten (11.8%) indicated that they had not been implemented in their area, and seven (8.2%) did not know. Of the 13 responding “other,” their free text comments highlighted inconsistencies and variation in implementation. A variety of working patterns was represented with just under one-third working full-time. There were a range of visiting patterns to primary schools ranging from “never visiting the school” (n = 2; 2.4%) to “other” (n = 36; 43.3%), which included a variety of reasons, such as, “as required.” The two most common locations for contact with primary school children were a quiet room in the school (n = 75; 90.3%) and the child's home (n = 67; 80.7%).
Process
Most respondents (92.8%) reported that supporting primary-school-aged children's mental health was an important part of their work. Almost three-quarters (72.3%) indicated that they were actively involved in supporting primary-school-aged children in need of early intervention. It is notable that 25 (30.1%) respondents indicated this was not the case. Respondents were asked about their confidence in delivering interventions to support, promote and improve primary school-aged children's mental health and emotional wellbeing. Although nearly two-thirds (62.6%) felt confident to deliver interventions to this age group, a notable proportion (21.7%) indicated lack of confidence.
Parenting support (76%), home visits (74.7%) and the Solihull approach (62.7%) were found to be the three main interventions used to support children's mental health (Figure 1). The Solihull Approach is an evidence-based intervention that aims to support parents to develop nurturing and responsive relationships with their child and equip them with skills to sensitively contain their child's emotions (Douglas & Johnson, 2019). Respondents were offered the opportunity to specify whether they used any other interventions. Several indicated that they used Let's Introduce Anxiety Management (LIAM), which is an intervention based on cognitive behavioral therapy to support CYP to manage symptoms of mild–moderate anxiety (NHS Education for Scotland, 2024). A large proportion (87.9%) responded that they used a person-centered and strengths-based approach when working with children and families.
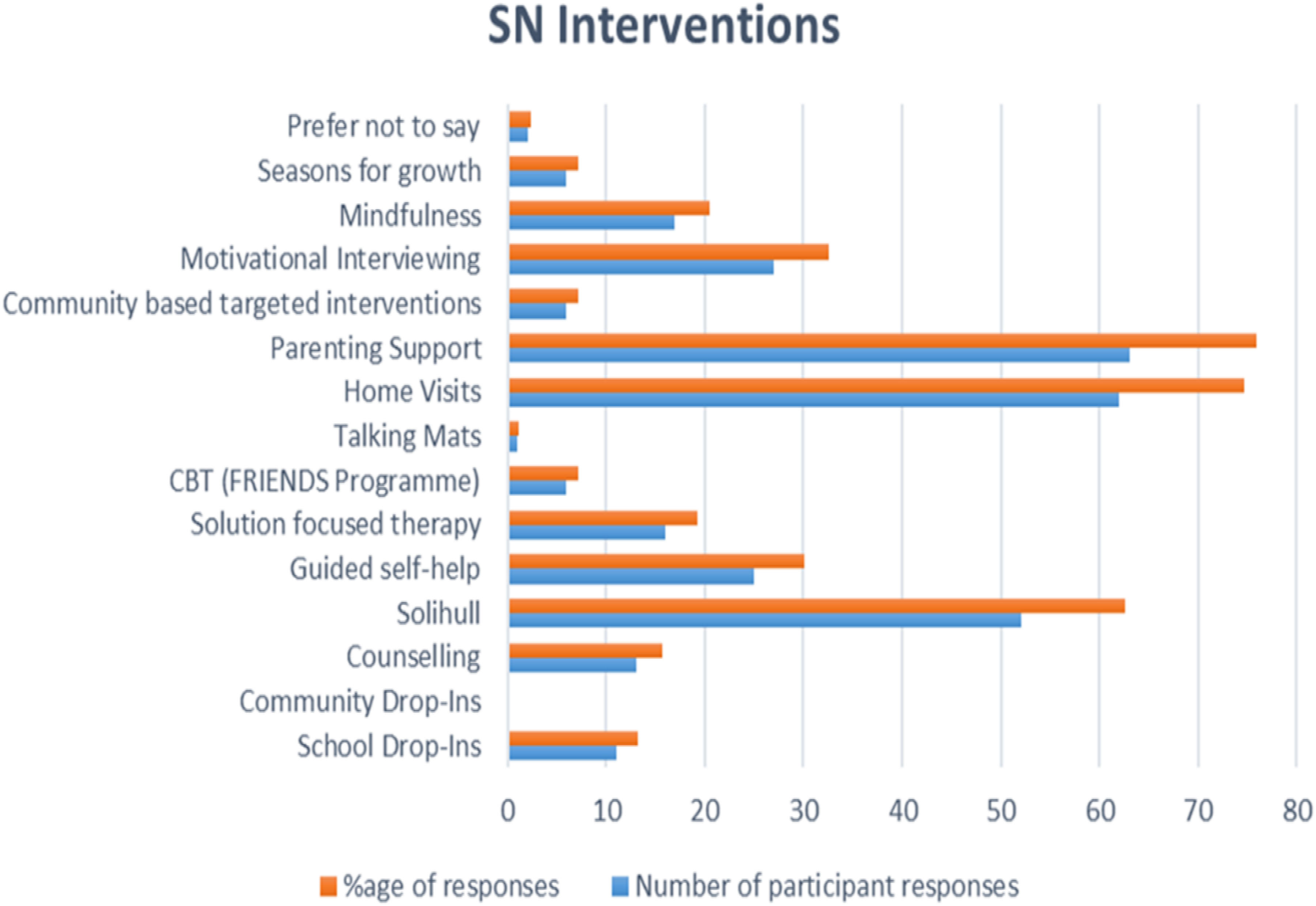
Phase one school nurse (SN) interventions.
Main Results
Analysis of the free text data identified three main themes: “Supporting children's mental health,” “Barriers to identification and support of mental health issues,” and “Educational preparation and training in mental health” (Table 2). Building and sustaining effective relationships with children, families and other professionals was viewed as essential. Yet, some reported this could take time and relied on the effectiveness of communication with professionals and an understanding of each other's role and responsibilities. Others indicated that limited time with children made it challenging to build relationships with them, and this was a source of frustration. Barriers to the identification and provision of support included lack of knowledge and understanding of the school nurse role, workload capacity and lack of resources. There were a variety of views about their educational preparation and training in mental health with some indicating there was not enough content on emotional/mental health in their school nurse programs and a lack of practical training to deliver mental health interventions.
Phase Two
Three key themes and eight subthemes were identified (see Table 4) and situated within the PPCT Model (Bronfenbrenner, 1995). Theme One linked to Person, Theme Two linked to Process and Theme Three linked to Context. Time had an impact on each theme.
Phase Two Themes and Subthemes.
Theme One: Understanding of Mental Health and Issues Impacting on Primary School-Aged Children
This theme explained participants understanding of mental health and the predominant perspective that it is viewed in the context of an individual's interaction with their wider world. It also explained their perspectives of the issues that primary school-aged children worry about.
Subtheme: Mental Health, Self-Care, and Their Wider World
Children, parents, and teachers shared similar understandings of the concept of “mental health,” with most referring to thoughts and feelings and how these affect a person's wellbeing. Except for one child who was very shy, the children clearly articulated their understanding of the term “mental health.” When asked what it meant, their accounts included “how you feel,” being “happy,” and “how your brain reacts.” For example, one child said: Like how you feel, like how your brain reacts to something. (C4) mental health is coping and how you are in yourself. If you said mental health when I was younger, you’d think that someone was ill. But mental health to me is actually, it's how, it's like it's your wellbeing. (P5) I think developing something that teaches children the understanding of mental health would remove that stigma…. (P4)
Subtheme: Children's Worries
Anxiety was cited by school nurses, parents and teachers as the main issue impacting on children's mental health, though many believed that children were anxious because their parents were anxious. For example, one of the parents commented: Parents I feel are often overly anxious about their children's wellbeing and often read into stuff that isn’t there. (P1) I use YouTube and stuff, but well I did use stuff where other people can comment. But then tons of my school friends reported me and because I had apparently posted my face which they think is ugly. (C3)
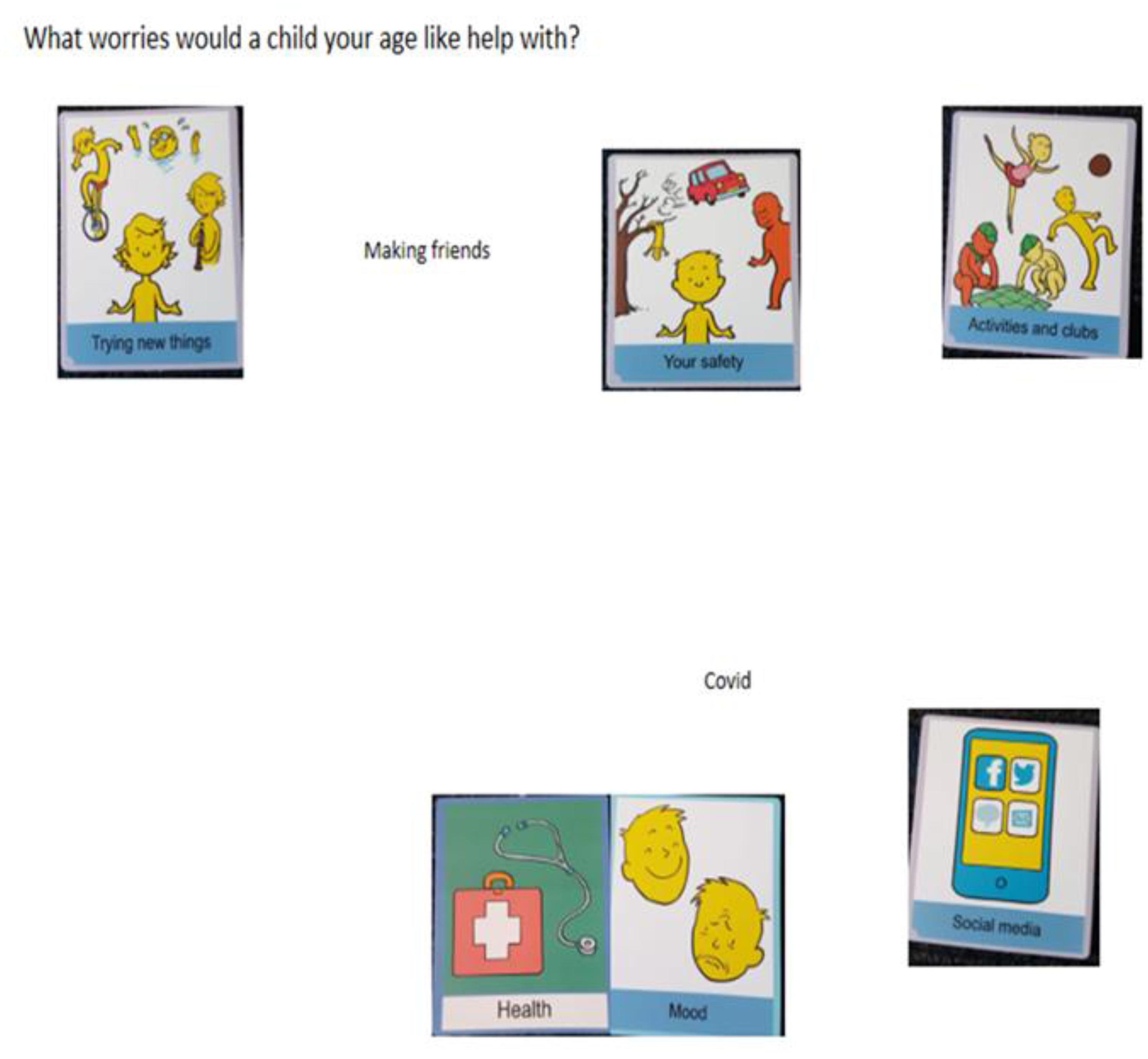
Child 8 picture supported conversation.
Theme Two: School Nurse Mental Health Practice
There were three recurring factors pertaining to the mental health work of the school nurse which combined to form theme two and the three subthemes. The importance of relationships was a golden thread running throughout the interviews.
Subtheme: Relationship-Centered Practice
Relationships were viewed as crucial for working effectively with children, parents, teachers, and other professionals. The children placed great importance on the need to know and feel able to trust the school nurse before feeling comfortable to share any worries. One child stated: if I knew them from my P1 then I could tell them now because I’ve known them for so long. If they just came in today and I had no idea who they were, I wouldn’t really want to tell them because I don’t know who they are…. (C6)
Subtheme: School Nurse Interventions
School nurses used a wide range of interventions, and they described innovative and creative ways of adapting their practice during the pandemic, with many using “walk and talk” interventions instead of home visits. Early intervention was viewed as essential, with many suggesting they should be in schools educating children about their mental health: We should be doing pieces of group work in school with young people right from an early age because then they know … if we teach them that literacy round and about their mental health or emotional wellbeing, then that's half the battle…. (SN4)
Subtheme: Holistic Perspective
A common metaphor used by school nurses, teachers and some parents was the importance of “obtaining a holistic picture” of each child. When asked what approaches to public health practice they use, the school nurses described three approaches which included a holistic, a strengths-based, and a medical approach. A holistic approach was the most widely expressed view, reflecting the findings of Phase One. The findings also indicate that school nurses view their practice through an ecological lens: It is about working with the parents to support the children. So, it is all about building the resilience of a community and not just the resilience of a child. (SN2)
Theme Three: Barriers to Accessing Mental Health Support From the School Nurse
Lack of awareness of the school nurse role, the gatekeeping role of schools, and workload capacity were the main barriers identified.
Subtheme: Lack of Awareness of the School Nurse Role and Remit
The school nurses indicated that there was a general lack of knowledge and understanding of their role and that children, parents, and professionals do not know who the school nurse is or what they do. This perception reflects the findings from Phase One but also confirms the findings of Woodhouse et al. (2016). One school nurse commented: there is still an element of people don’t know what we do, whether it is nit nurse etc.… (SN6) I am sorry because our school doesn’t have a school nurse. (C3)
Subtheme: The Gatekeeping Role of Schools
The interviews with parents highlighted, that schools, particularly the head teacher, influenced their access to the school nurse. For instance, one parent commented that she had been informed that there was not a school nurse for the school: I think that I have asked about the school nurse a couple of times…. They said there isn’t one, she doesn’t come here or something like that. (P3) For mental health I would say we probably tend to go more Ed Psych than the school nurse team. (T1)
Subtheme: Workload Capacity
Workload capacity was consistently expressed as a barrier to the school nurse's mental health work, and they described their work as reactive rather than proactive. Child protection, lack of resources, including retention of school nurses were seen as barriers to early intervention and support. Strong feelings were expressed at the lack of recognition of their specialist education and value of their role in comparison to health visitors and perceived impact on retention: until we are recognised on a par with family nurse and health visiting, we are not going to retain staff … we are spending so much money training people and they’re leaving as soon as they are done… (SN4)
Discussion
Drawing on bioecological systems theory, this mixed methods study has addressed the aims and research questions by exploring and explaining school nurses’ mental health work supporting primary-school-aged children. It has generated a novel and contextualized understanding of school nurses’, children's, parents’, and teachers’ experiences in Scotland, building on and contributing to the evidence to support their public health role.
Participants’ experiences and understanding of the mental health work of the school nurse are influenced by a range of factors, the most significant being related to their awareness and knowledge of the school nurse role. The children and parents’ experiences and understanding of the school nurse and their work in supporting primary-school-aged children's mental health was based on their knowledge of who the school nurse is, and their contact with the school nurse. Children and most parents had no knowledge or experience of contact with the school nurse, and they thought the school nurse was the first aider in the school. It is noteworthy that over a decade earlier, Chase et al. (2010) reported similar findings. Moreover, a consultation with school-aged children in Scotland commissioned by the Scottish Government to inform the refocused school nurse role revealed similar findings (Woodhouse et al., 2016), which implies that seeking children's views was tokenistic as this research suggests their views have not been acted upon. Although the teachers had experience of working with school nurses in their current roles, this was not reflective of their previous experience of working across different primary schools and within different local authorities. They also had limited knowledge that the school nurse was a specialist in community public health nursing, and they were unaware of the refocused school nurse role and school nurse priority areas and pathways. Misunderstanding of the school nurse role is not confined to Scotland, which is perhaps not surprising, given that globally the educational preparation and guidance for school nurse practice differs. For instance, in the United States of America, it varies depending upon the state (Willgerodt et al., 2018).
School nurses considered their role to be less visible and accessible since the introduction of the School Nurse Priority Areas and Pathway due to changes in their practice, reflecting the findings of Doi et al. (2018). These changes included drop-in sessions no longer being offered and health promotion activities in school being stopped. There were several reasons underlying these changes, and these included the role of the school nurse being more targeted on vulnerability, child protection and looked-after children, changes to the referral system and health promotion not being included as a priority area. The school nurses in Phase Two expressed views that these changes had impacted on their ability to be actively involved in mental health work and to have contact with children and their parents in school or at home. Their views help to explain the finding from Phase One, that the frequency of visits to schools was dependent on the vulnerability and need of the children and needs of the school. In both phases, school nurses indicated that they visited schools in the most deprived areas more frequently than schools in more affluent areas. This reflects the experience of the teachers who both worked in schools located in deprived areas and described frequent contact with the school nurse. It also explains why the children and the parents had no experience of the school nurse, as their schools were in more affluent areas.
There is recognition that the prevalence of mental health issues in CYP from all backgrounds is increasing. According to McDaid and Park (2022) in their report on the economic case for the prevention of mental health in the UK, poor mental health cost the Scottish economy £8.8 billion in 2019. Yet, this does not include the unseen personal costs to the child and their family that impact on their quality of life, such as being socially isolated and stigmatized due to their mental health. The parents were very aware of the stigma associated with mental health, and the need for education about mental health, which supports McDaid and Park’s (2022) contention that primary prevention could be cost-effective for the economy. Primary prevention is integral to specialist community public health nursing practice and is clearly articulated within the new field-specific standards of proficiency for SCPHN-SNs (NMC, 2022). Yet, in both phases, the school nurses were not involved in prevention. Notably, school nurses who had worked in the school nursing service prior to implementation of Scotland's Curriculum for Excellence for children aged 3–18 (Scottish Executive, 2006), indicated that it had impacted on their preventive role as it resulted in them handing over health promotion activities in school to teachers.
Lack of confidence, knowledge, experience, unmet training needs and difficulty accessing training have been identified in previous research as barriers to school nurse involvement in delivering mental health interventions to support school-aged children's mental health (Pryjmachuk et al., 2012; Skundberg-Kletthagen & Moen, 2017). Extensive mental health training was offered to school nurses in both phases, albeit some respondents in Phase One indicated that training could be more difficult to access if they worked part-time. Participant accounts in Phase Two were significant as they highlighted differences in their perceptions of training and its value for their practice. These differences appeared to be linked to the attitude of the school nurse, length of experience working in the service, and relevance of training for practice. The findings contribute key nuances as there was an expressed need for training in practical interventions and resources specifically to use with primary-school-aged children.
Over the last 20 years, research with school nurses working in the UK, Norway, Sweden, Finland, and the USA has highlighted that lack of resources, staffing issues and child protection workload are barriers to school nurses’ capacity to support children's mental health (Hoskote et al., 2025; Jonsson et al., 2019; Markkanen et al., 2021; Skundberg-Kletthagen & Moen, 2017; Wilson et al., 2008). Despite this, in both phases, workforce capacity was cited as an issue that constrains their mental health work. In Phase One, shortages of staff were highlighted, but limited details were provided to explain the reasons for this. The accounts of the school nurses in Phase Two identified that recruitment and retention of school nurses and their redeployment into acute services during the first lockdown were barriers. Their redeployment during the pandemic also contributed to their feelings of being undervalued (Sammut et al., 2023). Strong feelings were expressed that school nurses were leaving the profession as their job grading and pay scale was not equivalent to SCPHN-health visitors (who have a higher pay grade in Scotland), and this was a source of frustration. Consequently, they felt that there was lack of recognition of their specialist education and lack of value attributed to their role. It is notable that, two decades earlier, Croghan et al. (2004) suggested that the job grading of school nurses should be addressed for these reasons.
School nurses in Phase Two expressed job satisfaction when working with children and they talked enthusiastically about the interventions they used with children to support their mental health. They also expressed a degree of disillusionment with the school nurse service. In both phases, school nurses described their work as being reactive rather than proactive, reflecting the findings of Jonsson et al. (2019) and Sammut et al. (2023), and the analogy of “firefighting” was used by one school nurse to describe this. It is remarkable that this tension in school nurse workload is not new (Spratt et al., 2010), which does question the value commissioners place on the provision of school nursing services and the school nurse role.
Access to schools and to school-aged CYP has been highlighted as a barrier in previous research. Lightfoot and Bines (2000) and Pryjmachuk et al. (2012) found that the ethos of the school and the attitude of senior members of the teaching team, especially the head teacher, influenced the extent to which school nurses could be involved in working with CYP and delivering interventions. Similarly, some school nurses in Phase One aired views highlighting that they were more likely to be contacted by the head teacher when there were concerns about a child if the head teacher knew them. The interviews with parents and teachers highlighted that the head teacher and depute head teacher had a gatekeeping role in regulating access to the school nurse service. School nurses can and do build positive relationships with head teachers, but to do this effectively and increase understanding of their mental health work, they need to be visible in schools. Notably, the teachers suggested that the gold standard would be to have a school nurse based in every school, reflecting a recently published report campaigning for a school nurse in every school in England (College of Medicine and Integrated Health, School and Public Health Nurses Association and Queens Nursing Institute, 2024). These findings are significant as they point to the need for school nurses to be included in whole-school approaches to mental health, working together with teachers, parents, children and people in the child's wider world to intervene early to promote good mental health and build resilient children and families.
Strengths
The Phase One study was a national cross-sectional online study and to our knowledge, the only one that has sought the views of nurses working in the school health service in Scotland, specifically about their mental health work with primary-school-aged children. In contrast to previous surveys of school nurses working across the UK, which have low response rates from Scotland (e.g., 4% RCN, 2016 and 3% Sammut et al., 2023), the response rate of 29.5% is significantly higher and therefore more representative of Scottish school nurse practice. Bioecological systems theory was used across the entire research process which serves to exemplify the practical application of ecological theory in the field of school nursing; and specifically in the context of their mental health work with primary-school-aged children. Currently there are no similar published studies, and thus this can be considered novel.
Limitations
Phase Two was undertaken in one health board area in Scotland, and the sample size of the participating school nurses, children, parents, and teachers was relatively small. Therefore, caution is required when interpreting the findings as they may not reflect the views of school nurses, children, parents and teachers across Scotland. Including children and parents with actual experience of contact with the school nurse may have provided a better understanding of the school nurse mental health role. Interviews were conducted online due to COVID-19, and it was difficult to develop a relationship with participants, particularly the children. It is possible that they may have shared more information if the interviews had been face to face.
Implications for School Nursing Policy, Practice and Research
The findings from this study have several implications to inform policy, school nursing practice and future research. Adopting a bioecological perspective may support school nurses to exercise their autonomy and agency, to lead efforts to raise awareness about their role promoting mental health in schools and communities. School nurses work at the interface between the school, the child, their family and community and are uniquely placed to build trusting, nurturing relationships, not only with CYP, but also their families and the community. They should exploit opportunities to be introduced to parents and children at key transition times, utilizing digital platforms to promote their service. By working more strategically, school nurses can use their leadership skills to ensure that their role and remit is included and clearly articulated in whole-school approaches to mental health. We already know that these approaches may help to address the associated issues of anxiety and poor school attendance (Rowlands, 2022). There is a need to increase literacy about mental health to normalize anxiety and to support early identification and support. Thus, it is essential for providers of school nursing education to ensure that the curriculum equips school nurses with the knowledge and skills required to identify and support primary-school-aged children's mental health and influence policy. Future research should investigate school nurse mental health interventions and resources, for example, the “walk and talk” intervention to assess the benefits and challenges of taking a school nurse intervention outdoors.
Conclusion
Though this mixed methods study was conducted in Scotland, the findings have significance for school nurses in countries with a similar school nursing service. This research shows that despite factors constraining school nurses’ involvement in mental health, they can play an even more vital role in supporting primary-school-aged children's mental health as part of a whole-school approach. Viewing school nurse practice through a bioecological lens has identified that building trusting relationships with the school-age child, parents, teachers, and key people in their wider world is crucial for providing effective and early support. To achieve this, it is fundamental that school nurses are working in schools and communities to promote good mental health and build resilience, as their mental health work is “all about the relationships.” Investment in recruiting and retaining school nurses must be prioritized by commissioners and policy makers and their role should focus on primary prevention.
Footnotes
Acknowledgments
Grateful thanks to the advisory groups and all the participants who gave of their time to support this study as without them it would not have been possible. Thanks to Talking Mats Ltd for permission to use their resources in this research.
Author Contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author received financial support in the form of fees paid for the PhD, Talking Mats Foundation Training and purchase of the Consulting Children and Young People Resource, University of Stirling.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.