
Abstract
This study investigated Swedish school nurses’ experiences, self-perceived knowledge, and attitudes towards HPV vaccination. A cross-sectional repeated questionnaire study was conducted. The results were compared to a previous study conducted in 2016. Additionally, open-ended responses were thematically analysed. A total of 344 nurses participated. Overall, more participants reported good self-perceived knowledge and favourable attitudes towards HPV vaccination compared to 2016. Still, nearly half expressed a need for further education. The thematic analysis revealed barriers including lack of training, inconsistent guidelines for addressing vaccine hesitancy and ensuring children's participation in decision-making, limited access to diverse information materials, and time constraints related to vaccination tasks. Since school nurses in Sweden are responsible for all aspects of school-aged vaccinations within the national immunization program, it is essential that they receive support to feel motivated and confident in addressing vaccine hesitancy. Continued education and the implementation of uniform guidelines are therefore necessary.
Human papillomavirus (HPV) vaccine prevents HPV-related cancers in both men and women, especially cervical cancer which is the second most common cancer among women of reproductive age (Sung et al., 2021). Unfortunately, vaccination rates remain suboptimal in most countries, meaning they fall below the levels needed to achieve herd immunity and meet public health targets (Shapiro, 2022). Consequently, there is a risk of not achieving the World Health Organization's (WHO) goal to eliminate cervical cancer - a strategy in which one of the three central targets is to reach 90% HPV vaccination coverage among girls by 2030 (World Health Organization, 2020a).
HPV vaccination has been offered free-of-charge in Sweden through the national school-based childhood immunization program (NIP) since 2012 for girls. In 2020, the gender-neutral vaccination program was introduced, meaning that all children in fifth grade (ages 10–12) are now offered HPV vaccination. In Sweden, compliance with early childhood vaccinations is high but acceptance of the HPV vaccination is lower: in 2023, 88% of all girls and 83% of all boys aged 12 were fully vaccinated with two doses (The Public Health Agency of Sweden, 2022; The Public Health Agency of Sweden, 2023).
To decline or postpone recommended vaccines despite available vaccination services, referred to as vaccine hesitancy, is considered a top-ten threat to global health by the WHO (World Health Organization, 2019a). This is a complex issue with varying impact in different sub-populations. Reasons for hesitancy may vary over time and type of vaccines (MacDonald, 2015). Specific challenges for the HPV vaccination concern its protection against a sexually transmitted infection (STI) and the young age (9–14) for recommended vaccination (Grandahl & Nevéus, 2021; López et al., 2020). The erroneous idea that vaccination may encourage sexual activity is commonly reported (López et al., 2020). Among boys and their parents, there is a misconception that HPV is an exclusively female problem (Grandahl & Nevéus, 2021).
One of the most important factors for the parental decision to vaccinate their children is trust in healthcare providers’ (HCPs) recommendations (Lin et al., 2021). In Sweden, nurses play a crucial role in parental acceptance of childhood vaccinations by building trust in the national vaccination program from an early stage, and support informed parental decision-making (Appelqvist et al., 2023). School nurses i.e., registered nurses with a specialist degree, are responsible for all aspects of administering recommended vaccinations to school-aged children and are considered the most reliable source of HPV vaccine information by Swedish school children (Enskär et al., 2024; Grandahl et al., 2019). The school nurse responsibilities include informing both children and parents, administering the vaccines, and offering vaccinations to unvaccinated children. Consequently, school nurses, the HCPs in this setting, play a key role in the success of the school-based vaccination program. However, HCPs may lack adequate knowledge, training, and confidence to deliver strong recommendations for HPV vaccination. Moreover, their own attitudes and vaccine hesitancy—shaped by concerns about safety, efficacy, or anticipated parental resistance—can significantly influence whether and how they recommend the vaccine (Lin et al., 2021). In 2013, following the introduction of the school-based HPV vaccination program, the research group performed a cross-sectional study to investigate school nurses’ knowledge of, attitudes towards and experiences of HPV vaccinations (Grandahl et al., 2014). In 2016 a repeated study was conducted (Grandahl et al., 2017). Generally, school nurses reported more favorable attitudes towards the HPV vaccine in 2016 compared to 2013, but still 56% stated they needed more knowledge. In 2016 a larger proportion of school nurses (90%) had been contacted by parents who had concerns about the vaccine, compared to 76% in 2013 (Grandahl et al., 2017). The increase of parental concerns in 2016 was likely due to extensive media debates and spread of misinformation about the safety of the vaccine at the time. These events had massive implications for well-functioning vaccination programs in other countries (Hanley et al., 2015; Suppli et al., 2018). Recently, we have experienced how the COVID-19 pandemic has caused setbacks in vaccination rates worldwide (Casey et al., 2024; Karafillakis et al., 2022). These instances highlight the importance of continuously monitoring vaccination programs. Given the crucial role of school nurses in HPV vaccinations, it is important to follow up on their experiences to ensure resilience of the school-based vaccination program. Therefore, this study aimed to investigate their experiences of the school-based HPV vaccination program. More specifically, to investigate:
If more school nurses had favorable attitudes toward HPV vaccination in 2024 compared to the previous study in 2016 If more school nurses considered that they had good knowledge about HPV vaccination in 2024 compared to the previous study in 2016 School nurses’ experiences of providing information about HPV vaccination School nurses’ experiences of barriers and facilitators for HPV vaccination
Methods
Study Design
This was a repeated cross-sectional questionnaire study.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Swedish Ethical Review Authority (dnr: 2023–01583–01). Informed consent was obtained from all participants.
Setting
In Sweden, HPV vaccination is mainly offered in fifth grade (children aged 10 to 12) in a two-dose scheme and requires parental consent. Unvaccinated children can get vaccinated free-of-charge through the school health services until the age of 18. In 2020, the Convention on the Rights of the Child was elevated to Swedish law [2018 : 1197]. The law does not state any age at when children are allowed to self-consent to healthcare decisions, but HCPs should evaluate the child's maturity on a case-by-case basis.
Recruitment of Participants
School nurses working with HPV vaccinations, currently employed in public or private schools, were eligible to participate. There is no official employment data on how many school nurses are working with HPV vaccination in Sweden. However, in total there were total 3,060 school nurses employed (part- or full time) in state driven primary and secondary schools in 2023 (The Swedish Association of Local Authorities and Regions, 2025). Participants were recruited in collaboration with the National Board of Swedish School Nurses (Riksföreningen för skolsköterskor, n.d). Study information was provided at their annual national congress in 2023, with approximately 1500 attending school nurses, as well as through their social media platforms. Additionally, we provided information about the study to the head of school health services and/or directly to eligible school nurses in each of the 290 municipalities. Participants were able to participate through Research Electronic Data Capture (REDCap) tools hosted at the university, or having the survey sent out in paper format (Harris et al., 2009; Harris et al., 2019). Written consent was attained from all participants. Two reminder emails were sent out if the school nurse had consented but not completed the questionnaire. Data collection started in spring 2023 and ended in spring 2024.
Questionnaire
The study-specific questionnaire used in the 2013 and 2016 study (Grandahl et al., 2014; Grandahl et al., 2017) was based on findings from previous studies clinical experience and input from experts in relevant fields. The original questionnaire's validity had been tested by a group of ten school nurses. In 2024, some of the gendered questions from the 2016 questionnaire were removed or re-phrased due to irrelevance or relating to recent changes of the NIP. Based on previous qualitative studies (Enskär et al., 2023; Enskär et al., 2024) questions about school nurses’ experiences were added. Furthermore, questions regarding children's participation in the vaccination decision were added to reflect recent legislation changes. The new questionnaire was again tested on three head school nurses before use.
In total, the final questionnaire consisted of 35 questions. Questions about participants’ background characteristics (n = 13) included age, sex, years of work experience, nursing specialist degree (pediatric nursing, public health or district nursing, school health nursing, other or none), school area (urban, rural or metropolitan), estimated number of children offered vaccination, and vaccination coverage at school level.
The questionnaire compromised the following main concepts:
Attitudes toward HPV vaccination (n = 2) Self-perceived knowledge about HPV vaccination (n = 5) Experiences of providing information about HPV vaccination (n = 12)
The concepts of attitudes and self-perceived knowledge consisted of statements followed by a multiple-choice four-point scale “Strongly agree” “Partially agree”, “Partially disagree” or “Strongly disagree”. Questions regarding experiences were followed by different multiple-choice answers, further described in Table 4.
Finally, there were five free text answers to questions concerning: other common reasons for parents to decline or postpone HPV vaccination, the most frequently received question from children about HPV vaccination, strategies used when communicating with hesitant parents, experienced difficulties with HPV vaccinations, and additional comments about HPV vaccinations. The 2024 questionnaire is provided as a supplementary file (S1).
Data Analysis
Quantitative Data Analysis
First, the quantitative data were described and comparisons were made between the 2024 and 2016 data. Differences were calculated using Mann-Whitney U test for ordinal variables, and Pearson's χ² or Fisher's Exact test for nominal variables. Independent sample t-test was used to compare scale variables between the two studies. Data were analyzed using SPSS software (28.0) and p-values of < 0.05 were considered statistically significant. The following variables were dichotomized: biological sex (man/woman), specialist degree (yes/no), and geographical area (rural/urban). Missing data was excluded from analysis.
Favorable attitudes toward HPV vaccination were defined as agreement with the following statements: the introduction of the vaccine to the NIP was appropriate, to have confidence in authorities’ decisions regarding the vaccination, that vaccination may increase awareness of sexually transmitted infections, and that children who initially decline should vaccination should be offered again. Additionally, disagreement with statements of common misconceptions about HPV vaccination – vaccination can cause serious side effects, vaccination may reduce participation in cervical screening, vaccination may result in increased number of sexual partners, and vaccination may result in decreased condom use – was considered indicative of a favorable attitude.
The 2024 data regarding school nurses’ experiences of providing information were presented in frequencies (n) and percentages (%). Data from the open-ended question concerning the most frequently received questions from children were sorted according to the topics and then quantified.
Qualitative Data Analysis of Open-Ended Questions
The COM-B model was used for a deductive thematic analysis of the qualitative data derived from open-ended questions in the 2024 questionnaire (Braun & Clarke, 2006). The WHO has adopted the COM-B model to assist authorities in identifying and analyzing factors that affect vaccination behaviors (World health Organization, 2019b). The model is based on the Behavior Change Wheel which allows for the identification of evidence-based intervention functions (Michie et al., 2011). It can be described as an interactional framework in which the behavioral determinants Capability (C), Opportunity (O) and Motivation (M), are needed to be in place for a behavior (B) to occur. Capabilities refer to having the required knowledge, skills and abilities; opportunities include contextual determinants impacting or making a behavior possible, such as sufficient time and resources; whereas motivation refers to internal processes influencing whether a person wants to perform a behavior. Motivational factors can be reflective (planning and evaluation of past experiences), or automatic (impulses, desires and inhibitions) (Michie et al., 2011). The use of the model allows to identify both individual and contextual determinants that can facilitate or hinder behaviors related to HPV vaccination. The steps of the thematic analysis are summarized below.
Searching for theory-driven themes: After familiarization with the data, text units were coded according to the pre-defined themes of the COM-B model's behavioral determinants. Units were then grouped together under the themes identified. Identifying barriers and facilitators: sub-themes describing barriers and facilitating factors within each theme were identified. Distinguishing between behaviors related to the varied tasks involved in school nurses’ work with vaccinations (B): The sub-themes were sorted according to the different behaviors described in the text units.
The analysis was an iterative process going back and forth between the original texts and the themes and sub-themes.
Results
Participants’ Background Characteristics
In total, 344 school nurses, representing all geographical regions (n = 21), and employed in 163/290 different municipalities participated in the present study. The sample size was lower in 2024 (n = 344) compared to 2016 (n = 736) but background characteristics were similar, as shown in Table 1. More school nurses reported a school vaccination coverage above 91% compared to 2016 (66% vs 43%, p < 0.001). Participants mainly vaccinated children in fifth grade (80%), while 10% vaccinated in lower-secondary school and 10% in upper-secondary school.
Background Characteristics of Participating School Nurses 2024 (n = 344) and 2016 (n = 736).
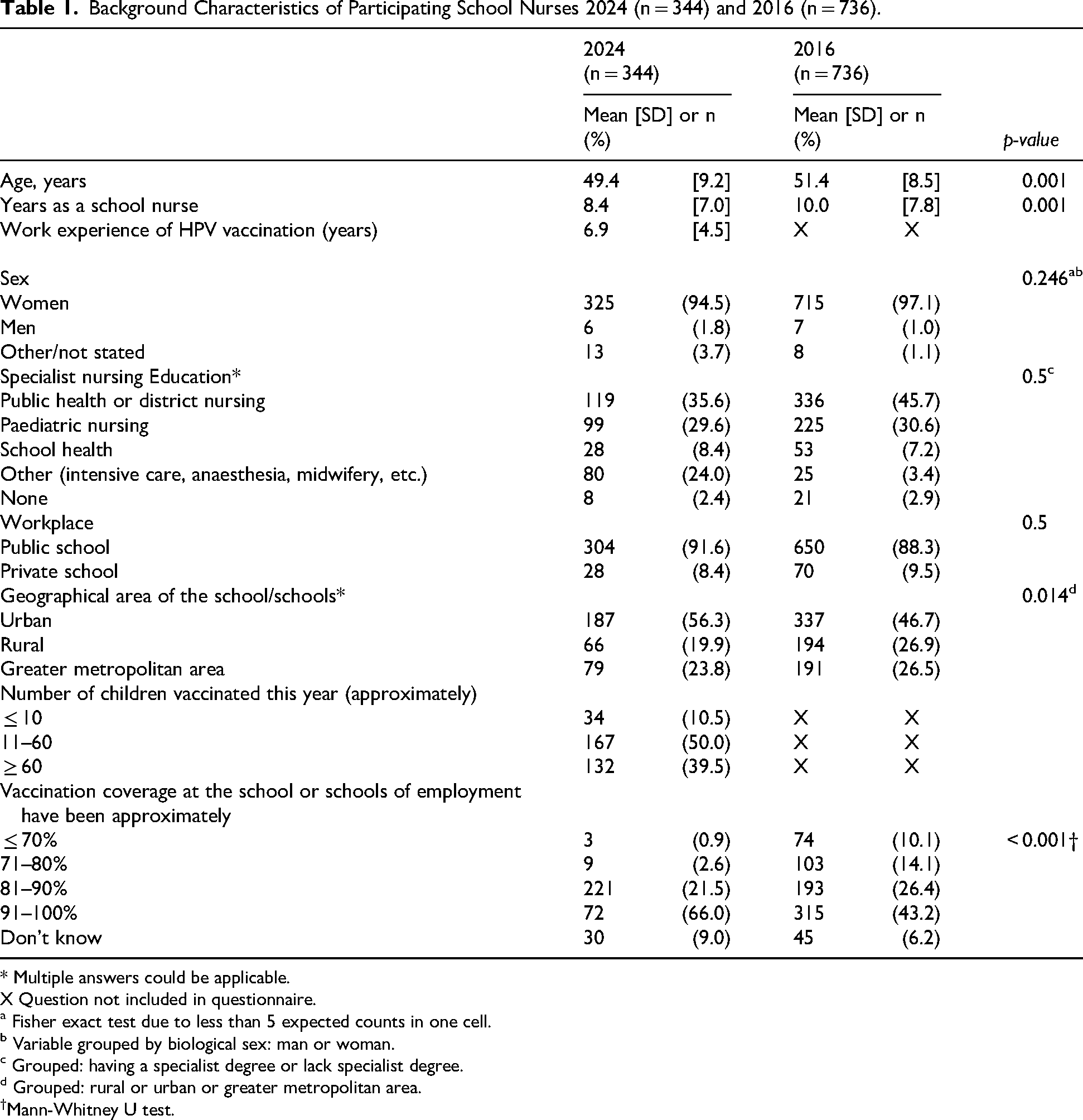
* Multiple answers could be applicable.
X Question not included in questionnaire.
a Fisher exact test due to less than 5 expected counts in one cell.
b Variable grouped by biological sex: man or woman.
c Grouped: having a specialist degree or lack specialist degree.
d Grouped: rural or urban or greater metropolitan area.
†Mann-Whitney U test.
School Nurses’ Attitudes Toward HPV Vaccination: A Comparison Between 2016 and 2024
In general, more participants reported favorable attitudes to the national HPV vaccination in 2024 in comparison with 2016. Detailed results are presented in Table 2. There were statistically significant differences in all attitude statements except for “HPV vaccine is more painful than other vaccines”, and “Fear of needles is a problem” (see Table 2). For example, more school nurses strongly agreed to the statements: it's appropriate that HPV vaccination was introduced in the national childhood vaccination program (99% in 2024 vs 86% in 2016, p = 0.001), and having confidence in the authority's decisions about HPV vaccination (96% in 2024 vs 67% in 2016, p < 0.001). Additionally, more school nurses disagreed to statements of known misconceptions. Still, a quarter partially agreed to the statement that HPV vaccination may reduce participation in cervical screening and 6% that vaccination may result in an increased number of sexual partners.
Attitudes Towards HPV Vaccination Among Participating School Nurses in 2024 (n = 344) and 2016 (n = 736).
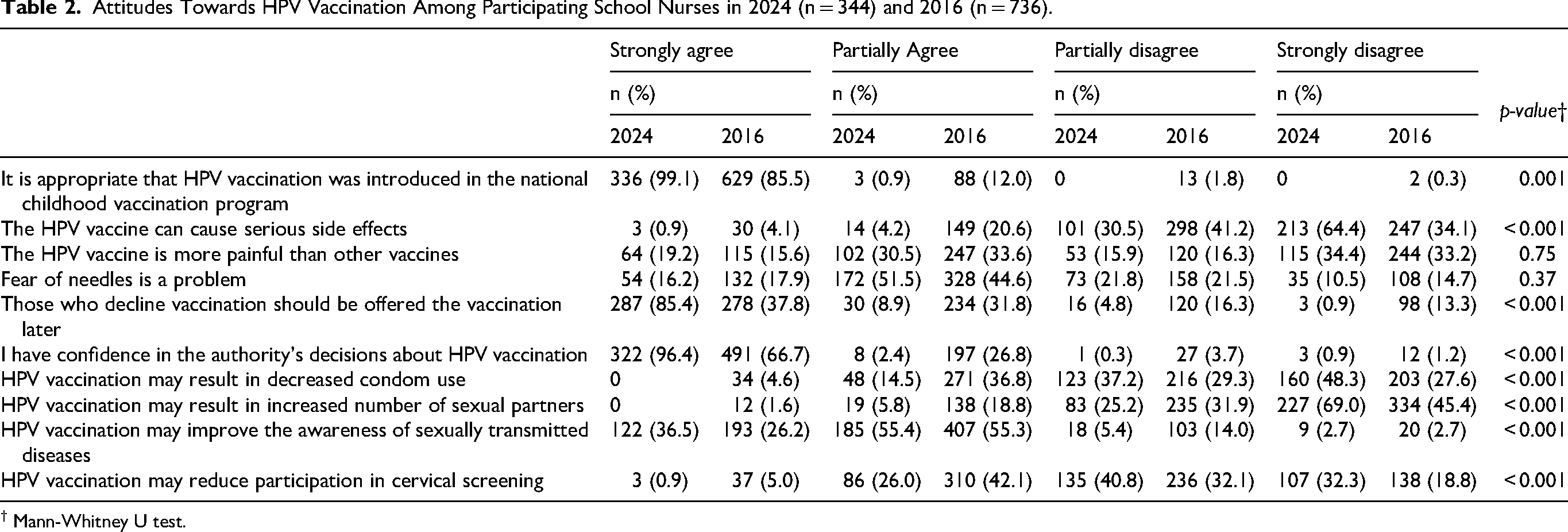
† Mann-Whitney U test.
School Nurses’ Self-Perceived Knowledge About HPV Vaccination: A Comparison Between 2016 and 2024
Significant differences were found across all statements regarding self-perceived knowledge, with a higher proportion of school nurses in 2024 agreeing to having good knowledge about vaccine safety and to inform and respond to families’ questions, compared to 2016 (see Table 3). Still, almost half (45%) of all participants in 2024 reported they wished to receive more education about HPV.
Self-Perceived Knowledge among Participating School Nurses in 2024 (n = 344) and 2016 (n = 736).
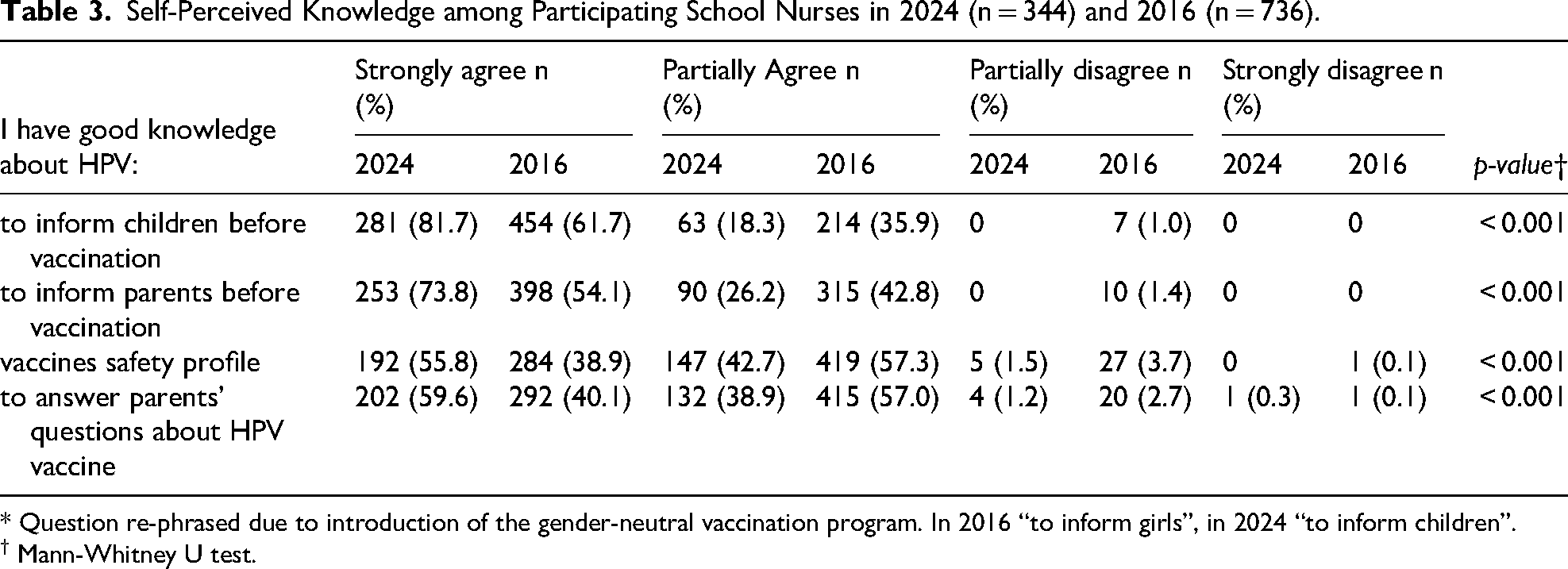
* Question re-phrased due to introduction of the gender-neutral vaccination program. In 2016 “to inform girls”, in 2024 “to inform children”.
† Mann-Whitney U test.
School Nurses’ Experiences of Providing Information About HPV Vaccination
Results from the 2024 data regarding school nurses’ experiences of providing information about HPV vaccination are detailed in Table 4. The majority of participants provided written information about the vaccination to parents. More than half (56%) only reported to provide written information to parents, while 44% reported two or more formats, most frequently a combination of written, and telephone or e-mail on the initiative of the parents. About one third reported that they initiated contact by e-mail/telephone to provide information, and 17% provided information at teacher-parental meeting.
School Nurses’ Experiences of Providing Information About HPV and HPV Vaccination in 2024 (n = 344).
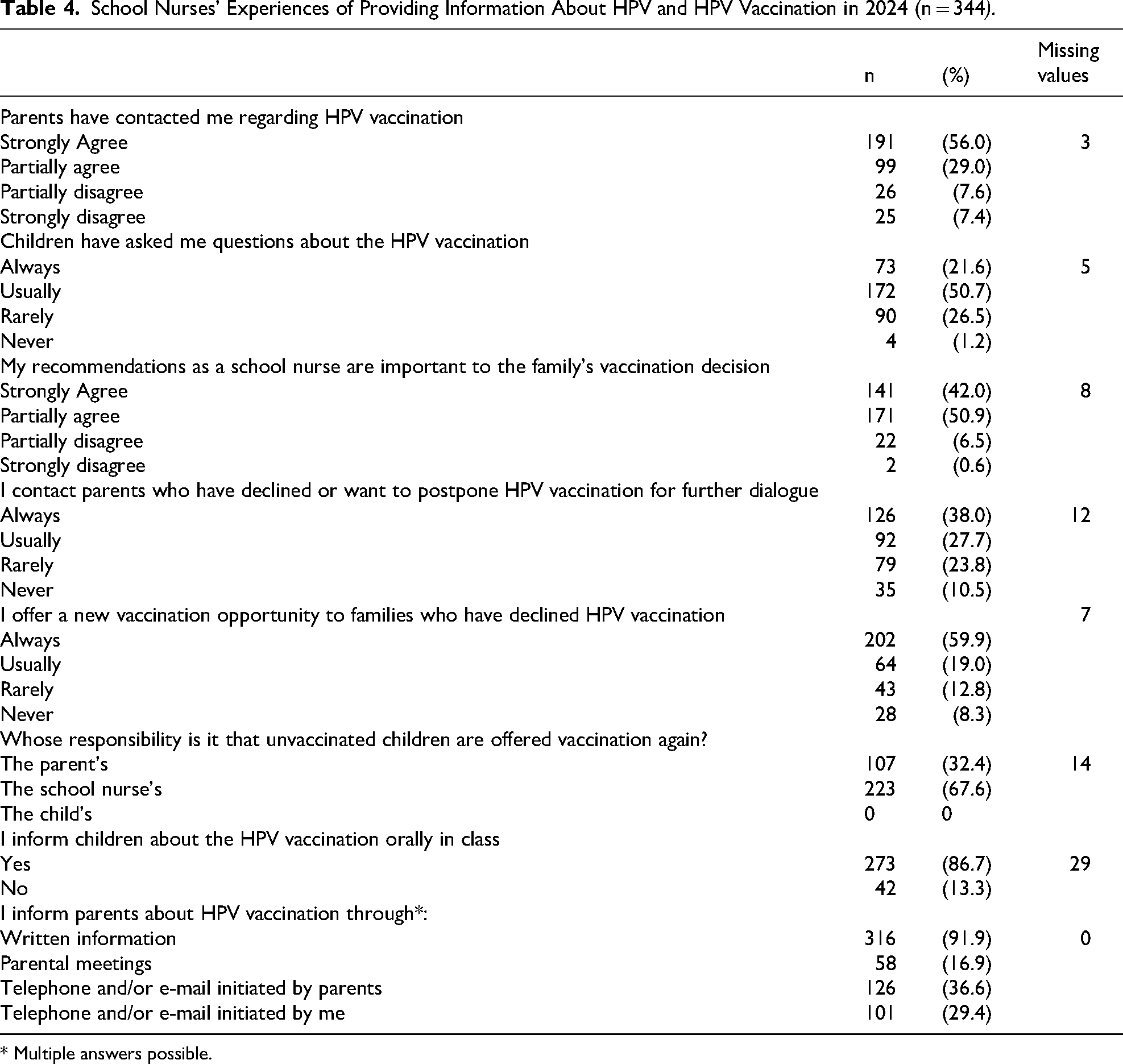
* Multiple answers possible.
A majority of participants (85%) strongly or partially agreed that they had been contacted by parents about HPV vaccination and 92% strongly or partially agreed that their professional recommendations are important to families’ vaccination decision. Furthermore, approximately two-thirds of participants reported that they always or usually contacted parents who had declined or postponed vaccination. Regarding the responsibility for offering additional vaccination opportunities to unvaccinated children, 68% identified the school nurse as primarily responsible, while 32% considered it the parents’ responsibility.
The most reported reasons for parents to decline or postpone vaccination (multiple answers possible) was: fear of side effects (62%), the young age of the child (35%), the child's fear of needles (33%), religious reasons (24%), fear of sexual risk behavior (10%) and the child has other medical conditions (6%). Other reasons were reported by 21% while 6% stated they did not know. Other reasons included open-ended statements concerning: that parents had also declined other childhood vaccinations, lacked awareness regarding the importance of vaccinating boys and that parents of children with neurodevelopmental conditions often had more concerns about the need to vaccinate their child and to acknowledge that their child will become sexually active in the future.
Most school nurses (87%) provided children with oral information, in the classroom, prior to vaccination and 72% used the Public Health Agency's informational material. Furthermore, A similar proportion (72%) reported to always or usually receive questions from children about vaccination. The most frequently received questions from children (n = 320) regarded: concerns about fear of pain “will it hurt?” (55%), wanting to know more “what is it, why should I take it and what will happen if I don’t?” (37%), “are there any side-effects?” (4%), about the vaccination procedure “what will happen?” (4%), “why do boys get vaccinated” (4%),”do I have to get the shot?” (4%), “why do I have to get two doses?” (3%), questions about sexual transmission (2%) and “I wish to get vaccinated but my parents do not consent, what do I do?” (1%).
School Nurses’ Experiences of Barriers and Facilitators to HPV Vaccination: Applying the COM-B Model
Data from three open-ended questions in the 2024 questionnaire were used for the thematic analysis: “Which strategies have you used when communicating with hesitant parents?” (n = 304), “I have experienced the following difficulties with HPV vaccinations” (n = 279) and “Additional comments about HPV vaccinations” (n = 132). The results of the qualitative analysis are presented in detail in Table 5, accompanied by quotes from the original data. The analysis identified barriers and facilitators for five different behaviors related to school nurses’ work with HPV: Informing children and parents about the vaccination, motivating hesitant parents, ensuring children's participation in healthcare decisions, managing children's fear of needles, and providing additional vaccination opportunities. For each behavior, sub-themes of barriers and facilitators are presented according to the main themes: Capability, Opportunity, and Motivation. The results are summarized below under each identified behavior.
Results from the Thematic Analysis of Open-Ended Questions to Swedish School Nurses (2024), Applying the COM-B Model.
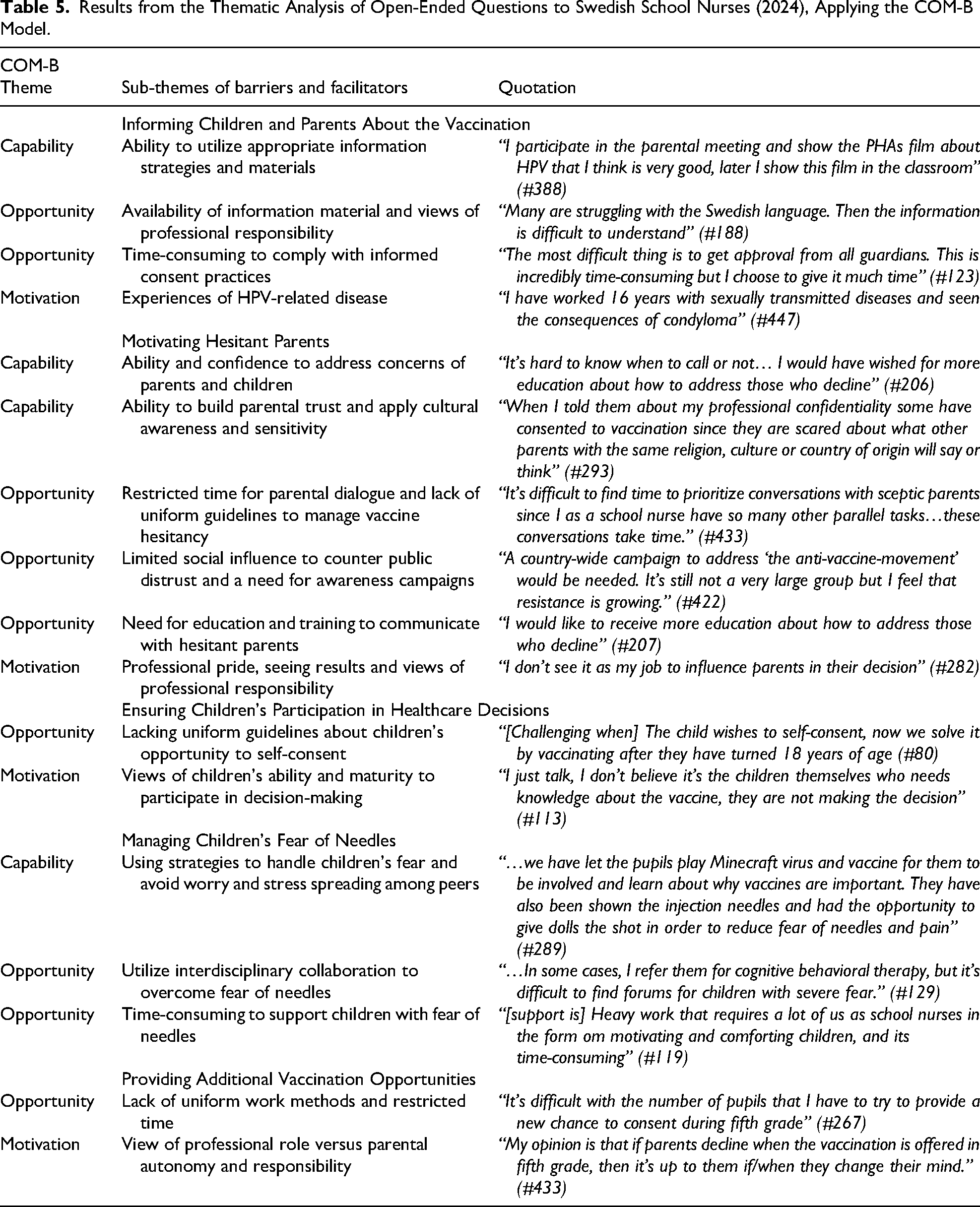
Informing Children and Parents About the HPV Virus and Vaccination
Participants described that facilitators to successfully promoting HPV vaccination were the ability to utilize appropriate information strategies and materials. To provide information in several formats was considered a means to adapt information to the individual needs of parents and children. A common strategy was to provide information repeatedly. Attending teacher-parental meetings were described as a good forum to provide a combination of face-to-face information followed by written information. Some described that they informed about the vaccination already at parental meetings in the child's first school year.
Informing children in class was regarded by participants as both a facilitator of children's participation and an opportunity for them to favorably influence the parents. The content of the information participants provided were influenced by their own views of children's maturity. Beliefs that children were too young to comprehend information or to participate in decision-making discouraged the nurses from providing extensive information. Instead, they focused more on the practicalities. Participants views about professional responsibilities to promote vaccinations influenced their strategies. It was argued that written information was sufficient and it was a parental responsibility to seek more knowledge. A practical example was to delegate the provision of vaccination information, both to children and parents, to the teachers.
Participants found it challenging to provide information to parents and children who were not fluent in Swedish or had low health literacy. Efforts to make sure the information was given in an appropriate language were prioritized but not always possible. They voiced a need for material adapted to different languages and different health literacy levels, and more clearly explained why boys should be vaccinated. A few stated that they used interpreters when communicating with parents who spoke a different first language.
To have personal experience of HPV-related disease and seeing the effects first-hand strengthened the sense of importance and opportunity to prevent disease. On the other hand, it could also make it difficult to talk about the subject and give a sense of hopelessness when knowing that some children would remain unprotected.
To comply with informed consent practices were seen as very important, but also described as the most tedious and time-consuming barrier. The school nurses prioritized most of their time to ensure that the formal documentation was correctly received in time. Furthermore, consent practices were described as rigid and not adapted to the complexity of different family situations such as when the school nurse cannot reach the parents and consequently not vaccinate.
Motivating Hesitant Parents
Participants described a lack of knowledge, training and confidence to address parental concerns and reasons for vaccine hesitancy. They also voiced an uncertainty about their professional mandate to contact hesitant parents, and the lack of guidelines to do so. Believing it was a parental responsibility to initiate dialogue with the school nurse, or not wanting to interfere in parental decisions discouraged active outreach. Further, a commonly expressed barrier was a lack of time.
On the other hand, nurses stated that they were motivated to reach out to hesitant parents because they had reflected about family circumstances that may call for additional support. Other motivational factors to actively motivate hesitant parents were professional pride, to take part in the elimination of cervical cancer, and seeing results of increased vaccine acceptance. Furthermore, cultural awareness and sensitivity were described as facilitators for addressing socio-cultural reasons for hesitancy. To be able to build parental trust facilitated not only vaccination dialogues but also fostered confidence in all health encounters with the school nurse. Multiple interactions and respectful dialogue with parents, during their child's schooling, facilitated fruitful relationships. Therefore, they voiced the importance of having present and reliable school health services where school nurses have time for the pupils and their parents.
The nurses described having limited social influence to counter public mistrust against vaccinations. Knowing that some families decline all vaccines, as well as experiences of parents rejecting further dialogue with the school nurse, were discouraging to continued efforts. Instead, participants voiced a need for awareness campaigns about the HPV vaccine and the introduction of a gender-neutral vaccination program.
Ensuring Children's Participation in Healthcare Decisions
The experience of conflicting wishes about vaccination within a family, either between the parents and the child or between parents, was described as a dilemma. Participants felt uncertain how to handle such situations. If the child wanted to get vaccinated but one or both parents decided against, nurses lacked confidence about letting the child's wish be final. Participants described that they informed the child about the possibility to get vaccinated later on, at an older age when they could self-consent. However, nurses described an uncertainty about how and when to conduct a maturity evaluation in order for the child to legally be allowed to self-consent, especially at younger ages. Furthermore, differing recommendations or guidelines concerning at what age children could self-consent was described. Statements about the recommendations and guidelines nurses complied with in this matter widely varied. Several stated that children had to wait until their 18th birthday.
Managing Children's Fear of Needles
The ability to counter spread of worry and stress among children was described to be important. That children talked among each other about the vaccine being painful or shared misinformation about its safety could increase the fear of being vaccinated. This behavior among children was described to be frequent among children aged 11 to 12, but common in all age groups. The fear of pain was also described to affect acceptance of the second dose. Parents of children with a pre-existing fear of needles were perceived to more easily de-prioritize the HPV vaccination. Furthermore, experiences of children declining due to fear of needles when permitted to choose for themselves were described. To properly inform and communicate with children, teachers, and caregivers facilitated a calm environment.
Knowledge about the importance of timely vaccinations was a motivational factor to prioritize giving support to children with fear of needles. The ability to use different strategies was then an important facilitator. Examples given were using pain relieving plasters, diversion, relaxation techniques and having parents present. However, this could be time-consuming. Therefore, interdisciplinary collaboration was seen as important. The opportunity to refer to other medical professions either within or outside the school health services, was also a facilitating factor. For example, children had been referred to cognitive behavior therapy, hospital play therapy or medical interventions such as nitro oxygen during vaccination.
Providing Additional Vaccination Opportunities
Different approaches to provide unvaccinated children with an additional vaccination offer were described. Local methods included providing new offers and information at start of every new school year, as a set talking point at the repeated mandatory health talks provided by the school health services. The nurses’ own view of their professional responsibilities motivated initiatives to actively provide additional vaccination offers. The various statements illustrated a lack of uniform methods, and restricted time was again voiced as a barrier.
Discussion
Main Findings
In general, more school nurses reported favorable attitudes towards, and good self-perceived knowledge about, HPV and HPV vaccinations, comparing results from 2024 and 2016. Most agreed to have been contacted by parents with concerns about the vaccination about the vaccination (85%), and to have received questions from children (72%). More than half (56%) of participants only reported to provide parents with written information about the vaccination. Furthermore, the majority (92%) agreed that their recommendation was important to families’ vaccination decision. However, 21% rarely or never offered a new opportunity to families who had initially declined vaccination and almost a third considered it to be the parents’ responsibility that unvaccinated children are offered a new opportunity. The thematic analysis of open-ended data identified several important barriers and facilitators connected to the COM-B themes of capability, opportunity and motivation to behaviors related to HPV vaccination in the school-based setting. These findings can inform future intervention development with the aim to strengthen school nurses’ important work.
Capability
One explanation for HPV vaccination rates being lower compared to other childhood vaccinations in Sweden is the transition from vaccinations being provided at child health clinics to the school health services (Appelqvist et al., 2023). In the ages 0–5 parents regularly accompany their children to health centers for check-ups and vaccinations where multiple interactions with a nurse overtime facilitates a trusting relationship (Appelqvist et al., 2023). The school health services, on the other hand, are predominantly communicating with parents through written information, as also seen in this study. To inform and promote the vaccine at the teacher- parental meetings was one way of bridging this gap. Unfortunately, only a minority of school nurses used this strategy. Furthermore, language and health literacy barriers are likely to be more prominent when information is provided mainly in written form (Grandahl et al., 2015; Sanders et al., 2009). Although school-based vaccination programs are regarded as the most equitable approach to delivering HPV vaccines, Swedish girls whose parents have lower income, lower educational attainment, or an immigrant background are less likely to receive the HPV vaccine (Wang et al., 2019; Wemrell et al., 2023), highlighting the need for more inclusive communication strategies and targeted outreach.
Opportunity
HCPs’ confidence about the benefits and safety of vaccinations is known to affect their recommendations to families (Garbutt et al., 2023; Karlsson et al., 2019; Lin et al., 2021). Although the majority of participants in 2024 reported good self-perceived knowledge about the vaccine and to be able to inform families, 45% still expressed a desire for further education. Specifically, they voiced a need for more knowledge and training about how to address vaccine hesitancy, especially to counter religious and cultural concerns among parents, which is in line with previous studies (Enskär et al., 2023; Runngren et al., 2022). Furthermore, there is a need to increase evidence-based knowledge and eradicate common misconceptions, foremost of which is the idea that vaccination will lead to increased sexual risk behavior (Grandahl et al., 2017). Sadly, these misconceptions were also present among school nurses in this study.
The participants described that parents of children with neuropsychiatric disabilities had more questions and concerns. A recent Swedish nationwide registry-based study found a lower vaccination coverage among girls with mental illness and neurodevelopmental conditions (Hu et al., 2024). These findings call for further research to explore underlying barriers to vaccine acceptance among these children and their parents. This is especially important since Swedish women with severe mental illness participate less in cervical screening and have a doubled risk of invasive cervical cancer (Hu et al., 2023). Furthermore, HCPs may benefit from education about the effectiveness of the vaccine, the lack of serious side effects, the importance of timely vaccinations and the importance of also vaccinating boys (Grandahl & Nevéus, 2021).
Fear of needles is a barrier for vaccine acceptance both from the perspective of HCPs and children. The ability to prepare children and use strategies to manage children's fear facilitated vaccine acceptance, while a barrier was that this was time-consuming. School nurses involved in HPV vaccination should be enabled to address children's individual need of support rather than to optimize workflow (Lindén & Odenbring, 2022).
To increase awareness about legal aspects of consent practices and children's right to participation in health decisions may also support school nurses to ensure children's participation. It's important to note that children's participation is not identical to self-consent but involves the right for the child to be informed and to speak their mind. However, lack of awareness about the legal aspects of children's right to self-consent and about how to conduct a maturity evaluation of the child has previously been reported as possible barriers for children's participation and uptake of HPV vaccinations (Audrey et al., 2020; Fisher et al., 2019; Karafillakis et al., 2021; Zimet et al., 2021). It's crucial that HCPs are aware and confident about adolescents’ legal right to self-consent and for them to communicate this to adolescents (McNally et al., 2023; Zimet et al., 2021). It is noteworthy that the school nurses participating in the present study emphasized the importance of building trust with families. From their perspective, this also presents a challenge, as allowing children to self-consent may risk undermining parental trust. Our results indicate a need for medical law education and uniform legal interpretations, at policy level, for school nurses to adhere to.
Motivation
In line with previous studies, we found that school nurses’ views of their professional responsibility affected their work methods in terms of active outreach to hesitant parents and provision of providing additional offers to unvaccinated children (Enskär et al., 2023; McNally et al., 2023). To empower school nurses by emphasizing their key role for the success of the HPV vaccination program and the importance of their strong recommendations for parental decision-making may strengthen their professional pride. The need of public awareness campaigns has previously been raised and could strengthen their role (Dionne et al., 2023). In addition, they need a clarified mandate for vaccine promotion and reliable routines for when and how to contact hesitant families.
Strengths and Limitations
The sample in the current study was similar to the 2016 study, however the sample size was smaller compared to the 2016 study despite similar recruitment strategies. One possible explanation is the impact of the COVID-19 pandemic, which may have disrupted the daily work routines of school nurses. Currently, there is no available data specifying how many employed Swedish school nurses meet the eligibility criteria—namely, those involved in administering HPV vaccinations. Although HPV vaccination is primarily offered in fifth grade, unvaccinated children can receive the vaccine through school health services until the age of 18. Moreover, high staff turnover and regional variations in the organization of school health services further complicate efforts to estimate the total number of eligible school nurses. After consultation with a statistician, it was concluded that a formal pre-study sample size calculation was not feasible. Nevertheless, the sample was considered adequate due to its broad representation of school nurses from all 21 regions in Sweden.
As described, modifications have been made to the questionnaire since 2016, which limits comparability. However, given that NIPs and school health services evolve over time, it is important to adapt the questionnaire to reflect current practices. Additionally, the analysis of both quantitative and qualitative data provides deeper insight into barriers and facilitators at both individual and organizational levels.
Implications for School Nursing
Although HPV vaccine coverage is high in Sweden, continued efforts are necessary to ensure all children are protected against future HPV-related cancers. School nurses play a key role in the delivery of the HPV vaccination program, yet vaccination is a complex task and only one of many responsibilities they manage. The participating nurses reported good self-perceived knowledge and positive attitudes toward the HPV vaccine. However, they also expressed a clear need for further education and training, particularly in addressing vaccine hesitancy among parents. Additionally, lack of tailored tools and resources, such as culturally and linguistically appropriate informational materials and sufficient time allocated for vaccination-related tasks, limits their capacity to effectively promote, administer, and follow up on HPV vaccinations. Consistent with previous research (Enskär et al., 2023; Enskär et al., 2024; Runngren et al., 2022) our results show a variation in work methods, legal interpretations, views of professional responsibilities, and guidelines which suggest a lack of uniformity in provision of HPV vaccinations in the school-based program. This is worrying since it may affect the equity of the NIP. In alignment with the Immunization Agenda 2030 - ensuring no child is left behind -, and to achieve the goal of eliminating cervical cancer, further efforts to strengthen school health services are essential to promote equity in immunization programs (World Health Organization, 2020b). Based on our findings, we propose the following actions to strengthen the school-based HPV vaccination program and the school nurses key role for HPV vaccinations
employ uniform guidelines to improve equity in the immunization program. develop tailored informational tools and increase awareness of existing resources among school nurses. provide ongoing education and training on children's rights to participate in healthcare decisions, strategies to address vaccine hesitancy, techniques for managing needle fear, and ways to counteract common misconceptions about HPV vaccination – including among healthcare professionals. launch awareness campaigns emphasizing the importance of timely, gender-neutral vaccination and highlighting the school nurse's role as a trusted source of information.
Supplemental Material
sj-pdf-1-jsn-10.1177_10598405251374726 - Supplemental material for School Nurses’ Experiences of the School-Based HPV Vaccination Program – A Decade Later
Supplemental material, sj-pdf-1-jsn-10.1177_10598405251374726 for School Nurses’ Experiences of the School-Based HPV Vaccination Program – A Decade Later by Ida Enskär, Tryggve Nevéus, Karin Enskär, Carolina Källqvist and Maria Grandahl in The Journal of School Nursing
Footnotes
Acknowledgments
We are very grateful to all school nurses who participated in the study. We are also grateful to the coordinating nurses, heads of school health services, and the National Board of Swedish School Nurses for their support and help to facilitate contact with school nurses. We are thankful for the valuable feedback on the statistical analysis provided by Uppsala Clinical Research Centre.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Gillbergska stiftelsen, Cancerfonden, The Swedish Research Council funding for clinical research in medicine, (grant number No specific grant number, 130744, 19040/19046).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.