
Abstract
This study compared the effects of a plastic-free diet program, a plastic-free diet education program, and BPA exposure feedback on Bisphenol A levels in adolescents with high use of packaged products. As a result of the questionnaires, adolescents with “high” usage of plastic-packaged products and “low” attitudes toward healthy eating were assigned to intervention groups simple random sampling method (n = 108) and urinary samples were collected. Post-tests were conducted after the plastic-free diet was applied to intervention 1, the plastic-free diet education program and BPA exposure feedback to both Intervention 1 and Intervention 2, and BPA exposure feedback to Intervention 3. All interventions were effective in reducing urinary BPA levels, decreasing the use of plastic-packaged products, and improving attitudes toward healthy eating. Implementation implications: (a) training for school nurses and stakeholders, (b) education for adolescents and families, (c) collaboration with stakeholders, and (d) enhancing guidance and counseling in school health services.
Keywords
Introduction
Bisphenol A (BPA) is recognized as an endocrine-disrupting environmental chemical (Khan et al., 2023). It is widely used in the production of polycarbonate plastics and food packaging materials (Khan et al., 2023; Sessa et al., 2021). The primary route of human exposure to BPA is oral, as it can migrate from plastic products or food packaging into food and beverages (İnce et al., 2018; Sessa et al., 2021). The exposure rate varies based on gender and age; urinary BPA concentrations are higher in school-aged children compared to other age groups (Zhang et al., 2024) and in women compared to men (Kim et al., 2023). These differences are primarily attributed to dietary habits in children who spend time at school (Kim et al., 2023) and the use of personal care products in women (Zhang et al., 2024).
BPA exerts toxicological effects by altering signaling pathways and is a potential risk factor for various diseases. It can bind to hormone receptors, leading to structural and functional impairments in hormone-sensitive organs, and interact with cellular receptors, causing cellular dysfunction (Khan et al., 2023). A systematic review of meta-analyses revealed that BPA is associated with metabolic disorders and increases the risk of cardiovascular and allergic diseases (Lin et al., 2023). Another study employing the same methodology demonstrated that BPA is linked to insulin resistance, obesity, hypertension, cardiovascular diseases, and polycystic ovary syndrome in children (Symeonides et al., 2024). As part of the Sustainable Development Goals (United Nations, 2023), it aims to significantly reduce the number of deaths and illnesses caused by hazardous chemicals by 2030 (Target 3.9) and minimize their adverse effects on human health (Target 12.4).
Studies focused on prevention show that dietary interventions (Kim et al., 2020; Rudel et al., 2011; Sessa et al., 2021) and educational interventions (Kaplan et al., 2022; Kim et al., 2021; Park & Chung, 2021; Yang et al., 2023) are effective in reducing BPA exposure. However, evidence comparing the effects of multi-intervention approaches on urinary BPA levels in multiple study groups within a school context is limited. School nurses play a critical role in reducing BPA exposure, raising awareness, and implementing educational programs. School nurses can conduct effective interventions within the school setting to promote plastic-free and healthy eating behaviors. Taking into account the dynamic nature of the school environment, they are capable of assessing rapidly changing environmental conditions and identifying potential health threats. They can lead the implementation of necessary measures to improve school health. The implementation of environmental intervention programs by school nurses is of critical importance in achieving a safe school environment and a healthy school community. For this reason, the present study aims to evaluate the effects of a plastic-free diet program, a plastic-free diet education program, and BPA exposure feedback on Bisphenol A levels in adolescents with high packaged product use and to compare the effectiveness of these interventions.
Purpose of the Study
The purpose of the study is to compare the effects of a plastic-free diet program, a plastic-free diet education program, and BPA exposure feedback on Bisphenol A (BPA) levels in adolescents with high usage of packaged products. The study consists of two phases.
For the first phase, the specific research questions are:
What is the level of plastic-packaged product usage? What is the level of attitudes toward healthy eating?
For the second phase, the specific hypotheses are:
Adolescents who participate in the plastic-free diet program will have lower urinary BPA levels compared to those who participate in the plastic-free diet education program (Intervention 1/Intervention 2). Adolescents who participate in the plastic-free diet education program will have lower urinary BPA levels compared to those who only receive BPA exposure feedback (Intervention 2/Intervention 3). Adolescents who participate in the plastic-free diet program will have lower urinary BPA levels compared to those who only receive BPA exposure feedback (Intervention 1/Intervention 3).
Method
Study Design
A descriptive design was utilized to address the first-phase research questions, while a single-center, single-blind, non-randomized experimental design was employed to test the hypotheses in the second phase.
Study Context
The study was conducted in two high schools under the jurisdiction of the Ministry of Education in Antalya, Turkey. One of these schools included a girls’ dormitory. Intervention group 1 was applied to female students residing in the dormitory, Intervention group 2 to non-residential female students from the same school, and Intervention group 3 to female students from the other school.
Participants
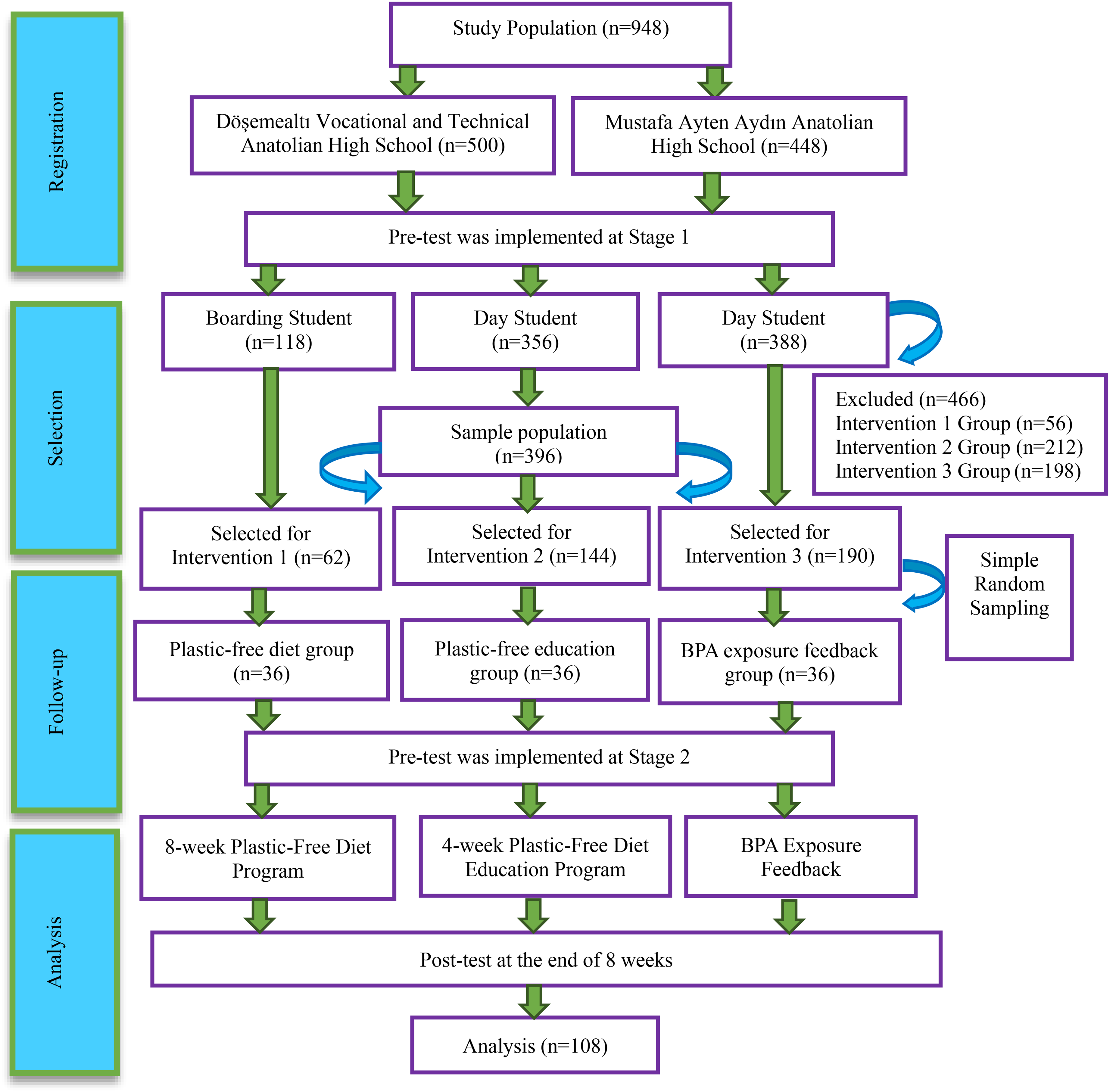
TREND (transparent reporting of evaluations with nonrandomized designs) flow chart.
Blinding
Participants in Intervention 1 were blinded to the plastic-free diet as they continued their routine meals in the dormitory without awareness of the intervention. Since participants in Intervention 1 and Intervention 2 attended the same educational program, they were unaware of which group they were in. Participants in Intervention 3, being from a different school, were unaware of the other groups. The primary researcher, who implemented the interventions, was not blinded. However, blinding was maintained during the evaluation of the results. Urinary BPA concentrations were assessed independently by researchers in a center unaware of the participants’ group assignments. Data analysis was conducted by a statistician who was also unaware of the interventions applied to the groups.
Data Collection
Interventions
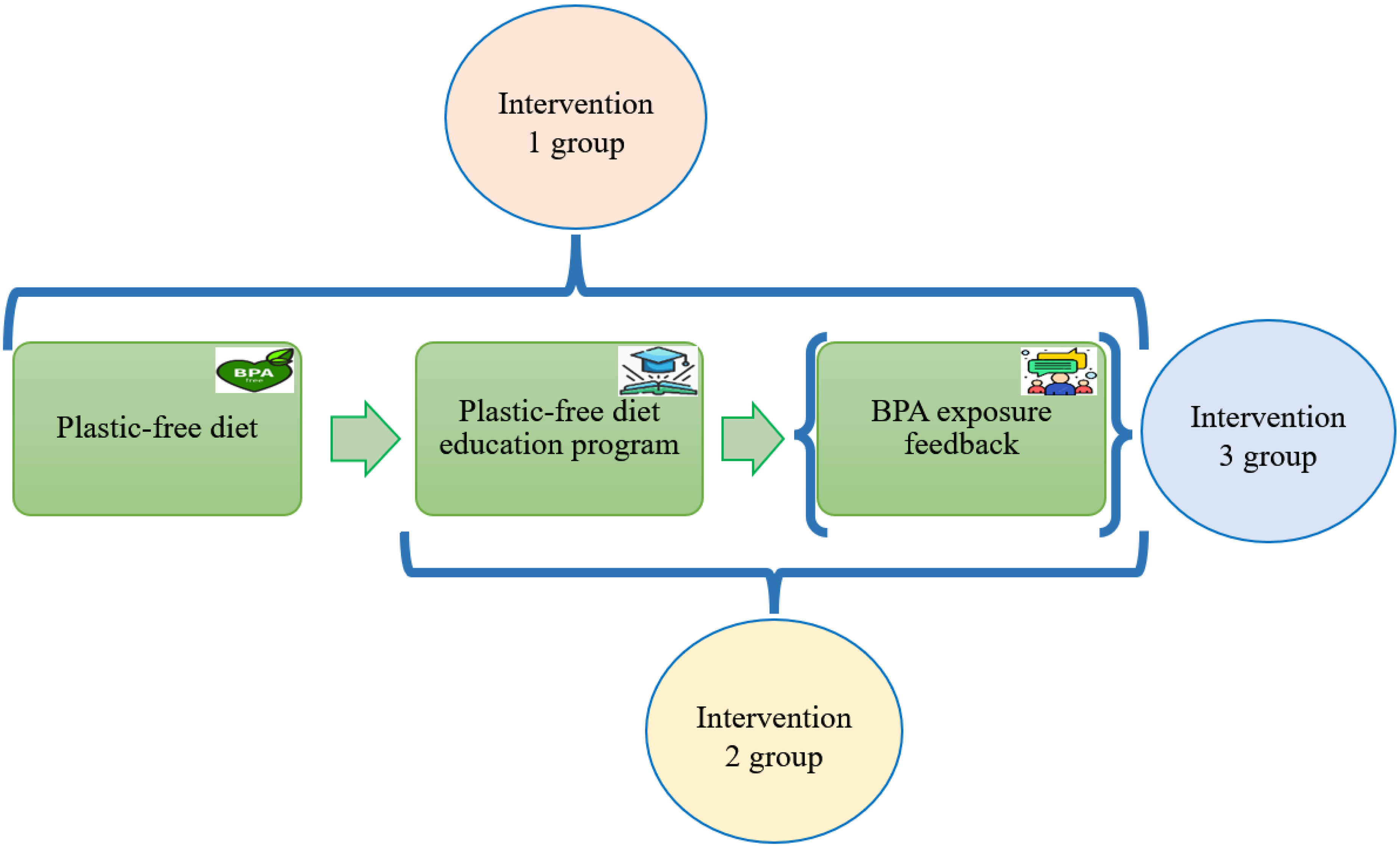
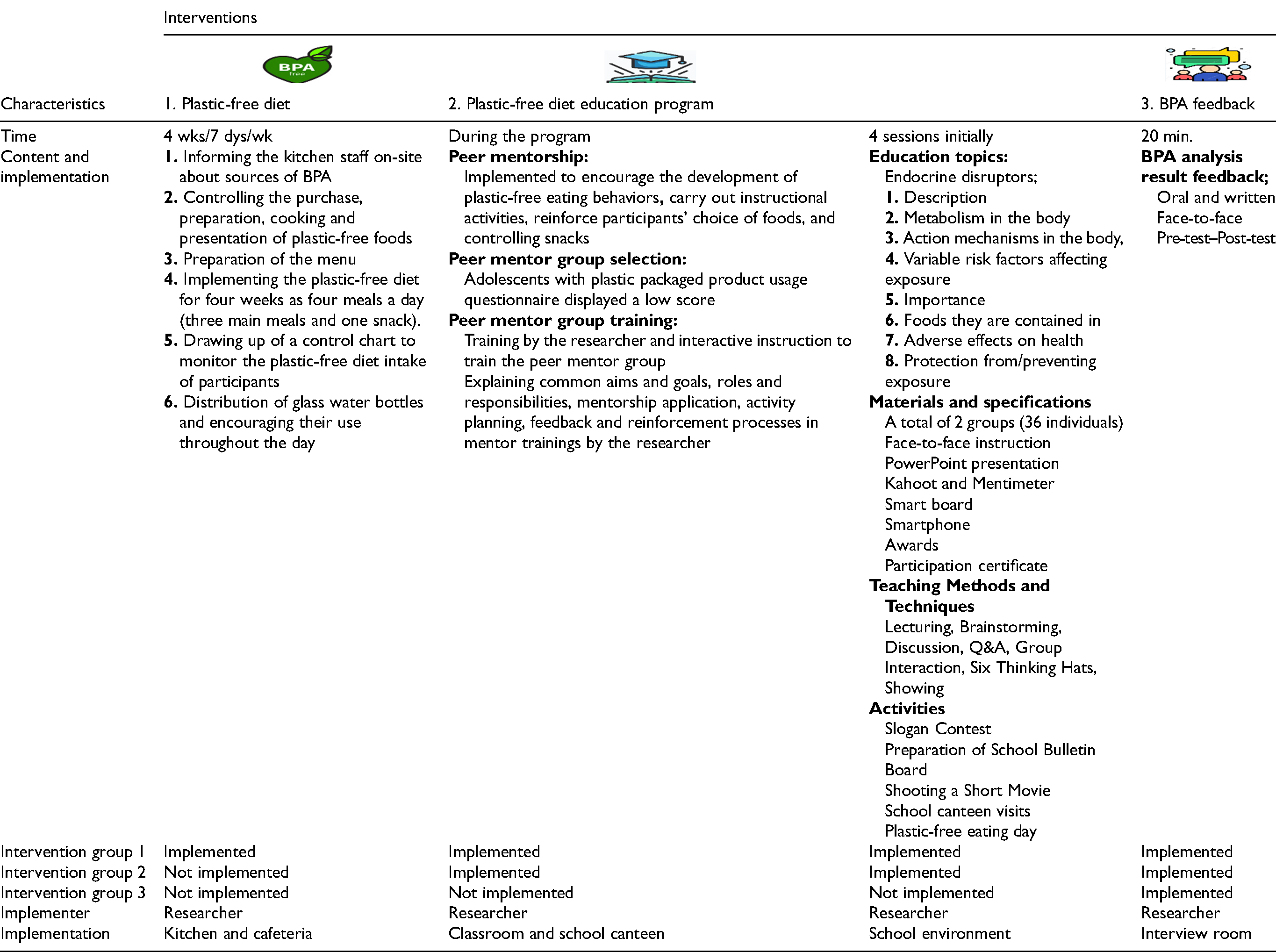
The interventions implemented in the plastic-free diet program included: (1) A plastic-free diet based on institutional regulations; (2) A peer mentorship based plastic-free diet education program focusing on individual empowerment; (3) BPA exposure feedback aimed at raising awareness. All three interventions were applied in Intervention 1, the plastic-free diet was excluded from Intervention 2 along with the other two interventions, and BPA exposure feedback was applied in Intervention 3 (Figure 2 and Table 1).
Initiatives by working groups.
Plastic-Free Diet Program.
Intervention Group 1: Plastic-Free Diet Program (Plastic-Free Diet, Plastic-Free Diet Education Program and BPA Exposure Feedback).
1. Plastic-Free Diet
The practices implemented in the plastic-free diet were as follows: (1) Before starting the diet, the dormitory kitchen staff received practical training on BPA sources. The kitchen was checked for plastic materials and replaced with non-plastic alternatives. Stainless steel products were used for food preparation and serving. A suitable kitchen environment was created for the plastic-free diet. (2) In line with the dormitory food procurement tender, some products previously packaged in plastic were replaced with glass jar alternatives (e.g., jam, honey, chocolate, coffee, powdered milk, etc.). (3) With the support of the assistant dormitory manager, the meal menu was prepared. (4) A control checklist indicating that the Intervention group 1 participants were on the plastic-free diet was created. After setting all the conditions, the plastic-free diet, consisting of four meals per day (three main meals and one snack), was applied to the Intervention group 1 under the supervision of the first author after the plastic-free nutrition education program (Table 1). After all conditions were established, a plastic-free diet education program and BPA exposure feedback were implemented, and a four-week plastic-free diet consisting of four meals per day (three main meals and one snack) was applied to the Intervention group 1 under the control and supervision of the first author (Table 1). According to the school dormitory rules, students were prohibited from leaving the school grounds without parental permission outside of school hours. Therefore, the control of ready-to-eat foods purchased outside the school canteen was ensured.
2. Plastic-Free Diet Education Program
Before the plastic-free diet intervention, face-to-face education was provided to Intervention 1 (n = 36), Intervention 2 (n = 36) groups, and peer mentors (n = 18) in four sessions. The educational topics covered endocrine-disrupting chemicals (EDCs), including their definition, metabolism in the body, mechanisms of action, modifiable risk factors affecting exposure, their importance, foods they can be found in, their negative effects on health, and prevention of exposure. The teaching methods used included lecture, brainstorming, discussion, Q&A, group interaction, six thinking hats method, and demonstration. A PowerPoint presentation on these topics was displayed on the smartboard. To enhance active participation and facilitate learning, online web 2.0 tools such as Kahoot and Mentimeter were used. Assessment activities aligned with the educational content were prepared. Throughout the program: (a) A slogan competition was organized every week, a school board was prepared, and a plastic-free eating day was organized; (b) A short film was prepared and filmed during the program; (c) In the final week of the program, visits to the school canteen were organized (Table 1).
After completing these educational sessions, glass water bottles were gifted to participants from both Intervention 1 and Intervention 2, and participation certificates were provided.
Plastic-Free Diet Education Program Activities
3. BPA Exposure Feedback
All participants in the study received feedback on their urinary BPA analysis value results, both from the pre-test and post-test. The feedback was provided face-to-face, with 20 min allocated to each participant for verbal and written communication. During the feedback session, participants were informed about BPA, the meaning of urinary BPA levels was explained, questions were answered, and individual attention was given to each adolescent. Feedback was provided in a private setting where the participant was alone (Table 1).
Instrumentation
In the first phase of the study, outcome data were obtained from the participant data form, the level of plastic-packaged product usage, and attitudes toward healthy eating. Additionally, urinary BPA level was evaluated as the primary outcome in this phase. In the second phase of the study, only the urinary BPA level was used as the outcome measure.
Data Analysis
Ethical Considerations
The study was conducted following the guidelines outlined in the Declaration of Helsinki, and it was approved by the Clinical Research Ethics Committee of Akdeniz University Faculty of Medicine (21.09.2022/572) and the Antalya Provincial Directorate of National Education (10.11.2022/63240970). Informed consent was obtained from both participants and their legal guardians in both phases of the study.
Results
In the first phase of the study, 862 responses were obtained for the survey and scale. After identifying outliers and removing participants who exhibited extreme values, a total of 826 responses were analyzed. A total of 108 participants were included in the second phase of the study, and all of them were analyzed.
First Phase Research Findings
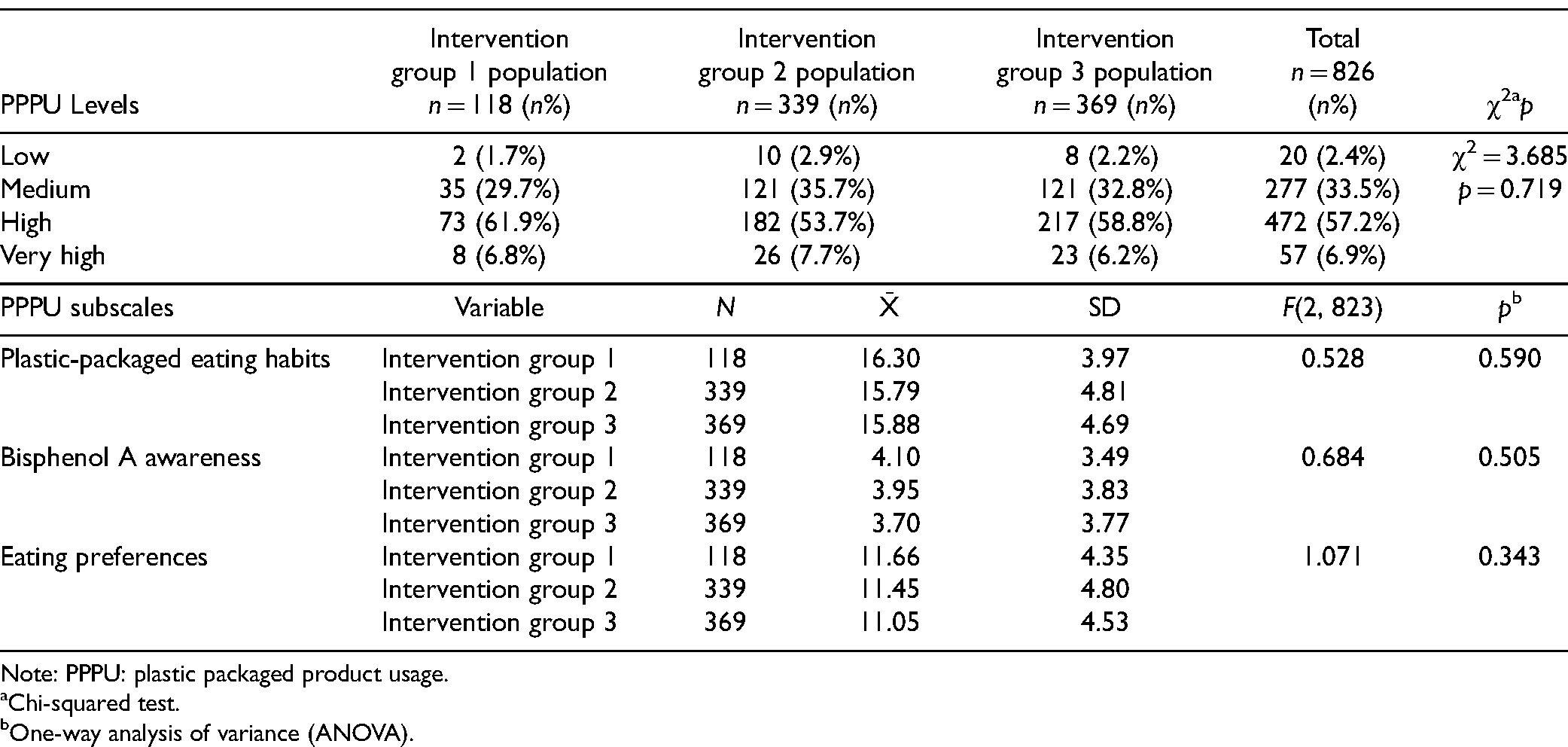
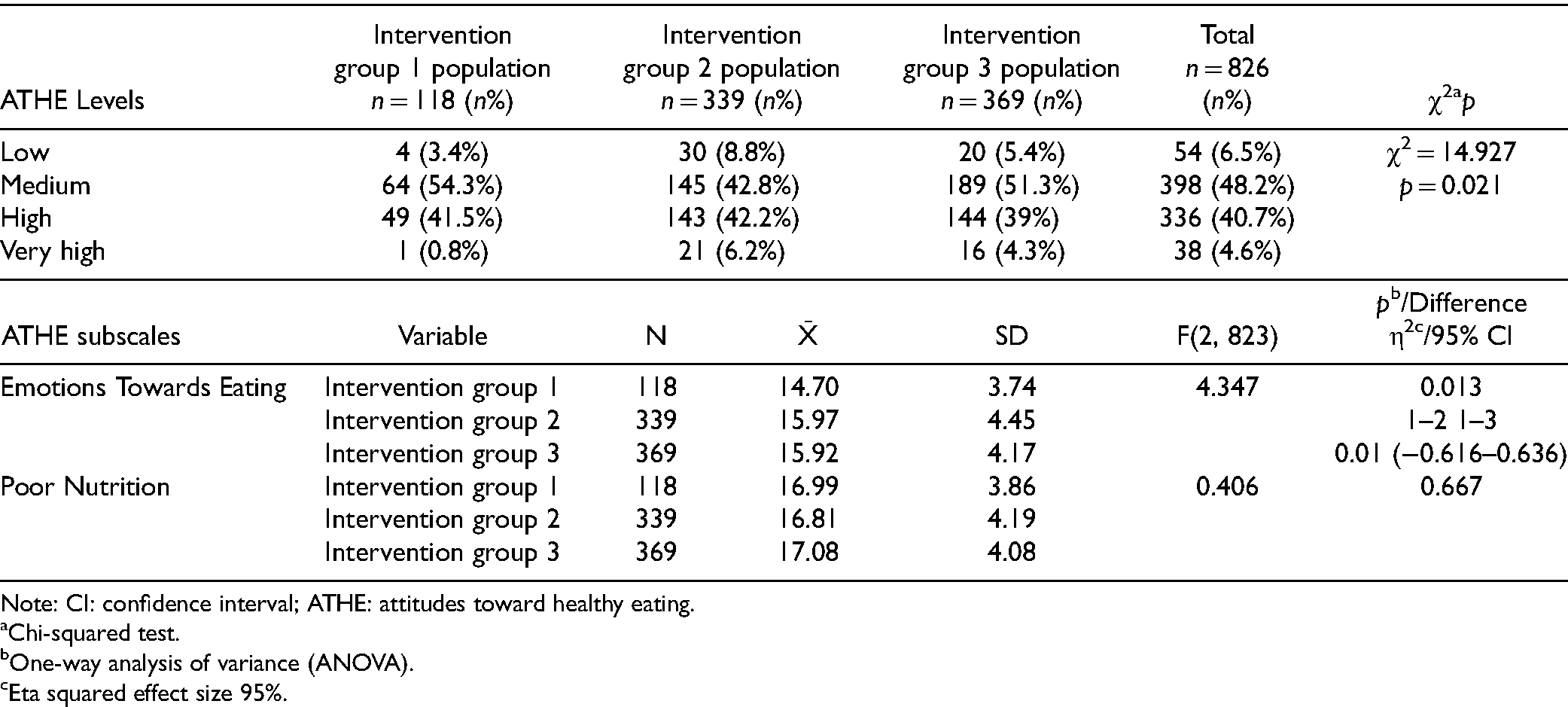
The distribution of participants’ plastic-packaged product usage levels and attitudes toward healthy eating are presented in Tables 2 and 3.
Distribution of Participants According to Their Use of Plastic Packaged Products.
Distribution of Participants According to Their Attitudes Towards Healthy Eating.
Second Phase Research Hypothesis Findings
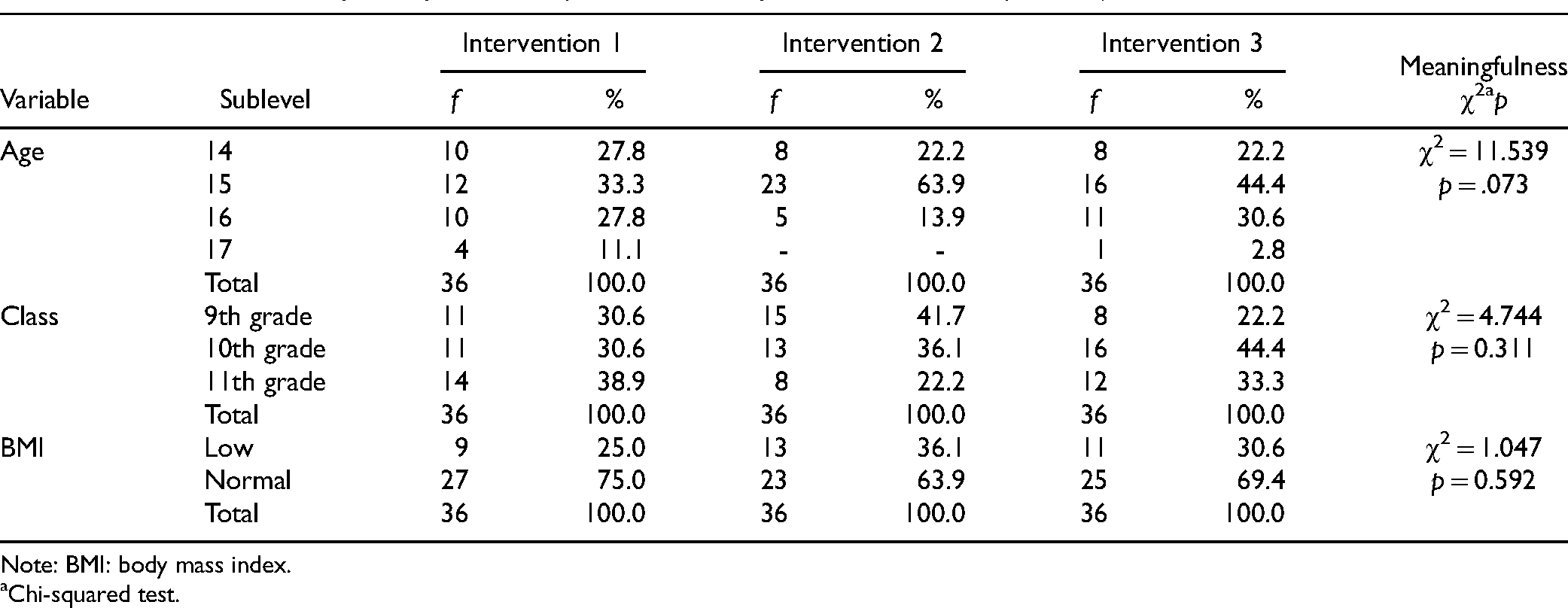
Table 4 shows the distribution of participants’ age, grade, and BMI. Statistical analysis revealed no significant differences between the groups. The average age of the study groups was: Intervention 1 = 15.22 ± 0.99, Intervention 2 = 14.92 ± 0.60, and Intervention 3 = 15.14 ± 0.80.
Distribution of Study Groups According to Their Descriptive Characteristics (Pre-Test).
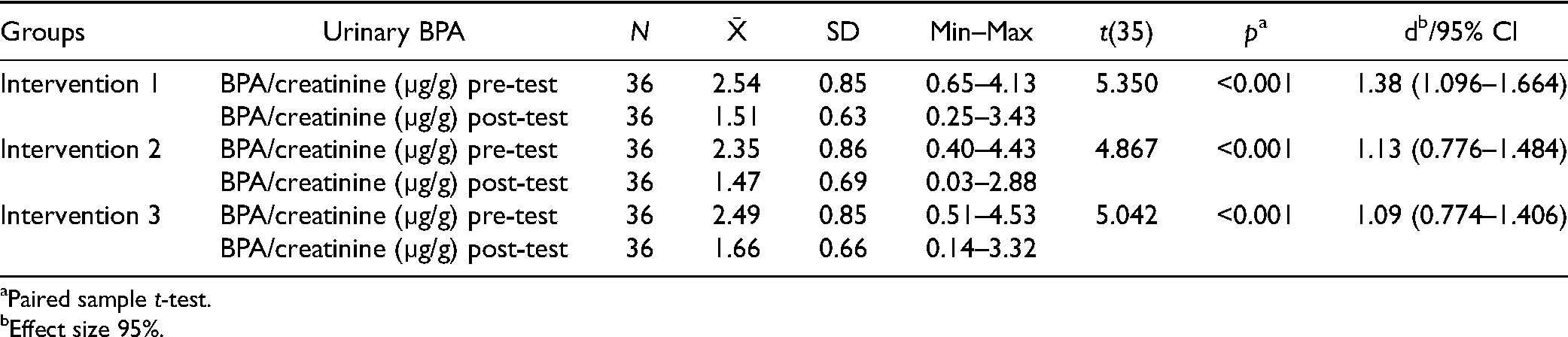
The pre-test BPA/creatinine (µg/g) values of the participants were close to each other, and no significant differences were observed between the groups (p = 0.624) (Table 5). The post-test urine BPA levels were found to be: Intervention 1 = 1.51 ± 0.63 μg/gcreatinine, Intervention 2 = 1.47 ± 0.69 μg/gcreatinine, and Intervention 3 = 1.66 ± 0.66 μg/gcreatinine. While BPA/creatinine (µg/g) values decreased from the pre-test to the post-test, no significant differences were found between the groups (p = 0.414) (Table 6). However, a significant time-dependent difference was observed within-sample difference groups’ pre-test and post-test BPA/creatinine (µg/g) values (p < 0.001) (Table 7).
BPA/Creatinine (µg/g) Levels of the Study Groups (Pre-Test) (n = 108).

BPA/Creatinine (µg/g) Levels of the Study Groups (Post-Test) (n = 108).

BPA/Creatinine (µg/g) Levels of the Study Groups (Pre-Test–Post-Test).
Discussion
1st Phase Research Questions
Plastic-Packaged Product Usage Levels
In both schools where the study was conducted (n = 826), more than half of the adolescents were found to have “very high” and “high” levels of plastic-packaged product usage (Table 2). The high consumption of plastic-packaged products by adolescents can be explained by the absence of lunch in both schools (except for students in the dormitory) and the fact that the school canteens predominantly sell plastic-packaged food.
Similar results were found in other studies that reported the levels of plastic-packaged product usage. In a pilot study conducted with Italian schoolchildren, most of the participants (n = 65) reported “high” and “medium-high” levels of plastic-packaged eating habits, and only 12% had “medium” level usage. No participants reported “low” usage, and only 12% exhibited virtuous plastic-packaged product usage behavior (Sessa et al., 2021). A national bio-monitoring study conducted with schoolchildren in Austria (aged 6–10, n = 85) found that 60% of children had fast-food consumption habits (Hartmann et al., 2023).
Similar behaviors have been observed in adolescents in other studies, consistent with the questions about eating habits in plastic packaging in the questionnaire applied in the study. In a large-scale study conducted in China, 48% of the population reported consuming take-out food at least once a week, and 75% had the habit of drinking bottled plastic water (Huang et al., 2023). A global meta-analysis of adolescent diets found that approximately half of adolescents consume soft drinks at least once a day (43%) and fast food at least once a week (46%) (Beal et al., 2019).
Both the literature and this study's findings show that adolescents have high levels of plastic-packaged product usage. This suggests that a significant portion of BPA exposure in adolescents could be diet-related. The overall picture reveals that plastic-packaged eating habits present a substantial risk to children's present and future health. Therefore, there is a need for packaging that does not contain BPA, along with improvement programs in school cafeterias, taking into account ready-to-eat food and packaged food consumption habits.
Attitudes Toward Healthy Eating
It was found that approximately half of the adolescents exhibited unhealthy eating attitudes (Table 3). Additionally, 23% of participants were underweight, 63% had normal weight, and 14% were overweight or obese. This is also consistent with findings from another study examining healthy lifestyle behaviors, which found that adolescents in health schools did not have very good healthy lifestyle behaviors and unhealthy eating behaviors were prevalent (Akcan & Ulusoy, 2023). Due to the limited sources on the sub-dimensions of emotion toward nutrition and poor eating behaviors, a full comparison with other studies could not be made.
Second-Phase Research Hypotheses
At the end of the study, BPA/creatinine levels significantly decreased between the pre-test and post-test within-sample difference groups (Table 7). All three interventions (plastic-free diet program, plastic-free diet education program, and BPA exposure feedback) were effective in significantly reducing the adolescents’ urine BPA concentrations. There were no significant differences between the groups, and the urine BPA concentrations of all groups were similarly reduced. Effect size analysis suggests that the plastic-free diet program was more effective than the plastic-free diet education program, and the plastic-free diet education program was more effective than BPA exposure feedback in reducing urine BPA/creatinine levels. Nevertheless, the interventions were only marginally different, and all were effective in reducing urine BPA/creatinine values. Even just providing BPA exposure feedback Intervention group 3 was sufficient to induce a change in urine BPA levels.
Plastic-Free Diet Program: Plastic-Free Diet
Adolescents in the plastic-free diet program did not have lower urinary BPA levels compared to those in the plastic-free diet education program. A more significant reduction in urinary BPA/creatinine levels (pre-test to post-test) was observed in Intervention group 1 compared to Intervention group 2. This effect is thought to be attributed to the implementation of the plastic-free diet. However, in the study, it was the most time-consuming intervention, requiring follow-up, difficult to control, and challenging to implement. In a study aimed at identifying effective interventions to reduce exposure to diet and personal care products, it was reported that dietary interventions were generally successful in reducing BPA levels (Yang et al., 2023). Looking at other studies that applied nutritional interventions, it was found that diet was effective in reducing BPA levels, with interventions ranging from two days to six months (Bae & Hong, 2015; Gonzáleza et al., 2020; Kim et al., 2020; Kim et al., 2021; Park & Chung, 2021; Peng et al., 2019; Rudel et al., 2011; Sessa et al., 2021).
Studies conducted with different aims and designs have demonstrated that diet plays an influential role in both increasing and reducing BPA exposure. Similarly, in this study, the plastic-free diet was effective in reducing urinary BPA levels among adolescents in the Intervention group 1. Providing BPA exposure feedback to all groups is believed to have had a significant impact, potentially contributing to the lack of difference observed between the groups. School nurses may utilize a plastic-free diet to improve school health, depending on the feasibility of field conditions and economic factors.
Plastic-Free Diet Program: Plastic-Free Diet Education Program
Adolescents in the plastic-free diet education program did not have lower urinary BPA levels compared to those who were only given BPA exposure feedback. The reduction in urine BPA/creatinine levels (pre-test to post-test) in Intervention groups 1 and 2 was more significant than in Intervention group 3. This demonstrates the difference made by the plastic-free diet education. The plastic-free diet education program played an important role in raising awareness and initiating behavior change among adolescents. This positive effect was reflected in the urinary BPA values as well. It is the most cost-effective, easily implemented, and repeatable intervention among interventions. In the absence of facilitating regulations, it is thought that informative practices aimed at protecting individuals are much more cost-effective and valid. When the cost of urinary BPA analysis is disregarded, BPA results feedback is the least time-consuming and most easily implemented intervention.
In a scoping review study, it was reported that educational intervention studies were an effective intervention in reducing urinary BPA levels (Yang et al., 2023). Other studies have also shown that educational interventions are effective in reducing BPA exposure (Kaplan et al., 2022; Kim et al., 2021; Park & Chung, 2021). A study involving literature-based dietary guidance for adolescents reported no significant change in urinary BPA levels. It has been stated that the lack of labeling information on packaged foods makes it difficult to avoid BPA exposure at the individual level (Galloway et al., 2018).
In this study, the plastic-free diet education program raised awareness among all school students through activities conducted with participants from Intervention groups 1 and 2. However, challenges such as limited access to non-plastic-packaged food and beverages in the school environment, the higher cost of glass products, and unavoidable BPA contamination from production in food products might have prevented a significant difference between the groups in terms of urinary BPA levels. Although individual efforts brought about change, environmental interventions are needed for further improvements.
Throughout this study, peer mentorship was implemented within the plastic-free diet education program in Intervention groups 1 and 2. In an experimental study, peer support through social network communication was used within a four-week dietary intervention to share experiences and reinforce behavior, and it was found to be effective in reducing BPA levels (Park & Chung, 2021). Similarly, in this study, intentional peer recommendations and guidance positively influenced the health behaviors of other peers. It is recommended that such methods be used in future studies. The study concluded that the use of plastic-packaged products and BPA exposure are responsive to educational interventions. School nurses can play a vital role in protecting and promoting school health and preventing diseases by providing health education aimed at reducing environmental health risks.
Plastic-Free Diet Program: BPA Exposure Feedback
Adolescents who participated in the plastic-free diet program did not have lower urinary BPA levels compared to those who were only given BPA exposure feedback. The reduction in urine BPA/creatinine levels (pre-test to post-test) in Intervention groups 1 and 2 was more significant compared to Intervention group 3. Furthermore, it was found that the urine BPA levels (pre-test-post-test) in Intervention group 3 significantly decreased. The feedback on the urinary BPA results provided to the adolescents increased their sensitivity to health risks and helped create individual perceptions of this risk, ultimately influencing behavior change. This study for the first time demonstrated that providing BPA exposure feedback alone can be an effective intervention in reducing exposure. No other studies have been found in the literature that have provided participants with urine BPA feedback similar to this study.
A study conducted with female university students in Korea found that a small-group, education-based dietary intervention incorporating self-assessment, solution development, and self-committing resulted in a decrease in urinary BPA levels (Park & Chung, 2021). A study conducted in the Netherlands compared a basic nutrition education intervention and an intervention including environmental feedback with a control group. The findings indicated that both types of education were effective in changing dietary behaviors; however, environmental feedback was found to be particularly more effective in increasing fruit consumption and reducing the intake of unhealthy snacks (Springvloet et al., 2015). In addition to individual-level factors, environmental regulations and feedback can play a driving role in influencing behavior. Based on the effect on urinary BPA levels, this intervention alone created awareness and behavior change among adolescents. Since all three interventions were effective in reducing urinary BPA/creatinine levels, school nurses and other health professionals can implement the intervention that best fits their working conditions. The study may contribute to enhancing school nurses’ awareness of environmental health risks and their collaboration skills.
Conclusions
The results showed that providing BPA exposure feedback alone, without applying a plastic-free diet or plastic-free diet education, significantly reduced urinary BPA concentrations. Both the plastic-free diet and plastic-free diet education interventions were also effective in reducing adolescents’ urinary BPA levels. The results demonstrate that the plastic-free diet program, plastic-free diet education program, and BPA exposure feedback interventions significantly reduced urinary BPA levels in adolescents. To reduce exposure further, individual protective behaviors should be supported by measures taken by authorities related to food preparation, packaging, and the promotion of non-plastic products.
Implications for School Nursing and Future Research
School nurses should prioritize health education, as adolescents’ consumption of plastic-packaged products and healthy eating habits are sensitive to plastic-free diet education. This can contribute significantly to the protection, improvement of public health, and disease prevention within the school community. School nurses should motivate adolescents to continue plastic-free eating habits to sustain healthy lifestyles. To establish healthy nutritional environments in schools, it is essential to ensure the active participation of parents and all school staff in educational, leadership, and counseling processes. Limiting the availability, presentation, and sale of plastic-packaged products in school food services and vending machines may serve as an effective measure to reduce plastic usage. Additionally, schools can contribute to the development of relevant policies and regulations by adopting an advocacy role against BPA-containing packaging. Schools have a significant role in ensuring access to safe food and promoting healthy eating habits. These efforts facilitate better health outcomes both during adolescence and later in life. Furthermore, they enhance school nurses’ awareness of environmental health risks and support their collaboration with other health and environmental professionals. The results emphasize the importance of school nurses’ preventive interventions in reducing adolescent BPA exposure.
The study compared adolescents’ urine BPA levels before and after the interventions, but the long-term or short-term effects on adolescent health were not examined. Therefore, it is recommended that comprehensive prospective studies be conducted to assess the negative health effects of BPA exposure.
Limitations
Since the plastic-free diet for Intervention group 1 was provided at the lowest cost, randomization could not be performed. The inability to fully control participants’ eating behaviors in real life and eliminate all sources of BPA exposure was a limitation of the interventions. Implementation difficulties included obtaining written permission from the school administration at every stage of the intervention, informing all school staff, and managing the challenges of the school environment. The adolescents’ plastic-packaged product usage habits were based on self-reported surveys, which may not reflect actual exposure. Contamination from other equipment was not reported when explaining urinary BPA values. Due to the sample size and results being limited to two high school groups, the findings cannot be generalized.
Supplemental Material
sj-docx-1-jsn-10.1177_10598405251340397 - Supplemental material for Comparison of the Effects of Plastic-Free Diet, Plastic-Free Diet Education and Exposure Feedback on Urinary Bisphenol: A Levels in Adolescents
Supplemental material, sj-docx-1-jsn-10.1177_10598405251340397 for Comparison of the Effects of Plastic-Free Diet, Plastic-Free Diet Education and Exposure Feedback on Urinary Bisphenol: A Levels in Adolescents by Fatma Ulusoy, Sebahat Gözüm and Mesut Parlak in The Journal of School Nursing
Footnotes
Acknowledgments
The authors are very grateful to the students who contributed to this study.
Author Contribution(s)
Author's Note
The protocol was registered in the Clinical Trials website (https://clinicaltrials.gov) (Trial number: NCT05746130). The study was presented as a poster at the 17th European Public Health Conference 2024 Lisbon, Portugal. Eur J Public Health. 2024 Oct 28;34(Suppl 3): ckae144.1512. doi: ![]() .
.
Data Availability
The present study consists of two phases, and datasets for both phases are available. However, as not all of the data analyzed from these datasets could be included in this article, data sharing is not applicable to this publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This manuscript was based on the first author's PhD thesis under the supervision of other authors. The thesis was supported by Akdeniz University Scientific Research Projects Coordination Unit with the project number TDK-2023-6702.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.