
Abstract
Understanding the school nurse's experience in human papillomavirus (HPV) vaccine promotion can reduce vaccine disparities. HPV vaccination is critical to cancer prevention. Despite the importance of the school nurse in vaccine promotion, there is a lack of understanding. This article aims to examine the knowledge, attitude, experience, and role of school nurses related to HPV vaccination and promotion in school settings. A systematic search for school nurses and their experiences related to HPV vaccination was conducted. A thematic synthesis was undertaken using the socioecological model. This review highlights the complexity of HPV vaccine promotion in schools over time. Multilevel factors impact nursing practice. Nurses have good vaccine knowledge and positive attitudes. Poor workflow processes, competing demands, and vaccine communication challenge school nurses. The themes that were synthesized informed the LEADS model. With the support of school nurses, reaching the goal of eliminating cervical cancer as a public health problem is possible.
Introduction
Certain cancers are strongly associated with common infections caused by the human papillomavirus (HPV), but many cases are vaccine preventable (Arbyn et al., 2018; Shing et al., 2022). HPV infects more than 13 million Americans each year with most infections occurring in late teens or early twenties (Centers for Disease Control and Prevention [CDC], 2023; National Cancer Institute [NCI], 2023). Many infections are asymptomatic, but approximately 10% become persistent and progress to cancer (US Food and Drug Administration [FDA], 2019). In 2018 an analysis of global data showed there were approximately 570,000 cases of cervical cancer and 311,000 deaths from the disease. Cervical cancer is the leading cause of cancer-related death for women living in certain parts of Africa (Arbyn et al., 2020). Additionally, the NCI (2023) attributes 70% of oropharyngeal and 90% of penile cancers to HPV infection. Although many cases can be prevented, HPV-related cancers continue to pose a major threat to global public health. Disease prevention and health promotion fall under the Community/Public Health principle in the National Association of School Nurses’ (NASN) Framework for 21st Century Nursing Practice™ (NASN, 2020). School nurses are heavily involved with promoting timely vaccination to adolescents (Patel et al., 2018). With adolescences as the target group for HPV prevention efforts, school nurses are central to HPV cancer elimination.
HPV vaccine completion rates differ globally for adolescents with Australia at 80.2% compared to the United States at 46% (Spayne & Hesketh, 2021). HPV vaccine coverage in Japan has remained low (<1%) due to public resistance and safety concerns (Haruyama et al., 2022). With high vaccine coverage, Australia is on track to eliminate cervical cancer as a public health problem by 2035. The success is largely due to high vaccine accessibility and school-based efforts (Brotherton et al., 2016; Hall et al., 2019). It remains critical to improve vaccination because certain HPV-related cancer diagnoses have risen recently in the United States (Francoeur et al., 2022; Liao et al., 2022; Yu et al., 2019). Due to the strong relationship between HPV infection and cervical cancer, female sex was central to early vaccine research and promotion. Health communication and vaccine behavioral experts proposed that the early gendering of the vaccine lowered acceptance among parents/guardians (Daley et al., 2017; Jit et al., 2014). Over time the link between HPV infection and other cancers led to inclusive vaccination campaigns. Unfortunately, inclusion of males in vaccination efforts did not normalize the HPV vaccine, which is evidenced by consistently higher rates of other adolescent vaccines like tetanus, diphtheria, pertussis, and meningitis (Bernstein et al., 2016; Daley et al., 2016, 2017). After 15 years of inclusive licensure, it is logical to question how gender and sex influence school nurses’ HPV vaccine promotion.
Despite the vital role school nurses play in adolescent HPV vaccination efforts, a global understanding of school nursing practice related to HPV vaccination promotion and administration is limited. A better understanding of school nurses’ experience with HPV vaccination activities is needed. Therefore, the purpose of this review is to systematically review the existing body of literature to aggregate, analyze, and summarize all relevant findings reported in scholarly publications that include school nurses’ experiences and roles in promoting and administering the HPV vaccine. The aim is to understand how multilevel factors affect the experience and role of school nurses related to HPV vaccination and promotion in school settings. Additionally, this review will examine how the biological sex of the adolescent influenced vaccine promotion.
Socioecological Model
Ecological models highlight how people interact with social and physical environments around them. The socioecological model (SEM) is a theory-based framework used in both quantitative and qualitative research studies to understand how behavior is shaped along a continuum of macrolevel and microlevel factors (Thomas & Harden, 2008; Uchendu et al., 2020; Webster et al., 2013). The multilevel framework helps conceptualize how relationships, communities, organizations, and policies shape individual behavior while asserting that health behavior is influenced by individual and environmental factors. SEM is used in multiple disciplines and is frequently employed to guide policy development and design interventions (Henderson & Baffour, 2015; Richard et al., 2011). Utilizing the SEM for data synthesis is based on the belief that school nursing practice is influenced by individual factors and the social and ecological environments where nurses live and work (McLeroy et al., 1988; Uchendu et al., 2020).
Methods
A systematic qualitative literature review was conducted using the Guide to Writing a Qualitative Systematic Review Protocol to Enhance Evidence-Based Practice in Nursing and Health as a guide (Butler et al., 2016). The review protocol was registered with PROSPERO (reference no. CRD42023391173). The George Mason University Institutional Review Board declared this study [2057726-1] exempt from review.
Search Strategy
To accomplish the aims, a thorough review of the literature was conducted by the main author. The databases MEDLINE, PubMed, and CINAHL were searched in March 2023 using the keywords: “Human papillomavirus”, “HPV”, “School Nurse”, “Nurse”, “Vaccine”, “Immunization”, “Adolescent Health”, “Child Health”, and “Cancer Prevention”. Included articles were English language, full-text, peer-reviewed, and published after the year 2006. The date range for included articles was from 2006 to March 2023. The HPV vaccine was originally licensed for use in the United States in 2006. Publications had to include participants who identified as school nurses and were involved with administering, promoting, and/or ensuring compliance with HPV vaccination among adolescents in school settings. Observational studies (e.g., prospective cohort, retrospective cohort, case-control, and cross-sectional), descriptive studies (e.g., ecological and survey), and qualitative studies (e.g., interviews and focus groups) were included. Studies were excluded if the research was conducted prior to HPV vaccine licensure in 2006. Research conducted only in clinical settings, articles that are focused on adult HPV vaccination, and/or those that do not include school nurses as participants were excluded. Studies that do not explicitly include school nurses were excluded. Experimental studies (e.g., randomized-controlled trials) and interventions were excluded.
Study Selection
The initial search of the databases resulted in 273 records. Automated search tools were used to reduce the records to English language, full-text, and peer-reviewed records. Publications eliminated before screening are noted with the PRISMA flow diagram (Figure 1) as records/reports marked as ineligible by automation tools (Page et al., 2021). Records (n = 57) that were not excluded by the automated tools were screened and books, commentaries, editorial, and single nurse interviews were removed. Remaining records (n = 31) were screened first by reviewing the title and abstract. Five records were excluded because the inclusion criteria were not met. Full-text review of the remaining articles (n = 26) was conducted, and two additional articles were included from reference list review. A total of 28 articles were selected for inclusion in the review.
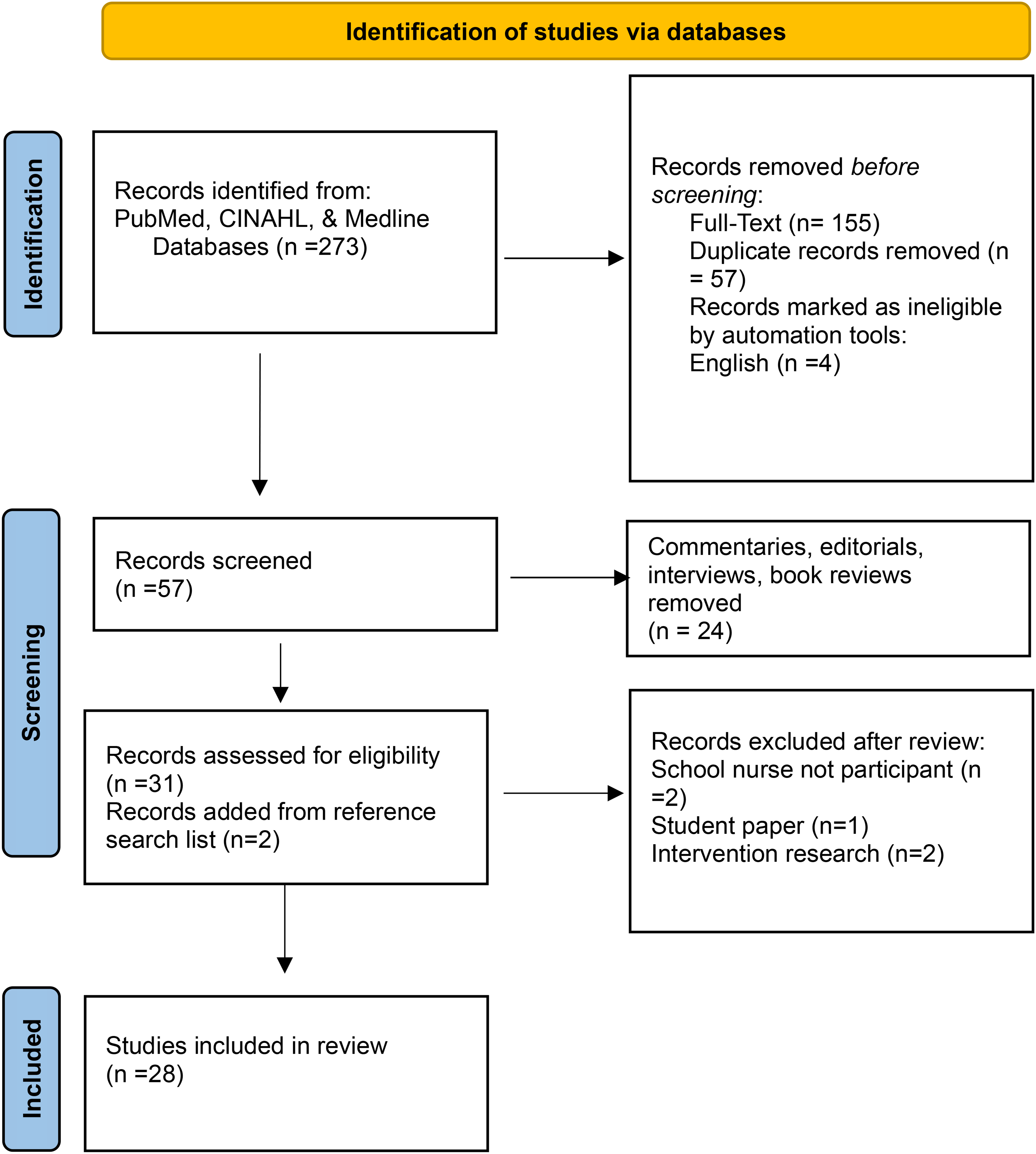
PRISMA 1 flow chart.
Quality Assessment
The quality of each study included in the review was assessed by two authors using a modified Critical Appraisal Skills Program Qualitative Checklist. Minor modifications were made to the checklist to allow for consistent assessment of quantitative, qualitative, and mixed-method studies. For example, the question, “Is a qualitative methodology appropriate” was modified to “Is the research methodology appropriate” (Butler et al., 2016; Critical Appraisal Skills & Programme, 2018). The checklist responses were quantified with each article being assessed and scored as 1 point for yes, 0.5 points for unsure, or 0 points for no for each question. Articles were classified as high quality (score: 9–11), moderate quality (score: 7.5–9), or low quality (score <7.5). Any paper that was scored below the low-quality threshold was excluded. Studies ranged from 8.5 to 11 points. All studies were considered adequate for inclusion. Only two studies explicitly considered the relationship between the researcher and the participants, however anonymized surveys can be deduced to have no relationship between the participant and the researchers. The complete quality assessment rubric can be found in Table 1.
Quality Assessment Rubric.
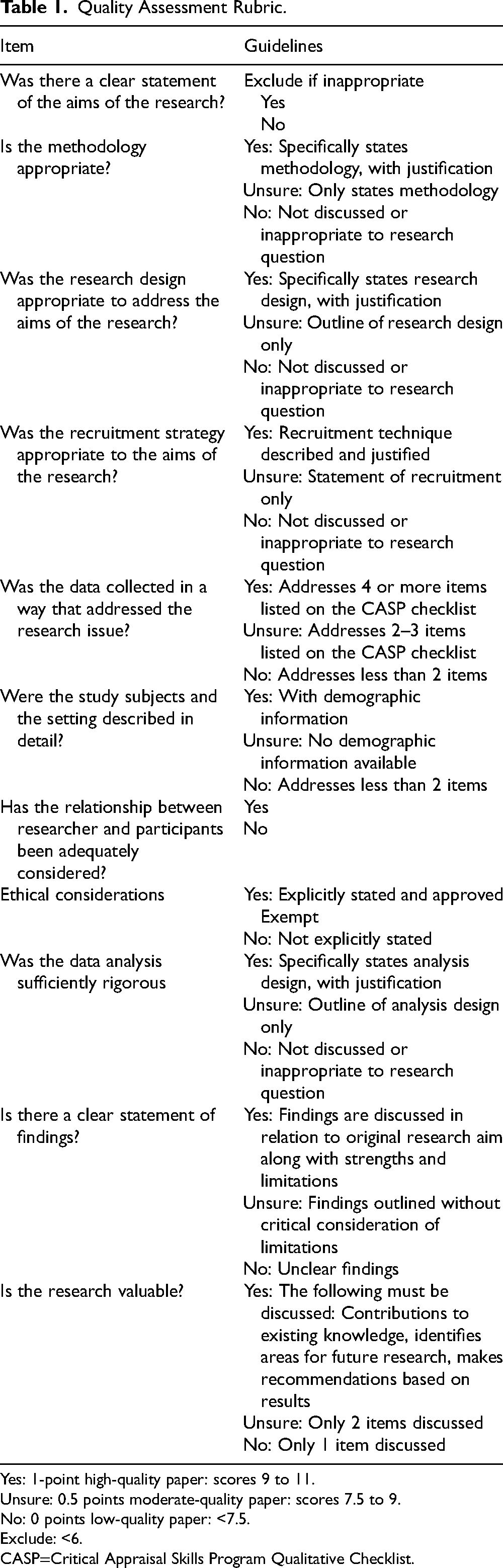
Yes: 1-point high-quality paper: scores 9 to 11.
Unsure: 0.5 points moderate-quality paper: scores 7.5 to 9.
No: 0 points low-quality paper: <7.5.
Exclude: <6.
CASP=Critical Appraisal Skills Program Qualitative Checklist.
Data Analysis
The philosophical foundation underpinning data synthesis is pragmatism. Pragmatism is a process of clarifying meaning with respect to practical implications. This review seeks to answer questions about how existing evidence can be leveraged to improve nursing practice so that improvements in population health and health equity can be achieved. A pragmatic approach uses existing frameworks rather than challenging the status quo which is found in critical qualitative approaches (Doane & Varcoe, 2005; Ramanadhan et al., 2021). The authors are clinicians and researchers, with experience in adolescent health, vaccine behavior, and reproductive health.
After screening, data extraction and thematic synthesis into higher level abstraction guided by the SEM was completed by the main author. Data extraction and synthesis were done via a qualitative review process performed using MaxQDA software. Selected articles were imported into MaxQDA so that the data could be managed and systematically analyzed (Amanfi, 2019). The first stage was deductive, line-by-line coding text using the SEM framework. For example, codes related to knowledge, attitude, and beliefs were coded as intrapersonal. In the second stage descriptive themes were developed by grouping codes with similarities. For example, codes were grouped if nursing practice was impeded or supported. Coding the data by the effect on nursing practice was instrumental to understanding the experience of the school nurse. In the third stage, relationships between the codes were synthesized into analytical themes within the levels of the SEM.
Results
Study Characteristics
Thirteen studies only considered vaccine promotion for female sex adolescents, with the remainder (n=15) being gender neutral (see Table 2). There were qualitative studies (n = 15), quantitative studies (n = 11), and mixed-methods studies (n = 2). Studies were from the eight different countries including the United States (n = 9), the United Kingdom (n = 9), Sweden (n = 4), Australia (n = 2), Finland (n = 1), Canada (n = 1), China (n = 1), and Peru (n = 1). Most studies did not explicitly state an underlying theory (n = 16). The SEM (n = 4), Diffusion of Innovation (n = 2), and Theory of Planned Behavior/Reasoned Action (n = 2) were used in more than one study. Grounded theory, naturalistic inquiry, competing demands, and framing theory were each used once by a study. Most studies were not exclusive to school nurses (n = 16) and included stakeholders such as teachers, administrators, parents/guardians, and adolescents. Twelve studies exclusively examined school nurses. Thirteen studies only considered vaccine promotion for female sex adolescents, with the remainder (n = 15) being gender neutral. The majority of studies exclusive to females were prior to 2015 (n = 7).
Summary of Studies.
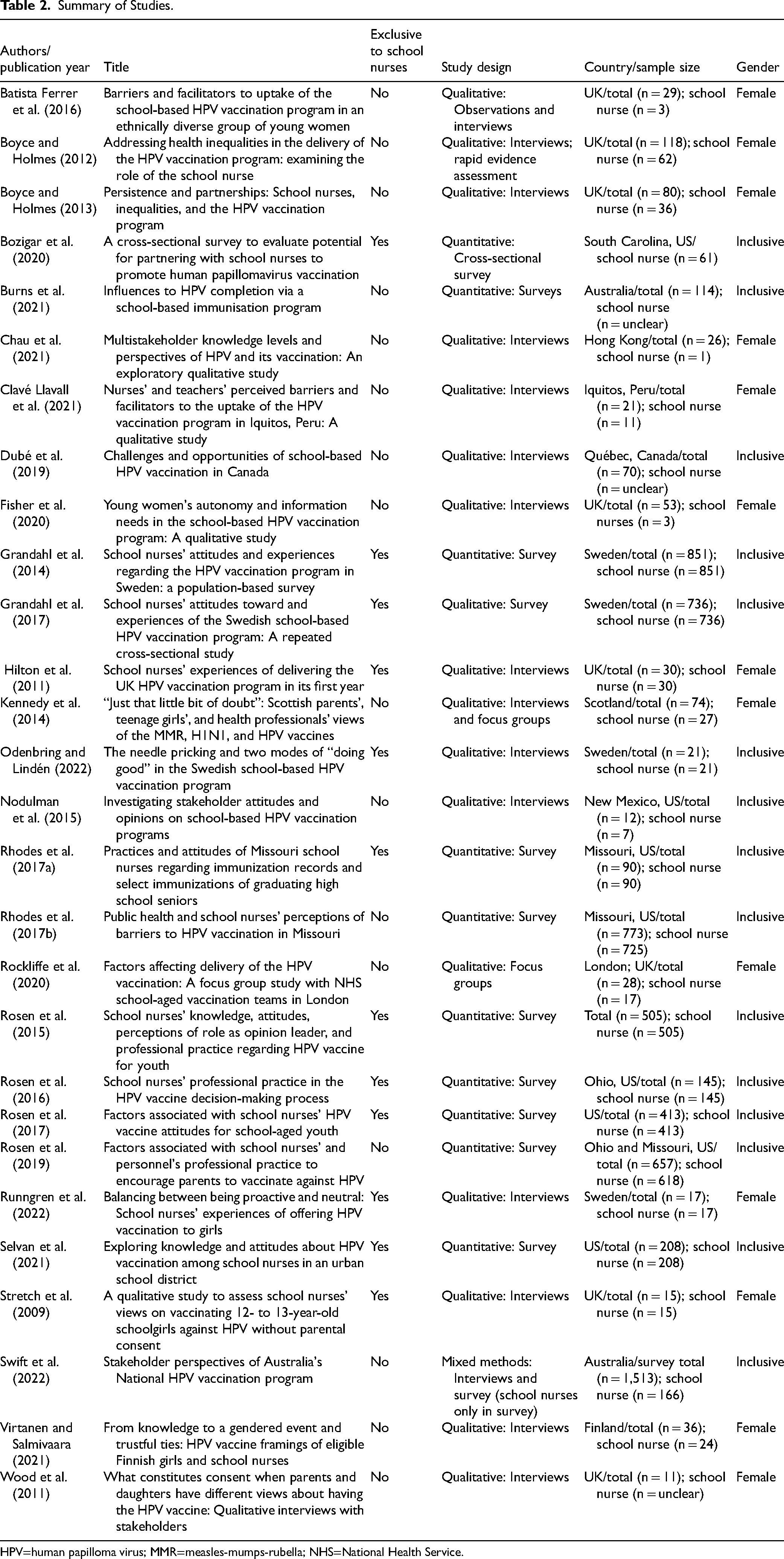
HPV=human papilloma virus; MMR=measles-mumps-rubella; NHS=National Health Service.
SEM Intrapersonal Level Themes
The intrapersonal level includes factors that impact nursing practice like attitudes, knowledge, beliefs, perceptions, and experience (McLeroy et al., 1988). Three themes were identified at the intrapersonal level.
General knowledge versus sufficient knowledge
Knowledge was measured as the range of the nurse's understanding of HPV infection and vaccination
Cautious optimism
School nurses overwhelmingly believe the HPV vaccine is safe, effective, and have confidence in vaccine authorities (Grandahl et al., 2017; Rosen et al., 2016; Runngren et al., 2022). The continuum of studies shows positive attitudes and early acceptance of inclusive vaccine strategies (Bozigar et al., 2020; Rosen et al., 2016; Stretch et al., 2009; Swift et al., 2022; Wood et al., 2011). Most nurses believe preteens should be vaccinated and support the inclusion of HPV vaccination in routine childhood immunization schedules (Grandahl et al., 2017; Rhodes et al., 2017b; Rosen et al., 2016; Selvan et al., 2021; Virtanen & Salmivaara, 2021). However, some nurses feel preteens are too young to be vaccinated, and vaccination efforts should target older adolescents (Grandahl et al., 2014; Selvan et al., 2021). Similarly, nurses feel that younger adolescents are less capable of self-consent when compared to older teenagers (Batista Ferrer et al., 2016). The belief that vaccine should only be given to older adolescents contradicts current HPV vaccine initiatives. Nurses are most concerned with vaccine side-effects (Kennedy et al., 2014; Stretch et al., 2009). In a study conducted by Kennedy et al. (2014) a nurse reported that they recommended a delay for a routine childhood vaccination due to the belief that vaccines may cause harm. The same nurse indicated that there was no scientific reason for the delay, and the recommendation was made due to the nurse's belief that the vaccine may be damaging when given too early. Most nurses believe HPV-related education is appropriated for adolescents, but acknowledge HPV transmission is a delicate subject and believe the best way to approach education is to focus on cancer prevention (Kennedy et al., 2014; Nodulman et al., 2015; Rosen et al., 2019). Of concern, Rosen et al. (2015) report that despite most nurses having positive attitudes, their intention to provide HPV vaccine information to parents/guardians remained low.
HPV vaccine influencer
Even with a moderate amount of knowledge and positive attitudes toward the HPV vaccine, many nurses report low confidence for addressing caregivers and students (Bozigar et al., 2020; Kennedy et al., 2014; Rhodes et al., 2017a; Rosen et al., 2017; Selvan et al., 2021). School nurses do see vaccine promotion as a part of their professional responsibility (Nodulman et al., 2015; Selvan et al., 2021), and feel confident they can access resources when needed (Rosen et al., 2016). Student age was relevant to vaccine promotion confidence, and nurses serving older adolescents (9th–12th) are more likely to recommend the vaccine to parents/guardians than nurses serving younger students (Rosen et al., 2019). Nurses understand the benefits of connecting with those who initially declined the vaccination and to offer the vaccination multiple times (Grandahl et al., 2017). However, school nurses feel they should not pressure parents/guardians (Runngren et al., 2022), and understand the limitations of their professional recommendation accepting that some will refuse HPV vaccines even when sufficient education is provided (Runngren et al., 2022; Stretch et al., 2009; Wood et al., 2011). Likewise, nurses do not see themselves as responsible for tracking why the HPV vaccine was refused (Selvan et al., 2021).
SEM Interpersonal Level Themes
The interpersonal level includes close social circles (friends, partners, family members, and coworkers). Close interpersonal relationships can influence behavior and contribute to life experiences by conveying social norms and establishing forms of social control (McLeroy et al., 1988). School nurses have complex interpersonal relationships, and are often the liaison between school officials, medical professionals, caregivers, students, and the larger community (Rosen et al., 2016). Although nursing practice may be influenced by personal relationships, professional relationships were the focus of the existing literature. Four interpersonal themes were identified.
HPV educator
Most school nurses provide education and answer questions about HPV vaccinations (Bozigar et al., 2020; Burns et al., 2021). Nurses who provide education to children in schools found centering education on cancer prevention is best and in-depth knowledge was unnecessary (Virtanen & Salmivaara, 2021). Nurses prefer inclusive education, but most nurses report education is provided to boys and girls separately (Grandahl et al., 2014; Rosen et al., 2019)
Relationships over enforcement
The HPV vaccine is seen as important but is one of many duties school nurses are responsible for. Nurses stated that their duties require ongoing relationships with families. Nurses therefore balance issues around the vaccination to protect longstanding, trust-based relationships (Hilton et al., 2011; Virtanen & Salmivaara, 2021). Nurses prefer not to probe if the HPV vaccine is refused and maintain a neutral position (Boyce & Holmes, 2013). When nurses did report a reason for refusal, safety concerns were noted more than religious or philosophical objections (Swift et al., 2022). The nurse's efforts to maintain good relationships extend to school-based immunization clinics. Although nurses provide multiple opportunities to vaccinate children of apathetic caregivers, nurses tend not to vaccinate children without explicit consent from a guardian. This is true even in areas where adolescents are legally allowed to self-consent for vaccination (Bozigar et al., 2020; Grandahl et al., 2014; Stretch et al., 2009). In cases where the child is due for a vaccine, but explicit consent is absent, school nurses hold the vaccine and refer students to primary care providers or a health department (Nodulman et al., 2015). This practice allows the nurse to sustain trust. Despite the possibility for problematic conversations, most communication related to the HPV vaccine is reported as positive (Hilton et al., 2011). When vaccine hesitancy does arise, nurses need medically accurate resources and good communication skills. Rosen et al. (2019) suggest a script with vaccine-specific prompts to support nurses in starting positive conversations with caregivers.
Needle phobia
Adolescent needle phobia is noted in several studies (Grandahl et al., 2014; Virtanen & Salmivaara, 2021; Wood et al., 2011). In schools where vaccines are administered, the nurses spend more time with fearful students. Nurses need extra time with needle phobic students, and see the care as central to good nursing practice (Odenbring & Lindén, 2022; Virtanen & Salmivaara, 2021). Odenbring and Linden note a nurse's experience with needle phobia, “I’ve had a lot of students who’re really scared, and it works eventually when you tell them that they’re the ones in control. We won’t do anything until you’re ready, and that normally works.” The quote highlights the importance of the school nurse's role as a caregiver during vaccine administration. Vaccine administration workflows should incorporate extra time for needle phobic students.
Counting on coworkers
A unique aspect of many school nursing positions is the absence of clinical peers (Virtanen & Salmivaara, 2021). When school nurses need a second nurse for safety, nurses from neighboring schools are called for help (Grandahl et al., 2017; Runngren et al., 2022). With limited access to clinical peers, relationships with key nonclinical staff members become very important. Nurses report that administrators, teachers, and secretarial staff play a significant role in HPV vaccine activities. Nonclinical staff help with administrative responsibilities such as follow up for vaccine records and consent forms (Clavé Llavall et al., 2021; Rockliffe et al., 2020). Clavé Llavall et al. (2021) captures a nurse's working relationship with teachers in rural Peru
SEM Organizational Level Themes
The places nurses work influence nursing practice. The organizational level includes structures, practices, policies, and norms within an organization. In this review, the organization refers to the school or schools where the nurse works. Factors can be formal or informal rules and regulations for operations including the school climate, schedules, and financial policies. Two themes were identified at the organizational level.
Consistently inconsistent
School-based vaccination activities are implemented differently between school districts and even vary between different schools in the same districts (Dubé et al., 2019). Similarly, there are differences in nurse staffing and HPV vaccine education requirements between public, private, and religious schools (Clavé Llavall et al., 2021). In some schools, HPV curriculum is included in reproductive health education taught to fifth and sixth graders. However, HPV curriculum must typically be approved prior to instruction (Bozigar et al., 2020; Rosen et al., 2017). Some school districts allow nurses to use class time to educate children about HPV and the vaccine, and some do not (Burns et al., 2021; Runngren et al., 2022; Virtanen & Salmivaara, 2021). In schools where classroom time is set aside, there are inconsistencies in the period of instruction and the type of information covered (Runngren et al., 2022). For example, some nurses only distributed educational pamphlets while others taught full classes on HPV and the importance of vaccination (Dubé et al., 2019). The school nurses prefer standardized education and allotted classroom time (Nodulman et al., 2015). Districts may benefit from sharing effective protocols and procedures from neighboring schools.
School resources
Schools that have access to resources and prioritize resources for vaccine compliance activities inevitably support school nursing practice (Batista Ferrer et al., 2016; Bozigar et al., 2020; Fisher et al., 2020; Runngren et al., 2022). Personnel resources include school-appointed vaccine champions who facilitate communication between schools, key stakeholders, and community partners. Schools can support vaccine champions with procedures and communication tools to standardize vaccine follow up. Schools with good follow-up practices have higher HPV vaccine rates when compared to schools without standardized follow up (Boyce & Holmes, 2013). Frequent school personnel turnover and funding shortages negatively impact the schools’ ability to invest resources into HPV vaccine activities (Grandahl et al., 2014; Hilton et al., 2011; Nodulman et al., 2015). Similarly, turnover makes building relationships, training, and institutional memory problematic (Dubé et al., 2019; Runngren et al., 2022). Electronic health records and integrated systems improve follow up and compliance efforts while simultaneously reducing the nursing workload (Clavé Llavall et al., 2021; Rhodes et al., 2017a). Technology also eases access to accurate, up-to-date online resources (Rosen et al., 2017). In schools with limited internet, the availability of written information helps nurses provide vaccine information to families (Clavé Llavall et al., 2021; Rhodes et al., 2017a, 2017b; Rosen et al., 2016; Selvan et al., 2021). In schools with the ability to administer vaccines on-site, one of the factors that increases student vaccination rates is the frequency of school-sponsored vaccine clinics. However, vaccine clinics are resource intensive and increase the nursing workload (Boyce & Holmes, 2012, 2013; Hilton et al., 2011). When nurses do not have support from the school, vaccination rates suffer. This is evidenced by the following quote found in Rockliffe et al. (2020), “What I’m finding is not all of the areas are, school-wise, supporting us. […] umm, I find that without the support of the schools, that makes it a hard job.” The ability of schools to supply resources during times of high vaccine activity is imperative for success. This is because the nurses continue to provide for the students’ other health needs. Vaccination activities pull the nurses away from services they provide to vulnerable and medically fragile students (Boyce & Holmes, 2012; Grandahl et al., 2017; Hilton et al., 2011). With adequate resources nurses are able to integrate vaccine activities with other school health practices (Odenbring & Lindén, 2022).
SEM Community Level Themes
The community level includes influences from within a larger, but still local, area that affects individuals, groups, and organizations. Factors may include relationships among organizations (schools, health departments, clinics), location of the school within the community, and influences from community leaders. Two themes were identified at the community level.
Community partners
Community partners like primary care providers, clinics, and pharmacies support school nursing practice related to HPV vaccination efforts (Bozigar et al., 2020). Partnerships with primary care providers offer an additional resource to address hesitancy (Runngren et al., 2022). Community partners also help access missing vaccination records of transient student populations (Nodulman et al., 2015). Nurses found maintaining relationships with community partners challenging at times. In the Clavé Llavall et al. (2021) study, nurses felt their opinion was not valued and that the partners were not aware of the needs of the children in the community: “One thing is to rule from a desk and the other thing is to come and get to know the reality (. . .) see reality so you can make all the decisions.”
Community priorities
Communities prioritize some health issues over others and direct resources accordingly (Hilton et al., 2011). The literature included in this review presents juxtaposed findings related to community economic status. On one side a school nurse in Swift et al. reports “We find that we often get lower uptake in schools in areas of socioeconomic disadvantage—less consent forms returned for the first dose as well as increased absenteeism.” The connection between lower vaccine rates and groups experiencing food insecurity and housing instability was also noted in another study (Hilton et al., 2011). Urgent needs, such as safety chronic illness, and absenteeism draw resources from vaccination activities. On the other side, Hilton et al. (2011) note community affluence impacts school nurses’ practice “… I think people from slightly poorer backgrounds expect you to do more hands-on things and be able to fix everything … people from slightly poorer back-grounds are often more likely to actually follow the advice you give, if you have that trust you can engage with them and they are more likely to listen and work with you rather than argue with you, whereas the more affluent parents sometimes think they know best.” School nurses work to improve vaccine access in communities with structural barriers but find little benefit in committing time and resources to communities that actively reject available vaccines (Hilton et al., 2011; Stretch et al., 2009). Nurses prioritize the most pressing community needs, and nurses serving larger schools in deprived areas are more likely to need supportive resources (Rockliffe et al., 2020; Swift et al., 2022).
SEM Societal/Policy Level Themes
The societal/policy level includes national and state laws and policies that allocate resources and influence health behavior. In the context of this study nursing practice scope, vaccine mandates, and healthcare policy were considered at the macrolevel (McLeroy et al., 1988). Two themes at the societal level were identified.
HPV vaccine laws
Compulsory vaccination and policies where vaccination is the default option are supported by some nurses (Clavé Llavall et al., 2021). However, as is seen with most political matters, nurses hold contradictory views and some assert that mandates cause unnecessary discourse. The studies suggests a better approach is to focus unofficially (without a mandate) on adolescent vaccine efforts (Nodulman et al., 2015). Rosen et al. (2019) note unsuccessful attempts to mandate HPV vaccines in Ohio and Missouri, highlighting the difficulty of passing legislation in the Unites States. Adolescent consent laws vary between jurisdictions (Dubé et al., 2019). School nurses’ application of consent law is affected by interpretation and how the vaccine is framed. For example, if the HPV vaccine is framed as a reproductive health intervention, adolescent self-consent is implemented similarly to other interventions such as birth control. However, if the vaccine is framed as a cancer-prevention intervention, self-consent is not as clear (Stretch et al., 2009; Virtanen & Salmivaara, 2021; Wood et al., 2011). State vaccine policies change, and school nurses need time to respond. When existing laws change, or new laws are passed, adequate notice allows nurses to implement the changes more effectively. Adequate preparation allows nurses to develop trust when new vaccines are required. Some policy changes are positive like reducing the 3-dose HPV series to the two-dose HPV series when vaccines are initiated before the age of 15, which improves compliance and simultaneously reduces the nurse's workload (Swift et al., 2022).
HPV campaigns: Who gets the vaccine and when
Initially the HPV vaccine was marketed to prevent cervical cancer in females (Grandahl et al., 2014; Hilton et al., 2011). Early vaccine campaigns were knowledge based and framed to protect against the sexual transmission of HPV infection (Hilton et al., 2011; Virtanen & Salmivaara, 2021). In some countries, female-only vaccine campaigns persist. The two studies from middle-income countries in this review focus on female-only vaccination. The exclusion of males is attributed to limited resources. Thus, nurses in under-resourced areas may be expected to exclude males from vaccine efforts despite the nurses’ willingness to implement gender inclusive promotion (Chau et al., 2021; Clavé Llavall et al., 2021). Female-only campaigns make it difficult for nurses to use a simplified message that centers around gender neutral cancer prevention. Nurses may not have the autonomy to vaccinate beyond the scope of the national vaccine guidance, but they can support a neutral position on HPV vaccine as cancer prevention.
Discussion
This systematic review highlights the complexity of HPV vaccine promotion in schools over time and the experiences and challenges that school nurses encounter. The findings provide insight on the multilevel factors that can impede or facilitate school nursing practice related to vaccine compliance. The formation of analytical themes from the synthesis of individual study findings gives insight on the knowledge, attitude, experience, and role of school nurses related to HPV vaccination and promotion in school settings. Similarly, the inclusion of a broad range of perspectives allows for the appreciation of the role gender plays in HPV vaccination and promotion in school settings. This study broadens the understanding of the socioecological factors that impact school nursing practice.
Limitations
Systematic reviews carry the risk of bias in the form of selection bias and publication bias. An exhaustive search strategy should minimize the risk of selection bias, but the exclusion of gray literature may increase the risk of publication bias. The choice to limit the systematic review to full-text, peer-reviewed studies was made to ensure that the included studies met the rigorous appraisal by experts in the field. However, valuable information may be lost from the exclusion of other types of literature, and thus is a limitation of this review. In addition, this systematic review is subject to language bias because studies published in a language other than English were excluded (Butler et al., 2016; Owens, 2021). To address tacit assumptions that could lead to bias, the research questions and procedures were predetermined. The studies in this review are predominantly from high-income countries and data were collected in different contexts. The published studies may lack critical contextual information because of bias or space limitations. The analysis was conducted by one author, which is a limitation. However, researcher reflexivity through journaling was implemented to reduce investigator bias. Additionally, the main author's subjectivity statement acknowledges their role as a practicing school nurse. Despite potential limitations, this review provides valuable knowledge to support school nursing practices as they relate to HPV vaccination.
Implications for Practice
The synthesis of school nurses’ experiences is useful for clinicians, researchers, and policy makers. Findings highlight key considerations for practices that support school-based HPV vaccine promotion. The themes were conceptualized into the lead, engage, adopt, develop, support (LEADS) model which highlights key facilitators to nursing practice (Table 3).
LEADS Model.
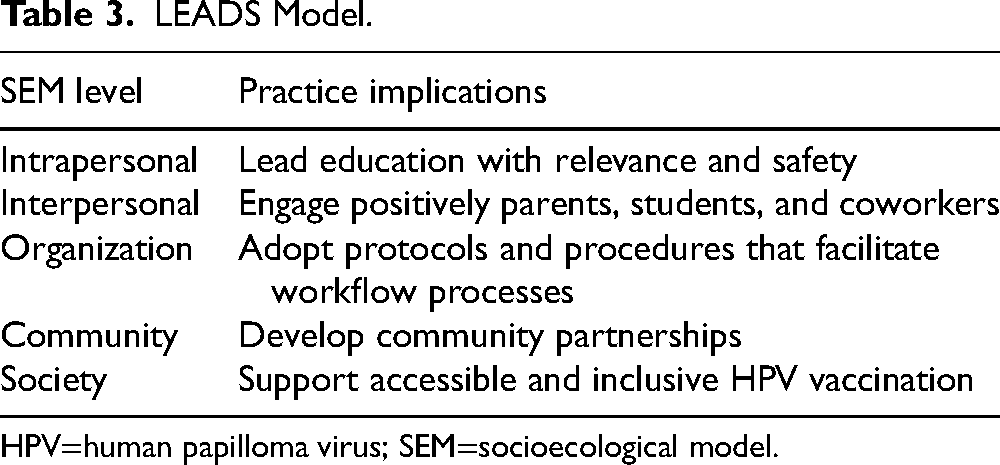
HPV=human papilloma virus; SEM=socioecological model.
At the intrapersonal level this review highlights the need for specific training on vaccine safety and efficacy (Rhodes et al., 2017b; Rosen et al., 2016). The lack of legal knowledge may inhibit the efficiency of school-based vaccine clinics. Therefore, nurses need clear guidance on both the local adolescent consent laws and the school's policy for administering the HPV vaccine without explicit caregiver consent (Batista Ferrer et al., 2016; Wood et al., 2011). Tailored education can not only address knowledge gaps but can also strengthen the belief that preteens are the best target population to be vaccinated (Kennedy et al., 2014; Selvan et al., 2021; World Health Organization, 2014). Therefore, nurse trainings should lead with vaccine relevance and safety.
To move beyond the intrapersonal level nurses must be able to confidently engage families. The NASN suggests that communication training such as motivational interviewing skills can empower nurses to engage with parents/guardians that have refused the vaccine (Bozigar et al., 2020; Rosen et al., 2015). The “Motivational Interviewing Tool to Improve Vaccine Acceptance” was associated with a statistically significant increase in early childhood vaccination (Cole et al., 2022). A similar tool may be helpful for nurses that support adolescent vaccine activities.
Needle phobia is present in up to 50% of adolescents, and more attention should be directed toward nursing interventions that alleviate fear (McLenon & Rogers, 2019). Roussel (2018) emphasized the importance of compassionate nursing care in overcoming needle phobia. To achieve the best practice, school nurses need support from nonclinical coworkers (Dubé et al., 2019; Runngren et al., 2022). Nonclinical colleagues can assist with administrative and logistical tasks, which allows nurses to focus on the students. Guided nurse communication can facilitate positive engagement with families and coworkers.
Nursing practice related to HPV vaccine can be facilitated when schools (organizations) provide resources and support particularly during busy vaccination times. Unfortunately, variations in vaccine and adolescent consent policies between jurisdictions makes borrowing or replication work processes challenging (Swift et al., 2022). School nursing practice can be further complicated by the fact that many nurses take on various healthcare roles in the school and may be the sole healthcare provider for multiple schools. Although schools and school nursing roles vary, it is important that schools adopt and adapt strategies that improve nursing workflows to support vaccine compliance activities.
Working with community partners and understanding the communities’ priorities can help school nurses manage resources more efficiently. Due to the limited number of clinical staff employed by the school, school-based vaccination efforts may need to be supported and attended by staff from health departments and primary care clinics (Willis et al., 2016). Even with community partners, HPV vaccine efforts may be challenged when the locality has competing priorities (Willis et al., 2022). Still, developing community partnerships and collaborations are pillars of the NASN Framework for 21st Century Nursing Practice and can improve school nurses’ HPV vaccine promotion.
Societal level laws and policies govern nursing practice. It is important that school nurses remain current on vaccine and self-consent laws and policies. Policy changes can facilitate or impede school nursing practice, and nurses must be given adequate time to respond to changes. To reduce vaccine disparities, school nurses should continue to support policies and laws that promote accessible and inclusive HPV vaccination.
There have been great strides in nursing practice related to school-based gender-neutral HPV vaccination. This is particularly true for high-income countries like Australia and the United States (Burns et al., 2021; Rosen et al., 2019). In countries where vaccine resources are more limited, females remain the prioritized target population, but school nurses are ready and willing to support male vaccination (Chau et al., 2021; Clavé Llavall et al., 2021). There is widespread acceptance of inclusive HPV vaccination for adolescents among school nurses. It may be premature to declare the end of HPV vaccine feminization, but the renewed focus on the vaccine as a cancer prevention strategy has simplified school nursing vaccine efforts.
Conclusion
Reaching the goal to eliminate HPV-related cancers like those of the cervix and throat as a public health problem is possible (Hall et al., 2019). Educational interventions focused on HPV prevalence, vaccine safety, and vaccine efficacy may improve intrapersonal barriers to HPV vaccination (Berenson et al., 2021; Tucker et al., 2021). Despite nurses having favorable attitudes and beliefs, many nurses do not routinely communicate with families about HPV because of low confidence (Bozigar et al., 2020; Grandahl et al., 2017). This is a particularly concerning finding because research shows that healthcare workers’ recommendations influence decision making related to HPV vaccination for their children (Gilkey & McRee, 2016; Oh et al., 2021). School support is essential for the success of vaccine activities. School nursing practice related to HPV vaccination is influenced by multilevel factors. This review highlights a clear need for additional research that is explicitly focused on the school nurse because other stakeholders may have very different roles and perceptions. There is also a need to explore the experiences of school nurses in states where the HPV vaccine is mandated such as Virginia, Rhode Island, and Washington DC, because school nurses serving in those states likely have a larger role and different experiences than school nurses serving areas without mandates. Furthermore, ongoing research is needed to appreciate the impacts of COVID-19 on school-level vaccine compliance.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.