
Abstract
As states legalize medical cannabis, school nurses face increased parent questions about administration at school. Although school nurses frequently collaborate on the development and implementation of medication administration policies, their perceptions of barriers to school-based medical cannabis administration are not well-documented. To explore these perceptions, we surveyed school nurses (n = 379) in sixteen states about their beliefs related to school-based medical cannabis administration policy development. Findings revealed school nurses from states completely legalizing cannabis expressed significantly fewer concerns about the safety, stigma, and federal status of medical cannabis than their peers in more restrictive states. Implications for practice include (a) education of key stakeholders, (b) collaboration with stakeholders to formulate medication administration policy; and (c) development of state-level guidance for school professionals.
Background
As medical cannabis gains acceptance among health care professionals as an alternative therapy option (Huntsman, 2021; Mouhamed et al., 2018; Rosenberg et al., 2015), interest in cannabis and cannabinoids for pharmacotherapy continues to increase, along with the number of medical conditions for which qualified medical practitioners may recommend patient use of cannabis and cannabidiol (CBD) (Budney et al., 2019; Hill, 2019). Federally, cannabis use is prohibited by the Controlled Substances Act of 1970 (Controlled Substances Act of 1970, 1970). Healthcare and pharmacists can only recommend its medicinal use. A variety of legal and societal concerns influence state cannabis legalization efforts, creating a continuum spanning from maintaining completely illegal status to adopting completely legal status (both for recreational and medical purposes). Currently, thirty-seven states and the District of Columbia have approved medical cannabis for those with serious medical conditions (Ananth et al., 2018; Asmelash & Alonso, 2020; National Conference of State Legislatures, 2021). Additionally, pediatric patients who have intractable seizures and cancers may receive medical cannabis when traditional therapies and medicines have not been successful (Ananth et al., 2018; Ben-Zeev, 2020; National Institute on Drug Abuse, 2018; Rosenberg et al., 2015; Woo et al., 2020). Woo et al. (2020) cautions healthcare providers and practitioners not to generalize medical cannabis products, as the ambiguity of regimen dosing and lack of research in the pediatric population creates a challenge to suggesting evidence-based recommendations for children.
As more states and health care professionals consider medical cannabis as a viable therapeutic option, parents increasingly seek to have school nurses administer medical cannabis to pediatric patients during the school day (DeWitt-Parker, 2016; Elliott, 2019; Patrick & Reiner, 2017). Due to the variability in state law and a general lack of specific guidance for schools, several factors may hinder the development of effective K-12 school medical cannabis administration policies (Bridgeman & Abazia, 2017; Patrick & Reiner, 2017; Robinson, 2020; Ruheel et al., 2021). Because school nurses are key stakeholders in the development and implementation of school medication policies, their perceptions of medical cannabis administration are an important lens through which to view the trend toward legalization of medical cannabis at the state level as compared to legal and societal factors affecting the viability of medical cannabis administration in the school setting.
Given the shifting medical, societal, and legal opinions related to the use of medical cannabis, Lewin's (1948) Theory of Planned Change provides a theoretical framework for examining the policy nuances that school nurse leaders must address when leading and managing tangible change (Shirey, 2013). This framework identifies three stages in the change process: (a) Unfreezing or letting go of an old pattern that was counterproductive in some way; (b) Moving/Transition, a change in thoughts, feelings, or behavior; and (c) Refreezing, where the change becomes a standard operation and assists in guiding organizational change (Shirey, 2013). To identify the forces behind these changes, Lewin's Force Field Analysis (FFA) categorizes factors for and against change as influential and driving forces (Shirey, 2013). Figure 1 depicts a force field analysis of school policy related to medical cannabis administration.
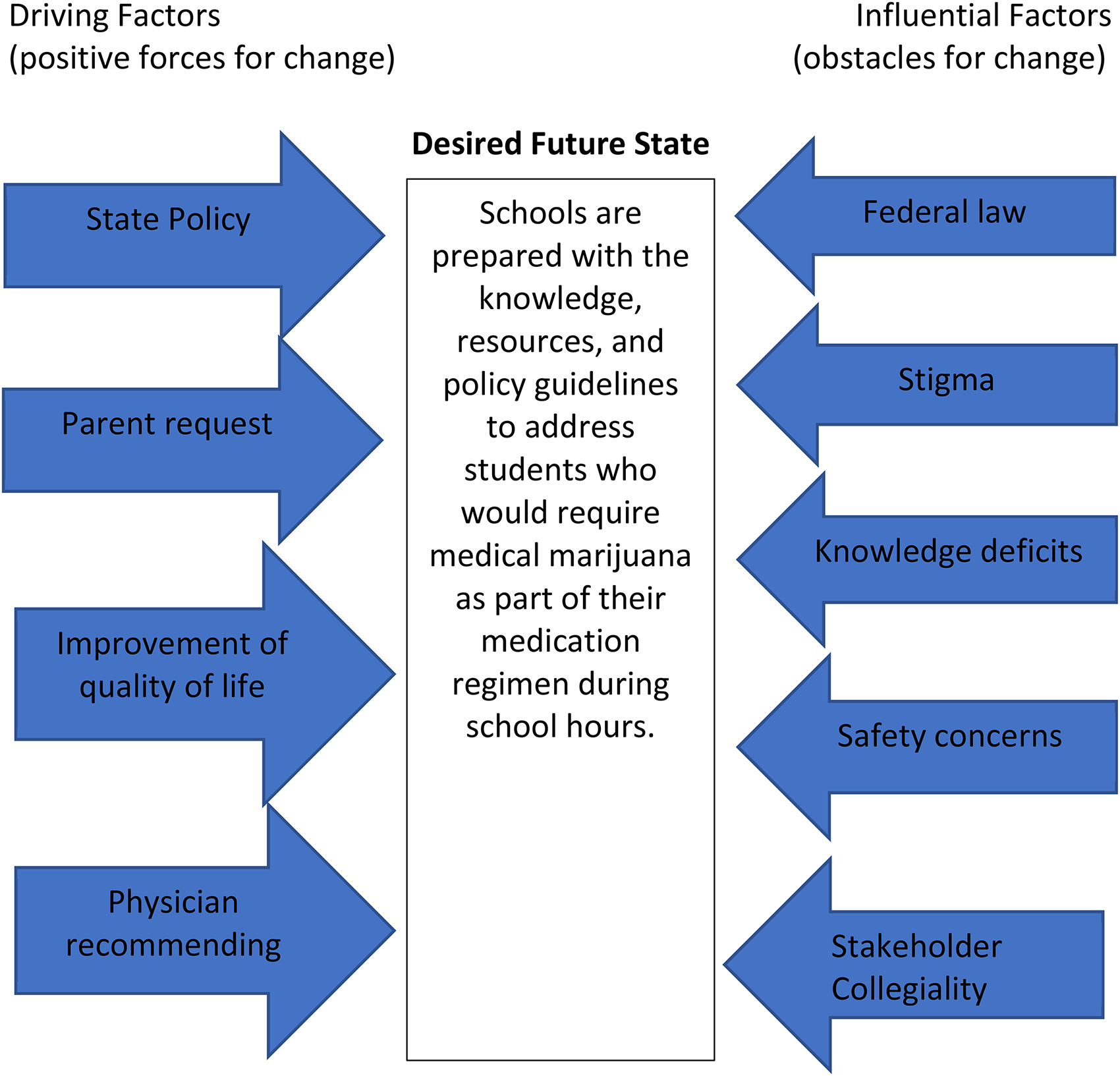
Force Field Analysis (Shirey, 2013) applied to medical cannabis policy in K-12 schools.
Introduction
With the expanded use of medical cannabis among pediatric patients (Patrick & Reiner, 2017; Ruheel et al., 2021), school nurses increasingly must address parent requests for school-based medical cannabis administration (DeWitt-Parker, 2016). In general, nurses who care for patients using medical cannabis must consider their code of ethics and practice standards in providing respectful, non-judgmental, and evidence-informed care (Balneaves & Alraja, 2019). As trusted health care professionals in their communities, school nurses should apply this reasoning when responding to requests for school-based medical cannabis administration that may conflict with community norms (Owen-Rankin, 2015). However, the lack of consensus on the efficacy (Ananth et al., 2018; Hakalovic, 2016), the lack of dosing parameters (Woo et al., 2020) and the ambiguous legal status (FindLaw, 2021; Findley et al., 2021 National Conference of State Legislatures, 2021;) of medical cannabis complicate these decisions. particularly for nurses in states that permit medical cannabis administration to school-age children.
Policy Development and Implementation Factors
A search of the literature yielded five policy development and implementation factors (federal law, stigma, knowledge deficits, safety concerns, and stakeholder collegiality) that may influence decision-making related to school-based medical cannabis administration policies.
Federal Law
In thirty-seven states, school nurses must navigate a policy conflict between federal law that still criminalizes cannabis and its products and the states’ decriminalization of medical cannabis relying on federal guidance permitting each state to develop cannabis regulations independently (Title II of the Comprehensive Drug Abuse Prevention and Control Act, 21 U.S.C. §§ 801–971; Branson, 2019). Former president, Barack Obama sent a memo in 2009 to federal prosecutors not to litigate those who distribute marijuana for medical reasons as long as in accordance with state law (Denisco, 2016). In 2013, the U.S. Department of Justice announced that states with medical marijuana policies must adhere to strong state-based enforcement, as state laws can be challenged at any time (Harris & Martin, 2021). Several U.S. House of Representatives members have introduced bills to decriminalize marijuana (Harris & Martin, 2021; Stracqualursi & Dezenski, 2020). However, cannabis remains a Schedule I substance, which limits research on its use as a therapeutic drug. In fact, the only FDA-approved, cannabis-derived medication that nurses can administer is Epidiolex, which creates another contradiction between cannabis’ federal status as a controlled substance and its use as an approved medication (The National Council of State Boards of Nursing, 2018; Rosenberg et al., 2015; U.S. Food and Drug Administration, 2020). This contradiction influences interpretation of the Nurse Practice Acts Nationwide in all states (National Council State Boards of Nursing, 2022), which prohibits nurses from administering Schedule 1 substances. Therefore, the enforcement of state medical cannabis laws and policies along with contradictory federal administrative guidance, results in an ambiguous and shifting legal landscape (Denisco, 2016; Findley et al., 2021; Patrick & Reiner, 2017 Ryan et al., 2021). As a result, school nurses may be uncertain whether they may administer medical cannabis to students without violating the Nurse Practice Acts (National Council State Boards of Nursing, 2022), even when state law permits its administration. Schools receiving federal funding is another hurdle districts will be faced with, should medicinal marijuana be permitted on school property. The Schedule 1 classification of cannabis causes hospitals and other settings that receive federal funding, either through Medicare reimbursement or other federal grants or programs, to pause to consider the potential loss of these funds should the federal government intercede and take action if patients are permitted to use this therapy on campus (Bridgeman & Abazia, 2017).
Knowledge Deficits
According to the National Council of State Boards of Nursing, nurses require practical information to care for the increasing number of patients utilizing medical cannabis. Unfortunately, cannabis is not typically a part of the curriculum in nursing schools, so nurses must seek information pertaining to cannabis administration on their own from reliable sources (Garcia, 2020; Zolotov et al., 2021). Rapp et al. (2015) reported that collaboration with colleagues in other states with similar levels of medical cannabis legalization can assist in bridging the knowledge gap. Further, nurses require access to supplemental educational and continuing education on medical cannabis that includes (a) the properties of cannabis and the endocannabinoid system; (b) dosing; (c) routes of administration; (d) safety considerations; (e) potential side effects and risk associated with use; and (f) creating effective treatment plans (Melnikov et al., 2019). Because these knowledge deficits also extend to school community members outside of the health care profession (Woo et al., 2020), school nurses must have the knowledge needed to effectively counsel the educators, parents, and community members that they serve.
Safety Concerns
As the building expert in medications and health conditions, parents, school staff, and administrators often refer questions about school-based medical cannabis administration to the school nurse (Patrick & Reiner, 2017). When considering these questions, nurses may express concern about a perceived lack of evidence-based literature and education surrounding medical cannabis therapy's safety and efficacy (Mouhamed et al., 2018) (Mouhamed, et al., 2018). However, the classification of cannabis as a Schedule I drug hinders medical cannabis research (Harris & Martin, 2021; Slawek et al., 2019), creating a barrier to gaining the evidence needed to evaluate safety and effectiveness (Compton et al., 2017; Hasin, 2017). Without clear guidance from governmental agencies, or appropriate professional literature to gain knowledge about medical cannabis, school nurses may have safety concerns. These safety concerns include (a) storage and administration of medical cannabis in the school setting; (b) potential side effects after administration; and (c) the logistics of when, how, and where to dispense the medication to students (King, 2019)(King, 2019). The lack of guidance specific to public school settings, school nurses may percieve safety risks outweigh the benefits to the individual student.
Stigma
Stigma surrounding the use of medical cannabis often introduces implicit bias from healthcare providers (Ryan et al., 2019), affecting the quality of a clinician-client relationship and care outcomes (Leos-Toro et al., 2018). Felnhofer et al. (2021) agree that medical providers’ attitudes toward medical cannabis impact their interactions with patients. Accordingly, the stigma associated with cannabis use—specifically, coupled with a perception that it is only a recreational drug with a high potential for abuse—may influence health care provider decision-making when patients request medical cannabis authorization (Balneaves & Alraja, 2019). Consequently, a lack of empirical knowledge of medical cannabis benefits and risks could heighten stigma among school nurses, reinforcing a hesitancy todevelop medical cannabis administration policy (Arnfinsen & Kisa, 2021; Balneaves & Alraja, 2019; Nugent et al., 2020; Rønne et al., 2021; Ryan & Hopko-Sharts, 2017; Zolotov et al., 2021) even when state law permits—but does not require—school-based administration.
Stakeholder Collegiality
School health policies affect not only students, but also the entire school community and staff (Branson, 2019; Robinson, 2020). One core role of the school nurse is to serve in a leadership position within the school to develop and evaluate school health policies. School administrators consider collaboration with the school nurse as an important component of health policy development and implementation (Maughan & Adams, 2011). School boards rely on this collegiality and collaboration to ensure that school district health policies both comply with legal requirements and address issues important to the school and community (Watson & Bogotch, 2016). If school nurses lack evidence-based knowledge of medical cannabis benefits, risks, and best practices, their guidance and advice to colleagues and community members may be biased.
Purpose of the Study
Although the professional literature propose development of school policies addressing parent requests for school-based medical cannabis administration (DeWitt-Parker, 2016; Nierengarten, 2018), differences in (a) key stakeholders’ social values, (b) legal requirements generated by multiple policy domains (federal/state), and (c) conflicting drug policy guidelines hinder the development and implementation of updated school medication administration guidance (Ananth et al., 2018; DISA, 2021; Lamonica et al., 2016; National Conference of State Legislatures, 2021). Additionally, the conflict between state and federal cannabis laws (Gilsbach, 2020),historical perceptions of cannabis as a dangerous drug (Lashley & Pollock, 2020) , and potential implications for their own practice (Patrick & Reiner, 2017) may deter school nurses from advocating for school-based medical cannabis administration, even when legal in their state. Consequently, school districts have devised a myriad of solutions for parents requesting school-based medical cannabis administration, including (a) on campus administration by a staff member other than the school nurse; (b) off campus administration by a parent; or (c) no administration during the school day (Americans for Safe Access, 2018; DISA, 2021; National Conference of State Legislatures, 2021). Therefore, school nurses face increased parent demands for school-based medical cannabis administration while confronting the concerns of education administrators about potential legal, public opinion, or safety repercussions (King, 2019; Patrick & Reiner, 2017; Slawek et al., 2019).
The purpose of this study was to explore school nurse perceptions of medical cannabis administration in the school setting and determine any relationship to the policy factors of Safety, Federal Status, Knowledge, Stigma, and Collegiality. Although Elliott (2019) provided a qualitative analysis of Southern California school nurse perceptions of knowledge deficits of medical cannabis administration, the extant literature lacks a comprehensive national investigation of school nurse perceptions.
As the lead health provider in schools, nurses’ perceptions are a critical component of effective school policy development and implementation. The specific research questions for this study were:
What is the frequency of school nurses reporting a medical cannabis policy for their district, both overall and disaggregated by state cannabis policy types (fully legal, medical only, illegal)? Do school nurse perceptions of each policy factor (safety concerns, knowledge deficits, stigma, federal status, collegiality with stakeholders) significantly differ by state cannabis policy type (fully legal, medical only, illegal)?
Method
To address the research questions, we employed a descriptive exploratory quantitative design (Fraenkel et al., 2019). This design provided a cross-sectional snapshot of the perceptions of school nurses related to policy factors that may influence school-based medical cannabis administration practices.
Research Sample, Setting, and Recruitment
The target population consisted of registered nurses who were specifically trained, educated, and currently employed as school nurses. To recruit participants, we gained permission to survey nurses affiliated with their state school nursing associations affiliated with the National Association of School Nurses in sixteen states. These states included three variants: (1) stateswith legalized recreational and medical marijuana, which will be referred to as “fully legal” states (2) states with legalized medical use of cannabis, which will be referred to as “medical only,” and (3) states where any cannabis, medical and recreational, is illegal, referred to as “illegal.” The National Association of School Nurses’ (NASN) would not collaborate to provide access to members for recruitment, , all state school nurse affiliates of the national association were invited to participate via an email. Table 1 identifies the state cannabis policy type and number of school nurses affiliated with the state school nurse organization for each of the sixteen states whose leadership agreed to provide access for recruitment for this study.
Participating States and Number of Association-Affiliated Nurses.
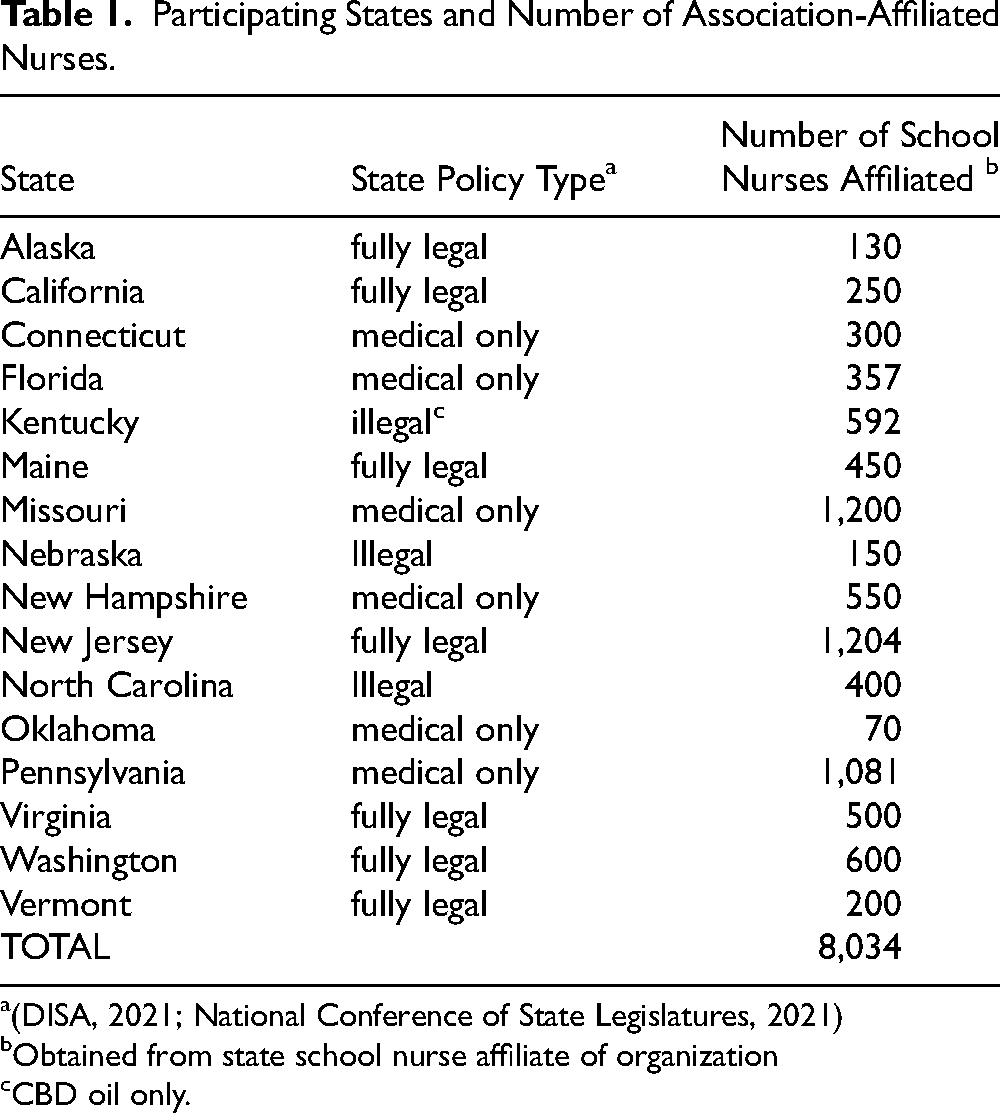
Obtained from state school nurse affiliate of organization
CBD oil only.
The sixteen states had a total of 8,034 members. Per Krejcie and Morgan (1970), the total population of 8,034 requires a sample size of 367 respondents as sufficient power for the study.
Instrumentation
We developed the questionnaire based upon a review of previous studies on medical cannabis perceptions of health care professionals (Elliott, 2019; Melnikov et al., 2019; Pereira et al., 2020). The first author conducted two pilots, one qualitative-style pilot on perceptions of school nurses, school administrators, and pharmacists who dispense medical cannabis and one quantitative pilot of school nurses in Pennsylvania. These pilots informed the major themes and influential factors of school nurses’ relationships with their administrators, knowledge deficits involving the topic of cannabis, and safety concerns—both with the storage and administration of medical cannabis, and the legal concerns of medical cannabis—which were incorporated into the questionnaire for this study. Additionally, the authors included selected themes from Elliott (2019) related to knowledge deficits on medical cannabis. The formatting of questionnaire items was modeled after those used by Pereira et al. (2020), asking the participants the degree to which they agreed with a statement. Each item was aligned with one of the five influential factors, resulting in a total of three items per factor. The items employed a four-point Likert-type scale ranging from strongly disagree (1) to strongly agree (4), omitting the middle neutral choice after analyzing the results of the quantitative pilot in July 2021 and considering whether social desirability might influence the use of a neutral response option (Chyung et al., 2017). Agreement indicated a favorable view of medical cannabis administration, and conversely disagreement indicated an unfavorable view.
We provided each state school nurse association director with a digital link to the Likert-type questionnaire through Survey Monkey and requested that they distribute the link to their members. A total of 8,034 surveys were distributed. Participants indicated consent through a checkbox on the welcome page of the survey; if a participant did not provide consent, the survey ended at that point. After sending out the questionnaire, reminders were sent out to all nonrespondents after 2 weeks. The survey remained open for a total of 1 month for responses.
Data Analysis
At the conclusion of the survey period, the authors exported the responses and uploaded the data into the Statistical Program for the Social Sciences (SPSS) for analysis. Data were aggregated by the 4-point Likert-type responses for the three items for each influential factor, and frequency distributions were calculated. For research question 2, an analysis of variance (ANOVA) was conducted using the state cannabis policy type as the independent variable. Significant influential force categories were analyzed using a Tukey post hoc test. For both the ANOVA and the Tukey post hoc test, p < .05.
Results
Overall, we received 413 responses to the questionnaire. Removing the questionnaires containing completely blank responses, a total of 379 responses were analyzed. Table 2 contains the response analysis of school nurse participation by state policy type.
Response Analysis of School Nurse Participation by State Policy Type.
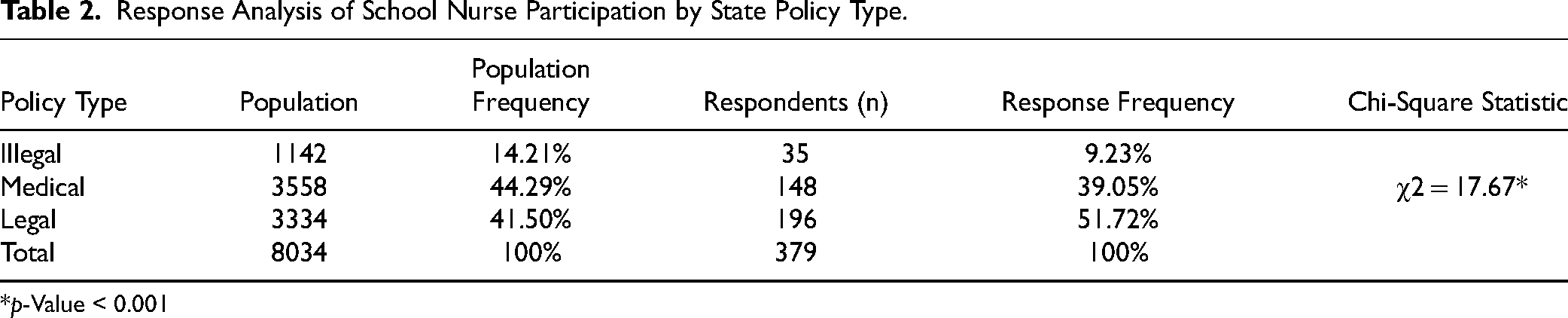
*p-Value < 0.001
Comparing the rate of response to the representation in the total population sampled, a non-response analysis (Fraenkel et al., 2019) found a disproportionally high response rate for nurses from fully legal states (51.72%), with a correspondingly lower response rate for school nurses from illegal (9.2%) and medical only (39%) states.
Research Question 1
Table 3 below displays the frequency of various staff member types permitted as per school district policy to administer medical cannabis overall to students, both overall and by state policy type.
Frequency of Individuals Permitted by District Policy to Administer Medical Cannabis.

Overall, approximately one fourth of school nurses reported that their school district had a policy permitting the administration of medical cannabis to students. When a policy existed, school nurses most frequently reported that the policy identified the parent as the individual authorized to administer the medical cannabis to the student. In contrast, school nurses reported having the authority to administer medical cannabis in only fifteen of eighty school districts with a policy permitting medical cannabis administration at school.
Research Question 2
A one-way ANOVA and Tukey post hoc test determined any significant differences in school nurse perceptions of each influential factor (safety concerns, knowledge deficits, stigma, federal status, collegiality with stakeholders) affecting cannabis policy development, disaggregated by state cannabis policy type (illegal, medical only, legal). The data for the ANOVA analysis are displayed in Table 4. Item responses ranged from 1- strongly disagree to 4-strongly agree. There were three items in each category and 4 points maximum per question, thus the possible scores within each influential factor category ranged from 3–12.
ANOVA Between Subjects Effects for Influential Factors by State Policy Type.
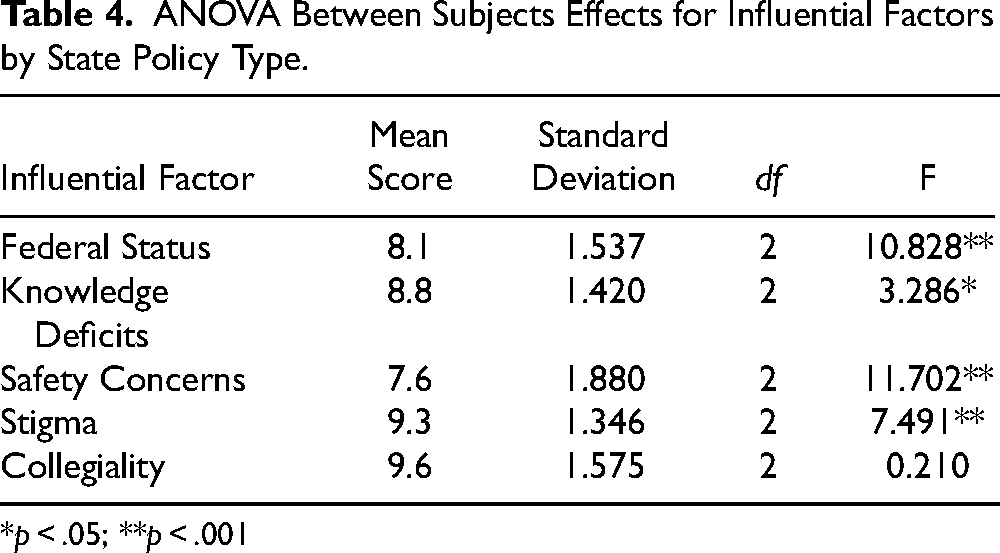
*p < .05; **p < .001
The ANOVA results indicate significant differences among the state policy types for all influential factors except collegiality. The influential factors of safety concerns, stigma, and federal status were significant at p < .001 between state policy types (illegal, medical only, fully legal. To determine the specific significant differences, Table 5 displays the Tukey post hoc pairwise comparisons for the four significant influential factors.
Tukey Post Hoc Pairwise Comparisons for State Policy Type.
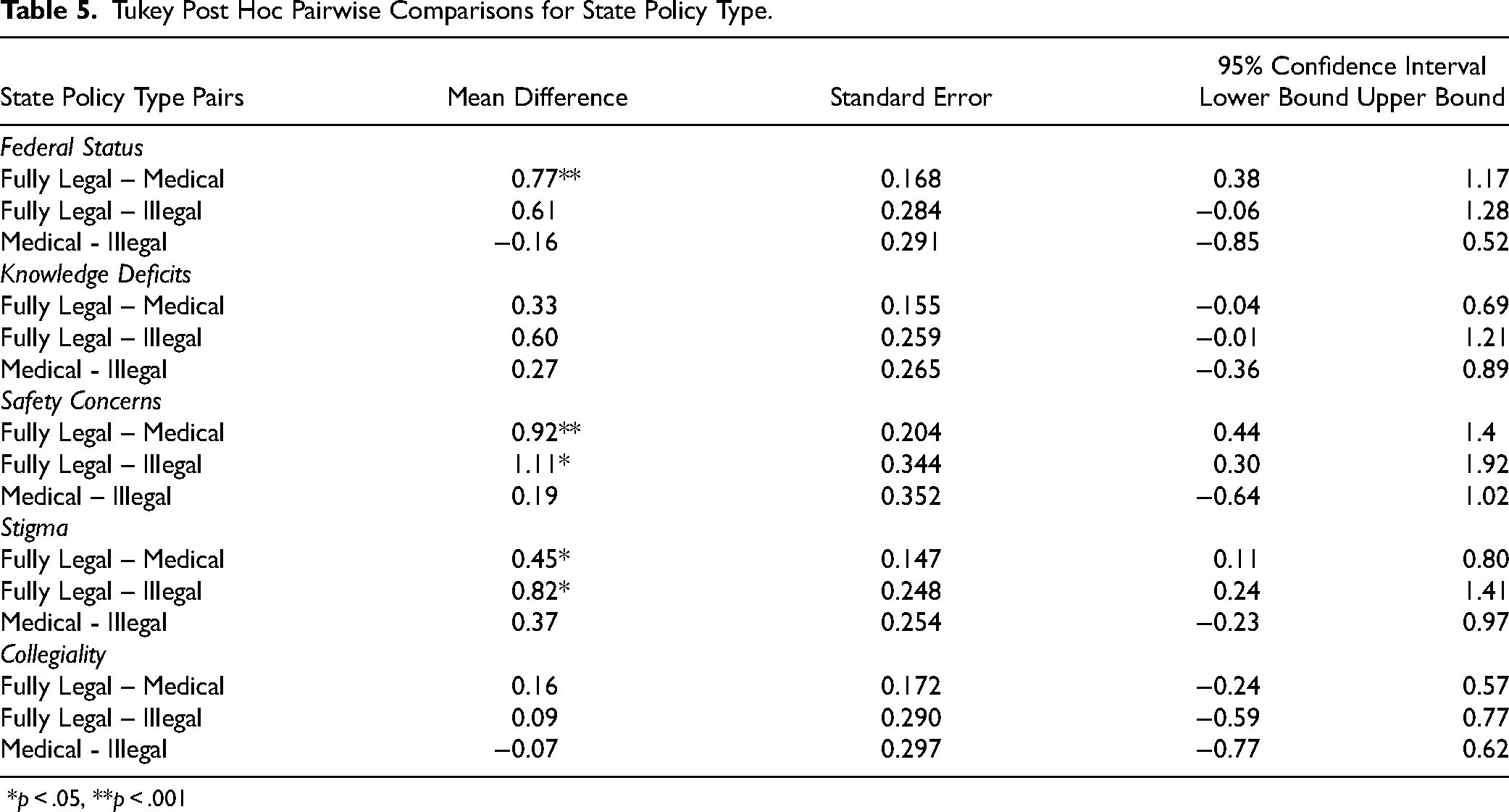
*p < .05, **p < .001
Analyzing the pairwise comparisons, the school nurse responses from fully legal states expressed significantly higher agreement than those for the medical only states for the influential factors of safety concerns, stigma, and federal status. Similarly, the responses from the fully legal states expressed significantly higher agreement than those from the illegal states for the influential factors of safety concerns and stigma. Although the knowledge deficits restraining force had a significant F-statistic, none of the pairwise comparisons had statistically significant mean differences.
Discussion
Research Question 1
As displayed in Table 3, approximately three-fourths of school nurses reported that their school district does not allow the administration of medical cannabis at school, even though virtually all nurse respondents work in states where medical cannabis is legal. The lack of school district policies permitting medical cannabis administration to students, even in states legalizing medical cannabis, may reflect a reluctance of school districts to address this issue unless they are required to do so. Reasons for this may include the ambiguity of state legalization and federal prohibition of marijuana use coupled with the potential consequences for both individuals and the school organization (Garcia, 2020; Patrick & Reiner, 2017). Few states publish guidance for schools addressing medical cannabis administration in the school setting. Of the thirty-seven states legalizing medical cannabis, only eleven states and the District of Columbia provide some type of guidance for schools (Americans for Safe Access, 2020). This lack of state guidance for policy development and implementation may deter districts from developing local policies because they are unsure as to the appropriate procedures and practices.
For the one fourth of school districts permitting school-based medical cannabis administration to students, the individual most frequently tasked with the administration is the parent. This finding aligns with the types of school district solutions that seek to straddle the contradictions between state and federal law (DeWitt-Parker, 2016; Melnikov et al., 2019; Nierengarten, 2018). Solutions such as these reflect a balancing of nurses’ concerns about compliance with the Nurse Practice Act (National Council State Boards of Nursing, 2022) and parental requests for administration as approved by a health professional (DeWitt-Parker, 2016; Patrick & Reiner, 2017).
Research Question 2
Federal Status
Not surprisingly, school nurses in the fully legal states expressed significantly less concern about the federal status of cannabis as a Schedule 1 substance (Branson, 2019; Bridgeman & Abazia, 2017; Devane, 2013; Patrick & Reiner, 2017) than their colleagues in medical only and illegal states. The consistency of legal expectations supporting both medical and recreational use of marijuana in these states may shape the perception that the ongoing conflict between federal and state status is not a large concern. Conversely, in those states where cannabis is illegal or approved only for medical use, school nurses may perceive a lingering stigma based on the federal classification and thereby maintain more fear of consequences for violating federal drug-free workplace requirements or losing government funding for school-based programs (Bridgeman & Abazia, 2017; Patrick & Reiner, 2017). Participants in this study split on whether cannabis should be reclassified from its Schedule 1 status, which reveals that school nurses are not all in agreement that medical cannabis should be treated as a ‘legal’ therapeutic option on the federal level. Anecdotally, school nurses may not be the only stakeholders hesitant to cross the federal policy line as school attorneys may recommend that districts avoid developing medical cannabis policies. Notably, Gilsbach (2019) postulates that the expansion of medical cannabis legalization within the past few years will require school entities to address this issue more frequently. Because this is a new area of law lacking bright line guidance, he recommends that schools proceed with caution.
Knowledge Deficits
Overall, school nurses did not significantly differ in their perceptions of knowledge deficits, with school nurses in illegal states scoring slightly but not significantly lower than their fully legal and medical only counterparts. Despite the relatively high mean scores, individual items in this category recorded a large percentage of nurses who desire more educational opportunities on medical cannabis (92%) because they do not feel confident answering questions from a parent requesting medical cannabis administration at school for their child (60%). These findings align with the findings of Elliott (2019) supporting additional educational opportunites on medical cannabis, as this topic is not generally included in most nursing curricula (Garcia, 2020; Zolotov et al., 2021). Lacking a solid foundation of knowledge of medical cannabis among health care providers is a common theme within the literature, and fear of the unknown may also create hesitancy in medical cannabis policy development (Arnfinsen & Kisa, 2021; Balneaves & Alraja, 2019; Nugent et al., 2020; Rønne et al., 2021; Ryan & Hopko-Sharts, 2017; Zolotov et al., 2021). By providing additional professional development opportunities on medical cannabis, school nurses’ confidence in discussing the issue with both school and community members may increase.
Safety Concerns
Overall, safety concerns received the lowest mean score (7.6), indicating the highest degree of concern. School nurses in fully legal states displayed less concern, possibly reflecting a perception of greater safety based upon state statutes removing all restrictions on cannabis use. The significantly higher levels of concern for school nurses in medical only and illegal states may be related to apprehension about the potential adverse effects of medical cannabis on students, such as (a) exacerbating pre-existing mental health conditions; (b) regulating the level of tetrahydroncannabinol a student receives (Hasin, 2017; Lafaye et al., 2017; Nugent et al., 2020); (c) triggering cannabis use disorder (Cerda, et al., 2017); or (d) impairing memory and cognition (Hasin, 2017; Hill, 2019). Unlike many other medications school nurses administer, the mechanism for approval and dispensing of medical cannabis provides ambiguity about the approval of the medical establishment for this drug (Davenport & Pardo, 2016; Rubin, 2017; Woo et al., 2020). Given the limited primary research on the safety of medical cannabis usage with school-age children (Arnfinsen & Kisa, 2021; ) coupled with the non-standard means of prescription, school nurses may hesitate to permit medical cannabis use in the school setting. Unfortunately, unless the federal government removes cannabis from the list of Schedule 1 substances, safety and efficacy research is likely to remain limited.
Stigma
Surprisingly, the overall mean score for stigma was the second-highest (9.3) among all influential factors. Stigma items explored whether perceptions of stigma related to cannabis use interfered with school nurse's decision-making related to use in school, the morality of denying a child use of their medical cannabis during the school day and supporting cannabis policy development. Although school nurses in both fully legal and medical only states expressed significantly less concern about stigma affecting their judgment, the perception of lack of stigma must be interpreted with caution. Governmental approval of medical use may alleviate some stigma for nurses in these states, but underlying stigma may persist (Isaac et al., 2006). The historical negative perceptions of cannabis use may be implicit rather than explicit (Cohen, 2010; Joffe & Yancy, 2004; Ryan et al., 2019), and therefore the school nurses may not be fully aware of the degree to which stigma may affect their decisions. This implicit bias can interfere with the willingness to advocate use for a patient with a qualifying condition (Melnikov et al., 2019). However, it is unclear whether any social desirability effects related to the moral imperative in nursing (Leos-Toro et al., 2018) may have influenced nurse responses indicating little concern for stigma, or whether any implicit bias based on stigma influenced the responses expressing higher levels of concern for safety and federal status. Also, the contradiction between the participants’ relative lack of concern about stigma and the nurses’ lack of consensus on whether cannabis should be removed from the Schedule 1 status may indicate that nurses are unsure about their beliefs related to recreational versus medical use of cannabis.
Stakeholder Collegiality
Stakeholder collegiality included school nurse involvement working with key stakeholders in developing policy, school nurse voice, and comfortability in communicating health policies for their district. Collegiality ranked highest overall with a mean of 9.6, indicating that school nurses did not view this as an area of concern. An overwhelming majority of respondents perceived that they were involved with the development of student health policies within their district, thus lack of school nurse collegiality does not appear to be an influential factor for the development of a school medical cannabis policy.
Implications for Practice
The study findings offer several suggestions for the K-12 setting. An initial step would be continued discussion of medical cannabis policy with school stakeholders. Additionally, school nurses should collaborate with their colleagues in other school districts to share best practices, concerns, and policy considerations. Maintaining professional, collegial relationships between school nurses and administration will lead to more effective development of policies that impact student health (Bacon et al., 2017; Bogaert et al., 2016; Juma et al., 2014) Should the use of medical cannabis continue to increase, formally educating the school nurses who are at the forefront of student health policy is imperative (Felnhofer et al., 2021). This education should include the potential side effects of medical cannabis, its uses, and interactions with other medications; filling any knowledge deficits within these topics may foster more acceptance for medical cannabis use in the school setting (Balneaves & Alraja, 2019; Garcia, 2020; Melnikov et al., 2019; Nugent et al., 2020; Rapp et al., 2015). To address uncertainty in policy development and implementation, state regulatory departments should develop and publish practice statements providing guidance to school nurses and administrators, particularly with respect to addressing the safety concerns, stigma, and federal status influential factors that inhibit effective responses to family requests (Balneaves & Alraja, 2019). Lastly, Federal Status and Stigma mutually reinforce each other; reclassifying cannabis from its Level 1 drug status federally may alleviate some of the hesitancy and stigma as noted in these survey results (Campbell, 2015; Taylor, 2016; Tilburg et al., 2019).
Limitations
Several limitations were present in this project. First, the sample size was limited to school nurses affiliated with their school nurse organization in sixteen states, thus the findings cannot be generalized to all practicing school nurses in the country. Replicating this study with a wider pool of school nurses in all states nationwide would better capture school nurse perceptions of the states where cannabis is illegal. During the implementation of this study, the landscape of cannabis has been dynamic , with changing state policies nationwide. At the time of distribution for the questionnaire, few states remained that completely banned cannabis use, and not all of these school nurses’ associations agreed to participate. Consequently, the disproportionately higher representation of school nurses from fully legal states and much lower representation of nurses from illegal states participating in this study may have influenced the overall results.
Recommendations for Further Study
To broaden this area of research, a timely replication of this study could survey school administrators, members of the school board, and school solicitors to determine whether their perceptions of the influential factors align with those of the school nurses. Knowing the perceptions of other key stakeholders could provide a more rounded view of the forces affecting medical cannabis policy development. An analysis of litigation related to school district medical cannabis policy presence or absence could provide insight on the legal risks involved in this developing policy area. By conducting a study to collect more school nurse perceptions nationwide, rather than those affiliated with their state school nurse association would also enrich this area of research. Lastly, a scoping review of medical cannabis policy guidance at the state level could determine the extent to which states address the significant influential factors into recommendations for policy development.
Conclusion
Despite many states legalizing medical cannabis use, an overwhelming majority of school nurses report that their school districts do not have a health policy addressing students who are requesting medical cannabis administered in the K-12 setting. Continued collegial discussion and education about the use of medical cannabis may assist healthcare professionals and school personnel in reducing stigma and thereby supporting proactive policy development to support those students who do not have an alternative for a symptom or disease when medical cannabis is effective. With the prevalence of medical cannabis use where other pharmaceutical treatments are not effective, continued research in this area is imperative to determine best practice for developing school policy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.