
Abstract
Approximately 7% of children live with food allergy, a condition that requires dietary avoidance to prevent an allergic reaction. In this qualitative study, we aimed to understand food allergy-related experiences, beliefs and learning preferences among children with and without food allergies, to inform a school-based, food allergy education program. Data were analysed thematically. We virtually interviewed children in Kindergarten-Grade 8 in Manitoba, Canada, with (n = 7) and without (n = 9) parent-reported, physician-diagnosed food allergies. We identified three themes: Naive reliance on peers and school staff to assist with food allergy management; Limited food allergy knowledge; and, Recommended food allergy curricula: complementary perspective. Our findings will help inform the development of a school-based, food allergy education program, with a long-term goal of minimizing food allergy-related worries and optimizing safety for children with food allergy. Ongoing, school-based food allergy education is needed.
Abbreviations
CSACI, Canadian society of allergy and clinical immunology; EAI, epinephrine autoinjector; URIS, United Referral Intake System
Food allergies affect up to 8% of children (Sicherer & Sampson, 2018). Strict avoidance of the allergen is necessary to effectively manage the condition. Accidental ingestion can result in severe reactions that require prompt administration of an epinephrine auto-injector (EAI) and subsequent assessment by an emergency room physician (Sicherer & Sampson, 2018). In addition to the acute impact of accidental exposures, food allergy has been found to impose chronic burdens on children and families in the form of increased financial costs and decreased well-being (Golding et al., 2021). Anxiety and depression have also been reported among parents and caregivers of children with a food allergy (Feng & Kim, 2019; Polloni & Muraro, 2020).
With an estimated prevalence of 8%, an average-sized classroom of 25 students will include two children with a food allergy, which underscores the importance of careful food allergy management in childcare centres and schools. In actuality, however, these environments may pose additional risks for accidental exposure as children not only spend a significant portion of their time—including time spent eating—at school and childcare centers, but they are also exposed to both staff and peers who may have limited baseline knowledge about the management of food allergy (Waserman et al., 2021). Recognizing the potential for allergic reactions, some institutions have implemented policies aimed at reducing risk, including implementing allergen-free zones and prohibiting certain allergens. However, some experts have argued that these policies actually do more harm than good as they may increase the risk of bullying and the social exclusion of children with food allergy, while doing little to reduce accidental exposures (Waserman et al., 2021).
Departments of Education across Canada have established guidelines—and, in some cases, legislation—for childcare centres and schools to address the risks surrounding food allergy via the development of anaphylaxis policies [Canadian Society of Allergy and Clinical Immunology (CSACI), 2016]. For instance, Sabrina's Law, in the province of Ontario, requires that all district school boards establish and maintain an anaphylaxis policy that includes strategies to reduce allergen exposure, employee training on how to deal with allergic reactions, the development of individual plans for students with severe allergies, and a communication plan to disseminate information about life-threatening allergies to employees, parents, and pupils (CSACI, 2016; Ontario Regulation c7, 2005). Similar legislation exists in Manitoba, Alberta, and British Columbia (Province of Alberta, 2020; Province of British Columbia, 2007; Province of Manitoba, 2009). In addition, Manitoba also offers the United Referral Intake System (URIS), a program that supports children with certain health conditions, such as food-triggered anaphylaxis, so that they can participate in various activities [e.g., education, childcare, respite services (Government of Manitoba, n.d.)].
While anaphylaxis policies and school-based training programs have demonstrated benefits, such as increasing confidence and proper EAI administration technique among childcare centre and school staff (Levinson et al., 2010; Patel et al., 2006), they fail to fully address the needs of food allergic children and their caregivers. In a 2012 Canadian survey of over 1,300 parents of food allergic children, roughly 4 in 10 parents reported that a lack of awareness and training in schools had put their child at risk; this was greater than the proportion who reported that training and awareness in school had helped their child (Cicutto et al., 2012). Inadequate food allergy management policies in schools have been noted in both Canada (Cicutto et al., 2012) and internationally (Ercan et al., 2012; Lawlis et al., 2017; Rhim & McMorris, 2001; Sicherer et al., 2001), the consequences of which can put children with food allergies at an unnecessary risk for anaphylaxis.
Notably, anaphylaxis policies and school-based training programs typically emphasize training childcare centre or school staff—not peers—and they tend to focus solely on management of accidental ingestion but exclude other important topics like risk reduction strategies or food allergy-related bullying (CSACI, 2016, p. 51–56). In contrast, national recommendations on food allergy management includes an educational component for the entire student population, with an emphasis on the unacceptability of bullying those at risk of anaphylaxis (CSACI, 2016, p. 18). In a qualitative research study in the UK in 2010, the majority of the 18 teenage participants relayed that they felt school peers did not appreciate how serious food allergy can be and that it would make things easier for them if their peers understood more about food allergy. In fact, half of the participants identified classmates as the group who most needed to receive food allergy education and information, in comparison with themselves, parents, teachers, and friends (Monks et al., 2010).
Few studies to date have assessed food allergy-related beliefs and experiences among children without food allergy. Amongst Korean children in Grades 4–8, those with food allergies were non-significantly better able to define anaphylaxis and providing allergen alternatives, compared to those without food allergy (Choi et al., 2015). Elsewhere, Australian researchers reported significant differences in allergy-related knowledge between the food allergic community and the general public, 20% of which were defined as <20 years, although not specifically school-aged (Stockhammer et al., 2020). These studies unfortunately provide little transferability within the Canadian elementary school context, thereby underscoring the importance of our work, which aims to elucidate the food allergy-related beliefs, experiences and learning preferences of children, including those without food allergy.
There is a pressing need to fill gaps regarding food allergy knowledge in childcare centres and schools by providing evidence-based communication that promotes the safety and wellbeing of children with food allergies. Since current food allergy programs focus on training childcare and school staff rather than children, it is difficult to assess the latter's understanding of food allergy management. Herein, we aimed to understand the perspectives of children with and without food allergies, specifically regarding their feelings, beliefs and experiences surrounding food allergies, and their preferences for the delivery of food allergy education in childcare centres and schools. The knowledge gleaned from this study will inform the development of a food allergy education program, consisting of grade-appropriate short videos, targeting childcare centres and school staff, as well as children with and without food allergy.
Methods
Participants
Through online convenience sampling via social media platforms (e.g., Facebook, Instagram, Twitter) and word-of-mouth, we recruited Manitoban parents of school-aged children [Kindergarten (K) through Grade 8] with and without parent-reported, physician-diagnosed food allergies.
Instrumentation
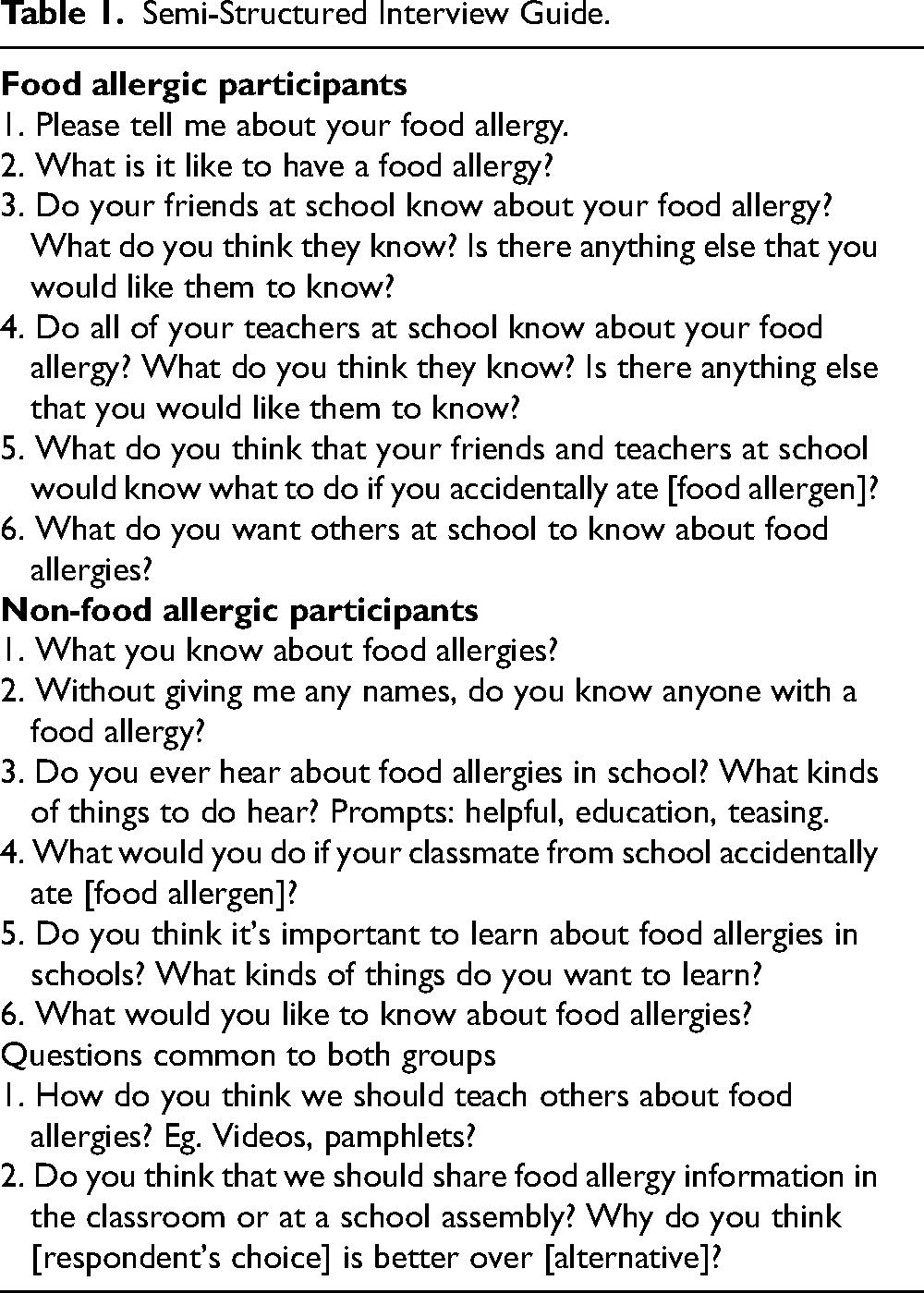
A semi-structured interview guide was followed (Table 1), allowing the interviewer to probe for expanded discussion and clarification. Participant recruitment continued until the data that arose from later interviews were found to be similar in content and sentiment to earlier interviews; this was considered to represent data saturation (Patton, 2015). The mean interview length was 12 min, and interviews were recorded and transcribed verbatim using a third-party transcription agency. Participating families received a $30 e-gift card for their involvement.
Semi-Structured Interview Guide.
Procedure
Parents of all the children provided written consent to participate in our study, and children aged 7 years and older also provided assent. Individual audio-recorded telephone interviews were conducted with the participating children between February and June 2021 by a trained research assistant, under the supervision of the research coordinator (initials blinded for review) and senior author (initials blinded for review).
Data Analysis
Baseline demographic characteristics were described (n/N, %, using Stata (College Station, TX). Qualitative data were independently read, coded, and evaluated by three research assistants using thematic analysis (Braun & Clarke, 2006; Patton, 2015). Transcripts were first read for surface descriptors, with words and phrases systematically and descriptively coded (e.g., “friends”, “epinephrine autoinjector”). Thereafter, transcripts were re-read to identify and code latent meaning (e.g., “disclosure of food allergy to friends”, “teachers’ access to epinephrine autoinjector”). Once data were fully coded, analysts worked to identify themes, as well as the relationship between the themes. The themes were generated using an inductive approach, whereby the content of the interviews informed each theme. The researchers then compared the themes to the interview transcripts to assess whether they were reflective of the data. Any disagreements on the content of themes were resolved through group discussion with the research team. This study was approved by The University of Manitoba Health Research Ethics Board [HS24358(H2020:458)].
Results
Participants
A total of N = 16 school-aged children, ages 5–13 years (K to Grade 8), both with (n = 7) and without (n = 9) food allergies participated in the current study (Table 2). The majority of these participants were male (62.5%) and were in K-Grade 4 (68.8%). Among those with food allergy, tree nut was the most commonly reported allergen (71%), followed by peanuts (57%), sesame (14%), wheat (14%) and shellfish (14%). The majority of the food allergic children reported regularly carrying their EAI (85%).
Participant Demographics.
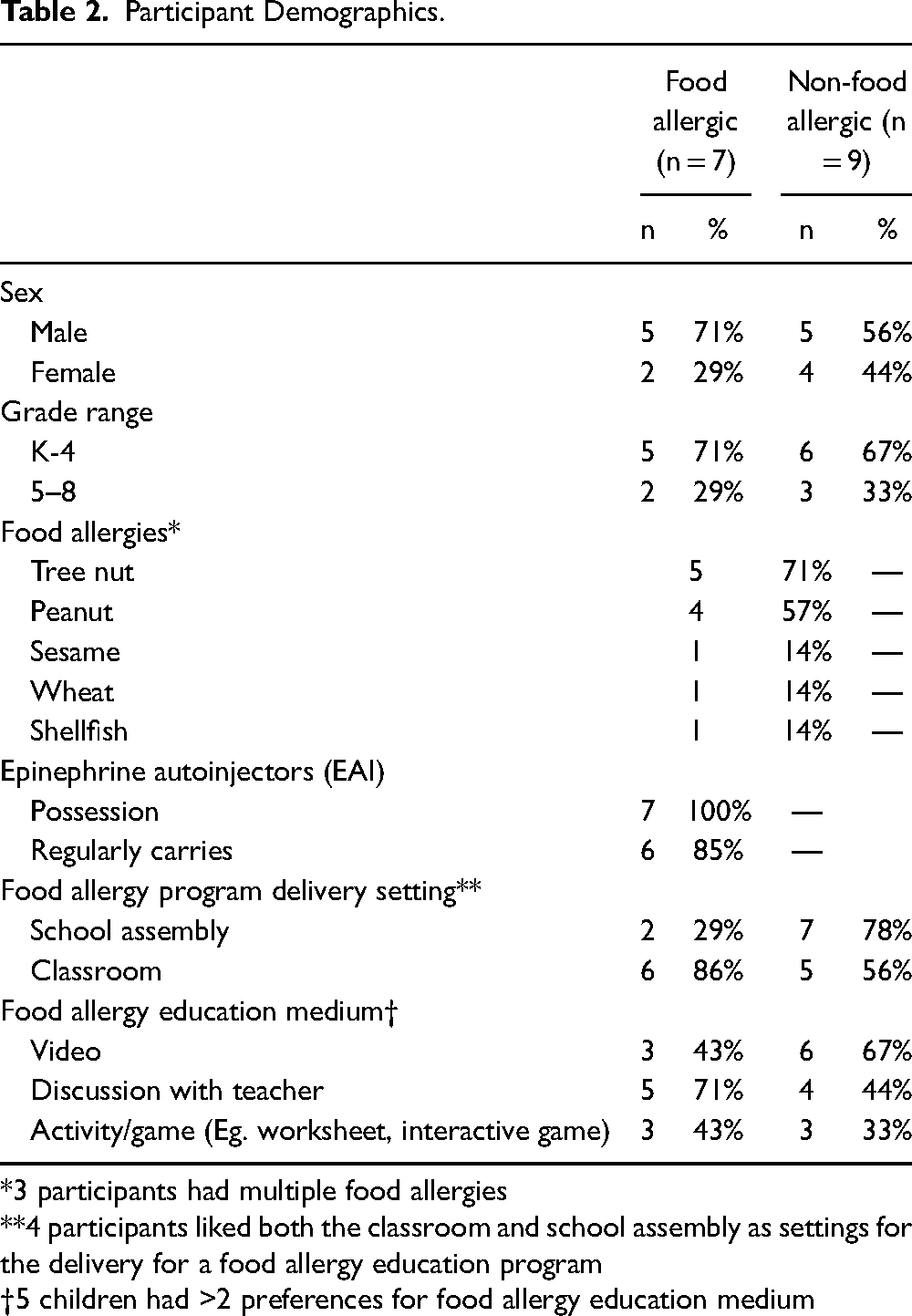
*3 participants had multiple food allergies
**4 participants liked both the classroom and school assembly as settings for the delivery for a food allergy education program
†5 children had >2 preferences for food allergy education medium
Thematic Analysis
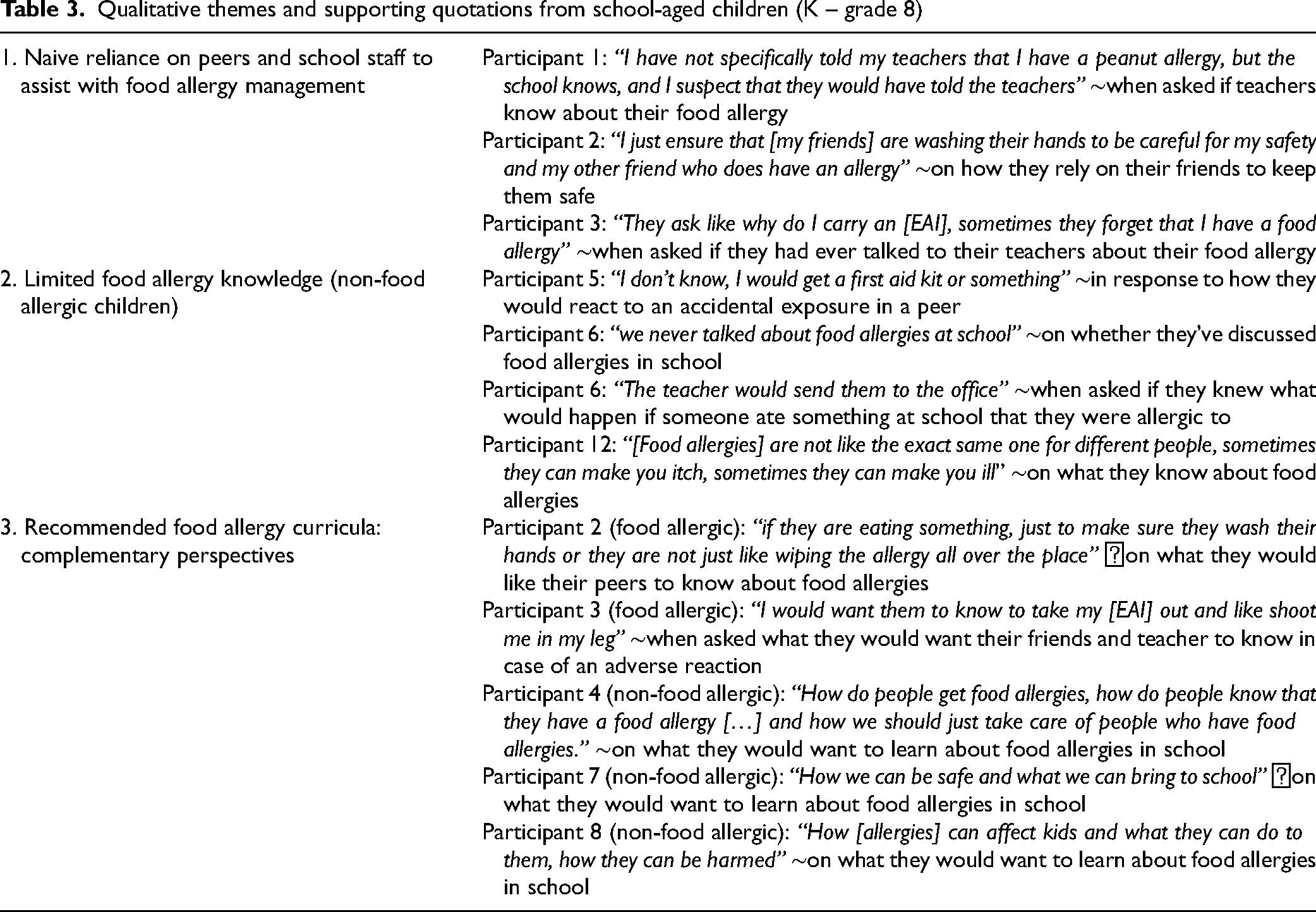
Thematic analysis of the interview transcripts was performed separately by three analysts (Patton, 2015). An initial reading for surface descriptive content identified similar concepts (e.g., knowledge and experiences with food allergies). A second reading identified latent meaning within these identified concepts (e.g., feelings of precariousness). Representative quotations were independently selected from the interview transcripts, semantic checks were discussed amongst the analysts and consensus was reached without disagreement. Thematic concepts were considered saturated once no new constructs emerged (Patton, 2015). A total of 3 themes were identified in the transcripts: Naive reliance on peers and school staff to assist with food allergy management, Limited food allergy knowledge, and Recommended food allergy curricula: complementary perspectives (Table 3). The first two themes were specific to children with and without food allergy, respectively, and the third theme was common to both groups.
Qualitative themes and supporting quotations from school-aged children (K – grade 8)
Theme 1: Naive Reliance on Peers and School Staff to Assist with Food Allergy Management (Children with Food Allergies)
This theme highlights a reliance on peers and school staff to assist in anaphylaxis management, albeit naively, as children with food allergies were unable to describe the level of food allergy knowledge held by these non-food allergic groups. Several children indicated that while their food allergy status was disclosed to school administration (often by parents), they were unsure whether their current teachers (or substitute teachers) and classroom peers knew about their allergy(ies), or where they kept their EAI. One child stated that they believed their teacher would know what to do in case of an accidental allergen ingestion “because I showed them where my [EAI] was”. This child followed up by saying that they were unsure whether their current teacher knows how to administer and EAI, and expressed that they sometimes forget to tell their substitute teachers where their EAI is kept.
Regarding the safekeeping of their EAI, one child stated, “I know that my school knows but I am not sure that my teachers know.” Another child stated, “I don't really know what they know”, regarding their teachers’ knowledge about food allergy and how to use EAIs. They expanded on this statement by saying, “that is the reason why my friends know”, highlighting that they rely on their peers to assist with food allergy management as a means of filling in gaps that may be present in the knowledge of school staff. Additionally, some children indicated they relied most on their closer friends to assist with food allergy management. For example, one child indicated, “people who I have known longer do know [what to do in case of accidental ingestion] as I have like gone over stuff with them before” as opposed to friends they met recently “who have not exactly had the proper experience with allergies as my older friends.”
In describing how they rely on peers to assist with food allergy management, older children (Grades 6–8), provided greater detail on how others can help keep them safe. As an example, one child indicated that they diligently “ensure that [my friends] are washing their hands to be careful for my safety” and stressed throughout the interview that others need to be “careful”, referring to the risks associated with cross-contamination. Several others explicitly mentioned that their friends check the ingredients of what they eat, as a way of reducing risks to the food allergic child.
Theme 2: Limited Food Allergy Knowledge (Children Without Food Allergies)
This theme, which was unique to children without food allergies, reflects their limited understanding of food allergies and their management. Younger children (K – Grade 4) reported the least amount of food allergy knowledge and reported that they did not discuss food allergies in school, other than the fact that certain foods were prohibited. This group knew that their peers with food allergies needed to avoid the foods that they were allergic to in order to prevent a reaction. However, when asked how they would respond to an adverse reaction in a food allergic peer, their answers were indicative of a lack of food allergy knowledge. For instance, one child responded, “I don't know, I would get a first aid kit or something”, while another believed that “the teacher would send them to the office”. Older children (Grades 5–8) knew some general details about food allergies, namely that they can differ amongst individuals and that presentation can vary. However, they were typically unsure about the routes of exposure and how to help in the event of an accidental ingestion. Despite this, some children did possess a vague understanding of how to manage accidental exposures. For instance, one child indicated that “I would probably tell someone in the class, if they knew how to use an [EAI] or whatever, but I am pretty sure you just open the lid and then you would put it into the leg or whatever”. Collectively, both age groups agreed that they would seek help from an adult, namely their teacher, in the event that a peer was suffering from an adverse reaction to a food allergen.
Theme 3: Recommended Food Allergy Curricula: Complementary Perspectives
This theme reflects what both groups of children would like to see in a school-based, food allergy education program. Most participants indicated that they saw value in such a program. The one child who indicated that they did not think it was important to learn about food allergies in school was a child without food allergy who said: “We never talked about food allergies at school so no [it is not important to do so]”. This suggests that the current lack of food allergy education in school signaled to them that it is not an important school topic, despite the fact that this child had also expressed that food allergies were important to know about in general.
More children showed a preference for delivery of the program in a classroom setting (n = 11; 68.8%) over a large group setting, such as a school assembly (n = 9; 56.3%). Of the 16 participants, 25% indicated that they liked both settings. Nonetheless, there were differences between groups. The majority of children with food allergies favoured a classroom delivered food allergy education program (85.7% vs. 28.6%), stating that they felt more “comfortable” in a smaller environment where they could engage in intimate discussions with their classmates and teachers. In contrast, the majority of children without food allergies preferred an assembly (77.8% vs. 55.5%) indicating that the larger setting would provide an efficient way to reach a larger audience (e.g., “I would do school so the whole school could hear.”). A lesson/discussion with a teacher was the most preferred teaching method amongst the children with food allergies (71.4%), whereas a video was the top choice amongst children without food allergies (66.7%). Children with food allergies were most concerned with educating peers and staff on preventing reactions, such as by encouraging them to “wash their hands” after eating, learning to read food labels, and how to treat reactions through use of an EAI. In contrast, children without food allergies were most interested in the etiology of food allergy, specifically “how do people get food allergies”, as well as how to identify and treat reactions.
Discussion
In this qualitative study, we sought to understand the personal experiences and perspectives of children, in K – Grade 8, on food allergy. We identified three themes from the interview transcripts, two of which were unique to each group of children. The first theme captures how children with food allergies relied on their peers and school staff to create safe spaces and help manage adverse events without knowing the level of food allergy knowledge held by these individuals. The second theme underscored the limited food allergy knowledge amongst the children without food allergies. In the final theme, both groups of children shared what they would want to see in a food allergy education program. Through use of a knowledge translation strategy (Graham et al., 2006), the information collected from this study, combined with partner engagement discussions on age groups and learning environments (classroom vs. school assembly), will shape the delivery of a food allergy education program geared towards school-aged children,
Consistent with existing research (Fenton et al., 2011; Monks et al., 2010; Stjerna, 2015), participants with food allergies disclosed that, they relied on others to help keep them safe. Nearly all children assumed that their teachers and school staff knew about their food allergies, as well as where they kept their EAI, however the majority could not recall ever having specific conversations on these issues; instead, they assumed that their parents had these discussions with school personnel. Participants in the current study also elaborated on how others helped keep them safe, specifically mentioning handwashing and disclosing ingredients when food is shared. These findings align with a 2015 study by Stjerna, in which children aged 11–17 years with food allergy admitted that they were dependent on their peers to help create a safe environment (Stjerna, 2015). This study also found that children with food allergies felt greater insecurity at lunchtime, which is less structured and more relaxed compared to the regimented, adult supervised, class time. The reliance of children with food allergies on others to help keep them safe further justifies the introduction of an in-school food allergy education program, in line with national recommendations (CSACI, 2016, p. 18).
While non-food allergic children in our study had a general awareness of food allergies—most consistently a cognizance of school/class food-bans and indirect experiences with food allergies through a family member, friend or peer—there were notable knowledge gaps amongst these participants. As food allergy knowledge gaps amongst participating children were wide, the content of such an educational program should be relatively broad and focus on basic food allergy information. Based on the results of the current study, it appears as though the program content should address topics indicated by those with and without food allergy, including EAI training and cross-contamination, and the pathophysiology and management of food allergy, respectively.
The majority of children in the current study shared a mutual interest in the idea of a school-delivered, food allergy education program, both for their own benefit and to help protect those around them. However, children with and without food allergy disagreed regarding the content, mode of delivery and the setting in which the food allergy education program should take place. Among children with food allergies, there was a notable preference for an interactive classroom discussion, whereas children without food allergies indicated that they would prefer to watch a video on food allergy delivered in a school assembly setting. Children with food allergies indicated they preferred the classroom setting, namely for reasons of embarrassment (for being different), increased comfort within their homeroom teaching environments and the greater perceived opportunity to ask questions. Amongst those with food allergy, the preference for food allergy education to be delivered in a more intimate classroom setting may be connected to food allergy-related stigma, which has been described in some, albeit not all schools (Dean et al., 2016). Participants in a 2015 exploratory study on health-related stigma amongst children with food allergies reported experiencing enacted (e.g., bullying, exclusion) and felt (e.g., embarrassment for being different) stigma as a result of their food allergy, with the latter being more common (Dean et al., 2016). Indeed, some participants in the current study expressed that they felt “embarrassed” by their food allergy, and a majority stated that they did not readily disclose their health status to others, with the exception of teachers and close friends. Those planning future food allergy education programs should consider the possibility of embarrassment on the part of children with food allergy. One important area of future research would be the extent to which food allergy education programs in schools normalize the concept of food allergies and reduce enacted and felt stigma.
Implications for School Health Policy, Practice, and Equity
Currently, there is a paucity of evidence-based research evaluating food allergy education in the Canadian school setting, given the paucity of national programs informed with input from children. Application of anaphylaxis risk reduction strategies (e.g., increasing food allergy awareness in schools), early recognition of reactions and swift treatment with an EAI, are crucial measures in effectively treating anaphylaxis and keeping schools safe for children living with food allergies. Recognizing this, several international groups have launched educational interventions to support food allergy awareness in schools. Several pilot studies employing food allergy training programs for school personnel and parents of children with food allergies, showed remarkable improvements in related knowledge post-delivery (Gillespie et al., 2014; Polloni et al., 2020). Food Allergy Canada has Allergy Pals and Allergies Allies—online platforms that offer peer mentoring support for children with food allergies, ages 7–11 and 12–15 years, respectively. The American Food Allergy & Education Research (FARE) group offers the Be a Pal ® training program, aimed at empowering children without food allergy knowledge so that they can help take care of those with food allergies (Food Allergy Research & Education, n.d.). The limited audience reach of existing programs further highlights the need for a formal, school-based food allergy educational approach that targets children with and without food allergies alike, with evidence-based, grade appropriate food allergy knowledge.
The role of the school nurse in food allergy management is significant, and multi-faceted (Santos et al., 2022). Given that there is a limited number of school nurses for a significant number of students, varying by school, and that oftentimes these nurses are not always on site, a formal educational approach for students will assist in allergic reaction prevention and management in case of an allergic emergency (Ben-Shoshan et al., 2008). In this capacity, the school nurse will be supported by those nearest to the emergency and a quicker response will be provided, benefiting the child facing the reaction. Additionally, previous literature suggests that school nurse knowledge of food allergy management is inconsistent and, in some cases, “self-taught”, in which case a formal education program would also serve as a refresher course for school nurses as well (Carlisle et al., 2010). Coinciding with the current “return-to-school” from the COVID-19 pandemic, school nurses will be facing a return to risks of allergic reactions in school. We have previously reported that children experienced an increase in anxiety since the pandemic, and that children with food allergy had experienced a reprieve in bullying when online school from home was in place (Merrill et al., 2022). A return to in person learning may increase the anxieties that accompany experiencing bullying, as well as exposure to possible allergens, in addition to COVID-19 anxiety. As such, school nurses and staff will be returning to a state in which children's mental health may be perturbed. To this end, a food allergy management educational program may assist in limiting allergen exposures, decrease bullying of food-allergic children, and allow school nurses and other personnel additional capacity to care for the mental health impacts COVID-19 has presented to children.
Limitations
We acknowledge several limitations of our study. Firstly, this study focuses on the individual experiences and perspectives of school-aged children in a single city. As such, our study may not reflect the opinions of school officials. The current study was also launched amidst the COVID-19 pandemic—a time when families were juggling competing priorities due to the lockdown and related public health restrictions, which may have affected participation. However, participants were actively recruited until successive interviews began to bring up many of the same concepts without major contradictions, per protocol, suggesting that the COVID-19 pandemic may have slowed the rate of recruitment but not the number of participants ultimately recruited. Interviews were relatively short, and this is likely a reflection of the limited knowledge that children both with and without food allergy had about the topic and a general reticence amongst this age group when speaking with unfamiliar adults. Lastly, this study focused on individual perspectives of school-aged children and did not involve a content analysis of school policies or their communication strategies; it is possible that there are existing school-based food allergy programs that are more comprehensive than the ones reflected in this study.
Conclusions
In this qualitative study, we identified three themes centered on the food allergy-related perceptions and experiences of school-aged children. Children with food allergies described their dependence on school staff and peers to help manage food allergies, despite the fact that children without food allergies relayed substantial gaps in their food allergy knowledge. Both groups shared a mutual interest in learning about food allergies, with some noted differences in content, method of delivery and setting. The information gleaned from this research will go on to inform the development of a school-based, food allergy education program. Further research is needed to evaluate the efficacy of food allergy communication to school-children, as well as intermittent reassessment of such programs. Future research to describe the thoughts of school nurses and teachers may also assist in the development of this education program.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Human Subjects Approval Statement
This study was approved by The University of Manitoba Health Research Ethics Board [HS24358(H2020:458)].
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Manitoba, (grant number University Collaborative Research Program Applicat)