
Abstract
We investigate the presence of health disparities in emergency department (ED) disposition decisions and if crowding levels might have an exacerbating role. Using data from a large, academic ED, we find statistically significant associations between ED disposition decisions and patient sex, race, as well as ethnicity, with male, Caucasian, and non-Hispanic patients being more likely to be admitted to the hospital compared with, respectively, female, African-American, and Hispanic patients. In line with earlier findings in other studies, we find that longer waiting times, suggesting higher levels of ED crowding, is associated with higher rates of admission. Moreover, longer ED wait times modified sex differences, suggesting that the disposition disparity in female patients might be exacerbated when the ED is more crowded.
Introduction
Health disparities, as defined by the Centers for Disease Control and Prevention (CDC), are “preventable differences in the burden of disease, injury, violence, or opportunities to achieve optimal health that are experienced by socially disadvantaged populations” (CDC 2008). Despite improvements in public health in general and growing awareness of the existence of health disparities in our society, studies have shown that disparities in different parts of our health care system have persisted or even widened over the years (Institute of Medicine (US) 2012). Emergency departments (EDs), which see roughly 130 million patient visits in United States every year (Cairns et al. 2018), are no exceptions. Prior work has established that health disparities exist in various forms in EDs, and socially disadvantaged populations are associated with longer length of stay, lower assigned acuity levels, lower medical resource usage, higher mortality rates, and lower likelihood of prioritization within the same acuity level (see Johnson et al. 2013, Lin et al. 2022, Pines et al. 2009, Rees et al. 2020, Schrader and Lewis 2013, Sedaghat et al. 2014).
In this essay, we focus on patient disposition decisions in the ED. Specifically, we investigate whether there is any evidence for the presence of disparities in disposition decisions with respect to patient sex, race, and ethnicity. We also investigate if operational factors such as ED crowding might contribute to the strength of any disparity that might exist. The disposition decision for a patient determines whether the patient will be discharged from the ED, admitted to the hospital, or transferred to a different location. Despite the evidence of disparities elsewhere in the ED, investigation of disparities in disposition decisions is important for two reasons. First, these decisions are made at the very end of ED encounters typically allowing for time to gather information and deliberation on each patient. As an example, this is in contrast to patient triage, where decisions are made within a much shorter time period, under limited information and relying to some extent on the triage nurse's general impression of the patient. Therefore, it is important to understand whether disparities are present even when there is (relatively) less time pressure and more information when making decisions. Second, studies have shown that errors and delays in ED disposition decisions can have significant long-term negative effects on the health and well-being of patients (see, e.g., Plunkett et al. 2011, Fernando et al. 2018). Therefore, any disparity that might exist in disposition decisions has implications that go beyond the ED, which suggests that its study is important to better understand the factors that contribute to differences in health outcomes for different demographic groups within our society.
There exists some prior work on disparities in ED disposition decisions. However, in most of this work, the focus has been narrower than ours in this essay. For example, some of the papers (e.g., Selassie et al. 2003, Lo et al. 2018, and Longcoy et al. 2022) concentrate on patients with specific health conditions only (respectively, trauma, heart failure, and coronavirus disease 2019 [COVID-19]), and others focus on pediatric patients alone (Chamberlain et al. 2007 and Zhang et al. 2019). In agreement with our findings, all these studies find socially disadvantaged groups are associated with a lower likelihood of admission. Arroyo et al. (2012), Ruger et al. (2003), Sacks et al. (2011), Selassie et al. (2003), Selassie et al. (2004), Venkatesh et al. (2019), and Wilson et al. (2016) analyze the general ED population, but their focus is on patients’ socioeconomic status captured through their insurance status. They find that patients of lower socioeconomic status are less likely to be admitted to hospital. Our analysis in this essay is different from these three papers in that we focus on disparities with respect to sex, race, and ethnicity controling for patients’ insurance status. To the best of our knowledge, Zhang et al. (2020) is the only paper that looks at race/ethnicity based disparities within the general adult ED patient population. Similar to our findings, this paper also finds association between race/ethnicity and disposition decisions. However, our focus is broader in that we also consider patient sex (in addition to race and ethnicity) as another variable where disparities might be present. More importantly, unlike any of the papers in the literature, we also investigate any effect ED crowding might have on disparities in ED disposition decisions.
Some of the papers in the literature investigated the relationship between ED crowding and disposition decisions. Chen et al. (2020), Gorski et al. (2017), and Ouyang et al. (2022) all find that, in agreement with our findings, increased ED occupancy is associated with higher hospital admission rates. However, these papers do not look into whether crowding might be playing any role in disparities. As we discuss in this essay, our analysis reveals that controlling for other factors, males are more likely to be admitted to the hospital than female patients, and regardless of sex, patients are more likely to be admitted to the hospital when the ED is more crowded. Interestingly, however, we also find that the effect of crowding is statistically stronger for male patients. These observations together suggest that disparities with respect to sex are exacerbated by increased crowding levels in the ED.
The question of precisely what leads to disparities in disposition decisions is out of the scope of this essay and we refrain from making any causal conclusions. However, one contributing factor could be decision makers’ implicit biases related to race, ethnicity, and sex. Implicit biases are very common and thus it would not be surprising to see them in ED decisions as well. In fact, Johnson et al. (2016) find not only some evidence of the existence of implicit biases through implicit association tests but also that these biases get stronger when the ED is more crowded. Similarly, within an experimental environment, Stepanikova (2012) observes that African-American and Hispanic patients are more prone to receiving less serious diagnoses when physicians are under significant time pressure. This impact of time pressure and cognitive load on decision-making, which would naturally increase during times when ED is more crowded, would explain our finding related to the impact of crowding on disparities with respect to sex.
One of the main objectives of this essay is to highlight this potential connection between disparities and operational factors that can impact decision making. Prior work, mostly from the healthcare operations literature, has already established connections between system load or cognitive load and decision making or various related measures such as service speed and quality of care; e.g., see Batt and Terwiesch (2017), Bavafa and Jónasson (2021), Berry-Jaeker and Tucker (2017), Chiu et al. (2018), Deo and Jain (2019), Kc and Terwiesch (2009), Kuntz et al. (2015), Pan et al. (2022), and Pines (2017). However, we are not aware of any papers that investigated the impact of operational factors on disparities in the ED.
Empirical Setting
Clinical Context
Following approval from the institutional review board, a retrospective cross-sectional study was conducted based on data collected during January 1–December 31, 2019 from a large, academic ED in the Southeastern US. During the study period, this ED had 62,552 patient visits, which is close to the mean annual number of patient visits to academic EDs across the US surveyed in 2016 (Peterson et al. 2019). In this ED, 59 beds are divided among one pediatric and five adult care areas. It is also one of the largest referral centers in its state and a Level I Trauma Center with a diverse patient population and a high hospital admission rate. The ED is part of a medical center, which is located within a metropolitan statistical area with a population of approximately 650,000. Based on data provided by censusreporter.org and US Census Bureau, the median age is close to 39, similar to the state median age. The percentage of Caucasian, African-American, and Hispanic populations are respectively 54%, 24%, and 12% compared with 70%, 22%, and 10% for the whole state. The median household income is close to $71,500, which is roughly 20% higher than the state median. However, approximately 14% of the households are below the poverty line, which is similar to the state percentage.
The ED under study operates in ways that are similar to most US EDs (see Figure 1). Through triage, patients are placed in one of the five Emergency Severity Index (ESI) categories (Gilboy et al. 2012). At the end of their ED visit, the majority of patients are either discharged or admitted to the main hospital.
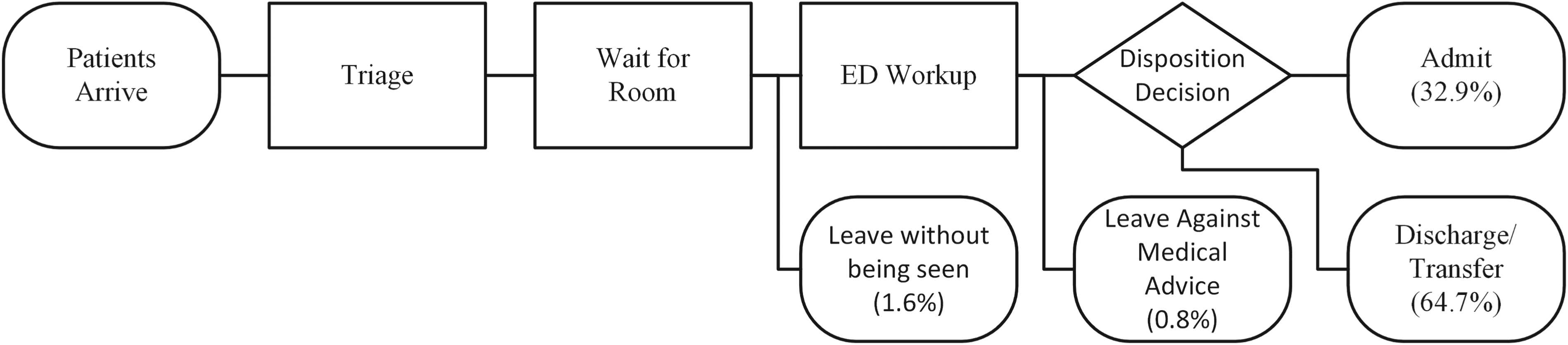
Patient flow within the emergency department (ED).
This study uses data extracted from the Epic Electronic Health Record Systems (Epic Systems Corporation 2022). For each patient encounter, information including patient demographics, acuity, chief complaint, care area within the ED, and time stamps for all major events during the patient's stay are contained in the dataset. For each patient encounter, if available, we also extract the related past medical history using ICD-10 codes, which are indicative of any comorbidities.
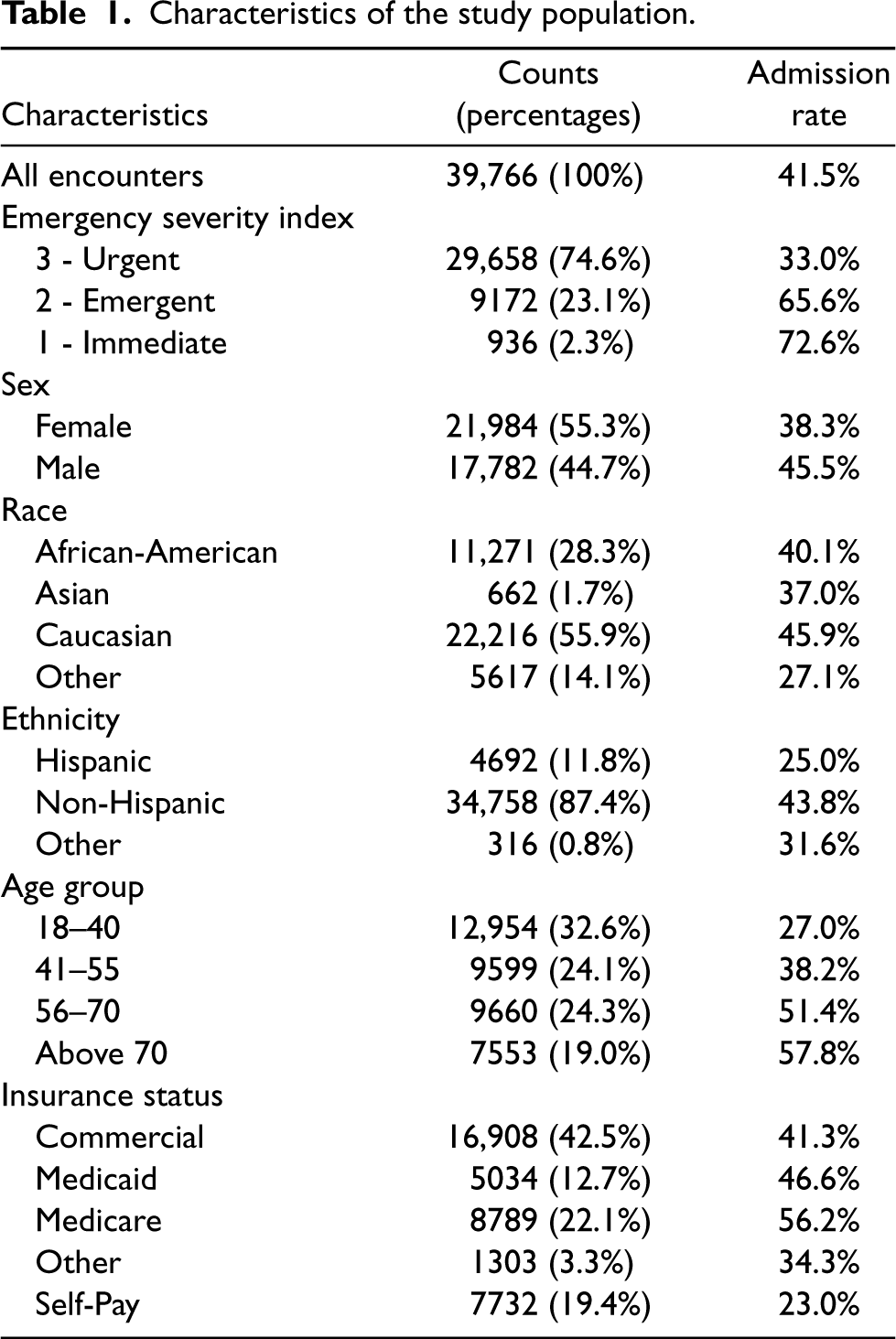
To prepare the data for analysis, we removed duplicate patient encounters and those with missing or erroneous information. Additionally, we excluded patients with a sex other than male or female due to their extremely low count (0.014% before cleaning). To avoid statistical instability, we excluded ESI 4 and 5 patients due to their small proportion (17.7%) and low admission rates (3.6%). We focus solely on adult patients who were treated in care areas A, B, C, and D with disposition decisions classified as “admission” or “discharge,” as these patients went through a more standardized care process and had complete data recorded. Consequently, patients who left without being seen or against medical advice, which make up about 2.4% of the dataset before cleaning, were excluded. (As Section EC.6 of the Online Supplemental material demonstrates, this does not introduce any significant selection bias.) Patients who were transferred to another facility were also excluded (around 1% in our dataset). Summary statistics of the resulting dataset can be found in Table 1.
Characteristics of the study population.
Characteristics of the study population.
Main Effect of Patient Demographic Variables
To investigate whether ED disposition decisions might be influenced by patient demographics, the primary response variable,
Explanatory variables included in the multivariable logistic model.
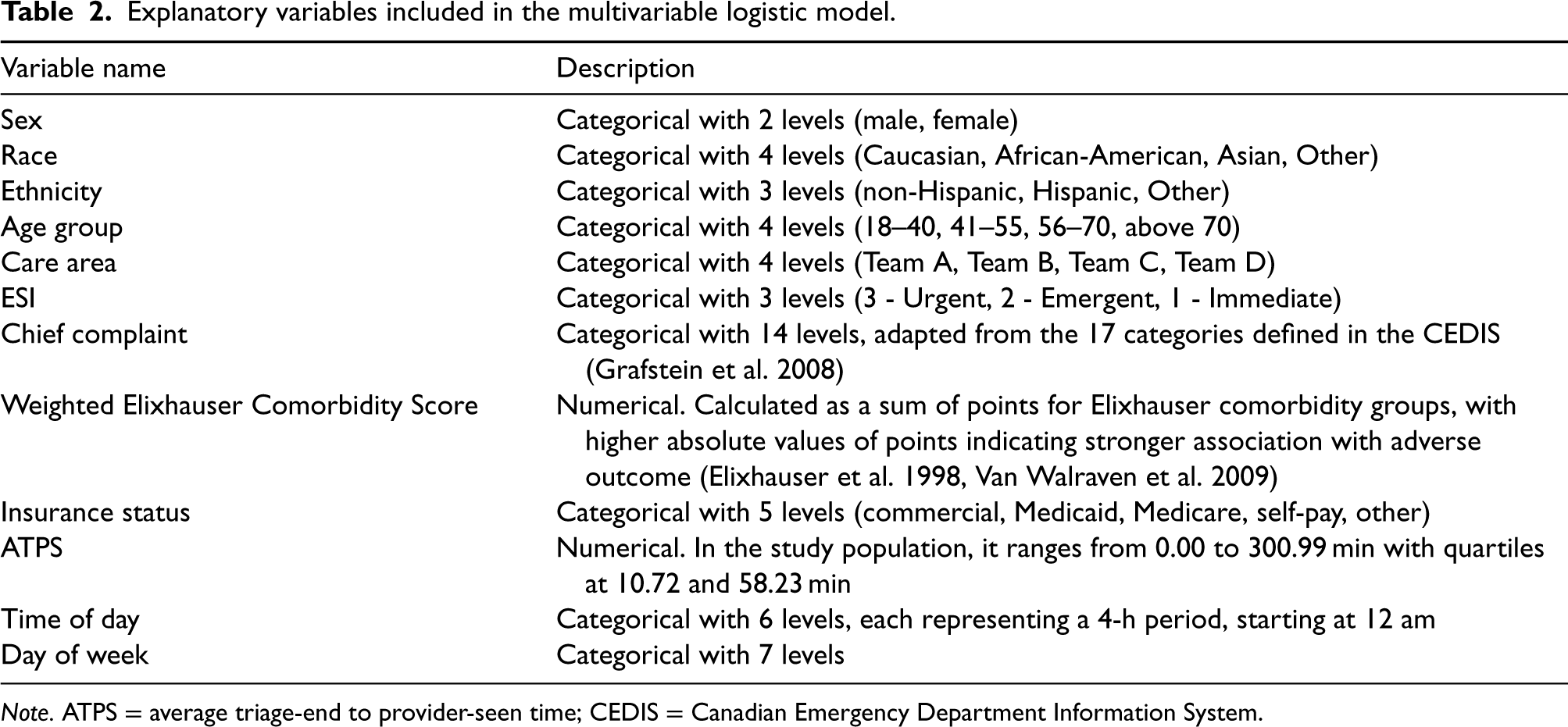
Explanatory variables included in the multivariable logistic model.
Note. ATPS = average triage-end to provider-seen time; CEDIS = Canadian Emergency Department Information System.
We use the above variables to construct the following specifications:

In addition to investigating the presence of disparities with respect to the demographic variables described above, we are also interested in whether ED crowding might have an exacerbating effect. When ED is crowded, ED staff need to process more information, ration resources, and make decisions more quickly. Given the partially subjective nature of disposition decisions and consequently their proneness to biases, we expect disparities surrounding admission decisions to be aggravated when ED is more crowded. To investigate the interaction effects between ED crowding and patient demographic variables, we create three additional Specifications, (2a), (2b), and (2c), based on Specification (1) by respectively adding the interaction terms
Results
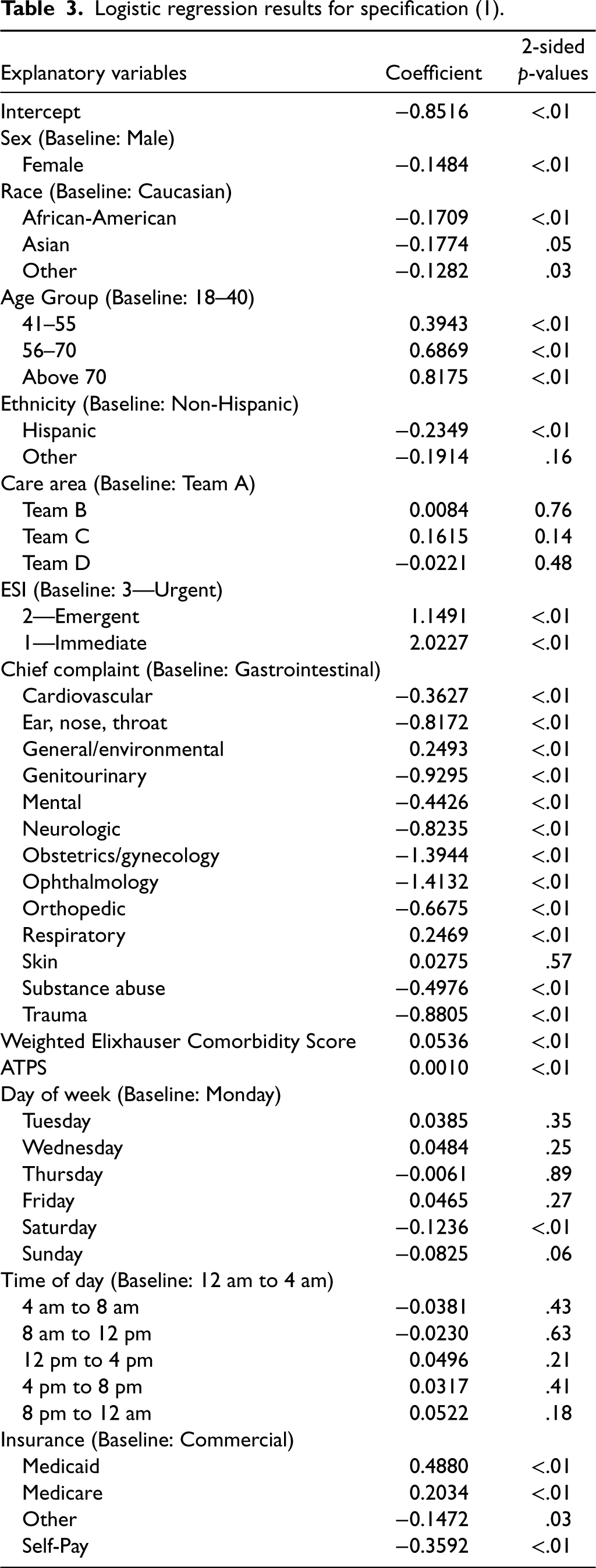
Table 3 presents the results of the logistic regression model obtained using Specification (1). (Our multicollinearity analysis revealed no evidence of strong multicollinearity; see Section EC.2 in the Online Supplemental material for details.) Patients of older age, higher acuity levels, and higher comorbidity scores are associated with a higher probability of admission. Compared with patients who are commercially insured, patients who list themselves as “self-pay” and “other” are less likely to be admitted while patients with “Medicaid” and “Medicare” have higher admission probabilities.
Logistic regression results for specification (1).
Logistic regression results for specification (1).
Our main interest is whether there is an association between demographic variables and disposition decisions. As Table 3 demonstrates, we find a statistically significant correlation between ED disposition and sex. (Throughout the paper, we use a significance level of 0.05.) In particular, females, compared with their male counterparts, are associated with lower admission probabilities. As for race, we also find that patients who belong to the race group of “African-American,” “Asian,” and “Other” are associated with lower likelihood of being admitted when compared to Caucasian patients with these associations being statistically significant. Lastly, ethnicity is also statistically significant with Hispanic patients associated with lower probabilities of admission compared to non-Hispanic patients. In a subgroup analysis, Specification (1) is separately applied to two groups: ESI 1-2 and ESI 3 patients. Significant associations between sex and disposition decisions are found in both groups. Nevertheless, race and ethnicity are only significant in the ESI 3 group, which suggests greater disparities may be present due to the high degree of uncertainty regarding patients’ health in this group. This difference between ESI 1-2 and ESI 3 patients could also possibly be due to the relatively smaller sample size for ESI 1-2 patients. Details of this analysis can be found in EC.3 of the Online Supplemental material.
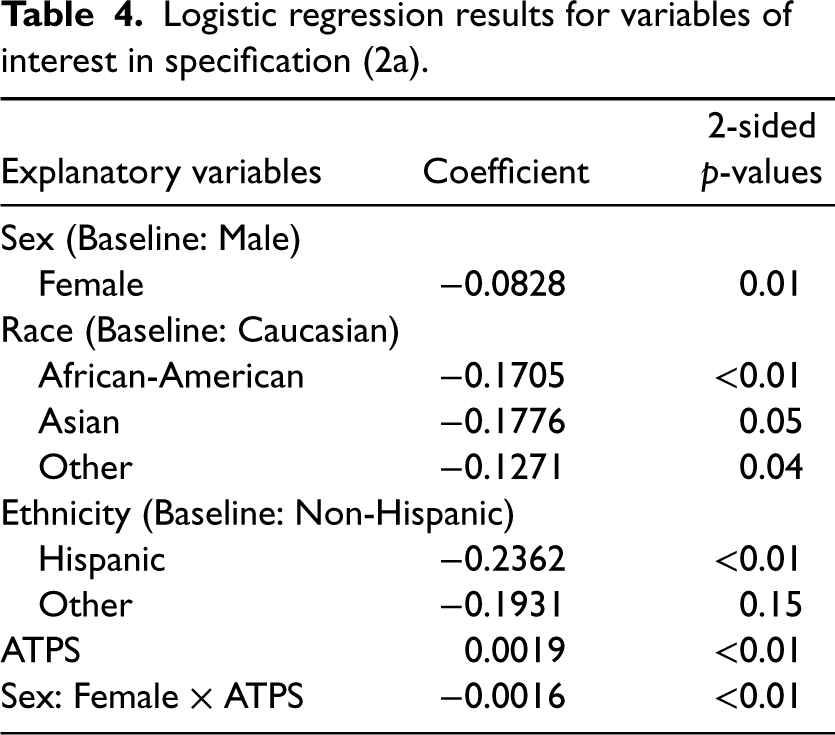
Similar to what prior literature has observed, we also find positive association between ATPS and admission probabilities in our dataset in Specification (1), indicating that patients are more likely to be admitted when ED is more crowded. Furthermore, from the results of Specification (2a) as shown in Table 4, we find that the interaction term between sex and ATPS is significant. This indicates that comparing two patients with similar conditions but of different sexes, the likelihood of admission for the male patient increases with a statistically higher rate as crowding level increases. See Figure 2 for a plot of admission probabilities and 95% confidence intervals as a function of ATPS for two patients one female other male, who received the disposition decision in Team A on a Tuesday between 4PM and 8PM. Both are Caucasian, non-Hispanic, and in the age group 18–40, and have an ESI level 3, a gastrointestinal chief complaint, commercial insurance, and a weighted Elixhauser comorbidity score of 0 (values chosen because they are the most common for each variable).
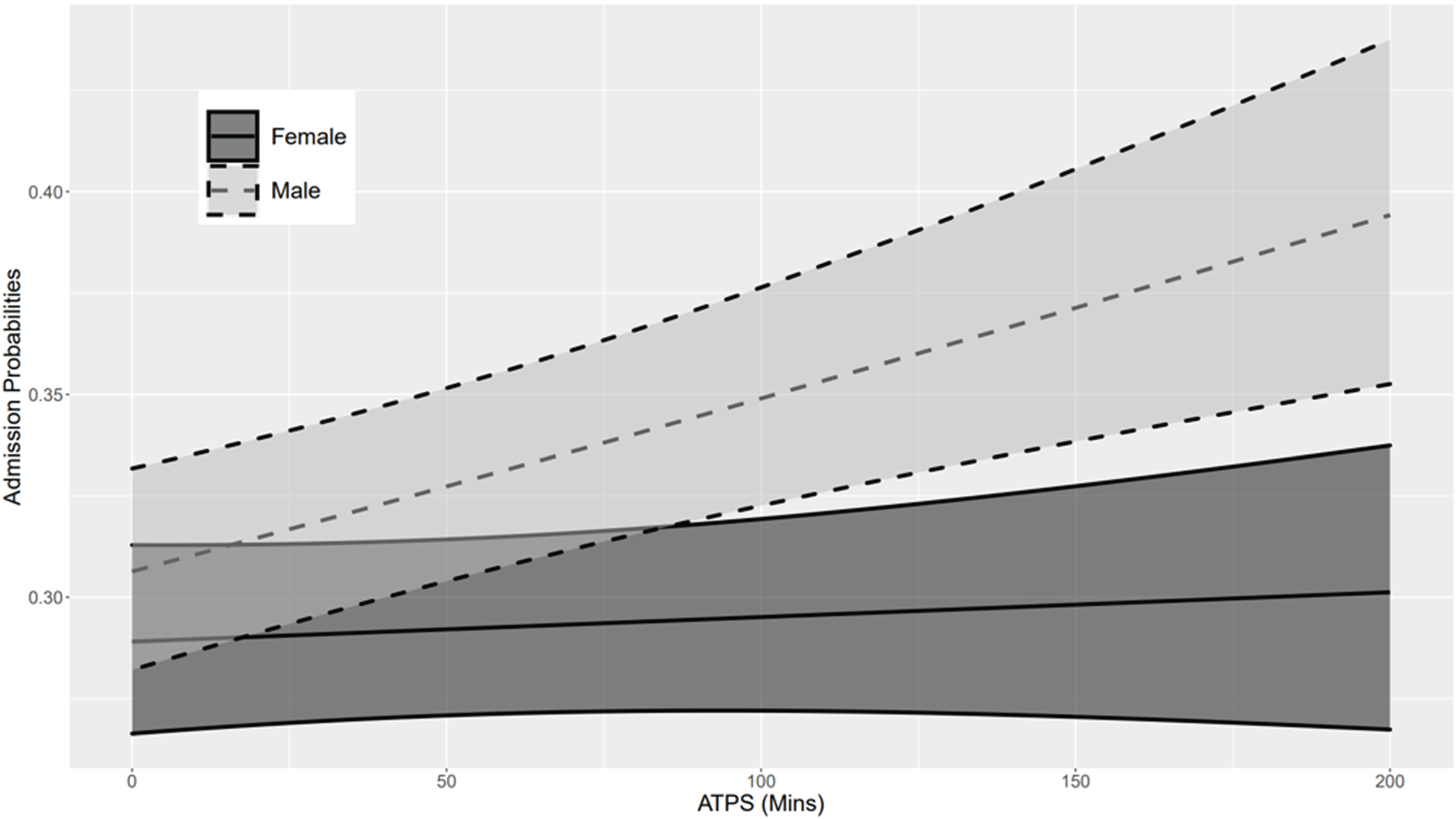
Interaction effect of sex and emergency department (ED) crowding.
Logistic regression results for variables of interest in specification (2a).
When we repeat the same analysis for race and ethnicity using Specifications (2b) and (2c), we find that although the signs of the coefficient estimates agree with the hypothesis that differences in the likelihood of admission are exacerbated when the ED is more crowded, no statistically significant association is found. This may be attributed to the relatively smaller sample size of non-Caucasian and non-Hispanic patients in our study. However, it is also possible that there are no interaction effects between crowding and either with race or ethnicity. Details of this analysis can be found in EC.1 of the Online Supplemental material.
To ensure that the levels of significance and the signs of the regression coefficients are not sensitive to the choice of control variables included in the model, we also carried out additional analysis in which we removed the control variables one at a time from Specification (1) and Specification (2a) and examined whether our results would be fundamentally different. As we explain in detail in EC.5, while the estimated values of the coefficients are different as expected, our conclusions regarding the statistical significance and hence our main findings and insights remain the same.
Consistent with prior research, we find disparities in ED disposition with respect to sex, race, and ethnicity after adjusting for age, clinical characteristics, and ED operational conditions. The presence of disparities in disposition decisions is noteworthy not only because of their potentially long-term effects on patients’ health, but also because unlike some of the other decisions made in the ED such as triage, they are typically made under relatively less time pressure with deliberation and input from multiple individuals, conditions that are known to make biases less likely. To be clear, we refrain from making any causal claims in this essay. In particular, we do not claim that disparities largely result from implicit biases in disposition decisions. Yet, we acknowledge that such a connection is likely and we believe that it is important for future work to investigate this question in more detail either with the help of a richer data set or experiments within a controlled environment.
If indeed the disparities we observe are a direct result of implicit biases, the fact that they are present even when conditions are not too stressful and permit making informed decisions points to how persistent such biases can be and the difficulty of addressing them. However, it is important to keep in mind that, at least in the academic ED where our data came from, disposition decisions are typically the result of input from multiple individuals, and the fact that decisions are made typically at the end of a long process does not necessarily mean that each individual who provides input into the disposition decision has time for deliberation.
Our work points to many interesting and important research directions in addition to the question of causality discussed above. One of the closely related questions that is worth pursuing in future research is a deeper investigation of disparities with respect to patients’ socioeconomic status. Many papers in the literature investigated disparities with respect to patients’ insurance status (see, e.g., Selassie et al. 2003, 2004, Sacks et al. 2011, Arroyo et al. 2012) and one can potentially view insurance status as a proxy for patients’ socioeconomic status. However, it is important to note that, it would be an imperfect proxy at best. Insurance status of the patient might bias decisions in different ways. For example, a decision of discharge as opposed to admission could partially be a result of a desire to protect the patient from a financial burden (if a discharge decision is deemed safe) and not any potential bias against patients of a certain socioeconomic group. Therefore, a delicate approach is needed to tease out the various ways insurance status might be impacting disposition decisions and reach conclusions based on socioeconomic status alone.
A potentially more impactful direction would be investigating and developing methods for alleviating disparities. Many institutions are aware of the presence of disparities and implicit biases, and provide training for their employees. However, to improve the effectiveness of such training, it can be helpful to develop new tools based on research in the area the trainee works in. For example, it would be ideal for a triage nurse or ED physician to get training using a tool that is specifically designed for ED healthcare workers. One untapped resource in developing such tools is simulation. Developing and validating a simulation environment where trainees are presented with randomly generated patient scenarios under realistic but simulated ED conditions and then provided with an assessment of their performances could be helpful in not only battling disparities but more broadly reducing decision errors in the ED. As part of such a simulation environment, it might be interesting to consider providing the trainee suggestions from a support tool, which is trained to provide “debiased” decisions and investigate in what way adoption of such tools would impact actual decisions made. It is also tempting to entertain the possibility of the use of such tools in practice. The real challenge is not the development of such debiasing methods as there have been significant developments in this area (see, e.g., Bellamy et al. 2019 and Mehrabi et al. 2021), but having such a tool thoroughly validated in practice and equally importantly gained acceptance by the emergency medicine community. While this seems like a long way from where we are today, given the increasingly rapid adoption of artificial intelligence tools, it may not be as distant.
Still, perhaps a more realistic goal in the short term could be to develop systems that will intervene by alerting healthcare providers and decision makers real time to the presence of conditions that have the potential to exacerbate disparities. Targeted evidence-based interventions to reduce disparities in clinical decision-making have shown promising initial results. However, such interventions are resource-intensive, and have so far largely been considered outside of the ED environment, such as specialty-specific outpatient clinic settings (see, e.g., Carter et al. 2020, Cykert et al. 2019, 2020, Pérez-Stable et al. 2019). More research is needed to understand the feasibility and potential benefits of employing such mechanisms in the ED.
One important and novel finding in this essay is that crowding might exacerbate sex disparities in disposition decisions. Even though all patients are more likely to be admitted when there is more crowding in the ED, the effect on the admission probabilities for male patients is much stronger. If implicit biases are the main culprit behind disparities, this observation would be in line with what we have already alluded above and is well-known in the literature on psychology and decision making: Increase in cognitive load strengthens implicit biases. This would also point to an interesting connection between EDs’ operational performance and disparities, and highlights the importance of the study of ED operations from the perspective of health disparities as well. From a practical standpoint, several implications of this finding are worth highlighting. First, key capacity-related decisions such as staffing levels should not be made only in consideration of standard operational performance measures like average length-of-stay, percentage who left without being seen etc. Implications of disparities should also be taken into account. Second, in connection with this, EDs should work on developing and directly tracking measures related to disparities. This is also in complete agreement with one of the recommendations of a workgroup convened by the American College of Emergency Physicians for addressing racial/ethnic disparities in emergency care (see Khidir et al. (2023)). Reporting standard operational measures at different racial/ethnic/gender categories might be a start, but statistical methods can be developed to properly measure existing disparities so that they can be included in the electronic healthcare record systems. Finally, any new system developed to alert ED managers and staff to the presence of conditions that exacerbate disparities should also include crowding as one of the contributing factors. More research will be needed to determine precisely what levels of crowding would be concerning.
Putting our findings together with some of the previously published results in the healthcare operations management literature, we can get a better picture of the detrimental effects of ED crowding on health outcomes and equity. We have long known that increased levels of workload negatively impact the quality of service provided to the patients and crowding is directly associated with poor health outcomes in EDs (see, e.g., Kc and Terwiesch (2009)). However, our results add another layer to this discussion pointing to how the impact of crowding might actually be larger than what we might initially think. First, as we already discussed in detail above, higher crowding levels in the ED might be contributing to disparities with respect to race, ethnicity, gender etc. (While we found statistical significance for gender only, more research is needed to comfortably rule out the existence of such a relationship with respect to race and ethnicity.) Second, we provided further support to the already identified relationship between crowding and hospital admission rate: the likelihood of admission is higher when the ED is more crowded. This suggests that crowding in the ED leads to higher occupancy in the main hospital not only simply as a direct consequence of increased patient demand, but also because of the impact crowding has on disposition decisions in the ED. This is concerning because prior work in the operations literature identified the close relationship between hospital occupancy level (see, e.g., Kuntz et al. (2015)) and medical errors and thus crowding in the ED is possibly contributing to errors in the main hospital as well. Finally, while our analysis points to crowding as a potential contributor to disparities in ED decisions, it would also be reasonable to suspect a similar relationship between hospital occupancy level and some of the important decisions (e.g., discharge) in the main hospital, which would suggest that ED crowding could be playing an indirect role in disparities in the main hospital. Clearly, however, research is needed to investigate whether these hypotheses can be substantiated.
Supplemental Material
sj-pdf-1-pao-10.1177_10591478241235000 - Supplemental material for An Investigation into Demographic Disparities in Emergency Department Disposition Decisions
Supplemental material, sj-pdf-1-pao-10.1177_10591478241235000 for An Investigation into Demographic Disparities in Emergency Department Disposition Decisions by Qian Cheng, Nilay T Argon, Christopher S Evans, Peter Lin, Benjamin Linthicum, Yufeng Liu, Abhishek Mehrotra, Mehul D Patel and Serhan Ziya in Production and Operations Management
Footnotes
Acknowledgments
The authors are thankful to the referees, the senior editor, and the co-editors of the special issue for their constructive comments, which helped improve this essay.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Agency for Healthcare Research and Quality through Grant Award Number R03HS029078. Data assistance from the NC Translational and Clinical Sciences (NC TraCS) Institute, which is supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number UL1TR002489.
How to cite this article
Cheng Q, Argon NT, Evans CS, Lin P, Linthicum B, Liu Y, Mehrotra A, Patel MD and Ziya S (2024) An Investigation into Demographic Disparities in Emergency Department Disposition Decisions. Production and Operations Management 34(4): 688–696.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.