
Abstract
We theorize how the nested-ness and knotted-ness of a pragmatic paradox shapes the experience of ensuing tensions. Our theorization draws on a qualitative, abductive study of essential workers (midwives) who were forced to accept contradictory work demands during COVID-19 lockdowns. Midwives experienced these demands as performing tensions stemming from an interconnected need to both protect wellbeing and risk wellbeing in their professional roles. In turn, midwives’ performing tensions were knotted with belonging tensions and nested within organizing tensions faced by societal leaders. Surprisingly, we found that although most midwives experienced contradictory and unrefusable demands as a disempowering pragmatic paradox, some experienced the same demands as a motivating duty. The crux was how midwives interpreted the alignment between knotted performing and belonging tensions. Our research provides a more nuanced view of how workers “live through” pragmatic paradoxes and offers insights into the complex interplay between power asymmetries and multi-level, interwoven paradoxes.
In times of crisis, societal and organizational leaders frequently impose demands on subordinate members that restrict members’ agency (Quarantelli, 1988). The need to accept these demands may be framed as part of a societal or organizational duty—that is, a moral or legal obligation to act in the interests of a greater good (Hannah et al., 2014). For example, during the early stages of the COVID-19 pandemic, millions of individuals worldwide accepted the obligation to socially isolate and work from home as part of a societal duty to limit viral transmission and protect public health (Pradies et al., 2021). But what happens when the agency-limiting demands of a duty are perceived as impossible to fulfill because they involve inherent contradictions? For instance, what happens when healthcare workers’ duties require them to protect public health and risk public health simultaneously? That, in brief, is the empirical puzzle we address in the present paper.
In addressing this puzzle, we advance scholars’ theoretical understanding of how workers experience pragmatic paradoxes. Pragmatic paradoxes are interdependent and contradictory demands that cannot be refused or navigated due to a lack of agency (Cunha et al., 2023). Scholarly interest in pragmatic paradoxes has recently grown due to their perceived potential to elucidate how power relations shape the experience of paradox (Berti & Simpson, 2021a). Proponents of paradox theory generally view paradoxes as persistent, contradictory, and interdependent tensions that can become sources of creative energy when accepted and embraced (Lewis & Smith, 2022). However, as multiple authors have noted (e.g., Berti & Simpson, 2021a; Cunha & Putnam, 2019; Fairhurst et al., 2016; Schad et al., 2016), most paradox scholarship is agnostic toward the ways in which power disparities restrict individuals’ agency in responding to tensions. Therefore, pragmatic paradoxes are theoretically interesting because they highlight a dark side to organizational paradox driven by power dynamics (Berti & Simpson, 2021a).
One aspect of pragmatic paradoxes that researchers have yet to explore is their potential “nested-ness” and “knotted-ness.” Nested paradoxes are those that manifest in tensions at multiples levels of analysis; for example, a paradox might entail tensions at the individual, group, and organizational levels (Jarzabkowski et al., 2013). Knotted paradoxes are those in which tensions stemming from multiple paradoxes are entangled, reducing actors’ ability to navigate one set of tensions without simultaneously addressing the others (Sheep et al., 2017). Although some studies suggest contradictory requirements can be embedded in multi-level paradoxes (e.g., Jarzabkowski et al., 2013), scant (if any) empirical research has explicitly examined (a) how the tensions associated with pragmatic paradoxes can be nested and knotted with tensions from other paradoxes or (b) how the nested-ness and knotted-ness of pragmatic paradoxes influence the subjective experience of them. This lack of attention is unfortunate because it limits scholars’ understanding of how pragmatic paradoxes arise in the context of complex organizational and societal systems (Jarzabkowski et al., 2022; Schad & Bansal, 2018; Sharma et al., 2021). Moreover, it represents a missed opportunity to explore how power dynamics interact with layered and interwoven tensions to shape the experience of paradox (Fairhurst et al., 2016).
The aim of this paper is to examine how the nested-ness and knotted-ness of a pragmatic paradox influenced the subjective experience of ensuing tensions. We address this aim through a qualitative, abductive study of healthcare professionals (midwives) who were essential workers during the COVID-19 pandemic in New Zealand (NZ). These midwives were contractually obligated to continue hands-on, face-to-face work in hospitals and communities throughout nationwide lockdowns. Because this obligation entailed a high risk of viral contagion, midwives faced a range of contradictory demands in performing their daily work tasks. For example, midwives were required to care for their clients while risking their clients’ wellbeing through viral exposure; they were required to uphold public wellbeing by providing ongoing maternity care while also risking themselves and their families (other members of the public) through exposure to COVID-19. Thus, midwives experienced a pragmatic paradox because they were forced to accept contradictory and interdependent work demands in performing their professional roles. Importantly, the performing tensions midwives experienced as a consequence of this paradox became knotted with belonging tensions stemming from their identities as members of the midwifery profession and NZ society. In turn, these performing–belonging tensions were nested within organizing tensions that NZ's societal leaders faced in attempting to protect both public and healthcare providers’ wellbeing as the pandemic unfolded. We explore midwives’ experiences of these knotted and nested tensions and, taking an abductive approach to analysis, theorize how midwives’ interpretations of the alignment between tensions influenced their psychological responses to the pragmatic paradox they faced.
Our work advances organizational paradox scholarship in three main ways. First, by showing how the tensions of a pragmatic paradox can be nested and knotted with other tensions, we provide a more nuanced perspective on the subjective experience of the phenomenon. Despite increasing interest in pragmatic paradoxes (Berti & Cunha, 2023; Berti & Simpson, 2021a, 2021b; Cunha et al., 2023; Li, 2021), little is known from empirical research about how individuals “live through” them. Prior conceptual research portrays pragmatic paradoxes as predominantly negative and disempowering—phenomena that ought to be eradicated from organizations because they are symptomatic of systemic and agentic power disparities (Berti & Simpson, 2021a; Cunha et al., 2023). However, our abductive discoveries raise the possibility that, under certain conditions, pragmatic paradoxes can be interpreted and experienced positively.
Second, and relatedly, we enhance understanding of pragmatic paradoxes as contextually situated phenomena shaped not only by imbalanced power relations but by the perceived legitimacy of the power relations underpinning them. The concept of duty is central to our theorization of how contradictory demands imposed on workers can be perceived as legitimate expressions of power asymmetries. We show that when agency-limiting, contradictory demands are framed as duties, they are more likely to be interpreted as positive and motivating. The crux is (a) how and why the duty is imposed on workers by leaders and (b) whether the duty enhances or undermines workers’ sense of belonging to the collective on behalf of which the duty is issued.
Third, we deepen understanding of nested and knotted paradoxes by exploring their interrelationship with power dynamics, thus connecting two growing areas of interest in paradox scholarship (Berti & Simpson, 2021a; Cunha et al., 2023; Fairhurst et al., 2016; Keller et al., 2021; Sharma et al., 2021). We reveal that when one set of tensions (e.g., performing and/or belonging tensions) is nested within a set of “higher-level” tensions (e.g., organizing tensions), power relations shape the experience of paradox at the lower level in important ways. Specifically, our data illustrate how an asymmetrical power balance between societal leaders and essential workers shaped the framing and interpretation of contradictory demands by lower-level actors, influencing their subjective experience of demands. We also show that when pragmatic paradoxes are knotted with other tensions, and when power relations limit actors’ ability to oscillate between poles of the “pragmatic” tension, actors are likely to shift toward the extreme pole of the interrelated tension, creating a polarized response.
Theoretical Motivation
The theoretical motivation of our paper is two-fold. First, we seek to understand how pragmatic paradoxes can be nested and knotted with tensions stemming from other paradoxes. Second, we seek to theorize how the nested-ness and knotted-ness of pragmatic paradoxes influences the subjective experience of them. Accordingly, we start by reviewing prior research on pragmatic paradoxes and on nested and knotted paradoxical tensions. We then introduce the concept of duties as agency-limiting demands that are related to both performing and belonging.
Pragmatic Paradoxes
The concept of pragmatic paradox originally surfaced in philosophy (O’Connor, 1948) and has subsequently been utilized in disciplines including communication studies and family therapy (Watzlawick et al., 2011). However, pragmatic paradoxes have come to the attention of contemporary organizational researchers thanks largely to efforts by scholars seeking to promote a more critical perspective on organizational paradox theory (Berti & Cunha, 2023; Berti & Simpson, 2021a, 2021b; Cunha et al., 2023). A key aim of this critical perspective is to elucidate the role of power relations in shaping the experience of paradox (Cunha & Putnam, 2019; Fairhurst et al., 2016). Pragmatic paradoxes are central to this aim because of their relationship with power dynamics (Berti & Simpson, 2021a).
Definitions of pragmatic paradox vary in their emphasis according to discipline. Although philosophers typically treat pragmatic paradoxes as intellectual puzzles revealing logical glitches in the interpretation of language (Martinich, 1983; O’Connor, 1948), organizational scholars view them more as contradictory demands embedded in intense social relationships (Berti & Simpson, 2021a, 2021b; Cunha et al., 2023). For example, Berti and Simpson (2021a, p. 256) cite Watzlawick et al.'s (2011) description of a pragmatic paradox as an “an order ‘that must be disobeyed to be obeyed.’” As their use of the word “order” implies, pragmatic paradoxes are often imposed on subordinates by superiors, as when a manager commands a subordinate to “act spontaneously” (Cunha et al., 2023, p. 454). A subordinate receiving this order is stuck between a rock and a hard place. If they attempt to act spontaneously, they will not be acting spontaneously because they will be following the order. Moreover, the subordinate lacks the legitimate social power (and, therefore, agency) to question the order through metacommunication (i.e., communication about the act of communicating) (Alvesson & Spicer, 2012; Berti & Simpson, 2021a). The subordinate is thus left with no legitimate course of action, paralyzed by the pragmatic paradox (Cunha et al., 2023). Although this example suggests pragmatic paradoxes are more likely to affect individuals nearer the bottom of organizational hierarchies, those higher up (e.g., managers, executives) are not immune to them (Berti & Simpson, 2021a). Nor are pragmatic paradoxes necessarily encapsulated in contradictory verbal directives; some arise from inequitable resource constraints and/or normative pressures embedded in actors’ unique social situations and identities (Berti & Simpson, 2021b; Cunha et al., 2023; Padavic et al., 2020). To accommodate these varied manifestations of the phenomenon, we define pragmatic paradoxes as contradictory and interdependent demands that, in the context of a social relationship, are implicitly or explicitly imposed on actors who lack the agency to refuse or navigate the demands.
Most existing research on organizational pragmatic paradoxes has focused on underlying power asymmetries (Berti & Simpson, 2021a; Cunha et al., 2023). Drawing on Fleming and Spicer's (2014) typology, Berti and Simpson (2021a) identify four dimensions of organizational power that give rise to various manifestations of pragmatic paradox. Coercion is an explicit form of agentic power that produces paradoxical “double binds”; double binds create “damned if you do, damned if you don’t” scenarios, as when a manager issues a contradictory verbal directive. Manipulation is an implicit form of agentic power that engenders “paradoxical predictions.” For instance, managerial communications might imply that following “best practices” will result in successful innovations, lulling employees into a sense of complacency that inhibits their ability to innovate successfully. Domination is an explicit form of systemic power that creates Kafkaesque organizations, forcing workers into Catch-22 situations. An example would be the situation of contract workers who must prove themselves as project leaders if they want to secure a permanent position, yet lack the formal right to lead projects due to their status as non-permanent employees. Subjectification is an implicit form of systemic power that leads to paradoxical “doublethink”; doublethink occurs when hidden power structures (such as dominant discourses and logics) shape individuals’ sense of self so deeply that individuals take contradictory demands for granted. For example, women might blame themselves for their inability to be both devoted mothers and dedicated workers (Padavic et al., 2020), despite this contradictory demand stemming from social structures beyond their control (Mharapara et al., 2023).
Berti and Simpson's (2021a) conceptual arguments, which have been echoed elsewhere in the literature (Cunha et al., 2023), provide valuable insights into (a) how and why social actors experience pragmatic paradoxes and (b) why redressing pragmatic paradoxes generally requires system-level remedial actions. However, an important aspect of pragmatic paradoxes not explicitly addressed in prior research is their potential nested-ness and knotted-ness. If pragmatic paradoxes are often imposed on social actors by those with higher levels of social power (Cunha et al., 2023), it might be because those in power are struggling with their own contradictory demands and goals. For example, organizational leaders might impose contradictory requirements on rank-and-file employees in response to conflicts between shareholder and regulatory demands (Jarzabkowski et al., 2013). Moreover, the contradictory demands of a single pragmatic paradox may be knotted with tensions stemming from other, related paradoxes. To illustrate, tensions stemming from the need to perform contradictory roles might be entangled with tensions stemming from the need to maintain conflicting identities (Cuganesan, 2017; Lüscher & Lewis, 2008). Part of the reason little is known about the nested-ness and knotted-ness of pragmatic paradoxes is that researchers have conducted scant (if any) empirical research on individuals’ subjective experiences of the phenomenon. Thus, we propose to advance knowledge by empirically examining how workers experienced a nested and knotted pragmatic paradox during COVID-19 lockdowns.
Nested and Knotted Paradoxical Tensions
Nested and knotted tensions reveal the inherent complexity and interconnectedness of paradoxes (Jarzabkowski et al., 2013, 2022; Keller & Sadler-Smith, 2019; Schad & Bansal, 2018; Sheep et al., 2017). To understand nested and knotted paradoxes, we must first define and categorize paradoxes at a more basic level. Organizational researchers generally conceptualize paradoxes as persistent contradictions between interdependent elements (Schad et al., 2016). Most typologies of paradox agree on four main varieties (Lewis & Smith, 2022; Smith & Lewis, 2011). Paradoxes of organizing involve tensions arising from the inherent challenges of coordinating multiple parts of a whole (Smith & Lewis, 2011); specific tensions include integration–differentiation (Tuckermann, 2019) and control-flexibility (Clegg et al., 2002). Paradoxes of performing entail conflicts between multiple roles, expectations, and/or objectives; for example, supervisors of self-managing teams might be expected to be in charge while simultaneously letting others take charge (Lüscher & Lewis, 2008). Paradoxes of belonging arise from conflicting identities (Sheep, in Sharma et al., 2021); they are likely to affect individuals who belong to multiple social groups with distinct value systems (Lüscher & Lewis, 2008) or whose work and non-work selves are inconsistent (Padavic et al., 2020). Finally, paradoxes of learning stem from the need to preserve existing knowledge, processes, and other elements while simultaneously dismantling such elements to make way for future versions (Smith & Lewis, 2011).
The concept of nested paradoxes adds another layer of complexity to this typology. Nested paradoxical tensions are those that surface across multiple levels of analysis—for example, the individual, group, project, organizational, and/or societal levels (Jarzabkowski et al., 2013; Keller et al., 2021; Keller & Sadler-Smith, 2019; Smith & Lewis, 2011). Authors have used various forms of linguistic imagery to capture the notion of nested paradoxes. Smith and Lewis (2011, p. 384) describe them as “cascading across levels”; Keller et al. (2021, p. 169) liken them to “nesting dolls or series of waves”; and Fairhurst et al. (2016, p. 7) refer to “layered tensions.” Whatever the metaphor, the idea is that when social actors experience paradoxical tensions at one level (e.g., the individual or group level), those tensions may be nested within tensions at a wider level (e.g., the organizational or societal level). The “wider” tensions in a nested paradox can be salient and visible to actors, or latent and invisible (Schad & Bansal, 2018). Research shows that actors’ responses to tensions at one level have flow-on effects for the experience of tensions at other levels (Jarzabkowski et al., 2013).
Knotted paradoxes involve entanglements of interrelated tensions (Jarzabkowski et al., 2022; Sheep et al., 2017). Tensional knots can occur within or between different types of paradox (Fairhurst et al., 2016). For example, Sheep (in Sharma et al., 2021) describes how a belonging tension that became salient during the COVID-19 pandemic (opener/economic vs. restrictor/health) was knotted with multiple tensions pertaining to individuals’ self-categorizations within broader social and demographic groupings (e.g., age, class, and/or political orientation). Meanwhile, Lüscher and Lewis (2008), writing before the term paradoxical “knots” was coined, revealed interrelatedness between performing and belonging tensions that were experienced by managers during organizational change. As such, they highlighted the importance of understanding how distinct types of tensions become interwoven in subjective experience (Fairhurst et al., 2016). Recent research shows that knots between distinct tensions and types of tensions are socially constructed through discursive and interactional processes (Jarzabkowski et al., 2022; Sheep et al., 2017; Sheep, in Sharma et al., 2021). Studies also suggest that interconnected tensions are constantly knotting, unraveling, and reknotting through dynamic processes that may enable dynamic equilibrium over the long term (Jarzabkowski et al., 2022). In sum, prior research reveals that knotted paradoxes are dynamic social constructs that (potentially) support the navigation of tensions. However, no studies we are aware of have explicitly addressed (a) how knotted paradoxes relate to pragmatic paradoxes in which power and agency limit the possibilities for navigating interrelated tensions; or (b) how the nested-ness of knotted paradoxes influences subjective responses to them.
Duties as Agency-Limiting Demands
Duties are moral or legal obligations toward the other members of a collective, the goals of a collective, or the rules and norms of a collective (Hannah et al., 2014). Duties can shape and constrain how individuals exercise their agency in two ways. First, duties can prevent individuals from undertaking actions that could harm collective welfare (Folger et al., 2013). For instance, a duty toward the other members of society prevented individuals from violating social distancing rules during COVID-19 lockdowns. Second, duties can compel individuals to act in ways they might not otherwise choose to act (Folger et al., 2013). To illustrate, some individuals were compelled by a societal duty to get vaccinated against COVID-19, despite reservations about the vaccine's safety and/or efficacy (Wakefield & Khauser, 2021).
Duties can be experienced individually or collectively (Collins, 2013). An individual organizational member can feel compelled by a duty that other members do not feel, as when organizational whistleblowers speak out in the interests of their wider society (Culiberg & Mihelič, 2017). Multiple individuals can also be compelled by the same duty simultaneously, as when millions of people socially isolated to prevent the spread of COVID-19. Whether experienced individually or collectively, all duties are inherently embedded in a relationship between individuals and a collective (Folger et al., 2013). By collective, we refer to any entity comprised of more than one individual. Thus, if a healthcare provider feels a duty toward a single patient, that duty is embedded in a dyadic relationship (a collective comprised of two individuals). If the members of a sports team feel a duty to always perform to their highest ability, their duty is embedded in their relationship with the team. The same applies when individual members of organizations, professions, and societies feel a duty toward their respective collectives.
This aspect of duties implies that they are inherently linked to individuals’ sense of collective belonging—to their social identities (Ashforth & Mael, 1989). When individuals “willingly” perform in ways consistent with a duty (whether through acts of commission or omission), it may be because their sense of social belonging and identification overrides their will to ignore or defy the duty (Wakefield & Khauser, 2021). Conversely, when individuals submit to a duty not willingly but because they fear the consequences of non-compliance, it could be that they do not identify strongly enough with the collective on behalf of which the duty is issued. Therefore, given that some duties entail contradictory demands (Folger et al., 2013), we draw on the concept of duty to understand how individuals interpret and respond to performing–belonging tensions associated with a pragmatic paradox.
Research Design and Methods
Our study implemented a qualitative, abductive research design. Qualitative data were appropriate for revealing the contextually situated experiences of our research participants (Gephart, 2004), while abductive analysis enabled us to generate novel theory based on unexpected findings in our empirical data (Folger & Stein, 2017).
Study Context
Our research context was NZ midwifery during the COVID-19 pandemic. NZ midwifery is part of a fully funded and universally accessible national health system. NZ recognizes the International Confederation of Midwives’ definition of a midwife as “a responsible and accountable professional who works in partnership with women to give the necessary support, care and advice during pregnancy, labor and the postpartum period, to conduct births … and to provide care for the newborn and the infant” (International Confederation of Midwives, 2017, p. 1). NZ's midwifery profession is autonomous from related healthcare professions such as nursing and medicine (Clemons et al., 2021), regulated by the Midwifery Council under the Health Practitioners Competence Assurance Act (New Zealand Parliament, 2003).
NZ midwives work in three distinct but related settings (Midwifery Council of New Zealand, 2021). First, approximately 30% of NZ midwives are self-employed and community-based. These midwives care for most (96%) birthing families in NZ through a case-loading, continuity-of-carer model. Second, ∼50% of midwives are employed in maternity facilities (e.g., hospitals, birthing units) where they provide maternity care on rostered shifts. Third, ∼20% of midwives work in support, educational, regulatory, and specialist roles.
Like other healthcare professionals, NZ midwives had their working lives upturned with the outbreak of the COVID-19 pandemic (Dixon et al., 2023). On March 21, 2020, the NZ government announced a four-level alert system to limit the spread of the virus (New Zealand Government, 2023). Two days later, Prime Minister Jacinda Ardern declared that within 48 hours, NZ would go into a strict, level-4, nationwide lockdown for an indeterminate length of time. Under level-4 lockdown rules, New Zealanders were legally required to stay at home and socially isolate in household “bubbles,” unless going out to fulfill basic needs or to exercise locally. The only individuals exempt from this rule were essential workers who needed to travel to and from their workplaces.
As NZ prepared for lockdown, midwives were informed by the Ministry of Health (via their professional support body) that “midwifery care in both the community and hospital are Essential Services. This means that, at Alert Level 4, midwives can continue to provide maternity care” (New Zealand College of Midwives, 2020, p. 1). The New Zealand College of Midwives (NZCOM) offered guidance to its members on minimizing the risk of contracting and spreading COVID-19 and informed community-based midwives that they “continue[d] to be clinically responsible for the maternity care coordination and provision for the women in their caseload” (New Zealand College of Midwives, 2020, p. 1). Meanwhile, facility-based midwives were informed of their contractual obligations by the District Health Boards (DHBs) they worked under (New Zealand Government, 2023).
Against this background, we decided to conduct a study exploring: (a) midwives’ experiences of safety and wellbeing during COVID-19 lockdowns; (b) how midwives’ close personal contacts (e.g., family and friends) reacted to them being essential workers; and (c) how midwives perceived the public's views on them being essential workers. As our analysis of study data progressed, we identified tensions as a central theme of midwives’ experiences. Accordingly, in line with an abductive approach, we “moved away” from our initial empirical focus (Rinehart, 2021) and increasingly drew on paradox theory to frame our study and inform our theory building.
Participants
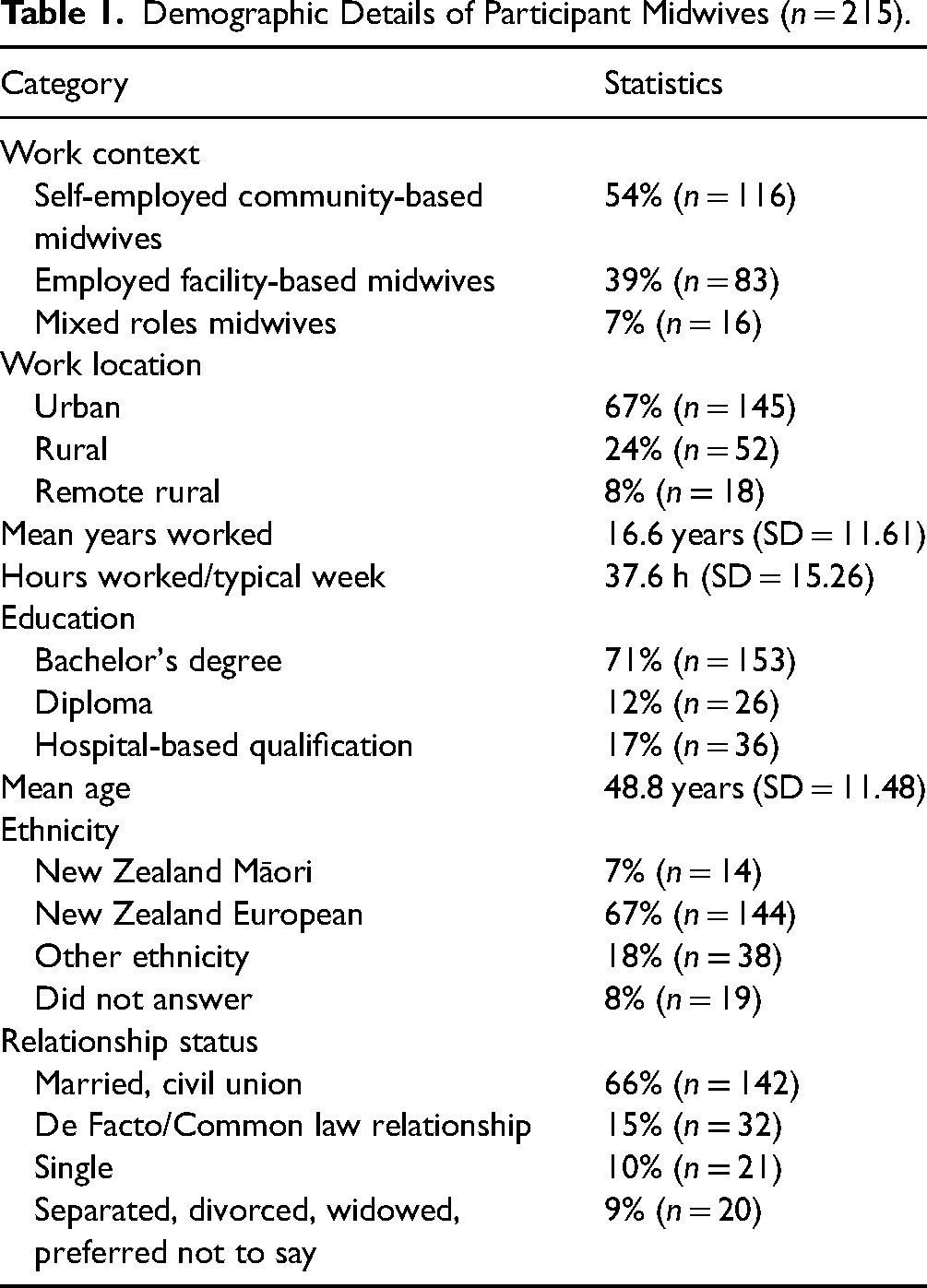
Participant recruitment was facilitated by the research team's professional contacts in NZ midwifery. After receiving approval for the study from our university's ethics committee, we contacted potential participants through NZCOM, whose membership includes approximately 2,230 midwives. NZCOM emailed members who had registered their willingness to receive research invitations. Upon completing the study, participants were offered the opportunity to enroll in a prize draw for 1 of 20 retail vouchers worth $50. We emailed reminders to participants 2 and 4 weeks from the initial invitation to increase the response rate. Table 1 provides basic demographic information about the participants in our sample.
Demographic Details of Participant Midwives (n = 215).
Data Sources
Primary Data
We collected primary data through an online, qualitative survey administered between November 2020 and January 2021. Although less common than interviews in qualitative research, open-ended surveys are increasingly seen as an effective method for collecting rich, qualitative data from a relatively large sample of participants (Braun et al., 2021; Neville et al., 2016; Terry & Braun, 2017). Ethical and practical advantages of qualitative surveys include: (1) ensuring genuine anonymity for participants (Braun et al., 2021); (2) allowing participants to respond in their own time (rather than during a scheduled meeting) (Terry & Braun, 2017); and (3) increasing participants’ comfort to discuss sensitive topics (which might be reduced in face-to-face interview situations) (Neville et al., 2016). In the context of COVID-19 lockdowns, the online delivery of our survey was particularly advantageous because it enabled us to gather real-time data without concerns about spreading or contracting the virus. The survey approach also permitted us to collect qualitative data from a broad cross-section of midwives (n = 215) within a relatively short period. The high number of qualitative responses we received enabled us to identify variance in our sample (regarding midwives’ individual responses to tensions), leading to richer theoretical insights (Locke et al., 2022). The online survey for the present study comprised of five open-ended questions, as presented in Appendix A in the online Supplementary materials.
Secondary Data
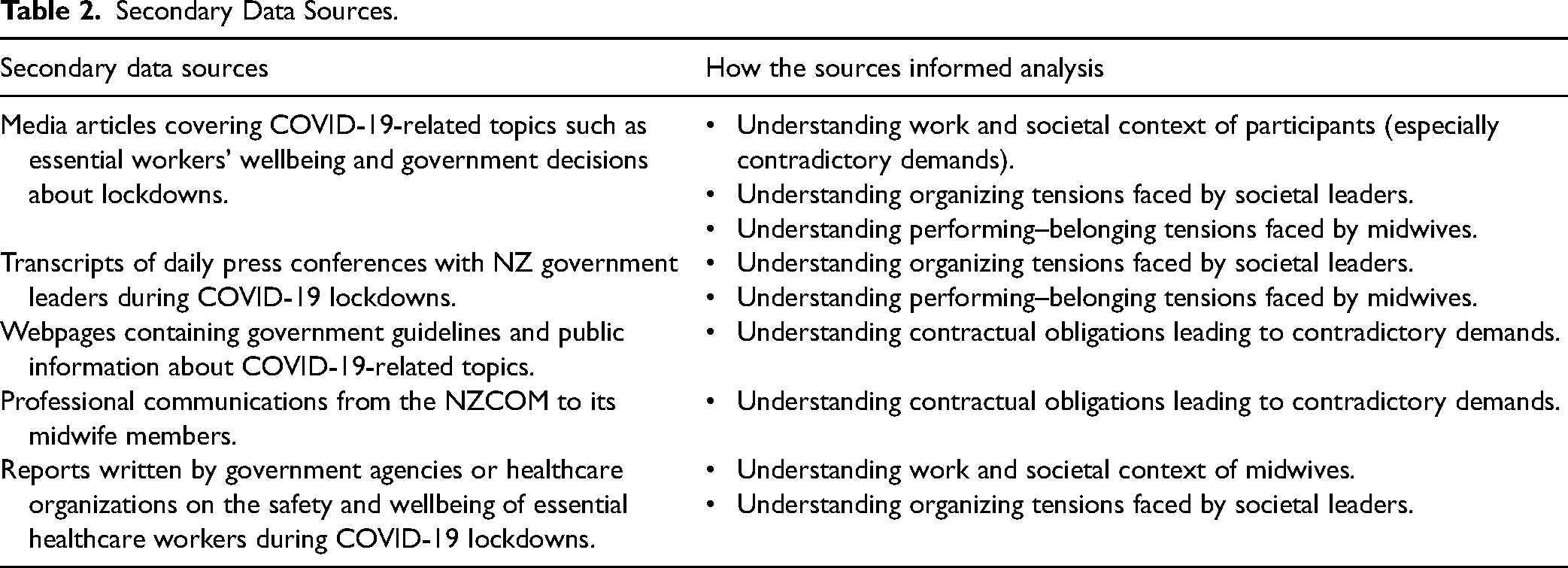
We supplemented our qualitative survey data with secondary data from media articles, government messaging and guidelines, transcripts of daily press conferences with government leaders, communications from professional bodies (especially NZCOM), and government and organizational reports. Table 2 provides an overview of our secondary data sources. Initially, we used these secondary data sources to better understand our participants’ work and societal context. As data analysis progressed, we realized the data were directly relevant to our emerging theoretical insights and we began to code text from secondary data sources in the same way we coded participants’ responses to our qualitative survey. This coding supported our understanding of the nested and knotted tensions experienced by our participants, as shown in Table 2.
Secondary Data Sources.
Data Analysis
We analyzed primary and secondary data using an abductive approach that involved constantly contrasting patterns in our data (emergent theoretical insights) with existing literature and theory (Folger & Stein, 2017). Abduction is akin to a process of discovery whereby researchers make creative inferences to generate novel theoretical insights from unexpected or surprising empirical data (Timmermans & Tavory, 2012). A key feature of abductive reasoning is the notion of “moving away” from an initial focus to facilitate creative theorizing (Rinhehart, 2021). Researchers might start data analysis thinking that their findings will be relevant to theoretical conversation A, yet subsequently recognize that their data have more to contribute to conversation B. Accordingly, while our initial motivation for collecting study data was to understand how working through lockdowns impacted midwives’ wellbeing, we developed a theoretical focus on paradoxical tensions after becoming immersed in the data. We iteratively refined this focus through multiple rounds of data coding, background reading, and theory construction. Refinements of our theoretical focus were primarily driven by (a) our evolving interpretations of what was interesting and surprising about our data when contrasted with prior theory and (b) reviewer feedback regarding the potential theoretical contributions of our study. Because this multi-round process was highly iterative and complex, we describe a simplified version highlighting the unexpected discoveries that drove our theorizing.
Step 1: Identifying Performing Tensions Experienced by Midwives
Our first unexpected discovery was that performing tensions were a central theme in midwives’ experiences of working through lockdowns. We made this discovery during the analytic stage of data familiarization and open coding (Charmaz, 2006). To make sense of midwives’ experiences, we started by reading through all participants’ responses to our qualitative survey and making memos about potential themes. All four authors participated in this step. The first author then conducted line-by-line, open coding of the full dataset to get a sense of how well those themes were represented in participants’ statements. At this stage, and following standard approaches to open coding (Charmaz, 2006), our analysis was guided not by an a priori theoretical framework but by the empirically grounded research questions: (1) How did working through lockdowns impact midwives’ safety and wellbeing? (2) How did relational and societal factors influence midwives’ experiences of working through lockdowns? We worked iteratively between memos and open codes until we identified a central theme—tensions—that would potentially give theoretical coherence to our early interpretations of empirical data.
We pursued this theme further through immersion in relevant literature. The theme of tensions suggested our research could be relevant to paradox theory, which focusses on tensions that are persistent, contradictory, and interdependent (Lewis & Smith, 2022). The tensions we initially identified in midwives’ experiences were linked to their performance of conflicting roles during the pandemic. For example, midwives described conflicts between their work and home roles, as in the following quote: “I felt some resentment that my job caring for others meant I couldn't see or care for my mother.” Accordingly, we drew from the paradox literature the idea that midwives had experienced performing tensions while working through lockdowns (Jarzabkowski et al., 2013; Lüscher & Lewis, 2008). Further analysis aimed to identify why midwives experienced performing tensions.
Step 2: Linking Performing Tensions to a Societal-Level Paradox
Our second discovery was that midwives’ experiences of performing tensions were linked to a paradox faced by societal leaders during the pandemic. This societal-level paradox involved an interdependent and contradictory tension between the wellbeing of healthcare recipients (the public) and the wellbeing of healthcare providers. As COVID-19 entered NZ, the public needed healthcare services to protect their wellbeing (i.e., their COVID-related and ongoing healthcare needs). Yet, to provide such services, healthcare workers were obligated to risk their own wellbeing by potentially exposing themselves to COVID-19 at work (Fenton, 2020).
We identified this tension by analyzing secondary data to better understand our participants’ work and societal context. For example, we read “communications” that midwives received from their professional support body following the government's announcement of nationwide lockdowns. We also read government guidelines, media articles, and press conference transcripts that were relevant to midwives’ experiences as members of the essential workforce (see Table 2). As our understanding of midwives’ work and societal context deepened, we realized that their experiences of performing tensions were embedded within organizing tensions that societal leaders faced in responding to the material conditions of the pandemic. Thus, drawing on additional ideas from the paradox literature (e.g., Jarzabkowski et al., 2013), we inferred that midwives’ performing tensions were “nested” within a broader, societal-level paradox.
Step 3: Identifying a Pragmatic Paradox Underpinning Midwives’ Experiences of Performing Tensions
Our third discovery was that midwives’ experiences of nested performing tensions were underpinned by a pragmatic paradox—specifically, the legal obligation to accept contradictory demands as part of a professional role. We identified this pragmatic paradox by integrating primary data relating to midwives’ experiences of performing tensions (see step 1) with secondary data relating to the societal paradox surrounding those tensions (see step 2). Through focused coding of primary data (Charmaz, 2006), we deepened our understanding of the performing tensions experienced by midwives. These tensions were characterized by perceived contradictions between the demands imposed on midwives and the objectives informing those demands. For example, midwives’ roles required them to protect maternity clients’ wellbeing through the provision of ongoing care while simultaneously risking clients’ wellbeing through viral exposure. Secondary data, including government announcements and professional communications from NZCOM, confirmed that these contradictory work demands were imposed as a legal/contractual obligation. Thus, midwives experienced the demands as a pragmatic paradox because they lacked the agency to refuse the demands without losing their jobs. Our primary data also suggested that most midwives felt like they lacked the material resources (e.g., personal protective equipment [PPE]) to navigate the contradictory demands effectively.
Notably, because the pragmatic paradox experienced by midwives stemmed from the need to provide in-person maternity care during lockdowns, we subsequently excluded data from midwives who were not required to provide care in face-to-face settings. For instance, we excluded responses from midwives whose roles enabled them to work from home and therefore avoid viral exposure. We also excluded data from a small number of participants who reported feeling entirely safe working through lockdowns, as these midwives perceived their roles as entailing no contradictory demands.
Step 4: Identifying a Range of Subjective Responses to the Pragmatic Paradox and Linking Positive Responses to the Concept of Duty
Our fourth discovery was that midwives’ subjective responses to the pragmatic paradox they lived through were not exclusively negative. We made this discovery by analyzing primary data to understand individual midwives’ subjective responses to the pragmatic paradox. While most midwives reported negative thoughts and feelings regarding their predicament, the content and tone of some responses suggested the midwives felt motivated by the experience. This discovery was surprising given that most research on pragmatic paradoxes portrays them as disempowering and paralyzing (e.g., Berti & Simpson, 2021a; Cunha et al., 2023). Intrigued, we double checked whether the midwives who seemingly felt motivated by working through lockdowns did not perceive their roles as entailing contradictory demands. For example, did midwives who were motivated by demands perceive no risk to themselves, their clients, or their families, suggesting they perceived no contradiction in the demands they faced (and therefore no pragmatic paradox)? Surprisingly, we found that this was not the case; some midwives both perceived their roles as involving contradictory demands and felt motivated by them. For instance, one midwife stated: “I was acutely aware that I did not want to bring the virus into the house but at the same time I felt a duty to my profession and society!” Such quotes suggested that what really distinguished midwives who felt motivated by contradictory demands was not how they perceived the nature of the demands but their framing of the demands as part of a duty.
Step 5: Theorizing Knotted-ness and Nested-ness of Tensions and Linking Perceived Alignment Between Tensions to Subjective Responses
Our final step in analysis was to theorize an explanation for the unexpected discovery made during step 4—namely, that imposed contradictory demands could be motivating when framed as part of a duty. We read into the duty literature (e.g., Folger et al., 2013; Hannah et al., 2014; Wakefield & Khauser, 2021) and found links between duties and social identities and identification (i.e., concepts related to individuals’ sense of collective belonging). This finding from the literature triggered further focused coding and analysis whereby we examined what our primary data said about midwives’ experiences of (a) belonging tensions (which are linked to social identities; Sheep, in Sharma et al., 2021), (b) the links (or “knots”) between belonging and performing tensions (Lüscher & Lewis, 2008; Sheep et al., 2017), and (c) how belonging–performing tensions were nested within and influenced by societal-level organizing tensions (see step 2). We then re-read each individual survey response to check patterns in how midwives’ experiences of nested and knotted tensions influenced their interpretations and experiences of contradictory work demands. Finally, we synthesized the aggregate patterns in our data to develop a theoretical model.
Findings
How does the nested-ness and knotted-ness of a pragmatic paradox influence the subjective experience of ensuing tensions? To summarize our findings regarding this question—which developed as our ultimate theoretical focus through the process of abductive analysis—we developed Figure 1. Starting at the far left, the figure shows that the material conditions of the COVID-19 pandemic gave rise to organizing tensions at the societal level. In turn, societal leaders’ responses to these tensions forced midwives to accept contradictory demands as part of their professional roles, creating a pragmatic paradox. Midwives experienced the pragmatic paradox as a constellation of knotted performing–belonging tensions which, because of their societal-level origins, were nested within wider organizing tensions. As we explain later, this nested-ness meant that midwives’ subjective experiences of contradictory demands were ultimately shaped by their interpretations of the “alignment” between performing tensions and a particularly salient belonging tension. To set the scene for our findings on the nested-ness and knotted-ness of tensions, we start by describing the societal context that gave rise to midwives’ experiences of a pragmatic paradox.
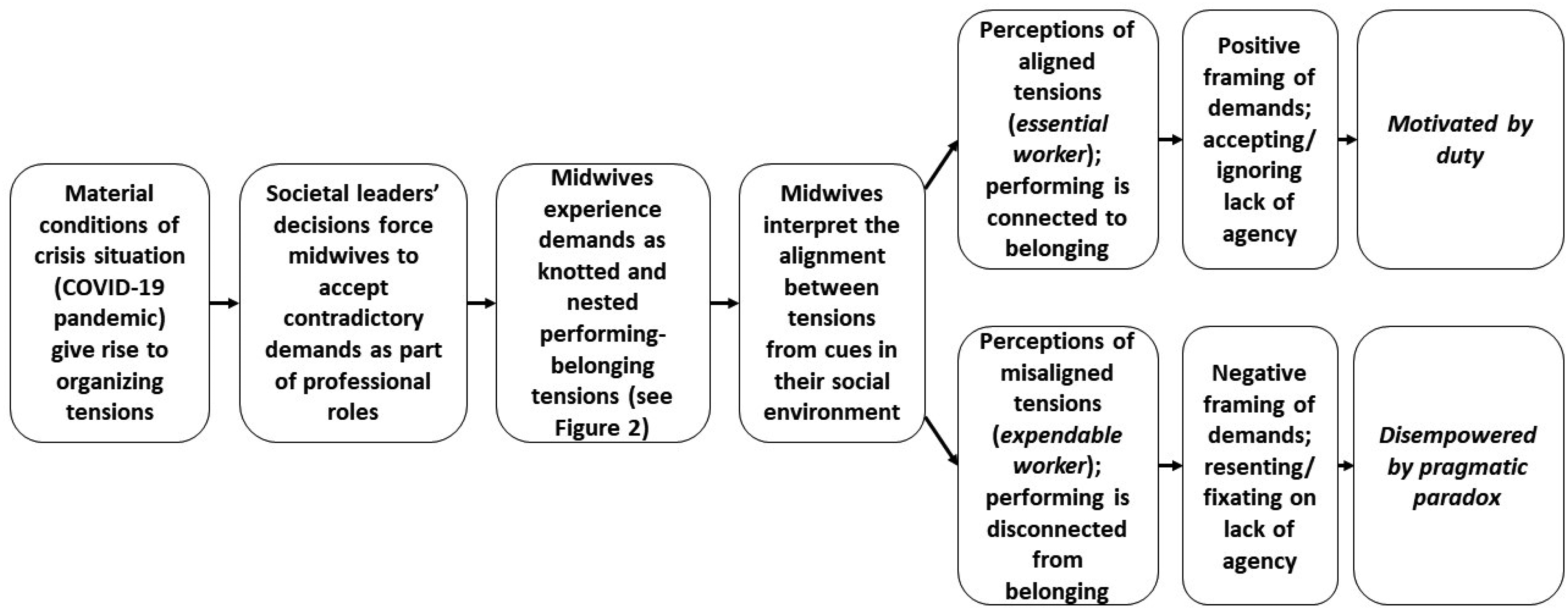
How the Nested-Ness and Knotted-ness of a Pragmatic Paradox Influenced Subjective Experiences of Ensuing Tensions.
COVID-19, the Public-Provider Wellbeing Paradox, and Contradictory Demands on Midwives
The COVID-19 pandemic was an enormous exogenous shock that created and heightened paradoxical tensions at multiple levels (Carmine et al., 2021; Pradies et al., 2021; Sharma et al., 2021). One paradox that emerged early in the pandemic related to tensions between the safety and wellbeing of the public (healthcare recipients) and the safety and wellbeing of healthcare providers (Kniffin et al., 2021; Pradies et al., 2021). As COVID-19 spread across the globe, the public needed healthcare services to protect and uphold their wellbeing. Yet, to provide such services, healthcare workers were obligated to risk their own safety and wellbeing—and potentially that of their family and household members—by exposing themselves to COVID-19 at work (Dhai et al., 2020; Fenton, 2020). We label the ensuing tension the “public-provider wellbeing paradox.”
We categorize the public-provider wellbeing paradox as a societal-level organizing tension for two reasons. First, the tension had to be managed at the societal level, typically by national leaders. The pandemic presented an imminent risk to public health; if not managed properly, it could easily overwhelm a country's health system (Boccia et al., 2020). Therefore, societal members had to cooperate on a mass scale to develop a coherent and cohesive response, and societal leaders generally assumed responsibility for coordinating this response. Second, and relatedly, societal leaders’ responses to the pandemic involved tensions inherent to the act of organizing (Smith & Lewis, 2011). Coordinating an effective response to COVID-19 necessitated organizing society's workforce into different units (essential vs. non-essential workers) to achieve a unified objective (minimizing the pandemic's impact on societal wellbeing). In turn, this created an organizing tension between differentiation and integration (Jarzabkowski et al., 2013); specifically, essential versus non-essential workers experienced different levels of risk (differentiation) as part of an integrated response to confronting the pandemic.
The NZ government's immediate response to COVID-19 was to implement a strict nationwide lockdown and to divide the nation's workforce into essential versus non-essential workers (New Zealand Government, 2023). Non-essential workers were to stay at home and isolate in household bubbles, while essential workers were obligated to continue working outside the home to ensure the public had ongoing access to critical services (New Zealand Parliament, 2020). Midwives were classified as essential workers and informed that they were contractually obligated to continue working through lockdowns. This information came either directly from the NZ healthcare authorities (for midwives employed in facilities) or via midwives’ professional body (which relayed information from the health authorities to community-based midwives) (New Zealand College of Midwives, 2020). For community-based midwives, guidance from the Ministry of Health was that they needed to provide in-person care when appropriate and to conduct consultations virtually whenever feasible (New Zealand College of Midwives, 2020). Midwives also received instructions on how to protect themselves and their clients from the risk of viral contagion using PPE and physical distancing. This guidance indicated that the NZ health authorities were aware of the interdependent need to simultaneously protect healthcare recipients’ wellbeing and midwives’ wellbeing.
However, our primary data reveal that most midwives were forced to practice under socio-material conditions that undermined their ability to protect themselves while also caring for their clients. To start, the nature of their work regularly forced them into close physical contact with their clients, implying that physical distancing and virtual consultations were frequently infeasible (whether in hospitals, birthing centers, or community locations). Next, many midwives work in the community, visiting clients in their homes or local clinics for perinatal consultations that require physical contact. During the pandemic, the healthcare authorities did not organize alternative spaces for such consultations, and many community clinics were closed (Crowther et al., 2021). Consequently, community-based midwives were obligated to visit clients in their homes, sometimes crossing the boundaries of multiple household bubbles in a single workday. Finally, under Ministry of Health guidelines, midwives were instructed to use PPE to minimize the risk of viral contagion during in-person consultations and births. They were also advised that this equipment would be supplied to them by their DHB (the local healthcare authority) (New Zealand College of Midwives, 2020). However, most midwives in our survey (and especially those working in the community) said they had extremely limited, if any, access to PPE provided by the healthcare authorities, with many stating they had to source and fund their own.
These material constraints, which were directly related to midwives’ position in the NZ healthcare system, forced them to accept contradictory yet interdependent work demands. Because midwives could not refuse these demands without losing their jobs and lacked the material and social resources to navigate the demands constructively, they experienced the demands as a pragmatic paradox.
The most immediate tensions midwives experienced from this paradox related to role performance. The objective of midwives’ professional roles was to care for their clients and, in doing so, support clients’ wellbeing. Yet, during the pandemic, fulfilling this role entailed an interdependent contradiction—namely, the risk that midwives could damage their clients’ wellbeing by unknowingly infecting them with COVID-19 while providing in-person care. As one midwife stated: I felt that I was in a very difficult situation. I was connecting with multiple ‘bubbles’ on a daily basis. I was scared that I could be in a position to pass COVID on to vulnerable people. (Community-based Midwife (CBMW) 201) While working in the hospital, I felt completely exposed to the virus. We had to enter and exit through [the] emergency department, which is the place most likely to hold infection, we conducted handover in a confined space, we had no choice but to make contact with every woman requiring assistance in antenatal, birth and postnatal. I felt every day I was exposed and put myself at risk, then brought it all home to my family. Every time I brushed past a bed sheet or comforted a woman in pain, I immediately imagined what this meant for my family. We were not offered masks unless caring for a confirmed positive woman, so I felt less than supported by our DHB [District Health Board]. We did our jobs at risk to ourselves and our families. (Facility-based Midwife (FBMW) 140)
In sum, the performance of midwives’ roles during the pandemic frequently necessitated contradicting the purported objectives of those roles. These contradictions gave rise to performing tensions between “protecting wellbeing” and “risking wellbeing.” As we show in the following subsection, midwives’ responses to these tensions cannot be understood without acknowledging how they were nested and knotted with other tensions.
Midwives Experience Demands as Nested and Knotted Tensions
Our data suggest midwives experienced their pragmatic paradox as a constellation of nested and knotted performing–belonging tensions. Figure 2 depicts how tensions were nested and knotted for midwives. The outer circle in the figure represents the organizing tension faced by societal leaders, which, as noted, stemmed from a conflicting yet interdependent need to protect both public wellbeing and essential workers’ wellbeing. Nested within this societal-level tension are the knotted performing–belonging tensions experienced by individual midwives. The “horizontal” axis (protecting wellbeing-risking wellbeing) represents performing tensions—specifically, the requirement to perform tasks that, in practice, conflicted with the purported objectives of performing those tasks (see previous subsection). The “vertical” axis (valued member of society-member of undervalued profession) depicts the most salient belonging tension that was knotted with midwives’ experiences of performing tensions. The figure's “diagonal” axes (essential worker-expendable worker) show an additional tension in which the entanglements between performing and belonging tensions are more seamlessly integrated. We explain and illustrate the model in the remainder of this subsection. Table 2 provides evidence of how we developed the model from empirical data.
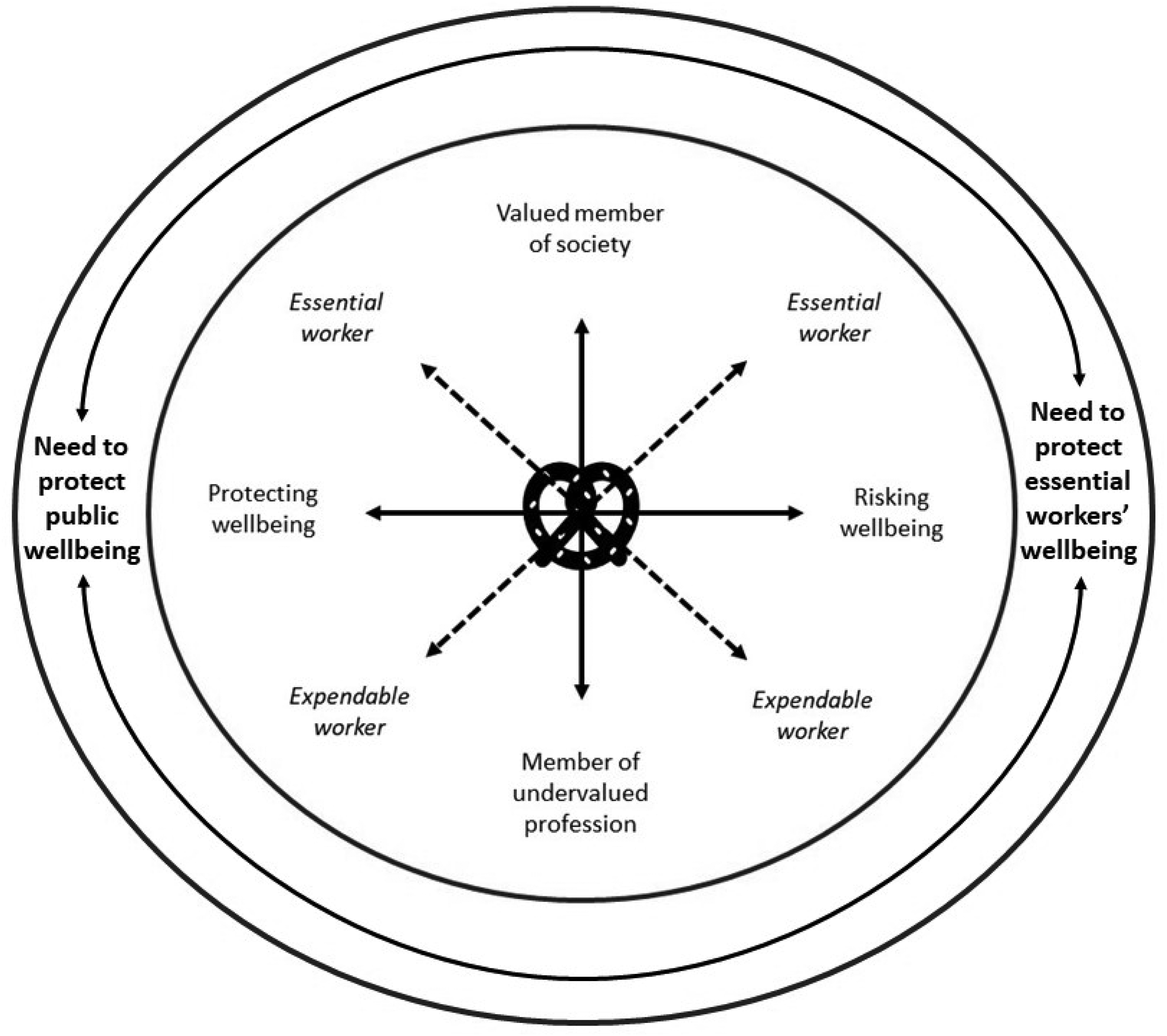
Model of Nested and Knotted Performing–Belonging Tensions.
Performing tensions were knotted with multiple belonging tensions (or identity conflicts) for midwives. For example, the risks involved in midwives’ roles surfaced tensions between their work and non-work identities. To illustrate, some midwives felt torn between being members of the essential workforce, with an obligation to protect and care for clients, and essential members of their own families, with an obligation to protect and care for their loved ones: My husband was angry at me at times and wanted me to stop work. I felt torn between being a midwife, being a mother and being a pregnant woman. (CBMW9)
However, we found that one tension became particularly salient due to its nested-ness within organizing tensions. This belonging tension related to midwives’ dual identities as valued members of their society and members of an undervalued profession (see Figure 2). As already shown, performing tensions stemmed from contradictory demands imposed on midwives by societal leaders. In turn, those contradictory demands were a response to organizing tensions that leaders faced in tackling the pandemic at the societal level. This nested-ness meant that when midwives felt performing tensions, it was within the context of their relationship with wider society. We found that this relationship rendered particularly salient a belonging tension relating to midwives’ perceptions of how well their society recognized and valued their work. On the one hand, midwives saw themselves as valued members of society due to their efforts to protect and uphold public wellbeing. On the other hand, they also viewed themselves as members of an undervalued profession due to society's perceived lack of recognition and support for their efforts.
The knotted relationship between this identity tension and performing tensions can be conceptualized as a hybrid tension in which the “knots” become seamlessly enmeshed. The two poles of that hybrid tension are described in Figure 2 as essential worker and expendable worker. Although used loosely during the pandemic, the term “essential worker” conveys an important message: that society cannot function without such individuals (Peredo et al., 2022). Stated differently, essential workers perform an indispensable role on behalf of the society to which they belong. This implies that for workers who are truly “essential,” performing and belonging are seamlessly aligned. Yet, to feel genuinely essential, workers must believe not only that they perform an indispensable role for their society, but that their society recognizes the indispensability of their role. If essential workers are not recognized as such, they feel “expendable.”
Our data provide insights into how midwives’ experiences of this hybrid performing–belonging tension were shaped by its embeddedness in a pragmatic paradox. Specifically, we found that because midwives’ experiences of performing tensions stemmed from unrefusable contradictory demands, they could not oscillate between poles of performing tensions (Smith & Lewis, 2011). In other words, midwives could not choose to either protect wellbeing or risk wellbeing because the socio-material constraints of their situation forced them to do both. However, midwives could oscillate toward one pole of the most salient belonging tension that was knotted with their experiences of performing tensions. This was because their sense of belonging (or not belonging) was under their subjective control (i.e., it was a matter of interpretation). As we show in the following subsection (see especially Figures 3 and 4), this constrained interaction between knotted tensions led most midwives to oscillate to an extreme pole of the belonging tension, and that polarized oscillation ultimately shaped how they experienced contradictory work demands.
Aligned Performing–Belonging Tensions Indicate Midwives are Essential Workers.
Misaligned Performing–Belonging Tensions Indicate Midwives are Expendable Workers.
Midwives Interpret the Alignment Between Tensions
Midwives interpreted the alignment between knotted and nested performing–belonging tensions from cues in their social environment. Cues came from multiple sources, including media coverage of essential workers, leaders’ communication (e.g., speeches and statements), perceptions of (non)support from healthcare authorities, and interactions with clients, community, and family members. Drawing on such social information, midwives determined whether the contradictory demands they faced in their roles (performing tensions) were aligned or misaligned with a sense of belonging. In turn, this (mis)alignment was related to the perceived balance between societal-level organizing tensions. If midwives felt their society was adequately balancing the tension between their wellbeing (as essential healthcare providers) and public wellbeing, midwives identified as valued members of society. Consequently, they perceived that performing and belonging tensions were in alignment. In contrast, if midwives perceived an imbalance in society's concern for their wellbeing versus public wellbeing, they felt like members of an undervalued profession. In turn, this perception undermined their sense of societal belonging, leading them to perceive misalignment between performing and belonging tensions. In aggregate, these distinct interpretations of the (mis)alignment between tensions triggered two different subjective responses to the pragmatic paradox. Figure 1 depicts this “forking” in subjective responses.
Aligned Tensions
Midwives who perceived aligned performing–belonging tensions interpreted relevant social information to indicate a balance in society's concern for midwives’ wellbeing versus public wellbeing. Key cues supporting this interpretation were: acknowledgment and appreciation from clients and colleagues; pride and support from family and community members; and recognition from societal leaders, news media, and the public. Notably, two “subgroups” of midwives were more likely to perceive aligned tensions: (1) facility-based midwives who were in regular contact with colleagues and managers and (2) community-based midwives who focused more on cues from their immediate social environment (e.g., their local community and interpersonal interactions) and less on cues from wider society (e.g., media coverage and leader communication). It seems that being in contact with coworkers and/or focusing on the local environment supported midwives’ interpretation that their efforts to uphold public wellbeing were reciprocated with concern for their wellbeing from others. In turn, this interpretation created a sense of belonging. Participant quotes illustrating this pattern include: I do feel community members appreciate midwives continuing to offer professional services during the various lockdowns. Many have said so to me and written it on social media. (FBMW87) [I received] lots of support from our community. Lots of thank yous [sic]. Supermarkets that catered to us with opening at special times. Just felt very carried. (CBMW66)
When midwives felt like valued members of society, they framed the performing tensions associated with contradictory work demands as part of a duty as essential workers. Figure 3 offers a visual depiction of this notion. Specifically, the figure shows that when midwives oscillated toward the “belonging” pole of the identity tension, relevant social cues pointed to them being recognized as genuinely essential workers. The figure also illustrates how this oscillation tended to be quite polarized (or extreme) because socio-material constraints blocked midwives from oscillating between poles of the knotted performing tension. One midwife captured how a sense of belonging was related to public recognition when she stated: “I feel we are necessary to public health and most whanau [clients and their families] appreciate our hard work and exposure to the potential risk of infection” (FBMW174).
In turn, as shown in Table 3, midwives who felt like genuine essential workers typically ignored or accepted their lack of agency regarding the imposed obligation to continue working through lockdowns. We suggest this was primarily due to their positive framing of work demands as part of a societal duty. A duty is not necessarily something individuals “want” to fulfill; rather, individuals fulfill duties from a combined sense of obligation and collective belonging (Wakefield & Khauser, 2021). The NZ government developed public messaging to leverage this aspect of duties during the pandemic, encouraging societal members to frame whatever sacrifices they made as part of a duty to “the team of five million” (i.e., the population of NZ). This meant that when midwives felt like they were valued members of NZ society, the ensuing sense of social identification drew their attention away from “having” to fulfill contradictory demands as part of their roles. Instead, these midwives were motivated by the need to support their society by working through the unprecedented, contradiction-ridden situation that was the pandemic. As one midwife stated: I found as a whole everyone was being supportive during the pandemic. New Zealand people are good at pulling together in a crisis as we’ve experienced in earthquakes and floods! I think women needed to know we as health practitioners would always be there for them as we have a duty of care as a nurse and midwife! Otherwise, you’re in the wrong job. I really feel women were comforted by the fact that our presence would never change. (CBMW15)
Evidence to Support Our Theorization of how the Nested-ness and Knotted-Ness of Tensions Influence the Subjective Experience of a Pragmatic Paradox.
Misaligned Tensions
Midwives perceived misaligned performing–belonging tensions when they interpreted social cues to indicate an asymmetrical concern for their wellbeing versus public wellbeing. The main cues supporting this interpretation were: lack of recognition for midwives in media coverage, leader communication, and public discourse; inadequate support with additional funding and safety measures (especially PPE) from government-run healthcare organizations; lack of appreciation from clients; and family interactions (e.g., conversations with children or spouses) suggesting midwives were being exploited by the government. Although the midwives who perceived aligned tensions focused primarily on cues in their immediate social environment, those who perceived misaligned tensions paid more attention to their “invisibility” in media coverage and to a lack of material support from healthcare authorities. Midwives who perceived misaligned tensions were also more likely to be community-based and to identify as members of an undervalued profession (as opposed to valued societal members) even before the outbreak of COVID-19 and ensuing lockdowns. These patterns were evident in quotes such as: I don't feel appreciated [by the public], but this is true outside of covid, because people don't understand the mahi [work] of a midwife in general. We are too often thought of as doing the same work as nurses. It was hurtful seeing on the news recognition for doctors, nurses, and other frontline workers but hardly anything for midwives. (CBMW9) I felt not very safe as there was very little PPE and it felt like midwives, even though [we were] on the frontlines HAVING to go into homes and seeing our clients face-to-face, were the last to be offered any PPE, having to source it ourselves at our own cost. (CBMW75)
A perceived lack of recognition, support, and appreciation for their work left midwives feeling disconnected from their society. In turn, this led to the perception that midwives were being treated like expendable workers, as illustrated in Figure 4. Midwives who felt like expendable workers resented and fixated on their lack of agency to refuse contradictory work demands. Such fixation and resentment were evident not only in the propositional content of participants’ written survey responses, but in their use of capitals and exclamation points: “It actually was not a DECISION! I actually had no option” (CBMW28); “we HAD NO CHOICE but to continue working” (CBMW55); “I didn’t have a choice! There was no decision to ‘work through’” (CBMW145). A significant reason midwives felt they lacked agency was their perceived inability to be seen or heard in mainstream news media and, by extension, by the leaders whose decisions were behind contradictory demands imposed on them. As one participant stated: “I think we were absorbed into ‘nursing/frontline worker’ very effectively and felt angry at mainstream media's ability to ghost us into an ‘unseen’ role” (CBMW70). Ultimately, midwives who felt disconnected from their wider society experienced contradictory work demands as negative, draining, and disempowering. Participants’ quotes encapsulating such subjective responses include: I felt helpless and had to keep working… During the first level 4 lockdown, I would be trying to breathe calmly in the car, to try control the panic, before seeing clients and having to pretend it was all OK. I feel midwives were very much alone out there. No PPE available. [I] had to spend $400–500 to source [my own PPE]. Most New Zealanders have NO IDEA what midwives do, during a pandemic or not. Pregnant women / clients may have appreciated us, but the general public does not. If a company offered a product or perk to essential workers, and listed a few…The list never includes midwives, it would be Nurses! Doctors! Supermarket workers, police…Our work is not seen or appreciated in wider society. (CBMW113) I remember the day I realized I was an ‘essential worker’ and all that entailed. I would be going out to communities, to the hospital, people's homes. I was more concerned that I would bring corona home to my family. That made me very uneasy, my family at home doing what they were supposed to do, locked down, staying put, staying away from others, and I was the one that was potentially endangering them. As an ‘essential worker’, I felt powerless to protect them, and forced to continue to care for the women [in my caseload]. (CBMW141)
Discussion
Drawing on a qualitative, abductive study of midwives who were essential workers during COVID-19 lockdowns, we examined how the nested-ness and knotted-ness of a pragmatic paradox influenced the subjective experience of ensuing tensions. The most immediate tensions experienced by midwives stemmed from unrefusable and contradictory work demands embedded in their professional roles. These demands gave rise to performing tensions by forcing midwives to carry out tasks that, in practice, conflicted with the purported objectives of the tasks. In sum, midwives’ roles entailed both protecting wellbeing and risking wellbeing. The fact that midwives lacked the agency to refuse the demands and the material resources to navigate them (due to midwives’ position in a system of power) implies that the demands constituted a pragmatic paradox (Berti & Simpson, 2021a).
We found that midwives’ subjective responses to this paradox could not be understood without identifying how performing tensions were knotted with belonging tensions and nested within societal-level organizing tensions. Because midwives lacked the agency and material resources to oscillate between poles of performing tensions (either protecting wellbeing or risking wellbeing), their subjective responses to contradictory work demands were shaped by their oscillation toward the extreme pole of a knotted belonging tension. Stated differently, midwives felt either motivated or disempowered by contradictory work demands depending on whether they perceived the demands as being aligned or misaligned with a sense of societal belonging. In turn, this framing of performing–belonging tensions was directly related to the tensions’ nested-ness within societal-level organizing tensions. Contradictory work demands were imposed on midwives by societal leaders who needed to simultaneously protect public wellbeing and essential workers’ wellbeing in response to the material conditions of the pandemic. Ultimately, midwives’ responses to the pragmatic paradox were shaped by their interpretations of how well their society's leaders—and members of the NZ public more generally—balanced this contradictory yet interdependent need as it related specifically to midwives.
Contributions and Implications
Our findings advance knowledge of pragmatic paradoxes in important ways. To start, we provide a more nuanced view of the subjective experience of pragmatic paradox. Most prior research on pragmatic paradoxes is conceptual, drawing on examples identified in empirical studies that were not explicitly focused on pragmatic paradoxes (Berti & Simpson, 2021a; Cunha et al., 2023). While these examples illuminate key features and antecedents of pragmatic paradoxes, they do not explicitly reveal how the knotted-ness and nested-ness of ensuing tensions influence subjective experiences of the phenomenon. Our most surprising discovery—that a pragmatic paradox could be experienced as motivating (rather than disempowering) given a certain alignment between knotted and nested tensions—highlights the importance of understanding how pragmatic paradoxes fit within a complex web of interconnected tensions occurring at multiple levels.
It is important to note that by illustrating how a pragmatic paradox was sometimes framed and experienced “positively” at the subjective level, we are not suggesting that pragmatic paradoxes are positive in any “objective” sense. Indeed, we emphasize that there are at least two potential readings of our surprising finding. The more “positive” reading is that, given the crisis situation of the pandemic, midwives and other essential workers needed to accept or ignore their lack of agency to refuse contradictory work demands in the interests of a greater good. The material conditions of the pandemic created immense stress on underprepared health systems worldwide (Kniffin et al., 2021). Safety measures needed to be implemented based on limited information about the virus (Carmine et al., 2021), and leaders faced material constraints in gathering and distributing sufficient quantities of PPE to essential workforces (Fenton, 2020). Arguably, under these material conditions, risking wellbeing was all but inevitably linked to protecting wellbeing. Therefore, if leaders and influential societal members could create a sense of belonging in midwives, encouraging them to frame and accept contradictory demands as part of a societal duty, it was a net positive for society.
The more “critical” reading of the finding is that midwives who felt motivated by contradictory work demands were victims of societal-level subjectification (Berti & Simpson, 2021a; Pérez-Zapata et al., 2016). As discussed earlier, subjectification is a systemic form of power that shapes individuals’ identities to such an extent that individuals may take for granted contradictory requirements and demands (Berti & Simpson, 2021a). Subjectification influences the meanings individuals attach to social phenomena by instilling dominant logics and norms, limiting individuals’ choices in responding to those phenomena (Pérez-Zapata et al., 2016). Arguably, subjectification is at play when individuals feel a sense of duty (Berti & Simpson, 2021b). Research shows that willingness to fulfill duties is closely related to social identities and identification (Wakefield & Khauser, 2021). Therefore, “willingly” accepting a duty that entails inherent contradictions may be a symptom of pathological subjectification (Berti & Simpson, 2021a). From this perspective, midwives who accepted or ignored their lack of agency to refuse contradictory work demands were as “objectively” powerless as those who fixated on their lack of agency and, consequently, felt “subjectively” powerless.
We remain neutral regarding which of these interpretations is better justified. We also suggest that the interpretation most likely to resonate with specific readers will depend on multiple factors, including duty orientation (Hannah et al., 2014) and political orientation toward pandemic-related issues (Sheep, in Sharma et al., 2021). What we do emphasize regarding our surprising findings is that they underscore the importance of understanding pragmatic paradoxes as contextually situated phenomena that cannot be understood in isolation from interrelated paradoxes and tensions. Particularly relevant are our findings regarding how pragmatic paradoxes can originate at “higher” levels and become knotted with different types of tensions at a “lower” level. Fairhurst et al. (2016) argued that understanding (a) power relations and (b) interwoven and layered paradoxes should be priorities for paradox researchers. Their calls have since been echoed by other scholars (e.g., Berti & Cunha, 2023; Cunha & Putnam, 2019; Keller et al., 2021; Schad & Bansal, 2018; Sharma et al., 2021). Our research provides insights that potentially address and connect both these calls, enhancing understanding of how power relations shape the experience of nested and knotted paradoxes.
The pragmatic paradox experienced by midwives was nested within a wider organizing paradox faced by societal leaders. Importantly, we found that this nested-ness provided an implicit frame of reference (Knight & Paroutis, 2017) for formulating a psychological response to the pragmatic paradox. Because unrefusable yet contradictory demands were a reaction to organizing tensions at the societal level, midwives framed the demands within the context of their relationship with wider society. That relationship involved a belonging tension between midwives’ self-views as valued members of society and members of an undervalued profession. In turn, this belonging tension became knotted with performing tensions stemming from contradictory demands. Critically, midwives could not refuse or navigate those demands because they (the demands) were governed by a power asymmetry between midwives and societal leaders (Berti & Simpson, 2021a; Cunha et al., 2023). In turn, this meant midwives could not oscillate between poles of the performing tension (protecting wellbeing or risking wellbeing) because they lacked the agency to do so. But midwives could oscillate toward one pole of the knotted belonging tension, which they did based on their interpretations of relevant social information. Ultimately, that “forced” and “polarized” oscillation shaped midwives’ subjective responses to the pragmatic paradox.
We suggest these findings provide much needed insights into the relationship between power dynamics and multi-layered, interwoven paradoxes (Fairhurst et al., 2016). One insight is that although power asymmetries may limit responses to one set of tensions (e.g., oscillating between poles of performing tensions), the same power relations may not prevent individuals from responding to knotted tensions (e.g., by oscillating toward the extreme pole of an interrelated belonging tension). We suggest this will be especially relevant when there is a discrepancy in how distinct types of paradoxical tensions are governed by socio-material constraints. In our study, performing tensions were related to physical acts of caring for clients in face-to-face encounters, meaning midwives could not escape the materiality of the tensions without breaching contractual obligations embedded in their relationship with the healthcare authorities. In contrast, midwives’ perception of belonging (or not belonging) was a purely “mental act,” implying it remained under their subjective control (notwithstanding the influence of subjectification). Accordingly, while societal leaders could control midwives’ bodies through the imposition of legal obligations, leaders could not fully control their minds. This finding supports calls for further research into how and why bodies and minds respond differently (or similarly) to paradoxes associated with power disparities (Heucher et al., 2024).
Another insight is that belonging tensions are connected to the perceived legitimacy of power asymmetries underpinning contradictory demands. When midwives felt they belonged to NZ society, they concentrated more on how their predicament was undergirded by material constraints, such as society-wide shortages of PPE. When midwives felt disconnected from society, they focused on how their situation stemmed from their lack of agency to refuse contradictory demands. These findings build on existing conceptual research (Berti & Simpson, 2021a; Cunha et al., 2023) by illustrating how underlying power asymmetries are perceived at the subjective level. Specifically, the findings show that responses to belonging tensions can shape the framing of nested pragmatic paradoxes as either (a) inevitable (and, therefore, legitimate) by-products of materially imposed organizing tensions; or (b) avoidable outcomes of power disparities. The findings also invite further exploration of how tensions associated with other nested and/or knotted pragmatic paradoxes shape the perceived legitimacy of underlying power relations. An equivalent scenario might involve employees who are motivated versus disempowered by unrefusable contradictory demands depending on their (the employees’) degree of (dis)identification with organizational leaders (Lee, 2016) and/or their organization (Brown, 2017). We suggest that future studies might also explore how the perceived legitimacy of contradictory demands relates to workers’ inferences regarding leaders’ motivations for imposing such demands. For example, are the demands of a pragmatic paradox perceived as a consequence of leaders facing an inescapable paradox themselves? Or do contradictory demands apparently stem from leaders’ incompetence or power hunger?
Finally, our research provides insights into how nested pragmatic paradoxes can inhibit metacommunication (Berti & Simpson, 2021a). Metacommunication refers to communication about the act of communicating (Alvesson & Spicer, 2012). Metacommunication may enable actors to navigate contradictory demands by, for example, joking about the absurdity of the demands (Jarzabkoswki & Lê, 2017). Conceptual research suggests that the inability to engage in metacommunication is a key reason low-power actors can be paralyzed by pragmatic paradoxes in organizations; effectively, such actors lack the agency to question the contradictory demands imposed on them by seniors (Berti & Simpson, 2021a; Cunha et al., 2023). Our research shows how a similar process can unfold at the societal level. During the pandemic, midwives lacked the opportunity to communicate directly with societal leaders about their experiences of contradictory demands. Arguably, if midwives had this opportunity, they might have been able to navigate their predicament more effectively (e.g., by gaining access to material resources to minimize risks to wellbeing). Midwives did have the opportunity to communicate with leaders indirectly, via news and social media (e.g., they could talk to journalists or post on social media about their situation). But critically, even though midwives could communicate information about their predicament via such media (they were not explicitly forbidden from doing so), they felt they generally lacked the social standing to be “seen and heard” by powerful members of their society. This finding suggests that for metacommunication to be effective in addressing pragmatic paradoxes (Berti & Simpson, 2021a), low-power individuals must not only be permitted to communicate about their situation with seniors, but also be seen and heard by those with political power.
Limitations and Future Research
We suggest two limitations of our research context and design to keep in mind when considering the conclusions of our research. First, the pragmatic paradox we identified was specific to the COVID-19 pandemic. The contradictory demands of risking wellbeing and protecting wellbeing are unlikely to have persisted once the most overwhelming impacts of pandemic subsided. Moreover, because we gathered data at a single point in time, we do not know whether midwives’ situation eventually changed during the pandemic, potentially enabling them to navigate performing tensions (e.g., with support from societal leaders and healthcare organizations). This temporal limitation of our research raises questions about whether persistence should be included as a defining feature of pragmatic paradoxes. Researchers investigating “non-pragmatic” paradoxes generally agree that interdependent contradictions must have a persistent or recurrent quality to meet the definition of paradox (Lewis & Smith, 2022). Yet, existing definitions of pragmatic paradox make no mention of persistence or recurrence (Berti & Simpson, 2021a; Cunha et al., 2023). Perhaps this is because pragmatic paradoxes have an inherently more ephemeral nature than other paradoxes. For example, when a manager paralyzes a subordinate by issuing a contradictory order (e.g., “act spontaneously”; Cunha et al., 2023), how long does the paralysis need to last for the situation to qualify as a pragmatic paradox? Does it only need to last until the subordinate is out of the manager's sight and able to get on with other tasks? Or until the manager forgets that they issued the order? Or until the underlying tensions and pressures that led the manager to issue the order are “resolved”?
This last question hints at an intriguing direction for future research. Prior studies imply that pragmatic paradoxes can exist in both salient and latent form because contradictory demands may stem from visible (explicit) or invisible (implicit) forms of power (Berti & Simpson, 2021a; Cunha et al., 2023). Our research explored midwives’ responses to a pragmatic paradox that became salient during a societal crisis. In turn, this paradox was nested within organizing tensions rendered salient by the urgency of responding to COVID-19 (Keller et al., 2021; Sharma et al., 2021). But what about latent pragmatic paradoxes that remain hidden from actors because they are nested in underlying tensions (Schad & Bansal, 2018)? If pragmatic paradoxes should be eradicated because of their disempowering effects (Cunha et al., 2023), then how can researchers and other individuals “make visible” the power asymmetries underlying them? Paradox scholars have developed a strong understanding of how the environmental conditions of scarcity, plurality, and change relate to the latency versus salience of tensions (Miron-Spektor et al., 2018). How, then, can researchers leverage this understanding to render latent pragmatic paradoxes salient not only to the actors affected directly by them, but to individuals with the power to address underlying socio-material conditions? Exploring the relationship between material scarcity and latent pragmatic paradoxes might be particularly relevant in coming years because, as the global environmental crisis deepens (Hahn, in Sharma et al., 2021; Hahn et al., 2015; Jarzabkowski et al., 2022), the power to control material resources is likely to become increasingly contested and consequential. How will resource-driven power struggles translate into contradictory demands imposed on workers and, more importantly, how can we make visible the experiences of workers entangled in such struggles?
A second limitation of our research relates to how we collected data. We examined midwives’ experiences through an online, open-ended survey. This approach to data collection afforded advantages such as enabling safe collection of real-time data as the pandemic unfolded, and it yielded a large number of qualitative responses, facilitating theorization based on variance in the sample (Locke et al., 2022). However, the approach did not permit us to ask follow-up questions or adjust our data collection protocol as the study progressed, as is common in other qualitative paradox research (e.g., Pamphile, 2022; Pradies, 2023). Thus, while our data were sufficiently rich and varied to enable abductive analysis (Folger & Stein, 2017), using more conventional qualitative data collection techniques (e.g., interviews, researcher observations) could provide further insights in future research on a similar topic. For example, knowing that midwives’ experiences of performing–belonging tensions were shaped by organizing tensions facing societal leaders, it would have been interesting to ask midwives about how they judged such leaders’ handling of the pandemic. Did midwives who felt a sense of societal belonging and duty also judge leaders’ actions and decisions to be more competent in the context of material constraints? And was the opposite true of midwives who felt disconnected from their society? Using interviews and other rich data collection techniques will help address such questions in future research on nested and knotted pragmatic paradoxes.
Conclusion
Our paper examined how the nested-ness and knotted-ness of a pragmatic paradox influenced the subjective experience of ensuing tensions. We provided novel insights into how workers “live through” pragmatic paradoxes, suggesting the experience can be disempowering or motivating. More importantly, we showed how pragmatic paradoxes unfold in complex social systems undergirded by power asymmetries and involving interrelated tensions at multiple levels. We hope our research inspires further exploration of how societies can navigate contradictory demands and address urgent challenges without disempowering certain members.
Supplemental Material
sj-docx-1-jmi-10.1177_10564926241301024 - Supplemental material for Societal Duty or Pragmatic Paradox? Exploring Midwives’ Experiences of Contradictory Work Demands During COVID-19 Lockdowns
Supplemental material, sj-docx-1-jmi-10.1177_10564926241301024 for Societal Duty or Pragmatic Paradox? Exploring Midwives’ Experiences of Contradictory Work Demands During COVID-19 Lockdowns by James Greenslade-Yeats, Tago L. Mharapara, Janine H. Clemons and Talei Jackson in Journal of Management Inquiry
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.