
Abstract
Perspective-taking, or engaging with the viewpoints of others, has been linked to a range of positive and negative interpersonal outcomes. However, it has only been researched infrequently in organizations, and questions remain about how it might be developed as a multidimensional cooperative process and problem-solving capability more widely. To better understand this, this article presents findings from a 2-year change intervention with 10 US hospitals. Interview data from three time points (393 interviews, 197 staff members) reveal dimensions and levels of understanding underpinning the development of organizational perspective-taking. Actors’ accounts suggested several major interrelated dimensions of perspective-taking operating at local and system levels, through affective concern, cognitive understanding, and motivational efforts to improve the sharing and interpretation of diverse perspectives. The study has implications for how organizations can better foster perspective-taking by building ecological structures and processes that assemble perspectives supportively, holistically, and frequently.
Introduction
For complex organizational systems to remain cooperative and interdependent, they need actors and units that can recognize and view issues from one another’s diverse perspectives (Boland & Tenkasi, 1995; Ku et al., 2015; Litchfield & Gentry, 2010). In this regard, the psychological process of perspective-taking has been of some interest to scholars of organization (Grant & Berry, 2011; Ku et al., 2015; Parker et al., 2008). In their recent review, Ku et al. (2015) refer to perspective-taking as “the active cognitive process of imagining the world from another’s vantage point or imagining oneself in another’s shoes to understand their visual viewpoint, thoughts, motivations, intentions, and/or emotions” (pp. 94–95).
Prior to conceptualizations of perspective-taking, the history of related concepts such as sympathy goes back several centuries in philosophy, politics, and economics, with empathy originating in the German aesthetic concept of Einfühlung, concerning how we observe, feel with or for, enter into and understand the emotions of other people (Davis, 2018). While sympathy and empathy are intertwined to some extent, they can also be confused and contested, with considerable distinct literature and traditions behind each. Although both concerns responding to the experiences and feelings of others, sympathy is generally held to be a more passive awareness of and matching to intense and/or negative feelings of others, whereas empathy concerns broader, more active efforts to know, understand and imagine what it would be like to be the other person (Davis, 2018; Wispé, 1986). Psychologist Carl Rogers, for example, posited empathy, not sympathy, as an important condition for making positive changes to personalities and relationships (Rogers, 1961). From roots in sympathy and empathy, perspective-taking emerged in the 20th century as a fundamental social and developmental process of human interaction, necessary for navigating a world of mixed motives, viewpoints, and boundaries concerning the self and others (Calvard, 2010; Galinsky et al., 2005; Parker et al., 2008).
Here our theoretical focus is not on sympathy except as a potential component of empathy, involving pity and concern for the difficulties of others. In turn, we are interested in empathy as an affective instance of perspective-taking associated with showing concern for gaining a non-judgmental understanding of the positive and negative experiences and feelings of others (Davis, 2018; Wispé, 1986). Our main interest, however, is in how the building of perspective-taking capabilities takes place as a broader supportive and cooperative process. This process is likely to involve interrelated aspects or components associated with feeling with/for, thinking about, understanding, relating, and responding to the viewpoints of diverse others on the main purpose of the organization and how to better achieve it together.
Our arguments and justification can be contextualized in terms of developing perspective-taking literature in management and social and organizational psychology (e.g., Ku et al., 2015; Litchfield & Gentry, 2010; Parker et al., 2008). Specifically, we seek to explore perspective-taking as a multidimensional interpersonal process that can broaden and build across dimensions and interactions into richer understandings of organizational perspectives. This view helps shed light on how people in organizations understand diverse experiences and viewpoints of diverse others in terms of specific aspects of emotions, knowledge bases, and efforts to share and interpret experiences. Perspective-taking here also potentially involves both interactions between pairs of people and more systemic, expansive views of multiple related perspectives across groups and agencies in a wider organizational system. In practical terms, investigating perspective-taking in this way can help understand how people relate to each other in more trusting, creative, and cooperative relationships at scale (Galinsky et al., 2005).
In sum, this article seeks to advance our understanding of perspective-taking in individuals, groups, and organizations by considering how it can be built up, developed, and expanded as an organizational or systems capability (Litchfield & Gentry, 2010; Pavlovich & Krahnke, 2012). Much research on perspective-taking has focused on isolated interpersonal pathways, based on laboratory studies or micro-interactions at work (Ku et al., 2015; Parker & Axtell, 2001). However, while crucial to understanding how perspective-taking operates between people, this research neglects understandings of how forms of perspective-taking might build from the interpersonal into more widely shared capabilities and experiences.
The remainder of this article is presented as follows. First, we review the literature on perspective-taking and interpersonal outcomes, followed by literature relevant to perspective-taking as an organizational and systems capability. Second, we present a secondary analysis of a wider qualitative study of a 2-year intervention carried out with a group of 10 hospitals seeking to improve the care of cardiac patients, and reduce mortality rates. The intervention was designed to aid creative problem solving through encouraging and building cooperation and shared understandings across an organizational system. The “perspectives” in question here were diverse views on how to achieve the main purposes of the organization (better patient care, and reduced mortality) and views on how to accommodate and integrate different perspectives to achieve those main purposes more effectively. Change coalitions of actors with diverse roles were formed in each hospital to meet periodically for facilitated discussion and exchanges of viewpoints regarding positive culture change and shared leadership responsibilities. In addition, we use recent perspective-taking theory and the data structure analyzed for presenting a framework of three perspective-taking dimensions (affective, cognitive, and motivational) and two levels (local and system). Finally, we discuss further how perspective-taking can broaden and build across repeated, varying interactions with diverse others, with implications for future research and practice.
Perspective-Taking and Interpersonal Outcomes
From within a psychological tradition, perspective-taking has been treated as a process where individuals are imagining the world from another person’s point of view. In interpersonal interactions, this process can generate affective states such as “empathic concern” for another perspective—feelings of warmth, compassion, care, and concern toward others experiencing difficult circumstances (Davis, 2018)—as well as social and cognitive reactions reflecting adjustments to and judgments of other perspectives (Galinsky et al., 2005; Parker et al., 2008). Perspective-taking and empathy are generally held to be both related and distinct parts of understanding others. Perspective-taking is overall a more cognitive, goal-directed intellectual process, while empathy is an emotional response that allows one person to affectively connect with another, making helping more likely overall (Ku et al., 2015; Parker et al., 2008).
While generally held to have positive effects on organizational relationships, ambiguities remain around processes and effects of perspective-taking, depending on the characteristics of the actors involved, the qualities of their relationships, and the bases for their interactions (Ku et al., 2015). Perspective-taking and empathy can have downsides, dark sides, and limitations depending on how they are directed, experienced, and assessed—for example, as too intrusive or exhausting, as leading to non-cooperative or manipulative behaviors, and as unbalanced or inviting social and ethical dilemmas (Bloom, 2017; Galinsky et al., 2005). In general, however, when at their most positive and effective in considering the viewpoints and needs of diverse others, perspective-taking processes and accompanying feelings of empathy can blend with and relate to a variety of virtuous behaviors relevant to management and leadership in organizations. Among others, these include altruism, compassion, helping, inclusion, and justice (Calvard, 2010; Hoffman, 2001; Parker et al., 2008).
In most reviews of perspective-taking, dyadic interactions are described, and a range of positive outcomes. Perspective-taking has been shown to promote cooperation, coordination, helping, moral development, reduced stereotyping, reduced attribution errors, creativity, emotion regulation, and conflict management (Ku et al., 2015; Parker et al., 2008). The capacity to engage in perspective-taking behavior willingly and effectively is also influenced at the interpersonal level by a range of moderators. These include the abilities and traits of actors, demands of the task or situation, and the relationships and contexts framing work interactions (Ku et al., 2015; Parker et al., 2008).
Beyond interpersonal or dyadic encounters between individuals, knowledge of how components of perspective-taking build and aggregate across groups and organizations remain limited. However, through various habits and measurable interventions, individuals in interaction can cultivate perspective-taking. These include controlled meetings, narrative scenarios with instructions to focus on imagining perspectives, and writing stories about the lives of diverse others (Ku et al., 2015). Perspective-taking habits also include curiosity about strangers; challenging prejudices and discovering commonalities; trying out life experiences of others; listening hard and opening up in conversation; inspiring mass action and social change; and developing an ambitious imagination (Krznaric, 2014).
Much perspective-taking evidence is based on experimental psychology, with insights limited to individuals and dyads. What is lacking is greater exposure to perspective-taking dynamics in field settings and contexts, concerning more holistic social and change interventions. This is important for organizations given that perspective-taking mindsets and behaviors represent crucial human microfoundations explaining, “how collective-level phenomena come to exist from individual-level phenomena” (Litchfield & Gentry, 2010, p. 201). This is also important for organizations because building perspective-taking across levels of social organization can be fragile, subject to breakdowns or counterproductive effects relating to competition and self-interest (Galinsky et al., 2005; Ku et al., 2015). Questions also remain concerning the optimal balance and combinations of dimensions of perspective-taking as they unfold and emerge across individuals and groups (Litchfield & Gentry, 2010). For instance, positive and caring emotional perspective-taking interactions may build employee helping, cohesion, and well-being, but be less effective for focused knowledge integration and problem-solving. Conversely, cognitive and intellectual perspective-taking may build learning and knowledge integration, but lack sufficient affective perspective-taking to address instrumental, competitive goal pursuit (Litchfield & Gentry, 2010).
Existing research on workplace perspective-taking in the form of experiments and surveys highlights how power differentials and social distances between actors need to be addressed and overcome to appreciate the perspectives of others (Galinsky et al., 2006; Galinsky et al., 2016). Powerful actors may show less concern, adjustment, and awareness toward less powerful perspectives, unless they are primed to experience a greater sense of responsibility toward them (Galinsky et al., 2016). However, in negotiations, cognitive perspective-taking can enhance individual and joint outcomes (Galinsky et al., 2008). Harnessing the social-psychological benefits of perspective-taking thus depends on shaping appropriate interaction contexts, goals, and addressing perceived differences in status, esteem, and power (Ku et al., 2015).
Field surveys of employees find positive interpersonal effects of perspective-taking, including cooperative and discretionary, prosocial behaviors. Employees integrate understandings and share experiences with others in different roles and groups, such as suppliers, co-workers, and customers, attributing favorable causes to their behaviors (Axtell et al., 2007; Parker & Axtell, 2001). Other positively reinforcing and virtuous associations have been found between perspective-taking and employee creativity, humility, pro-diversity attitudes, customer service, respect, and voice (Grant & Berry, 2011; Madera, 2018; Ng et al., 2021; Wang et al., 2017).
However, the interpersonal view is partial if we consider that perspective-taking in organizations can unfold within and across complex systems and interdisciplinary communities (Boland & Tenkasi, 1995; Litchfield & Gentry, 2010). Here perspectives are built up into patterns of goals greater than the sum of their parts. More systemic approaches to perspective-taking in organizations are needed, rooted in the emergent development of shared processes and capabilities (Parker et al., 2008). Indeed, Ku et al. (2015) suggest that “much more research should be conducted in this area, translating perspective taking from a social psychological construct to an organizational capability” (p. 92).
Building Perspective-Taking as an Organizational and Systems Capability
Perspective-taking can aggregate up across interactions to affect higher-level functioning of groups, organizations, and systems (Parker et al., 2008). Some team studies show that perspective-taking operates as members try to make sense of their dissimilarities (Williams et al., 2007), and elaborate their diverse perspectives into team creativity (Hoever et al., 2012). Perspective-taking can also develop across multiple teams when deployed collectively as a way of supporting and improving positive intergroup relations (Todd & Galinsky, 2014).
This aggregate view of perspective-taking remains largely implied or theorized, rather than empirically explored. Some fieldwork in knowledge-intensive organizations has proposed that communities of knowing with specialized perspectives and expertise practice “perspective making” across boundaries of exchange, necessitating communication systems designed to support it (Boland & Tenkasi, 1995). Building on the psychology of perspective-taking at the individual level, another conceptual framework outlines individual goal and contact antecedents, intermediate goal and power integration mechanisms, and organizational outcomes, such as knowledge integration and absorptive capacity (Litchfield & Gentry, 2010). Similarly, Pavlovich and Krahnke (2012) propose psychological organizing mechanisms that build on shared feelings of connectedness, positive emotions, and self-other integration. Here, our aim is to build on these emergent conceptualizations of perspective-taking as a group and organizational capability. Our theoretical focus is to further explore the multiple dimensions and levels of perspective-taking engagements, in terms of how interacting people and groups in organizations understand the diverse experiences and viewpoints of diverse others, involving aspects of different emotions, knowledge bases, and efforts to share and interpret different experiences.
We propose that shared perspective-taking is an organizational process, involving various events, activities, ideas, and cooperative interactions (Cloutier & Langley, 2020). Perspective-taking is also relational, involving reciprocal and simultaneous interactions across the “rich connections and interdependencies of organizations and their members. . .a configuration of relationships. . .the multiple meanings and perspectives that continuously emerge” (Bradbury & Lichtenstein, 2000, p. 552). Individuals recognize interdependencies as they inquire into the perspectives of other individuals and groups, accounting for distributed cognition to test and build shared representations (Boland et al., 1994). These dialogs between perspectives enable participants to create new knowledge and organizational change, by distinguishing sharing of responsibilities and possibilities for practice (Tsoukas, 2009). For perspectives to connect systemically, organizations need an ecology of learning interactions, based around framing issues, building dialogs, and enabling forms of action (Senge et al., 2007). Perspectives based on organizational roles allow for individuals and groups’ partial inclusion in perspective-taking processes across the organization (Katz & Kahn, 1978), while also maintaining distinctiveness in the different insights they have to offer (Brewer, 1991).
However, the diverse groups and perspectives making up organizations have to come together to share and integrate perspectives, and be formally supported in doing so (Gittell & Douglass, 2012). Powerful groups and coalitions in organizations can affect patterns of learning and influence (Miller & Lin, 2010), and departmental silos and routines create barriers to interpretation that need to be overcome by greater contact mechanisms to achieve innovation in products and services (Dougherty, 1992).
Perspective-taking across an organization and system is valuable because each perspective across diverse teams and functions tends to contain knowledge that the others lack for understanding problems, filling crucial gaps in representation (Cronin & Weingart, 2007). More democratic, inclusive, and participative organizational cultures can provide a scaffold for building perspective-taking into effective collective deliberations (Morrell, 2010). There are concerns that organizations and populations now have a deficit when it comes to perspective-taking, and a duty to try to improve these capabilities through training and interventions (Bazalgette, 2017). Collective perspective-taking capabilities can help designers focus on seeing things from a user’s perspective (Köppen & Meinel, 2015), stakeholders create common ground on social issues (Tuazon et al., 2021), and managers learn about recovery from organizational scandals and crises (Hay & Samra-Fredericks, 2019).
In sum, we argue that perspective-taking capability in organizations and systems emerges at higher levels from relational processes involving individual and group interactions and dialogs, exploring diverse but interdependent roles, identities, and functional backgrounds. This can improve organizational performance through learning, cooperation, and knowledge integration. However, empirical investigations into these processes remain limited, and existing literature suggests more qualitative field studies are needed and justified in terms of their potential for offering more holistic, interconnected, and relational views of how and why organizational perspective-taking takes place (Ku et al., 2015; Litchfield & Gentry, 2010; Parker et al., 2008). The aim of our study was, therefore, to try to better understand how interrelated dimensions and levels of perspective-taking vary, broaden, and build through interpersonal experiences toward a more widely shared capability, contributing to bridging or integrating investigation of both interpersonal and systemic conceptualizations of perspective-taking.
Method
Health care and hospital settings are highly appropriate for studying perspective-taking, given their complex systems of diverse leaders, specialized groups, and agencies, whose views and priorities can vary in their alignment (Begun et al., 2003). Accordingly, this article draws on data from a wider project involving a longitudinal, mixed-methods intervention study of 10 hospitals over a 2-year period from 2014 to 2016 (Bradley et al., 2018; Curry et al., 2015, 2018). We analyzed qualitative data from 393 in-depth interviews with 197 clinical and management staff across three time points—baseline (n = 162), 6 months (n = 118), and 18 months (n = 113). Across time points, 78 staff were interviewed once, 40 twice, and 79 three times. The 197 participants comprised physicians (n = 42), physician assistants/advanced practice nurses (n = 6), nurses (n = 54), management and administration staff (n = 32), quality improvement staff (n = 22), emergency medical services staff (n = 13), pharmacists (n = 13), and “other” (social work, case management, and cardiac rehabilitation; n = 15).
Participants were engaged in a collaborative quality improvement change intervention called “Leadership Saves Lives (LSL).” This intervention was implemented within and across 10 U.S. hospitals. Each hospital established a guiding coalition that included 15–20 key staff involved in the care of heart patients with acute myocardial infarction (AMI). Coalition members included staff from multiple departments (cardiology, emergency medicine, pharmacy, quality improvement, and cardiac rehabilitation), professions (physicians, nurses, technologists, administrators, and physician assistants), and levels (senior executives to front-line staff). The semi-structured interview guide across the three time points asked hospital coalition members questions about expectations and perceptions of interactive experiences within the guiding coalitions, and of change implementation within and beyond their hospitals.
Members of this network of hospital coalitions participated in on-site workshops, all-hospital annual forums, and a web-based platform for knowledge sharing and continuous remote support. The intervention was designed to foster the uptake of evidence-based practices and to support creative problem-solving within the guiding coalitions. Workshop content included experiential learning sessions focused on promoting role clarity, working across professional and organizational boundaries, working in hierarchy, creating psychological safety, developing accountability for shared goals, and encouraging productive conflict (Bradley et al., 2018; Curry et al., 2015). In more objective terms, the intervention was largely successful, with six hospitals experiencing significant reductions in 30-day risk-standardized mortality rate (RSMR) after AMI over 2 years (Curry et al., 2018).
For this study, the large qualitative dataset was revisited and re-coded by a team of three, using a scaffolding mixture of existing codes on roles and relationships, and new codes reflecting dimensions of perspective-taking identified using data and literature (Morse & Mitcham, 2002). We sought to analyze the 10 participating hospitals as an ecology of perspective-taking, to “encompass the interacting organizations, groups, and agencies that together create the knowledge needed for value creation in a given sector” (Dougherty & Dunne, 2011, p. 1221).
The coding team comprised two authors who were “insiders” to the intervention as health care experts, facilitators, and interviewers, and one “outsider” who acted as a perspective-taking, management, and psychology expert. The coding team carried out the analysis through “standard, systematic, inductive processes in which we circled back-and-forth between data and theory” (Brown & Coupland, 2015, p. 1320). Consideration was given to the main research question of how shared forms of perspective-taking build from interactions, as well as integrative reviews and conceptualizations of perspective-taking from the literature (Ku et al., 2015; Litchfield & Gentry, 2010; Parker et al., 2008). We also used the constant comparative method component of grounded theory to cycle across a large data set and simultaneously code, check and revise data fragments, and incidents (O’Reilly et al., 2012).
Open coding was used to break down and select data judged most relevant to perspective-taking and empathy in terms of instances of how staff were relating to the roles and experiences of others in the 10 change coalitions and hospitals over time; for example, listening, caring, learning, sharing, problem-solving, and voice. Next, axial coding was used to further elaborate, contextualize, and cluster codes into categorical levels and dimensions of perspective-taking—for example, local/interpersonal versus collective/systemic levels, and affective/cognitive/motivational dimensions (Corbin & Strauss, 1990). Finally, the cells of the resulting framework and data structure were further mapped and inter-related as major themes and subthemes. Themes were underpinned by representative quotes and concrete, granular illustrations of how perspective-taking was manifest in hospital interactions, its capacity building across the various, repeated experiences of interactions and practices referencing both the local and system levels of perspectives (Bradley et al., 2007). The three time points and 10 hospital identifiers also provided additional contextualization of the intervention and change influences on participants.
Findings
Coding and analysis resulted in a 2×3 matrix and data structure of major themes and subthemes, as shown below with illustrative codes and quotes, in Table 1. The data structure indicates a framework of mutually reinforcing conceptual relations involved in major perspective-taking dimensions—both at the interpersonal level, and at the system level building into a more widely shared capability. Perspectives arose from diverse roles and experiences; views on how to achieve the main purposes of the organization (better patient care and reduced mortality) and how to accommodate and integrate different perspectives to better achieve them.
Perspective-Taking Data Structure.
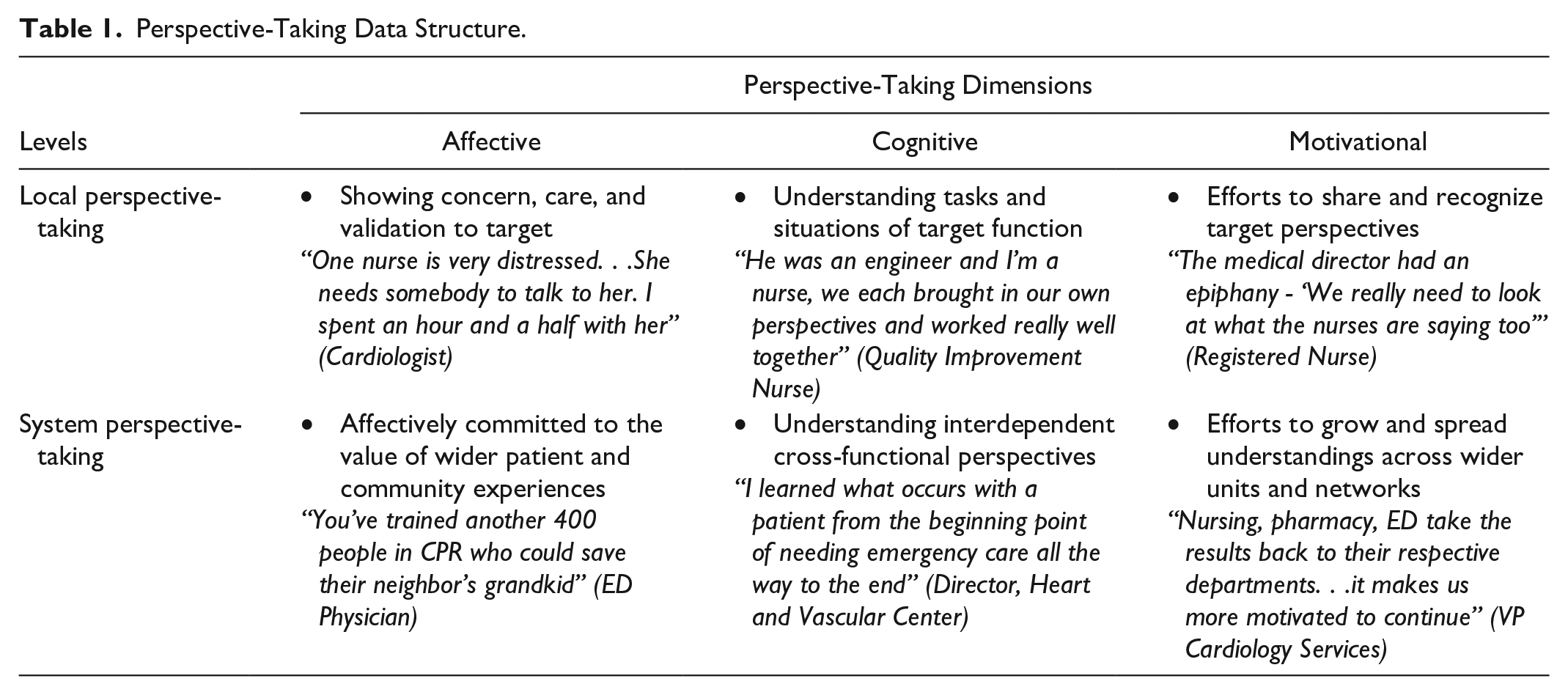
First, two levels distinguish between degrees of abstraction or scope in the nature of perspectives engaged with. The local level reflected interpersonal perspective-taking exchanges between coalition members or actors working closely together at the same hospital. The system level reflected shared perspective-taking concerning multiple perspectives making up entire organizations and agencies across the integrated health care system. Second, a threefold distinction was identified between dimensions of perspective-taking. An affective aspect (empathy and concern for others), cognitive (understanding of tasks and responsibilities), and motivational (efforts to improve and share understandings).
Across the three time points in all 10 hospitals, there was a general increase in the frequency of open data codes relating to openness and problem-solving. There was evidence of all six forms of perspective-taking in Table 1 in all hospitals at all three time points, but with far greater quantities of evidence at the 6- and 18-month time points, rather than the baseline. In general, the data suggested that perspective-taking was occurring in various mutually reinforcing ways from the outset of the change intervention, becoming more frequent and systemic by the later stages, but still simultaneously local and personal, so not necessarily following a linear or incremental progression.
In terms of hospital-level variations across the 10 hospitals studied, 6 experienced reduced mortality rates over time and increased positive staff reports of culture change, partly determined by their having more diverse coalition members, more interactive coalition meetings, and more positive conflict management norms than the remaining four (Curry et al., 2018). However, again, all 10 hospitals showed broadly similar evidence of all dimensions and levels of perspective-taking, suggesting that there were no dramatic variations at the hospital level, potentially due to the relatively uniform purpose, and delivery of the intervention overall.
We do not rule out the possibility of more fine-grained temporal and organizational variations in perspective-taking authenticity and effectiveness, and return to critical reflections on these issues below in the discussion. What this study finds and shows by way of its framework is that perspective-taking occurs and is experienced broadly through multiple major dimensions across repeated and varying other-oriented interactions and connections with diverse parties. In turn, this helps build repertoires of both interpersonal (dyadic) level understandings and ultimately, more system-level understandings and empathy for the shared organizational goals and issues faced by more widely interconnected perspectives.
In ways similar to investing in and experiencing positive emotions and relationships, perspective-taking capabilities “broaden and build” (Fredrickson, 2001); broadening through a variety of thought and action dimensions, and building through cumulative reinforcement and sharing of skills and resources across an organization (Dutton et al., 2006). The study framework thus represents a novel exploration and synthesis of work on the more dyadic/interpersonal experiences of perspective-taking (e.g., Ku et al., 2015; Parker et al., 2008), in conjunction with work on the more higher-level, holistic systems experiences of perspective-taking (e.g., Boland & Tenkasi, 1995; Litchfield & Gentry, 2010; Pavlovich & Krahnke, 2012).
The six subthemes in Table 1 are elaborated on further below. Where participants are quoted, their unique anonymous ID is given as a hospital letter and respondent number in brackets, as well as their role and the time point of the interview.
Local affective perspective-taking
An affective dimension of perspective-taking at the local level was described as arising from personal, intimate, and emotional interactions experienced between pairs of organizational actors, both on the hospital coalitions taking part in the change intervention, and in the hospitals themselves. Where empathy, in general, involves non-judgmental understanding of the positive and negative experiences and feelings of others, empathic concern emerged as a more specific affective theme in our analysis, indicating where people experienced feelings of warmth, compassion, care, and concern toward others experiencing difficult circumstances (Davis, 2018). Accounts included warm and caring emotional experiences, potential sympathy for distress, and other positive affective reactions involved with listening to others’ perspectives and anticipating, relating to, and validating their needs (Parker et al., 2008). These were also described in salient terms when experienced across disciplinary or hierarchical boundaries.
For instance, one cardiovascular surgeon shared how he responded to a nurse who was distressed about how another physician had been treating her with a lack of confidence in her ability. The doctor emphasized the importance of considering her perspective with a sense of empathic concern, showing care, and support. As actors with high power and status, doctors were particularly central to changing emotional dynamics in local perspective-taking interactions, by recognizing other perspectives warmly with positive affirmations, active listening, and a sense of open and safe approachability.
She wanted to talk to me. I was very tired but said yes because I know she is very down. This is my nurse who is going to take care of my patient, and how she feels about another doctor. . .I can be the biggest doctor and write all the orders, but. . .I must thank this nurse for really taking good care. (ID G_1, Cardiologist; 18 months) [This doctor] has really become a good listener. . .a lot of people would turn their ears off when he would start to speak, because he would just go on and on. Now he makes his point a little quicker and is more open to listen to other people. That is a huge change. (ID I_16, Respiratory Therapist; 18 months)
Expressions of empathic concern between staff working in different parts of the hospital and cardiac care pathway were described in terms of gratitude and pride. Where perspectives were invited, participants reported feelings of significance and worth to the organization.
The cardiologist may ask me a question, ‘What’s pre-hospital’s take on that?’ They ask me for my input. I am not just a fly on the wall here. Thank you. I appreciate and respect that. (ID A_1, Paramedic; 6 Months)
Empathic concern was also described as an overcoming and absence of negative emotional interactions between individuals that might hinder perspective-taking—“from a nursing perspective it is interesting to hear physicians discussing amongst themselves without getting petty or accusatory” (ID G_12, Nursing Education Specialist, 18 months).
The time and space of the intervention outside of the busy, pressured accountabilities of daily work created a necessary set of interpersonal conditions for the broadly empathic sense of familiarity, liking, oneness, and similarity to support local affective perspective-taking.
The key is knowing that that other person has the same hopes, fears, wants, and dreams that you do. It is not until you let down your guard and realize that, that you can feel safe and come out in that. That is when you find out that we are all one. We all have strengths that reach out to everybody else’s weakness. We have weaknesses that other people’s strengths reach out to. We are stronger together than we ever are apart. (ID I_16, Respiratory Therapist; 18 Months)
System affective perspective-taking
Participants also described affective perspective-taking as building to encompass a more abstract system level. The system level comprises interacting perspectives across departments, the patient journey, and the hospital and broader community, consistent with how positive emotions can broaden and build across relationships and connections through shared resources and repertoires (Fredrickson, 2001; Pavlovich & Krahnke, 2012).
Patients and members of the community served by the hospital were a focal emotional viewpoint for the system as a whole. The patient’s perspective represented a salient and integrative goal for empathic concern (Litchfield & Gentry, 2010). This viewpoint was at once personal and transcendent, as concern for a customer or user might represent a salient perspective for developing products and services (Dougherty, 1992).
How would you feel? For everybody, we have to remind them that it is personal. . .We experience it every day and forget that community members don’t. We have to put ourselves back in their shoes. (ID I_16, Respiratory Therapist, 18 Months) It is great to get everybody in [and to emphasize] we are all human and it could be our loved one rolling in, because we are in a community and it often is. (ID G_12, Nursing Education Specialist; 18 Months)
System affective perspective-taking was also driven through the organizational culture by displays of openness and commitment from senior leadership, prompting excitement and desire around being involved in authentic communication, and the general sharing of perspectives.
The commitment is important. It comes from senior leadership, part of the culture. If they see it as important, and the message gets pushed to people at the bedside, then it helps everybody be more committed and want to be part of it. (ID I_12, Director of Quality Improvement; 18 Months) The ICU director began by saying, ‘Hey guys, I’m going to throw something out that’s probably not going to feel very good, but I want us to talk about it.’ I am just cheering in my mind. I have been trying for years to get to this. Finally we can talk about things and really talk instead of everything feeling sugar coated and like we’re not getting to the issues. (ID I_14, Chief Nursing Officer; 18 Months)
Local cognitive perspective-taking
In contrast with the concern, openness, and respect of affective perspective-taking, the cognitive dimension was more explicitly focused on imagining and understanding how others were thinking, and not just understanding their knowledge, but relating to it and taking it into account (Litchfield & Gentry, 2010).
Locally, this meant actors learning about the skills and capacities of other actors, what their job roles and tasks involved, and appreciating both the similar and different issues and needs they faced.
Some of the people I’ve worked with before, but some I didn’t know what capacity they had. I knew that they worked in a certain department, but I didn’t know much of what they did. A lot of these people in the other departments have similar issues. That makes it a lot easier for me to communicate with them what I need, and vice versa. (ID D_4, CathLab Manager; 18 Months)
These local cognitive perspective-taking interactions involved seeing ways through various degrees of conflict in terms of closing and bridging gaps between different functionally diverse representations of organizational issues (Cronin & Weingart, 2007).
I butted heads with cardiology extensively at the beginning. They’re the bad guys, we’re the good guys. I see things from their perspective a lot now. Wow, they’re really just trying to do the same thing I am, just from a different angle. (ID B_7, EMS Physician; 18 Months) We worked well together, because I bring in the clinical side and he brings in the statistics side. Because he was an engineer and I’m a nurse, so we each brought in our own perspectives to this and worked really well together. (ID E_4, Quality Improvement Nurse; 18 Months)
Cognitive perspective-taking also appeared in the data as attributional understanding, because typically interactions involved an improved sense of the cause-and-effect of how and why diverse others enacted the views and behaviors that they did. This allows for reduced biases in understanding others, and fairer, more sophisticated cognitive representations and explanations for reasoning about their situations (Parker et al., 2008).
Interactions were grounded in understanding interdependent links in a patient care pathway—“you have a patient that can travel from an ambulance to an ED to a cath lab to a floor to a critical care - multiple people are putting their hands on this patient” (ID C_18, Case Manager; 18 months). Attributions involved discussing underlying causes revealed by increased adoption of local perspectives for problem-solving purposes.
Physicians are collaborating very well with pharmacists because they know the pharmacist is going to be looking at the meds. Our team pharmacist representative will say, ‘Yeah, but that won’t work because. . .’ Well, let’s investigate. . .It’s back and forth, very collaborative dialogue. (ID J_9, Cardiology Practice Manager; 18 Months) You cannot change people's perceptions or behaviors if you don't understand why they're doing what they're doing to begin with or not doing it. You have to know where people come from. Grouping with these different people has made me more aware of things that make other people tick. (ID I_17, Emergency Physician; 18 Months)
System cognitive perspective-taking
The cognitive dimension at the system level reflected an increase in scope, so that understanding covered how and why work was done across the entire system. More shared, holistic accounts of the interdependent knowledge and interactions of the hospital system showed how cognitive perspective-taking could support collective mind in organizations, as attentive to how perspectives constitute the system (Weick & Roberts, 1993).
That’s probably where our biggest challenge is, is getting the staff level in areas to understand how they impact AMI care. It’s not all about the cath lab. There are opportunities to impact that patient’s care at every point along the way. (ID H_7, Quality Improvement Officer; Baseline) We got everybody together to better understand what everybody’s roles were. We’ve done a pretty good job of breaking down some of those walls for the people who thought they understood what we do versus seeing what we actually do. It gave us a broader platform to show what we have been doing and where we can get better. (ID J_12, Pharmacist; 18 Months)
The cognitive processing of interlocking perspectives from across the hospital and health care system resembled the building of a shared understanding of distributed connections, pathways, bottlenecks, overlaps, and differences. Participants were able to attribute hospital problems and solutions to shared or distinctive causes as expressed by different perspectives. Similar perspectives could be connected and validated in common ground, whereas differing perspectives could be meaningfully differentiated, interrogated, and elaborated in relation to overall organizational purpose.
We all have the same amount of pressure, just in different places. Realizing that commonality was key. I feel the pressure of my clock ticking away, get him up to the cath lab. Understanding the cath lab is under the same thing, opening my eyes to the whole experience. (ID B_7, EMS Physician; 18 Months) We have pharmacy, primary care, cardiology, administration, ED. Nursing and physician-side, cath lab nursing, floor nursing, ICU nursing. We have a lot of people at the table who otherwise would never have been, which is big. They can speak up, make suggestions, observations. That applies all over the hospital. (ID A_11, Medical Director of Cardiothoracic Surgery; 6 Months)
Attributional understandings of perspectives moved away from blame and defensive rigidities locating perspectives within particular groups or locales and toward greater appreciation of how data and insights flowed across the connections between perspectives. This clarifies how perspective-taking relates to the cognitive capabilities involved in organizations seeking to map and improve processes and product or service quality.
They are tracking delays and time of discharge from the order until they actually leave. That data has helped us see a bottleneck. Just by having that data through the cardiac educators being involved in all these cardiac patients. That was a a-ha, a good serendipitous moment. (ID C_3, CathLab Director; 18 Months) When we've had disagreements, it's been more of a perspective disagreement from where you are within the system of care, which gives insight as to why that may or may not be a problem. What you realize is there will be a time or limit, constraint, or something that we need to change or find a work-around. (ID A_20, Emergency Department Physician; 18 Months)
Participants also used figurative language to reflect the complexity of system cognitive perspective-taking. Most literally, this included everyone being represented “around the table” or “all at the same table,” but also different “sides,” “ingredients,” and “pieces” of the organization fitting together in a “continuum” relating to multiple aspects of patient care.
I like to use my cake metaphor. You have ingredients and a recipe. You can't make a cake without both, right? There is a lot of ingredients to the discharge process. The recipe changes as a function of who is ordering. There's so many different dimensions to it. . .it's not in your standard flow chart. (ID H_1, Quality Improvement Manager; 6 Months) This has been an excellent opportunity for all of us to sit at the table and make this work to make a difference in these patients. Everybody has their own little piece of the pie working at trying to help this or that. It’s nice to have a group project that has so many different disciplines committed. (ID H_2, Pharmacist; 6 Months)
Local motivational perspective-taking
A final dimension was motivational—the intervention creating necessary conditions for wanting to engage perspectives willingly. Motivation is an important part of building perspective-taking because of the many demands and moderators that can hinder its effectiveness (Ku et al., 2015; Parker et al., 2008). Furthermore, perspective-taking is highly imperfect because people are rarely accurate mind readers (Ickes, 1997), but instead rely on prosocial motivations to improve sensitivity and awareness (Litchfield & Gentry, 2010).
In joining a hospital coalition, participants reported how it addressed various interpersonal motivations to overcome an egocentric point of view. At the local level, participants reported feeling motivated to be included in a significant sharing of perspectives, to listen and learn, to have time and space to think in stimulating ways from other points of view, and the rewarding prospect of building mutual recognition across silos and boundaries.
I have enjoyed the meetings. Sitting in there and watching the interactions. When I have piped up, throwing in my two cents and my questions, I have been taken seriously and listened to, which is nice. (ID J_25, Nurse Case Manager; 18 Months) That cultural change of listening to one another for input—getting input, wanting input—is a big step. (ID A_11, Medical Director of Cardiothoracic Surgery; 6 Months)
The motivational aspect of participation and belongingness in change was fulfilled by being part of a coalition. This created conditions for wanting to learn by engaging with the perspectives of other members, and satisfying curiosity about the limits of one’s own perspective and expertise in relation to others.
I have learned to look at things from very different points of view. Not just my point of view or what is best for my people. To not be so. . .to try to understand what it is going to take for other people to come around. I've become patient with that. Before, I was very impatient. I didn't understand why people couldn't see something I thought was blatantly obvious (ID I_17, Emergency Medical Director; 18 Months) I think that one of the most fun things about LSL is the different perspectives that people bring to the table because you can’t really be the content expert in everything. (ID G_12; Nursing Education Specialist, 18 Months)
At the same time as the intervention generated local motivations for perspective-taking in the coalition, it also made coalitions aware of the levels of motivation required to overcome dynamics of blame, defensiveness, and silos to build trust in ways that would support and sustain perspective-taking.
We had quite some silos we had to dismantle. . .You have to stay with something, no matter how difficult it gets because when you get to the other side, it's so nice. You can talk about anything and it is not defensive and more ‘how can we improve?’ We built trust within the group, and it never was punitive or negative. It was all talking on processes to try to take out the ‘you did something wrong’. (ID I_12, Quality Director; 18 Months)
System motivational perspective-taking
The motivational dimension at the system level emerged from efforts to spread the engagements with a shared perspective and the expansiveness of perspective-taking to support health care growing as a system; through relationship-building, equality, and consensus around important standards. Some coalition members commented on this in terms of other meetings, hospital facilities, and sites across a region.
It has been a very exciting opportunity. . .the entire LSL project. As we continue to grow as a system, to be able to share some of our successes and failures with the other facilities as well and continue to spread some things. (ID H_2, Pharmacist; 6 Months) We had a regional leadership meeting talking about LSL and brainstorming how to improve cardiac care from the time the patient’s picked up until they got here. Good ideas came out of those sessions. (ID F_5, Emergency Department Physician; 18 Months)
A motivation to standardize more effective processes across the system corresponded to a motivation to connect perspectives through common language, goals and information, gaining acceptance, and input into change initiatives along the way.
We are bringing twelve sites in, in addition to all the hospital folks. There’s absolutely going to be shared learning. Standardization of workflows, everybody speaking the same language, looking at the same information and then they can learn from each other. (ID F_11, Associate Chief of Quality and Patient Safety; 18 months) Twenty-eight hospitals. There’s so many people that know this verbiage, they understand what we’re doing. This has been hugely accepted within the region - this patient education tool. Nurses, ICUs are so excited there is finally something that provides patients with good information. (ID F_18, Nurse Coordinator; 18 Months)
Spreading motivational perspective-taking across the system involved dialog and gestures reflecting shifts in the motivations of traditionally powerful perspectives (typically doctors) associated with interventions, and decisions. Openness and responsiveness from these powerful actors signaled that they were motivated and served as motivating to others, who felt listened to and that sharing their perspectives was worthwhile.
I can definitely see Doctor N [a cardiologist] trying to work with his community partners and get involved with EM. The ER asked him for money to help support a barbecue. Rather than saying, ‘it's not my problem’, he is like, ‘how much do you want?’ I have been impressed with their willingness to do whatever it takes to build communication. (ID J_20, Clinical Nurse Specialist; 6 Months) Doctor W is so good at what he does. He also has some very strong opinions. At one of our first meetings, we were trying to determine goals. We were talking about mortality. We were really divided. It was an intense conversation. I think I got him and several other leaders to understand that we do more than exercise patients. (ID H_3, Cardiac Rehabilitation Director; 18 Months)
The motivational direction, intensity, and persistence of trying to share and interpret perspectives across the system gained further momentum as inputs and self-reinforcing feedback loops fed into the same overarching system-wide goals of patient care and reduced mortality. Balanced feedback on how timings and demands of various groups would be affected fed into a motivating cycle of change, improvement, and understanding with reference to system-wide goals and outcomes.
We were giving information back on how patients did, where times were, so they could gauge and work towards improvements. Sometimes you’re not quite aware of timelines for door in your facility, door out, and trying to give them the feedback loop. Also how their patients did. This went really well and your patient did really well. (ID F_3, Physician Assistant, 18 Months) We always want to change, to do things better, but don’t always know how it’s going to affect different groups involved. It is nice to have different people to step up and say, ‘well, if you do this, this is going to be the back fall’. (ID J_21, Emergency Department Liaison; 18 Months)
Discussion and Conclusion
To date, perspective-taking has largely been researched as an individual and interpersonal psychological phenomenon, modified and assessed by laboratory studies, controlled interactions, and self-report surveys (Ku et al., 2015). This field study and change intervention in 10 hospitals is among the first to investigate how dimensions and levels of perspective-taking can unfold, inter-relate, and build up in organizations.
The three dimensions and two levels identified develop management and psychology literature on perspective-taking dimensions and processes by showing the breadth and depth of perspective-taking as a multidimensional cooperative capability. In this view, perspective-taking has mutually reinforcing, complementary affective, cognitive, and motivational aspects that can broaden and build across diverse interactions into richer local understandings and more expansive system understandings of the organization (and beyond). These holistic understandings comprise interconnected perspectives on the main purposes of the organization (better patient care and reduced mortality) and ways of exploring the accommodation and integration of different perspectives on how to achieve those main purposes. This contribution also represents a novel exploration and synthesis of work on the more dyadic/interpersonal experiences of perspective-taking (e.g., Ku et al., 2015; Parker et al., 2008), in conjunction with higher-level, transcendent systems conceptualizations of perspective-taking (e.g., Boland & Tenkasi, 1995; Litchfield & Gentry, 2010; Pavlovich & Krahnke, 2012).
We qualitatively analyzed a 2-year change intervention involving hospitals and coalitions with members diverse in status and function to determine how perspective-taking can be cultivated and emerges after intervals of 6 and 18 months. The intervention shows how interacting people and groups in organizations can come to better understand the diverse experiences and viewpoints of diverse others in terms of different emotions, knowledge bases, and efforts to share and interpret different experiences. The three dimensions of perspective-taking confirm and are broadly consistent with existing work on its affective, cognitive, and motivational foundations in interpersonal interactions (Ku et al., 2015; Parker et al., 2008). However, a more substantive contribution lies in articulating mutually reinforcing links between levels and dimensions of perspective-taking that build and spread beyond local, interpersonal interactions. As a whole, the framework suggests that perspective-taking builds and emerges in response to intervention as a relational and intersubjective process, establishing itself more widely as perspectives are more consistently exchanged across a wider ecological system of functions and organizations.
These findings also develop conceptual frameworks suggesting how perspective-taking develops at more collective levels through communication, connection, and integration (Boland & Tenkasi, 1995; Litchfield & Gentry, 2010; Pavlovich & Krahnke, 2012). At the same time, we concede that the current framework was developed in a relatively inductive and exploratory way, based on secondary analysis of an intervention that was primarily concerned with organizational change and cooperative problem solving rather than perspective-taking per se. While this allowed us to investigate perspective-taking in a field setting as a by-product of this broader intervention, it also means the framework should be subjected to further research and refinement to confirm its integrity and contingencies in other settings. For instance, because the study design was derived from a broadly uniform, positively perceived change intervention, it did not allow us to investigate perspective-taking variations and growth patterns across hospitals, units, and time points in a more detailed process-driven or critical manner.
Indeed, perspective-taking represents a complex psychological capability, with many conditions and mechanisms affecting its processes and interpersonal outcomes (Galinsky et al., 2005; Ku et al., 2015). In organizations and systems, this study shows that wider shared engagement with perspective-taking is likely to rely on intergroup contact experiences, knowledge sharing, shifting power relations, integrative goals, and distributed agency. At their best, perspective-taking and feelings of empathy can fit together in positively reinforcing relationships with other virtuous behaviors shown by managers, leaders, and other change agents, such as altruism, compassion, and inclusion, with potential ripple effects for interconnected organizational stakeholders and beneficiaries, as was the case for hospital staff and patients in this study. At the same time, we cannot fully rule out demand characteristics and impression management in our findings, as participants responded positively to the aims and spirit of the intervention, and focused on positive changes they might have wanted to believe or demonstrate. However, the consistencies across the relatively large sample and the fact that the intervention reduced mortality rates over the 2 years in 6 of the 10 hospitals mitigate against such explanations (Curry et al., 2015, 2018). While the remaining four hospitals still showed broadly comparable evidence of perspective-taking, the lack of reduced mortality rates in these organizations suggests that perspective-taking may not always shape effective outcomes as part of a wider culture change, where boundary conditions around diversity, conflict, and interactive encounters merit further research attention.
The study also highlights the difficult choices facing perspective-taking research on a larger scale in organizations, around disentangling interrelated aspects of the experience, and associated interventions. Future research should therefore continue to explore the multiple differentiated layers and dimensions of perspective-taking processes, which can vary in how authentic, effortful, emotional, conscious, accurate, and altruistic they are (De Waal, 2008; Ickes, 1997; Tuazon et al., 2021). For instance, potential downsides and limitations have been proposed, where perspective-taking can become too emotionally involved, and be based on perceptual error, antisocial motivations, or varying levels of cognitive elaboration (Galinsky et al., 2005; Litchfield & Gentry, 2010). Clearly, perspective-taking is not necessarily a panacea for cooperation and harmony. This study indicates this in terms of the persistence and resource investments involved in the intervention. Committed participation was crucial for working through emotional reactions, defensiveness, silos, rigidity, and misunderstandings encountered at earlier stages.
Unless fostered appropriately, perspective-taking and empathy may be viewed as illegitimate or misguided, and need to be weighed against related concepts like justice and compassion, which have clearer ethical foundations and rationales (Bloom, 2017). Furthermore, perspective-taking difficulty, effort, and effectiveness are likely to vary according to different targets and distances across the groups and divisions of an organizational system. Closer observational methodologies, alternative interview protocols, and critical perspectives focused on power relations may be helpful for probing these nuances of perspective-taking experiences. Our findings also suggested that in health care settings, some perspectives have more integrating force and salience as rallying or reference points, such as patients and high-status doctors. In future research and other settings, similar consideration might be given to focal leadership perspectives, customer or beneficiary perspectives, and competing perspectives of particular minorities and departments, depending on the aims of researchers.
It was also challenging in the current research to isolate and disentangle components of a complex intervention and their distinct effects on perspective-taking. While findings confirm that the intervention was largely successful in fostering perspective-taking among many of the participants, it involved a variety of participatory components and varied forms of implementation. These included different experiences that could shape perspective-taking capabilities, such as process improvement workshops within hospitals, annual conventions across hospitals, and ongoing remote support through technological systems.
Fine-grained understandings of perspective-taking in organizations remain challenging given the complex, varied frameworks and debates around its aims, processes, and results. Here, we have developed theory and data aligned primarily with relatively recent literature in management and social and organizational psychology on major perspective-taking dimensions and levels. However, future research should continue to study other potential field settings, activities, and applications. For instance, perspective-taking interventions are often discussed in relation to diversity training exercises (Pendry et al., 2007), but are still under-researched in terms of how or why they achieve their objectives. Perspective-taking capabilities are implicated in health care and other high-reliability settings, where interventions often involve collective leadership, distributed responsibilities, and integrated safety cultures (Buchanan et al., 2007; Vogus et al., 2010). These practices enable, enact and elaborate the exchange of diverse perspectives by encouraging sustained attention to important viewpoints and experiences (Vogus et al., 2010). More quantitative perspective-taking research in organizations can establish its nomological network and construct validity alongside other influential constructs underpinning positive sharing of perspectives, including trust, psychological safety, and learning.
The findings of this study have practical implications for whole-system change programs and organizational systems attempting relational adaptations across levels and boundaries. Findings suggest that shared and organized perspective-taking needs supportive structures and processes which place importance on all three dimensions. Interventions should encourage interacting people and groups to understand the diverse experiences and viewpoints of diverse others in terms of different emotions, knowledge bases, and efforts to share and interpret different experiences. In doing so, over time, people are more likely to relate to different perspectives on how to achieve the main purposes of the organization and explore the accommodation and integration of different perspectives on how to achieve them more effectively.
Furthermore, interventions should emphasize the importance of recognizing and encouraging both local level perspective-taking interactions between pairs of people, and coalitions and meetings where system-level perspective-taking experiences involve building a shared appreciation of multiple perspectives in aggregate across groups and agencies. Practices might include protected time for problem-solving, diverse change coalitions, sharing of data and evidence, and deliberately open, egalitarian sharing of views associated with roles, functions, and hierarchies. While challenging to align and sustain, these conditions reflect relatively low risk, low cost supports for many organizations. Leaders and facilitators can attend to multiple, interrelated dimensions and levels of perspective-taking in framing these practices. A variety of organizational actors with different perspectives can be involved as change agents, enabling them to work enthusiastically across boundaries to make improvements and process a range of views and details (Dattée and Barlow, 2017).
Addressing the social positions of change agents can help to shift profession-centric mindsets outward by exposing actors “to other organizational and professional perspectives” (Lockett et al., 2014, p.1125). This suggests a balance between the power to influence change and the proximity to promote it across perspectives, between elites and the front line, suggesting the socialization and development of mid-level status groups will be crucial to perspective-taking efforts (Lockett et al., 2014). Building an integrated organization around common connections entails bringing people together in sufficient numbers with time to appreciate similar outlooks and priorities and develop sustained change (Vogus et al., 2010).
In this way, perspective-taking also has important practical implications for the social psychology and foundations of organizational design and interdependence, suggesting that people in today’s organizations have to come together more to deliberate on how their differing tasks, goals, and knowledge affect the design of workflows (Raveendran et al., 2020). Perspective-taking highlights the affective, cognitive, and motivational challenges associated with such exercises, in terms of managing silos and distances between teams and roles, and the motivations to cross boundaries from insider to outsider, and vice versa. This study suggests actors benefit from being able to oscillate between the personal and the transcendental in perspectives, the local and the system, as they try to understand and imagine other points of view. The study also suggested the benefits of caucusing—assembling various perspectives and identity groups in different configurations over time to discuss conflicts, problems, and relationships (Fiol et al., 2009; Haslam et al., 2003).
In conclusion, this study shows how organizations can make appropriate framings and investments for developing shared perspective-taking capabilities across dimensions and levels by trying to integrate and adapt an ecosystem of perspectives toward greater overall purpose, learning, and improvement. Perspective-taking constitutes a particular kind of emergent organizational adaptation experience, and with the proper conditions in place to support it, organizations can maximize the promising potentials (Ku et al., 2015).
Footnotes
Declaration of Conflicting Interests
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study and data collection were supported in part by funding from a research grant from The Medicines Company, Parsippany, NJ, USA.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.