
Abstract
Objective
To explore the use of shared decision-making (SDM), a collaborative approach to care between healthcare providers, patients, and their families, in cleft lip and/or palate (CL/P) care.
Design
PubMed, CINHAL, Embase, and Dentistry & Oral Sciences Database were searched for studies reporting on SDM in CL/P pediatric care (<19 years). There were no restrictions on date, language, or study design other than case studies and systematic reviews.
Results
A total of 13 studies were included. Overall, parents reported high levels of perceived involvement in SDM. Pediatric patients shared this view, though the desire for SDM was age-dependent with patients expressing a greater desire for involvement as they aged. Qualitative data revealed 4 main themes, including understanding and knowledge of cleft care and treatment, factors influencing decision-making and patient autonomy, psychosocial and emotional dimensions in decision-making, and moral responsibility and identity in decision-making.
Conclusion
The current study highlights that SDM is valued by parents and patients in CL/P care. Further research is needed to understand how SDM can be more clearly integrated into routine CL/P care. Specifically, studies should explore the gap between perceived and actual involvement using standardized SDM measures, as well as identify key barriers and enablers to effective implementation.
Background
Cleft lip and/or palate (CL/P) patients face complex, staged treatment plans that require long-term multidisciplinary care and several decisions that significantly impact functional, aesthetic, and psychosocial outcomes. Because of this, the importance of shared decision-making (SDM), defined as a collaborative approach to care between healthcare providers, patients, and their families/caregivers that balances patient values and goals with scientific evidence, has gained increased attention. 1 SDM has been conceptualized through numerous models that outline how patients and clinicians collaborate during healthcare decision-making. While large variability exists among these models, the most consistently reported components include describing treatment options, making the decision, patient preference, deliberation, creation of choice awareness, and learning about the patient. 2 These model components are often described as a stepwise process in which clinicians first make explicit that a choice exists, then share information about options and outcomes, explore patient preferences, and deliberate together to reach a decision. 3
While early decisions in CL/P care are typically made by caregivers, as patients transition through childhood and into adolescence, their involvement in care may evolve as they mature. Existing qualitative studies suggest that children and adolescents with CL/P desire a greater role in their care decisions than they are often given. 4 Although most children show this desire for their opinions to be valued in decision-making, parental perspectives on whether and how much children should be involved in care remain inconsistent.4,5 However, youth who feel included in surgical decision-making report greater satisfaction with both the decision process and its outcomes, and greater self-esteem.6,7 Furthermore, the SDM approach to care reduces decisional conflict, increases knowledge of care, decreases psychosocial difficulties, and, in some cases, increases satisfaction with care.7,8
Despite the relevance of SDM to cleft care and pediatric patients’ desire for involvement in surgical decision-making, there is limited information on how SDM is applied in this clinical context and whether it meaningfully improves outcomes. A systematic review was performed to evaluate the existing literature on SDM in cleft care, with the goal of identifying the use of SDM in CL/P care, defining SDM themes in this context, and highlighting areas to inform the development of future care models or interventions that enhance patient-centered care.
Materials and Methods
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews (PRISMA) 2020 guidelines. 9
Eligibility Criteria
We included studies with children and adolescents (along with their families/caregivers) with syndromic or non-syndromic CL/P receiving surgical or multidisciplinary (dental treatment, speech therapy, etc) care. Randomized control studies, cross-sectional studies, observational studies, and qualitative studies were included. Studies that reported on care without SDM and/or adult patients (>19 years old) were excluded.
Search Strategy
The search strategy was developed with the assistance of a medical librarian. PubMed, CINHAL, Embase, and the Dentistry & Oral Sciences Database were searched from the time of their inception to September 11, 2025, with no language restrictions (Supplemental File 1). Additionally, a grey literature search was conducted. 10 The retrieved documents were uploaded to Covidence (Veritas Health Innovation, Melbourne, Australia), and duplicates were removed. Abstract and full-text screening was performed against inclusion/exclusion criteria by 2 independent reviewers, and disagreements between the 2 reviewers were resolved through discussion and by consultation with the senior author. Reasons for study non-eligibility were documented by the reviewers. Reference lists of included articles were screened with backward and forward citation searching to identify any additional relevant studies that met the inclusion criteria.
Risk of Bias Assessment
The risk of bias assessment was performed by 2 independent reviewers using standardized Joanna Briggs Institute (JBI) critical appraisal tools, as appropriate. 11 JBI tools provide a structured approach to evaluating methodological quality and identifying potential sources of bias. Any disagreements arising between reviewers were addressed through discussion. Regardless of quality, all studies were included in the analysis.
Data Extraction
Data extraction was performed by one author using an a priori data extraction form, and checked by at least one other author to ensure accuracy. Data extracted included author, country, publication year, intervention, study design, outcomes of significance to the study review question, and specific objectives. Any disagreements arising were resolved through discussion.
Data Analysis
Study descriptions and characteristics were summarized. Due to heterogeneity in survey measures, scales, and questionnaires, quantitative findings were described narratively. Qualitative data was analyzed using a thematic synthesis as described by Thomas and Harden. 12 This 3-stage process was utilized as it was designed to analyze data pertaining to individuals’ perspectives and experiences and is commonly used in SDM literature.13,14 This approach applies principles of thematic analysis while retaining the integrity of the original study findings, thereby enabling effective aggregation of recurring themes across studies. 15 First, reported themes, subthemes, and supporting participant quotations were extracted from the included studies. Second, extracted themes were reviewed and inductively coded to identify patterns and areas of conceptual overlap across studies. Finally, related codes were grouped into overarching analytical themes that synthesized findings across the included articles. The analysis was conducted by one author and reviewed by a second author to enhance reliability.
Results
Study Characteristics
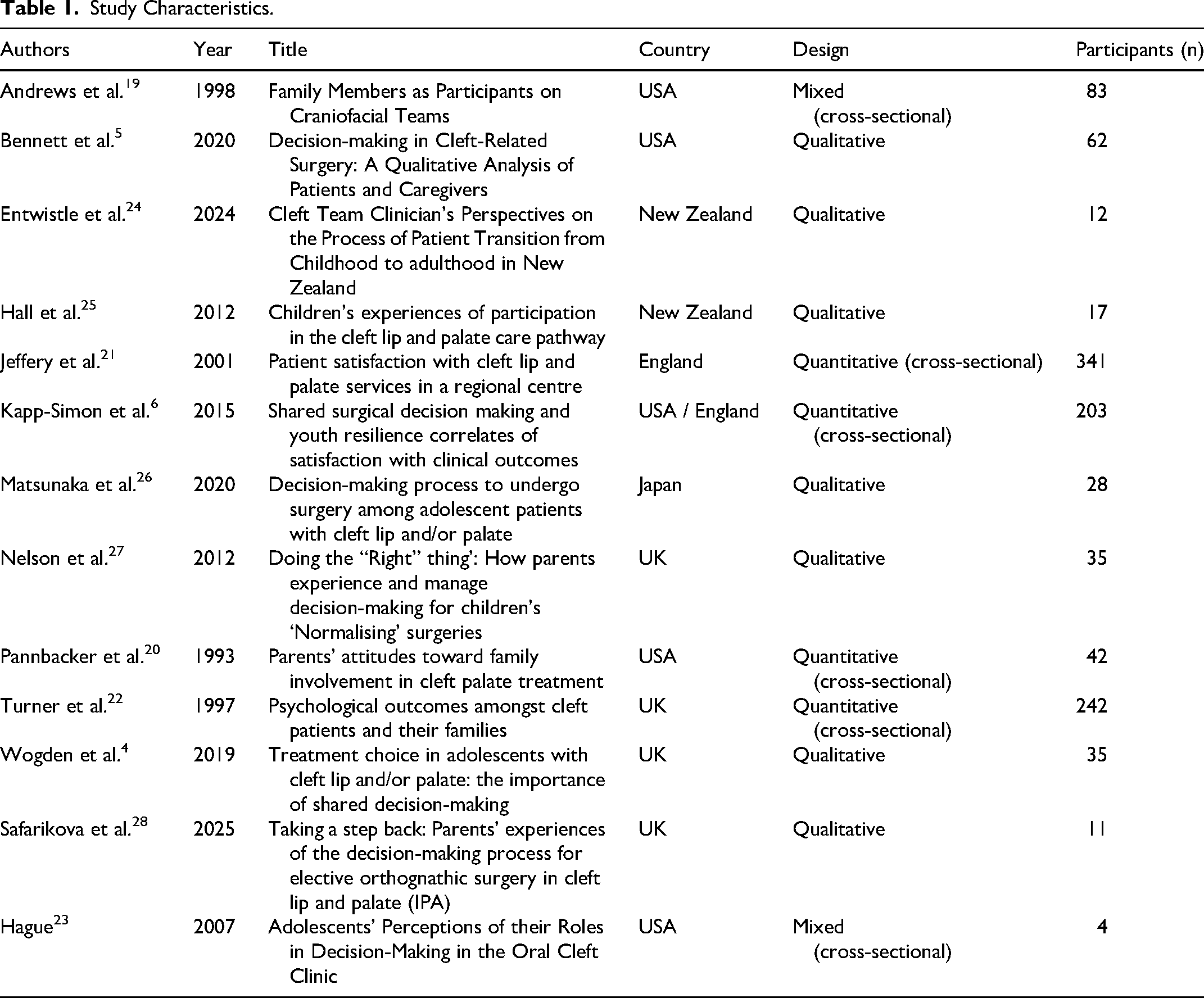
The search strategy revealed 1820 articles. Of 1378 screened studies, 37 were assessed, and 13 were included from 1993 to 2025. Studies used qualitative (n = 7), cross-sectional quantitative (n = 4), or mixed-methods (n = 2) designs and represented 1115 participants with 92% from English-speaking countries (Figure 1).
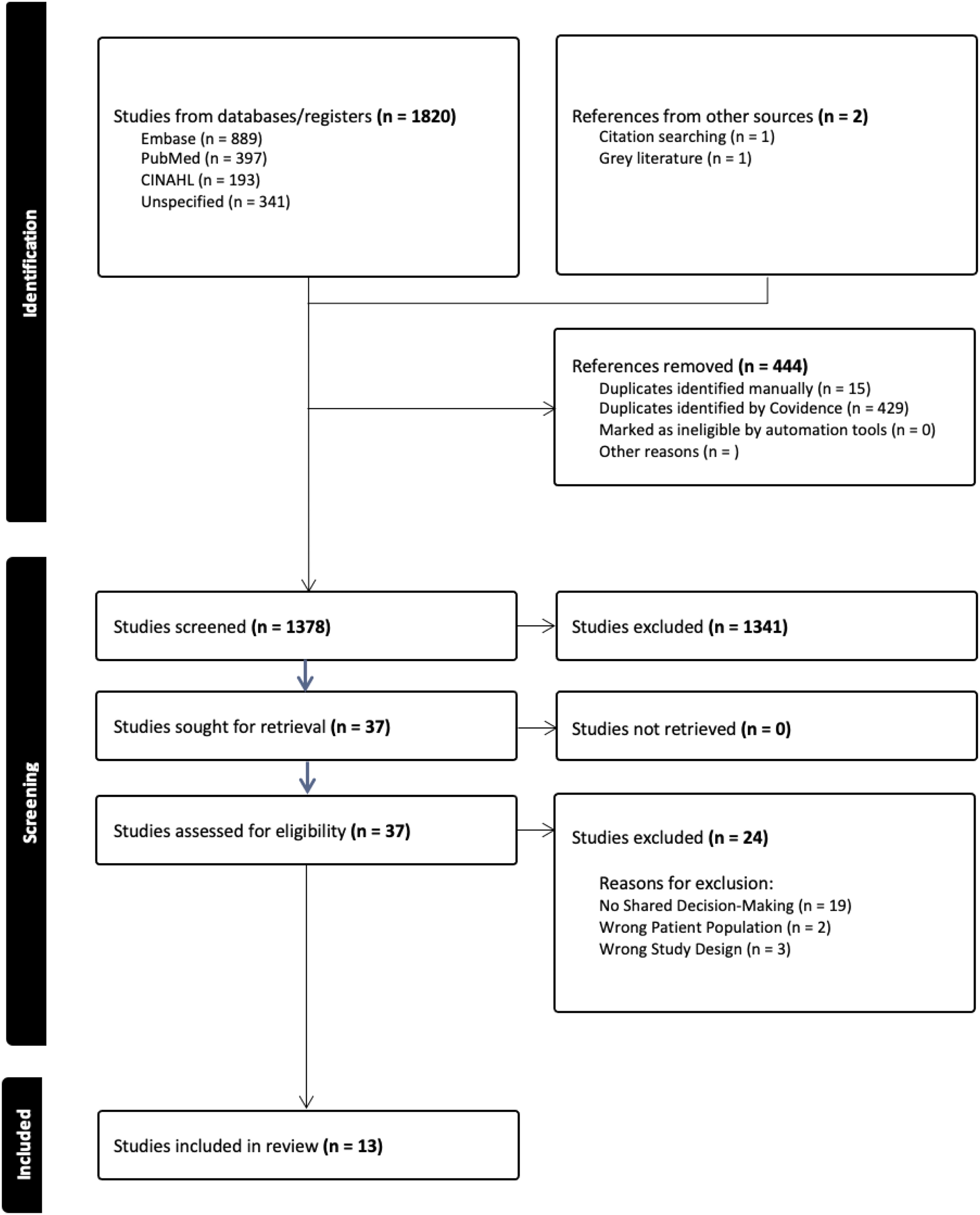
Flowchart detailing study screening and inclusion process based on PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). 9
Risk of Bias Assessment
Articles that met the inclusion criteria were critically appraised for risk of bias using JBI tools as appropriate to their study design. Two studies were evaluated using the checklist for analytical cross-sectional studies. 16 Both studies were assessed as high quality, achieving full scores of 8. Four studies were appraised using the checklist for prevalence studies, 17 with scores ranging from 5 to 7 out of 9. Lower scores in this group were primarily attributable to whether the sample was appropriate for the population, uncertainty of the suitability of participant recruitment strategies, and adequacy of sample size. The remaining 8 studies were evaluated using the tool for qualitative studies 18 and scored between 7 and 10. The most common methodological limitation, identified in 7 of the included qualitative studies, was the omission of the researchers’ cultural or theoretical positioning, as well as insufficient reporting of the potential influence of the researcher on the research process, thereby limiting the ability to evaluate study-level bias.
Description of Quantitative and Mixed-Methods Studies
All 6 studies that examined and reported quantitative data on SDM in CL/P used survey designs, but there was heterogeneity in the data due to differences in target populations, survey measures, questionnaires, and response scales. Participants included patients, their families/parents/caregivers or a combination of both with the sample size ranging from 4 to 341. Across studies, quantitative data primarily assessed perceived involvement in decision-making, desire to participate, comfort levels, autonomy, and alignment between parents and children. Given the variability in measurement tools and response scales, findings are summarized narratively below.
Parents consistently reported high levels of perceived involvement in decision-making. In one study, parents were asked about the following items: “I was part of the decision-making process with the team” and “I felt comfortable participating in the team meeting”; the median scores were 4.13 and 4.49, respectively, on a 5-point Likert scale. 19 Similarly, 91% of parents reported participating in treatment decisions, yet 36% wished they had more opportunity to participate in decision-making. 20 This was also displayed in another study reporting that 30% of parents felt they wanted to be more involved in treatment planning decisions, 21 but the remaining 70% felt they were able to participate in what felt like the right amount. In the same study, 37% of parents felt very involved, and 45% felt they were fairly involved. 21
Four studies asked children ranging from 3 to 18 years about their current involvement in SDM. Patient-reported data revealed moderate levels of participation and desire for participation in decision-making. One study found that the child's preference for involvement in care depended on age, with adolescents aged 15-18 being more likely to desire SDM compared to those aged 11-14. 6 Another study found that 23% of 15-year-old patients felt excluded from treatment planning as parents or specialists were perceived as the primary decision makers. 22 A study on adolescent participants found that when asked “I already make decisions about my cleft” and “I will be ready to make decisions about my cleft when I turn 18,” found a median score of 1.25 and 1.67, respectively, with 2 indicating strongly agree and −2 indicating strongly disagree. 23 Comparably, a study exploring factors related to involvement in decision-making found that participants aged 15-18 years were more involved in decision-making compared to those aged 11-14 years, regardless of sex. 6
Overall, the quantitative findings across studies converge with parents and patients reporting overall involvement in decision-making within CL/P care providers. Parents and children report current involvement in treatment and express a continued desire for SDM. There remains a gap between desired participation depending on child age; however, as youth transition to adolescence, there is consistency in desire for greater autonomy. Parents broadly feel comfortable and included in treatment decisions, but in one study, 52% reported that they perceived their participation as only slightly effective (Table 1). 20
Study Characteristics.
Thematic Analysis of Qualitative Studies
A thematic analysis was conducted to synthesize findings from the included qualitative studies, resulting in 4 overarching themes, as illustrated in Table 2. One study included clinicians (n = 12), one included health care professionals (n = 5), and the remaining studies included patients (n = 81) and/or their parents/caregivers (n = 106).
Summary of Thematic Synthesis Analysis.
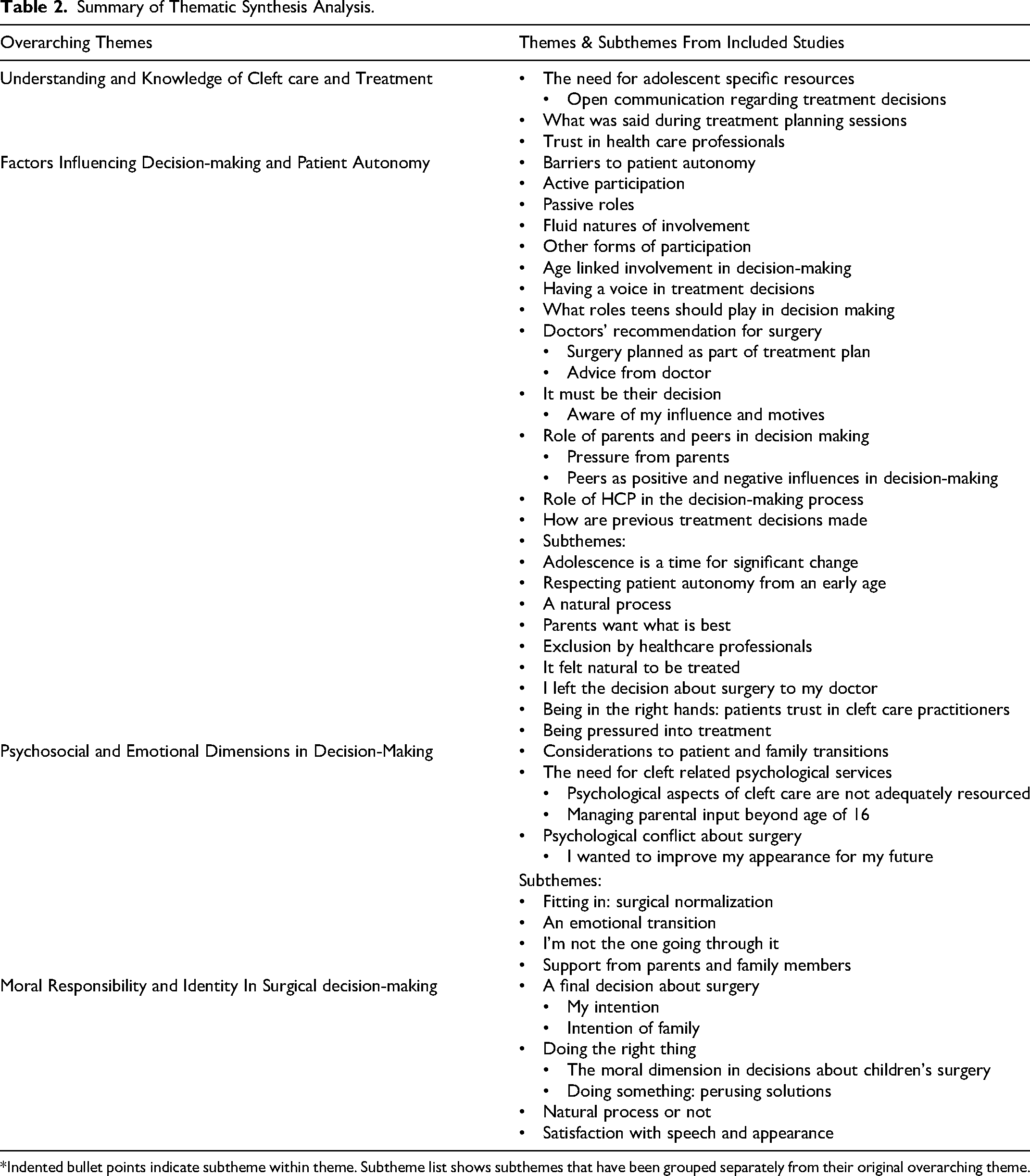
*Indented bullet points indicate subtheme within theme. Subtheme list shows subthemes that have been grouped separately from their original overarching theme.
Theme 1: Understanding and Knowledge of Cleft Care and Treatment
Firstly, understanding and knowledge of cleft care among patients and parents were largely shaped by their interactions with healthcare providers. Factors such as length of appointment and frequency of follow-up, as well as trust and a strong therapeutic relationship, were identified as important foundations for SDM: Where there is uncertainty or inconsistency between patients and their families, and the procedure in question is non-urgent, we offer more consultations until we all feel convinced that this is the way forward. This usually results in success for the whole family unit. (Participant 10)
24
One study investigated what was said by patients and their families during treatment planning sessions and identified broad themes such as making treatment decisions and attempting to gain information about their care.
23
Health care professionals also highlighted a need for more adolescent-specific resources to assist with the implementation of SDM. Poor understanding is a barrier, good understanding is a facilitator… I would imagine that the kids that have sort of grown up with a better understanding of cleft might have an easier time taking a bit more ownership over that decision-making.
24
Theme 2: Factors Influencing Decision-Making and Patient Autonomy
Another key theme that was identified was the various factors that influence a child's autonomy. Many children expressed a desire to be involved in decision-making, but the extent of this involvement varied. Some felt that the decision should ultimately be theirs, whereas others requested the support of their parents and health care providers: What I would like in my treatment would be for me, if it comes down to it, if I want to say yes or no to what's going to happen.
23
I like my mom to help me decide about that, like if I should have it done.
23
In contrast to this, some children felt that surgery was something they would likely undergo at some point, a perspective often shaped by the expectations of their parents and health care providers. I've been going to this hospital since I was young, so it just seemed like part of the flow. There was an expectation that ultimately I would have the treatment. (Boy, 18)
26
Age played an important role, with greater involvement seen as patients aged and demonstrated increased capacity to understand their decisions, though the exact age at which this transition occurred is subjective and inconsistent across studies: I feel when I was younger it was more of an adult's decision (especially as a baby) but we get more freedom to choose as we get older …from about seven. (YP6 aged 17 years)
4
Peers also played a role in shaping school-aged children's attitudes toward surgery. Parents emphasized that it was the child who would experience the procedure and thus the final decision should ultimately rest with them. Healthcare providers were seen as valuable contributors to decision-making, but participants emphasized that their involvement was most effective when there was an established sense of familiarity and trust.
Theme 3: Psychosocial and Emotional Dimensions in Decision-Making
Psychosocial and emotional aspects of the decision-making process were viewed as highly important but often not adequately attended to in cleft care. Clinicians highlighted the need for ongoing psychosocial support, particularly as children mature and face the emotional challenges associated with shifting decision-making responsibility from their parents to themselves.
Children identified motives behind surgical decisions, including aspects of their physical appearance and self-esteem. Me, my parents and my orthodontist decided together for me to have braces as I wanted a better smile and have more self-esteem. (YP3, aged 15 years)
4
Throughout this process, parental support was consistently identified as a key factor in helping children navigate these complex experiences and decisions. My mother is the biggest supporter [ … ]. My mother would always go to appointments with me and help us and the HCPs discuss treatments together. (YP7)
4
Theme 4: Moral Responsibility and Identity in Surgical Decision-Making
A final theme that was generated was the concept of moral responsibility and identity in surgical decision-making. Parents described a strong sense of moral responsibility to “do something” for their child, balancing this drive with a desire to ensure that any decision aligned with what was genuinely best for them: It's fairly simplistic, the choices we had were to do something about it or not and you can’t not do anything, so you have to do something. (Father of Tom aged 11 months).
27
These considerations often intertwined with questions about who should make the final decision, highlighting the moral tension between parental duty, child autonomy, and the pursuit of psychosocial well-being. In several studies, participants identified aspects of identities, such as social pressures and societal beauty standards as motivating factors to undergo treatment. It's only with the other kids bullying her and saying things that got her thinking can you have this done, would it make any difference? We can only say we don’t think you need it - you’re beautiful as you are - it's other people that haven’t seen what you’ve gone through, or experienced what you’ve come through. (Father of Kelly aged 17 years)
27
Parents also highlighted that it is a natural process for their children to take a greater responsibility in their care as they become able to understand the implications of their decisions. This transfer of responsibility provided relief for some participants and strong emotions related to a loss of control for others. It sounds really awful, but in a way it was a little bit of a relief. Because as a parent with a child that needs treatment it's all on you. I’ve got to make this decision. What if I make the wrong one? (Pat)
28
Discussion
This systematic review aimed to provide a summary of the current literature surrounding the role of SDM in cleft care between parents, children, and healthcare providers. Across studies, parents consistently reported a high level of involvement in the decision-making process, though some expressed a desire for greater involvement. Children and adolescents reported moderate involvement that was age-dependent, with older patients expressing a greater desire to be included in the decision-making process. Qualitative analysis identified trust and communication among patients, parents, and healthcare providers as central to the SDM process. Parents described a tension between wanting to do what is best for their child and respecting their growing autonomy. Children were also influenced by peers and broader societal norms, which shaped their desire to undergo certain procedures. Together, these findings highlight the shared desire for patients, families, and their healthcare teams to be involved in the decision-making process as a team. This demonstrates a need for more consistent psychosocial support to help families navigate the emotional and social factors that shape cleft-related treatment decisions.
The studies included in this review focused primarily on the current prevalence of SDM in cleft care. All the studies reported findings on perceived levels of SDM as experienced by patients and their families, rather than observed SDM by researchers during a clinical encounter. Furthermore, many SDM perception measures may be subject to ceiling effects, as parents and patients often rate SDM highly for reasons such as reluctance to criticize clinicians or overstating their child's emotional well-being, making it difficult to determine how meaningful these measures truly are. This underscores the importance of using mixed methods, triangulating data, and directly observing clinical interactions to ensure a greater accuracy of reported SDM frequency in a clinical setting. It should therefore be noted that perceived use of SDM following a clinical appointment may not always be representative of the true prevalence of SDM.
Given the lack of standardized SDM measures, it is difficult to ascertain if parents and patients understood what truly constitutes SDM, as opposed to merely having some involvement in the appointment. The inconsistency across measures and scales utilized to quantify SDM and patient and parental involvement in decision-making also made it difficult to perform quantitative analysis of data. Moving forward, the development and use of standardized questionnaires to assess the role of SDM in CL/P care is required.
The studies included in this review focused primarily on what is currently happening in CL/P clinics. Given that parents and children expressed a desire to be more involved in the decision-making process, further research is needed surrounding the potential barriers or enablers to the implementation of SDM protocols in cleft clinics. The child's desire to be involved, as well as the evolution of their role as they age, also needs to be considered. These insights will support the development of strategies to integrate SDM into routine care for all patients and families. Following implementation, standardized measures should be developed and utilized to evaluate the utilization and efficacy of SDM in these clinical spaces.
Conclusion
Given that CL/P treatment requires numerous procedures and decisions with meaningful effects on a child's function, appearance, and psychosocial well-being, SDM supports patients, families, and clinicians in discussing options and developing care plans aligned with patient values. Our findings suggest that SDM is valued during clinical encounters by patients and their families. While most participants reported feeling involved in decision-making, no studies reported on direct observations of SDM during clinical encounters. We note that there may be a difference in perceived SDM and actual use of SDM, especially with a lack of standardized SDM questionnaires. Future research is needed to explore the implementation of SDM in clinical care and comparison of SDM in settings using standardized questionnaires. This will help to inform how SDM can be best used in improving the quality of care for patients and their families receiving CL/P care.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656261453332 - Supplemental material for A Systematic Review of Shared Decision-Making in Cleft Care
Supplemental material, sj-docx-1-cpc-10.1177_10556656261453332 for A Systematic Review of Shared Decision-Making in Cleft Care by Alicia Reil, Reann Post, Paul Hong and Michael Bezuhly in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgments
The authors would like to thank Darlene Chapman for her contributions to the literature search.
Author Contributions
AR: study design, data collection and analysis, manuscript preparation; RP: data collection and analysis, manuscript preparation; PH: study design, manuscript preparation; MB: study design, data collection and analysis, manuscript preparation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Protocol Registration
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.