
Abstract
Objective
To assess the surgical protocols followed in the treatment of non-syndromic UCLP across Indian cleft centres and identify factors influencing secondary surgical outcomes.
Design
Prospective cross sectional design.
Setting
The study was conducted in 14 sary/tertiary care comprehensive cleft centres.
Participants
The study included 307 patients with non-syndromic UCLP across three age groups (5, 12, and 20 years) from 14 centres nationwide.
Outcomes
Data was collected through a standardized web-based form. Variables recorded included surgeon specialty and experience, surgical sequence, presurgical orthopaedics, primary surgical techniques, and their association with the need for secondary procedures such as lip/nose revision, velopharyngeal surgery, fistula repair, and alveolar bone grafting. Descriptive statistics were generated, and associations between variables were analysed using Fisher's exact test.
Results
Millard's technique was the most commonly used approach for primary lip repair across all age groups. Presurgical orthopedic plates, nasal conformers, and the specific lip repair technique were not significantly associated with the need for lip or nasal revision surgery, although the wide confidence intervals indicate considerable uncertainty in these estimates. Similarly, the type of palatal repair and use of intravelar veloplasty were not significantly associated with fistula formation or the need for secondary velopharyngeal or fistula repair procedures. Across centres, wide variation existed in techniques used, but no one approach showed superiority in reducing secondary surgery needs.
Conclusion
Despite the observed variability in surgical weak associations were found between specific surgical techniques or surgeon-related factors and the need for secondary surgical interventions. The wide confidence intervals highlight the uncertainty of these findings and the need for further national-level audits, underscoring the challenge of establishing best practices in cleft care without robust systems for comprehensive data collection and consolidation.
Introduction
To evaluate and improve the healthcare services, standardized measurement of outcomes is a fundamental prerequisite. 1 Recognizing the complex and varied nature of craniofacial anomalies and their associated morbidities, both the American Cleft Palate-Craniofacial Association and the World Health Organization have emphasized the importance of continuous monitoring and standardization of surgical procedures in the management of cleft lip and palate (CLP), a developmental anomaly with a variable prevalence.2–5 This approach supports effective intervention and the delivery of evidence-based care, but also contributes to improved patient outcomes.2,3
Recognising the limited availability of nationwide audits and the increasing need to align clinical practice with evidence-based interventions in cleft care, two major multicentre initiatives, the Eurocleft project in Europe and the Americleft project in North America, were undertaken in the past two decades.6,7 Both initiatives were prompted by the findings of the CSAG study, which led to significant restructuring of cleft care services in the UK. These large-scale audits examined regional variations in the burden of cleft conditions, surgical and orthodontic care pathways, and patient and parent satisfaction relative to deformity severity and treatment outcomes.6–8 Their results revealed considerable discrepancies in surgical protocols, underscoring the wide variation in practice patterns even within individual countries.6–8
The Asian subcontinent reports the highest prevalence of CLP globally.4,5 India, being the most populous country and a developing nation, contributes substantially to this global burden. Despite the high demand of healthcare services, access to quality and affordable surgical care including cleft management, remains limited in many regions of the country.5,9 While the Smile Train initiative has significantly transformed the landscape of CLP care in India, offering free surgeries and raising awareness, India lacks a dedicated national level cleft outcomes audit. 10 This critical gap was addressed with the launch of the Cleft Care India Study (CCIS), a multi-centric initiative aimed at not only systematically collecting and analysing the national burden of non-syndromic unilateral CLP (UCLP), but also at documenting the orthodontic, speech, and surgical care provided to patients across the country.
Previous publications from CCIS have reported the methodology in detail, and evaluated the other outcomes of unilateral CLP patients managed at the participating centres (work submitted for publication consideration). 11 The present work aims to identify the surgical protocols followed in the management of patients with non-syndromic UCLP, with a focus on exploring the various factors influencing surgical outcomes.
Method
This study was approved by the Institutional Ethics Committee (approval no. 18/2279/JMI/IEC/2020) on 10 November 2020 at the Data Coordinating Centre and individual ethical committee approval at each of the participating centres. All participants provided written informed consent prior to enrolment in the study. This research was conducted ethically in accordance with the Declaration of Helsinki.
A total of 14 centres from different regions of the country participated with each centre contributing surgical pre-orthodontic data for at least 30 non-syndromic cleft patients. To ensure uniformity across centres, a standardized data collection protocol was developed, and data was prospectively collected via a dedicated web portal. The portal captured information on the educational background and clinical experience of the operating surgeon. Detailed surgical history for each recruited patient, such as techniques used, age at surgery, bone grafting (if performed), and presence of oronasal fistula (if any) were also collected.
Patients with non-syndromic UCLP were included. Cases with a Simonart's band were eligible if the band measured less than 5 mm in width. Patients with incomplete or isolated cleft lip or palate were excluded.
Prior to data entry, designated personnel from each centre underwent rigorous training and were calibrated to ensure consistency in data collection. The data collection forms were pilot tested prior to study initiation. Each centre was required to submit records for at least 10 patients in each of the following age-based groups: Group I: 5 years ± 6 months, Group II: 12 years ± 6 months, and Group III: 20 years ± 6 months.
All Statistical analyses were undertaken using Stata v18. Frequency distribution and percentages was computed for all the categorical variables while associations between these variables were evaluated using Fisher's exact test. P-value <0.05 was considered to be statistically significant.
Results
5-Year-Olds
A total of 76 patients aged five years were included in the analysis. Eighteen patients (23.7%) received pre-surgical orthopaedic (PSO) treatment using plate appliances, of whom 12 (66.7%) used extraoral strapping and 4 (22.2%) did not have any strapping. Data on strapping were unavailable for the remaining two patients. In the remaining 58 patients (76.3%), the appliance was either not used or information regarding usage was not recorded. Among those who received PSO, three patients (16.7%) continued appliance use up to the time of palatal repair.
Information on the sequence of surgical procedures was available for 56 patients. Of these, 45 patients underwent a staged protocol involving primary lip repair followed by a combined repair of the hard and soft palate as a second intervention. A two-stage approach involving lip and anterior palate repair as the first surgery, followed by hard and soft palate closure as the second intervention, was undertaken in 11 patients. Both lip and palate surgical procedures were most commonly performed before the age of one year, with the mean age at lip repair being 0.45 ± 0.86 years and at palatal closure 0.85 ± 0.92 years.
Information regarding primary lip repair was available for 54 patients (71.05%). Among these, 28 (51.85%) were operated by oral and maxillofacial surgeons and 26 (48.10%) by plastic surgeons. The majority of procedures were performed by surgeons with more than two years of experience (n = 49; 90.74%). Primary rhinoplasty was predominantly undertaken without nasal conformers (n = 47; 87.04%). In the few cases where conformers were used, they were typically fitted one week postoperatively (n = 5; 71.43%).
Separate muscle layer dissection was documented in 33 patients (61.11%), while a vomerine flap was used in 11 patients (20.37%). No postoperative complications were recorded in 48 patients (88.89%), although data were missing for five patients (9.26%).
Millard's rotation-advancement technique was the most frequently used approach for lip repair (n = 41; 75.93%), followed by the Afroze technique (n = 4; 7.41%). The choice of primary lip repair technique did not demonstrate a statistically significant association with the need for secondary lip or nasal revision, secondary velopharyngeal surgery, or fistula formation (p > 0.05; Table 1).
Effect of Pre-Surgical Orthopedic Treatment and Factors Associated with Primary Lip Repair on Secondary Surgical Procedures in 5-Year-Old.
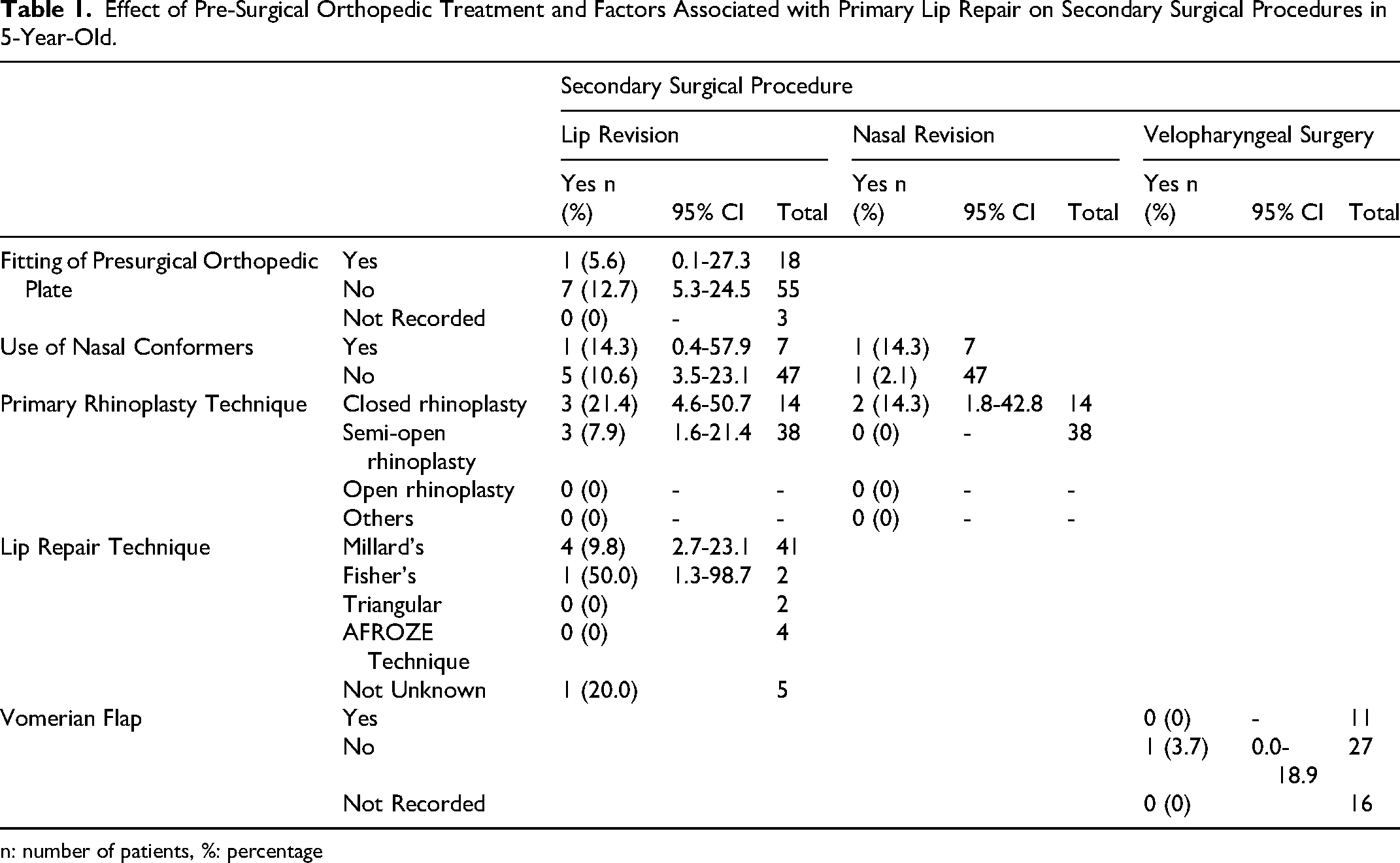
n: number of patients, %: percentage
Palatal repair was performed in 52 patients (68.42%), most commonly by oral and maxillofacial surgeons (n = 29; 55.77%). Surgeons with more than two years of experience undertook the procedure in 47 cases (90.38%). Intravelar veloplasty was carried out in 29 patients (55.77%), although procedural details were not documented for 15 cases (28.85%). Subperiosteal palatal dissection was the most frequently reported technique (n = 27; 51.92%), predominantly in conjunction with Langenbeck flaps (n = 18; 34.62%) or Bardach's two-flap technique (n = 16; 30.77%).
Postoperative complications occurred in four patients (7.69%), each with a different manifestation: dehiscence, surgical site discharge, fistula, or incomplete closure. Complication data were unavailable for an additional four patients (7.69%). Fistulae were documented in 13 patients (17.11%), although only four (30.77%) were symptomatic, reporting food impaction, nasal regurgitation, or increased nasal discharge. The hard palate was the most common site affected (n = 5; 38.46%), with fistula sizes ranging from 1 to 4 mm.
The effect of presurgical orthopaedics, lip repair and palate repair on the need for secondary surgical procedures, presence of fistula or fistula location showed a really wide confidence intervals, highlighting the uncertainty in the results. The lack of power restricted the use of statistics to calculate the significance level (Table 2).
Effect of Factors Associated with Palatal Repair on Need for Secondary Surgical Procedures and Site of Fistula Formation in 5-Year-Old.
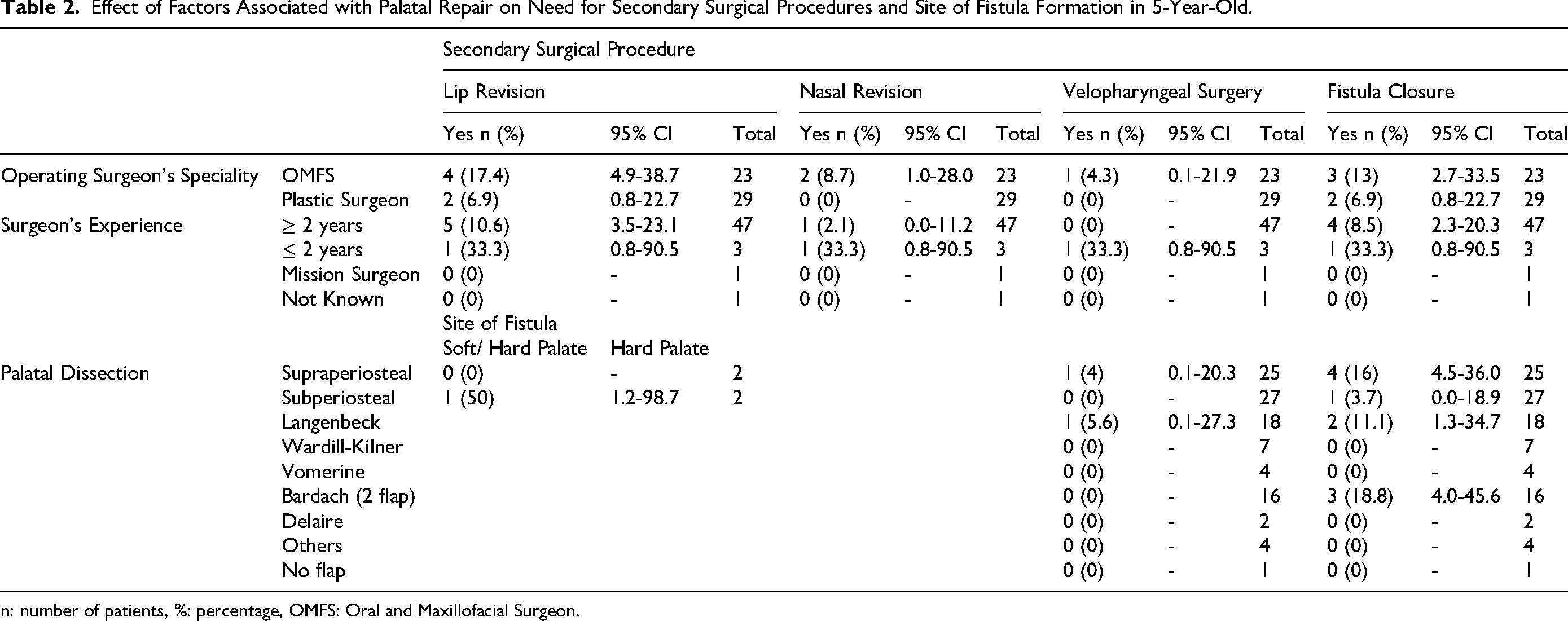
n: number of patients, %: percentage, OMFS: Oral and Maxillofacial Surgeon.
For 12-Year-old
A total of 165 patients aged twelve years were included in this analysis. Of these, five patients (3.03%) had received pre-surgical orthopaedic (PSO) appliances, with two (40.0%) also using extra-oral strapping. In the remaining cases, PSO appliance use was either not undertaken or not documented.
Details on the surgical sequence were available for 105 patients. The most frequently reported protocol was a staged approach consisting of primary lip repair followed by combined hard and soft palate closure (n = 59; 56.19%), with the mean age at lip repair being 0.79 ± 1.61 years. A two-stage approach involving lip and anterior palate repair as the first surgery, followed by hard and soft palate closure as the second intervention, was undertaken in 11 patients (10.48%). A three-stage protocol beginning with lip adhesion, followed by definitive lip repair and subsequent palatal surgery, was also recorded in 11 patients (10.48%). Additionally, lip repair combined with soft-palate closure as the initial procedure, followed by hard-palate closure as the second procedure, was performed in 10 patients (9.52%).
Among the 12 year old age group, primary lip repair surgical information was documented in 94 patients (56.97%). Most procedures were performed by plastic surgeons (n = 71; 75.53%), followed by oral and maxillofacial surgeons (n = 18; 19.15%), with the majority of surgeons having more than two years of experience (n = 74; 78.72%).
Primary rhinoplasty was infrequently undertaken in this cohort, with 76.6% of respondents (n = 72) reporting no surgical nasal intervention. The use of nasal conformers was exceptionally uncommon, documented in only one patient (1.1%).
Separate muscle layer dissection was recorded in 35 patients (37.23%), and a vomerine flap was utilised in 11 patients (11.70%). No postoperative complications were reported in 88 patients (93.62%). Millard's rotation-advancement technique was the most commonly employed method for lip repair (n = 64; 68.09%), followed by the triangular flap technique (n = 15; 15.96%).
There was no statistically significant association between the primary lip repair technique and subsequent outcomes, including the requirement for secondary lip or nasal revision, velopharyngeal surgery, or the presence of an oro-nasal fistula (p > 0.05; Table 3).
Effect of Pre-Surgical Orthopedic Treatment and Factors Associated with Primary Lip Repair on Secondary Surgical Procedures in 12-Year-Old.
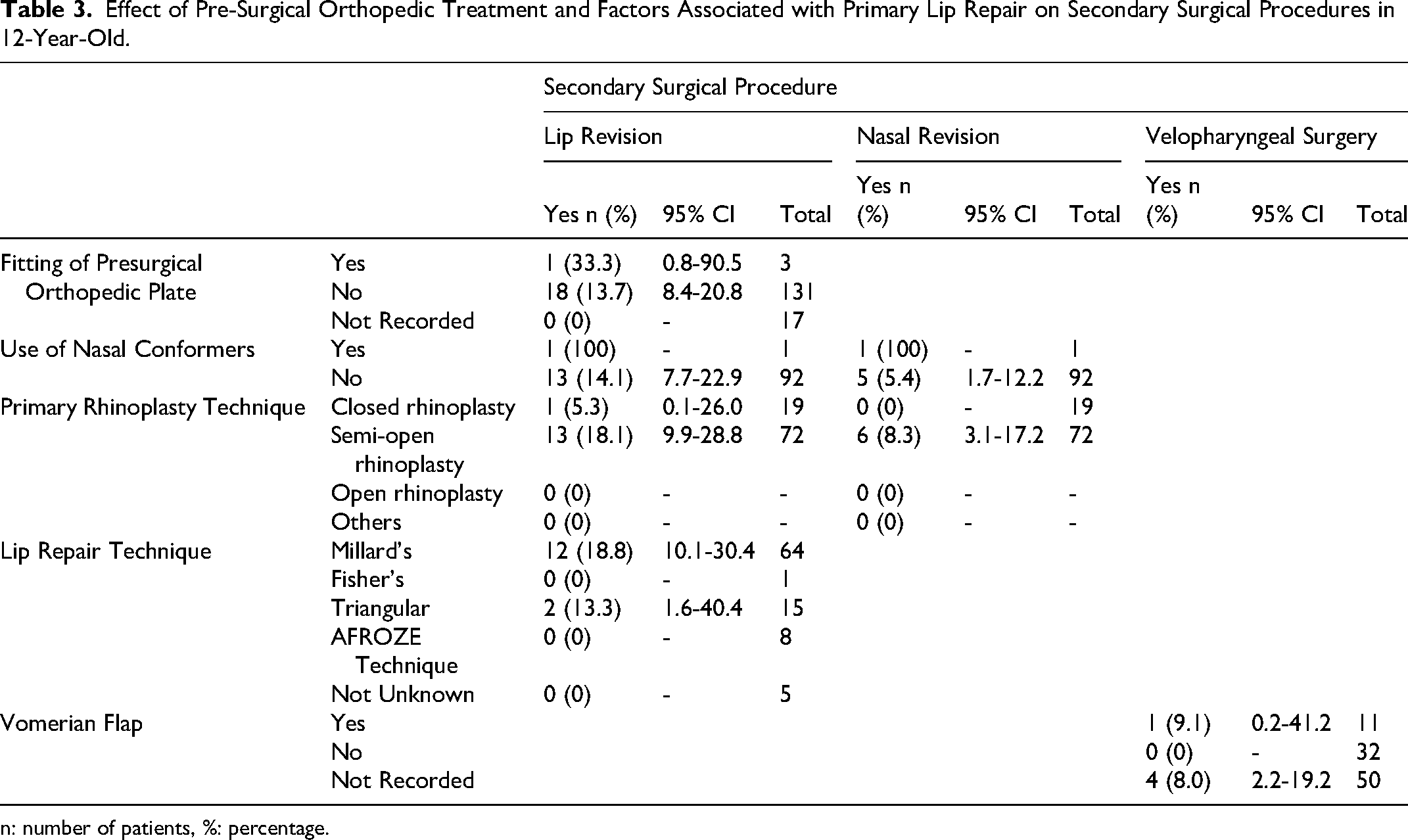
n: number of patients, %: percentage.
Palatal repair surgical information was available for 79 patients (47.88%). The surgery was predominantly carried out by plastic surgeons (n = 59; 74.68%), with the vast majority having more than two years of surgical experience (n = 67; 84.81%). Intravelar veloplasty was documented in 34 patients (43.04%). However, procedural details were unavailable for 39 patients (49.37%). Supraperiosteal palatal dissection was the most commonly reported technique (n = 42; 53.16%), and the Langenbeck flap (n = 25; 31.65%) and Bardach two-flap technique (n = 38; 48.10%) were the most frequently utilised flap designs.
Regardless of the technique employed, fistula formation or the requirement for repeat palatal repair was noted in 10 patients (12.66%). Overall, oro-nasal fistulae were present in 23 patients (13.94%), with more than half reporting associated symptoms such as nasal discharge, nasal regurgitation of liquids, or food impaction (n = 12; 52.17%). The hard palate was the most commonly affected site (n = 12; 52.17%), and the recorded fistula size ranged from 1 mm to 10 mm.
The effect of primary surgeries and presurgical infant orthopedics on the need for secondary surgical procedures, presence of fistula or fistula location showed wide confidence intervals in the results, undermining the overall precision of the results. (Table 4).
Effect of Factors Associated with Palatal Repair on Need for Secondary Surgical Procedures in 12-Year-Old.
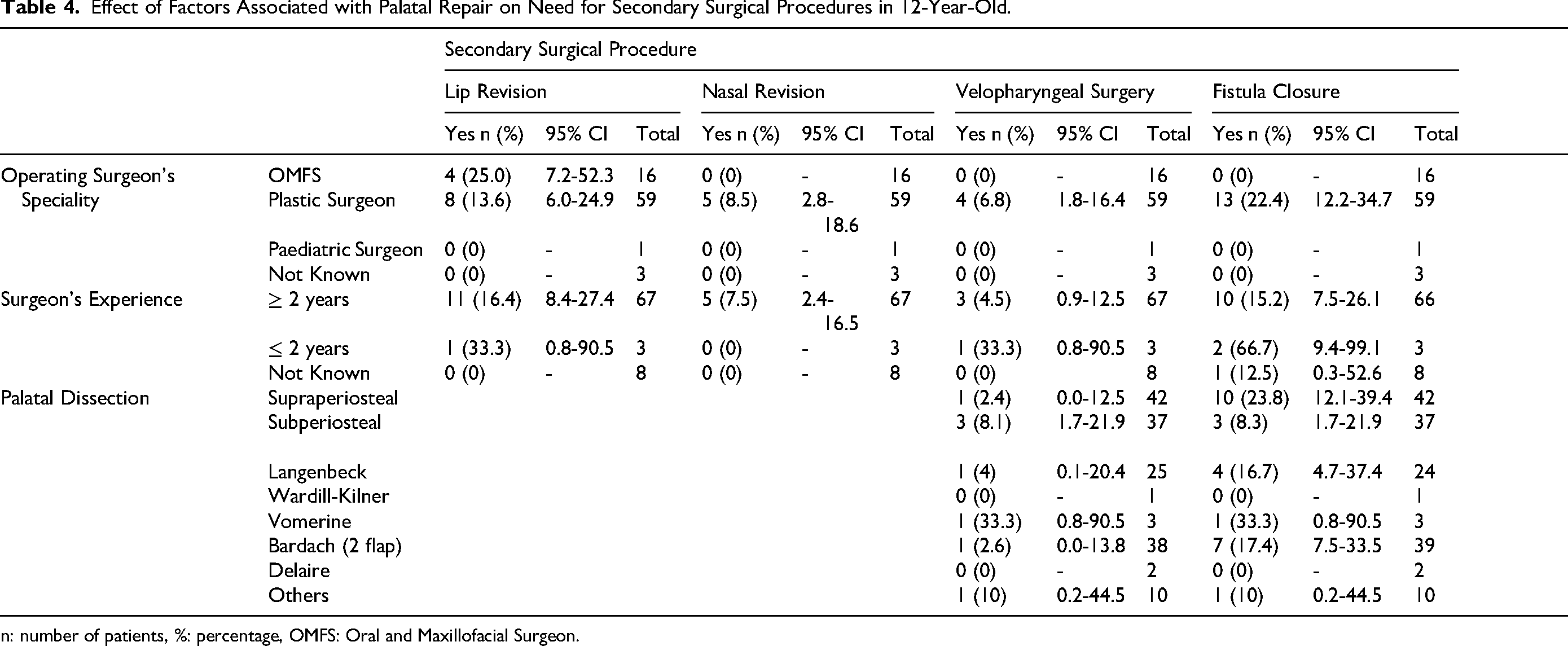
n: number of patients, %: percentage, OMFS: Oral and Maxillofacial Surgeon.
For 20 Year old
A total of 66 patients aged 20 years were reviewed. Of these, only two patients (3.03%) had received a presurgical orthopedic plate. Three distinct surgical sequences were identified for lip and palate repair in this age group. An initial lip repair followed by hard and soft palate repair was the most common surgical sequence. The ages for lip and palate surgeries were not reported for 51 patients (77.27%) and 63 patients (95.45%), respectively. In the remaining small cohort, the mean age for lip surgery was at 1.53 ± 2.72 years, and for palate repair was 2.33 ± 1.52 years.
Details of primary lip repair were available for 21 patients (31.82%). Most procedures were performed by plastic surgeons (n = 11; 52.38%), and all surgeons had a minimum of two years of experience. Primary rhinoplasty was undertaken in 21 patients (31.82%), although nasal conformers were used in only one case (4.76%). Muscle dissection as separate layers was performed in six patients (28.57%), and a vomerine flap was utilized in four patients (19.05%). No complications were reported for any of these procedures. Millard's technique was the most commonly used method (n = 9; 42.86%), with the remaining techniques showing relatively even distribution. There was no statistically significant association between the lip repair technique and the requirement for secondary surgical procedures (p > 0.05; Table 5).
Effect of Pre-Surgical Orthopedic Treatment and Factors Associated with Primary Lip Repair on Secondary Surgical Procedures in 20-Year-Old.
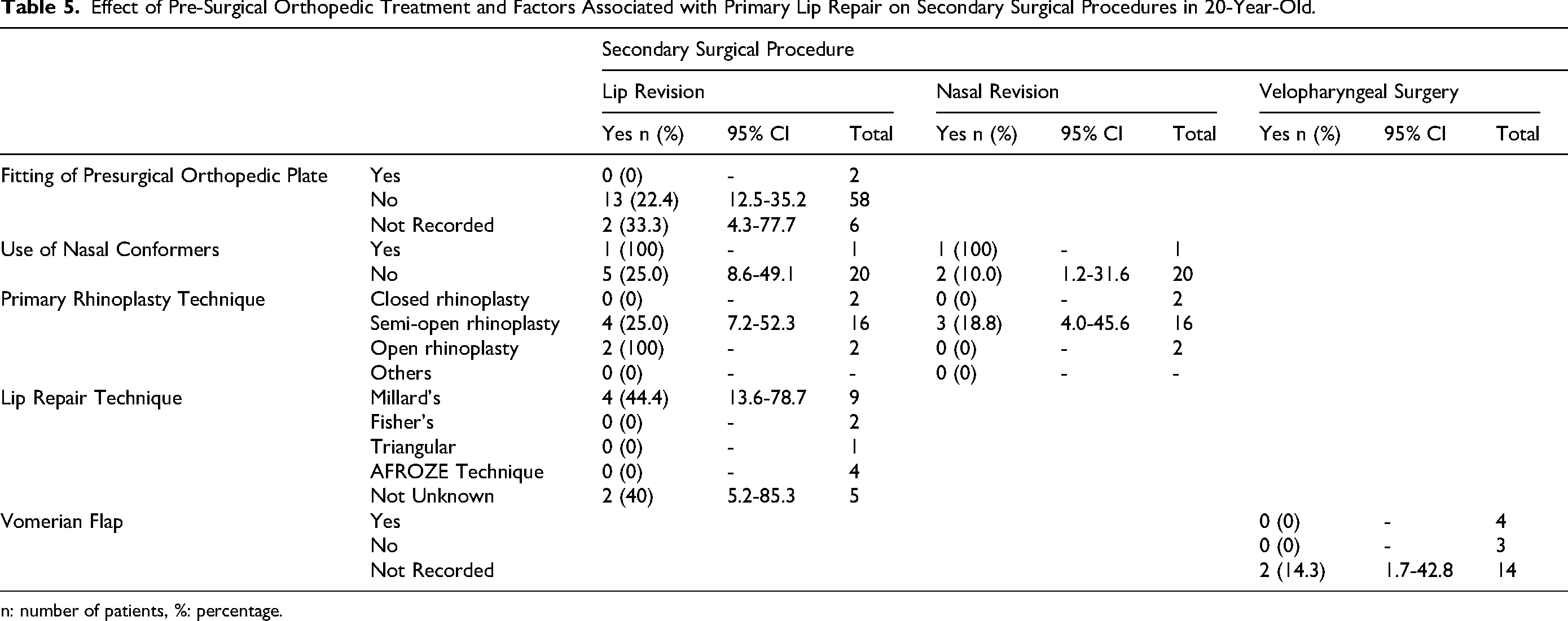
n: number of patients, %: percentage.
Primary palatal repair was documented in 19 patients (28.79%), with procedures performed by plastic surgeons in nine cases (47.37%) and oral and maxillofacial surgeons in seven cases (36.84%). Intravelar veloplasty was undertaken in 11 patients (57.89%), and subperiosteal palatal dissection was the most frequently employed approach (n = 13; 68.42%). The Bardach two-flap technique was the most common flap design (n = 8; 42.11%). Postoperative complications were minimal, with 17 patients (89.47%) reporting no issues. Fistula formation was absent in 57 patients (86.36%). Among patients with fistulae, the hard palate was the most frequently affected site (n = 5; 55.56%), with defect sizes ranging from 0.5 to 6 mm.
The results from statistical analysis on the need for secondary surgical procedures, presence of fistula or fistula location showed a really wide confidence intervals, highlighting the uncertainty in the results. (Table 6).
Effect of Factors Associated with Palatal Repair on Need for Secondary Surgical Procedures in 20-Year-Old.
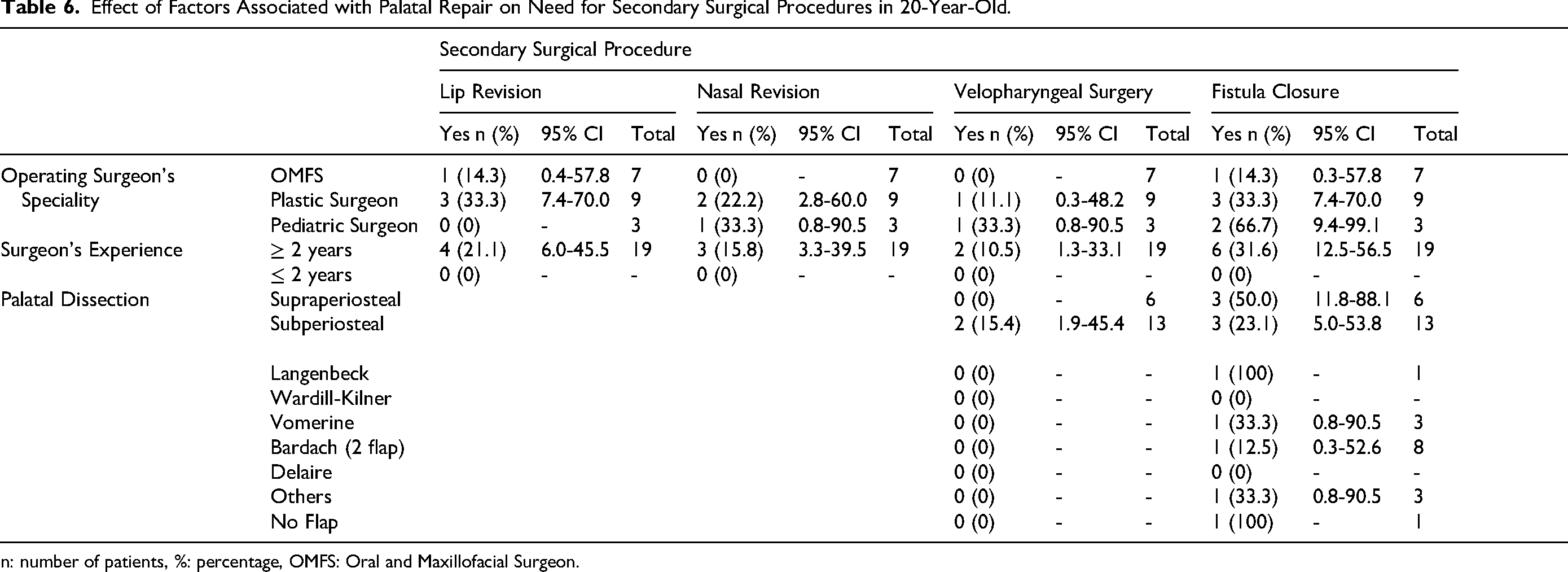
n: number of patients, %: percentage, OMFS: Oral and Maxillofacial Surgeon.
Discussion
The present study found no significant association between the use of a presurgical orthopedic plate and the need for lip revision surgery. Across all three age groups, a higher proportion of patients did not undergo lip revision surgery regardless of whether a presurgical orthopedic plate had been used.13,14 While the presurgical orthopaedic treatment is gaining more popularity and its use is largely increasing among cleft centres, there is substantial variation in clinical protocols and is often influenced by institutional practices and surgeon preference, contributing to ongoing debate regarding their standardized use.12,13 Additionally, the evidence on their use from long term studies are also lacking. 14 A similar pattern was observed in relation to the use of nasal conformers and the subsequent need for lip and/or nasal revision surgeries, with both variables showing no statistically significant associations and a high proportion of patients not requiring secondary revisions. Our observations are consistent with those reported by Garland et al., who emphasized the difficulty in drawing definitive conclusions about the long-term benefits of presurgical orthopedic interventions, largely due to heterogeneity in patient management strategies. 15
There was considerable variation in the type of lip repair technique employed between centres, with no statistically significant association between the specific technique used and the subsequent need for revision surgeries across any age group. The choice of technique is frequently influenced by the surgeon's training, experience, and individual preference.16,17 The rate of lip revision surgeries is found to have a heterogeneity. Contrasting the reported increase in secondary revision surgeries, we found that most patients reviewed in our study did not require these revision surgeries, irrespective of the primary lip repair technique used.6,18 Among the different lip revision surgical techniques, Millard's rotation-advancement method emerged as the most commonly adopted, consistent with previous reports in the literature.16,17 The results of the present study are in accordance with findings of Americleft data that reported no statistically significant association despite the variation in need for revision surgeries. 19 These variations may reflect differences in surgical expertise, case complexity, or the presence of additional anomalies.
The present study was limited in statistical power due to the small sample size, which restricted our ability to detect the effect of primary surgeries on secondary revision procedures. The wide confidence intervals observed in the data reflect the uncertainty of the estimates and precluded formal statistical significance testing. Therefore, these findings should be considered exploratory and hypothesis-generating rather than definitive. This limitation is consistent with other cleft audits, where retrospective data similarly constrained the ability to draw firm conclusions.19,20
The surgeon's preferred technique for either lip or palate repair, their specialty, or their level of experience, showed a statistically significant association with the need for lip or nasal revision surgery. These factors also lacked significant association with the need for secondary velopharyngeal surgery or fistula closure. This trend was consistent across all age groups evaluated in the study. Surgeons from varying specialties, including plastic surgery and oral and maxillofacial surgery, as well as those with differing years of clinical experience, demonstrated comparable outcomes with respect to secondary revision procedures. These findings may suggest that revision surgery outcomes may be more strongly influenced by patient-specific factors, such as the severity and morphology of the cleft, rather than by the surgeon's specialty or seniority. However, drawing this conclusion with wide confidence intervals remains controversial. It is important to point out the sample obtained in the present study may not be large enough to account for the variation in the surgical techniques followed and the number of surgeons involved.
The presence of fistula incidence varies widely, ranging from 0–60%. This can be influenced by several factors, including the surgeon's experience, preferred technique, extent of the cleft, timing of surgery, concomitant presence of cleft lip, and any associated syndromes.22,25 While some studies suggest that fistula formation following primary repair can be predicted based on the surgical technique employed, this remains a matter of debate.21–24 Importantly, it is universally agreed that a treatment failure rate of approximately 10% is generally not considered high, further underscoring the complexity of care rather than a deficiency in surgical outcomes
Given the variability in cleft presentation, no single surgical technique fits all cases, and the final choice rests with the operating surgeon based on intraoperative findings. Despite these variations, most techniques have yielded favourable results, as reflected in this study. Although data in the CCIS was prospectively collected, certain details were frequently missing from submissions by participating centres, a limitation also noted in the Eurocleft and Americleft projects.8,26 As seen in those initiatives, achieving complete data from all centres is challenging. By compiling data from centres across different regions of India, the CCIS has highlighted heterogeneity, which may, in turn, reflect underlying region-specific barriers to cleft care.27,28 This analysis extends current evidence and highlights the need for a customised national cleft database capable of capturing regional variations in care delivery and outcomes.
The present study shows that there is no common protocol followed by centres across India. Currently, the choice of surgical care is largely provider-driven. However, there is a growing need for an evidence-based, outcome-driven approach that empowers clinicians to make informed decisions based on the comparative advantages and limitations of each protocol. 29
Limitations
A key limitation of this study is its reliance on retrospectively collected data from patient records for primary surgeries. While the majority of patients underwent surgery at their designated treatment centers, some data were missing, primarily due to patients having received their primary surgery at different institutions. Due to the limited statistical power of our sample, we opted to present the data using confidence intervals rather than statistical significance tests for each outcome. Additionally, the sample sizes for the 5 and 20 year old groups were small, reflecting the cleft review protocol in Indian cleft centres, where the first multidisciplinary review typically occurs around seven years of age. Furthermore, 20 year old patients are usually discharged before this age unless they are undergoing extended orthognathic treatment.
Conclusion
The most common surgical sequence reported was staged lip repair followed by hard and soft palate repair. There was no statistically significant association between the use of a presurgical orthopedic plate and the need for lip revision surgery. No statistically significant association was identified between the lip or palatal surgical technique used and the subsequent need for revision surgeries in any age group assessed. Reported fistula incidence demonstrates wide variability across studies.
Although surgeon specialty, experience level, and the surgical sequence employed did not demonstrate any statistically significant effect on primary surgical outcomes or the need for secondary interventions, these results should be interpreted with caution as they may not fully reflect real-world clinical variation. Further national-level audits comparing outcomes between centres are required to ensure consistent delivery of high-quality, evidence-based cleft care across the country.
Footnotes
Acknowledgements
We thank Smile Train India for their extensive support with the study. We thank Ms Mamta Carol for supporting us during the development stage. We would also like to thank Akila Bharatha Mahila Seva Samaja (ABMSS) and Government of India for their support with the study.
ORCID iDs
Ethical Approval and Consent
This study was approved by the Institutional Ethics Committee (approval no. 18/2279/JMI/IEC/2020) on 10 November 2020 at the Data Coordinating Centre and individual ethical committee approval at each of the participating centres. All participants provided written informed consent prior to enrolment in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Scheme for Promotion of Academic and Research Collaboration (SPARC), Government of India and UK India Education and Research Initiative (UKIERI), United Kingdom (Grant No: P1025)
UK-India Education and Research Initiative, Scheme for Promotion of Academic and Research Collaboration, (grant number P1025).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Grant Number
SPARC project No: P1025