
Abstract
Objective
To explore the relationship between sleep behaviors and language development in children with cleft lip and palate (CP ± L).
Design
Cross-sectional analysis of questionnaire data from a national cohort study.
Results
Parental concern about sleep was low overall (13.0% at 18 months, 7.9% at 3 years), but higher in children with RS and syndromic diagnoses. At 3 years, parents of children with cleft palate were more likely to be concerned about sleep than those with cleft lip only (P = .009). Reports of sufficient sleep were high (>88% across all ages), but children with RS showed a decline over time. Significant positive correlations were found between sufficient sleep and language outcomes at all ages (τ = .087, P = .004 at 18 months; τ = .131, P = .002 at 3 years; τ = .445, P < .001 at 5 years). At 5 years, this association remained after controlling for confounders (r = .347, P < .001).
Conclusions
Sleep behaviors were associated with language development in children with CP ± L. These findings highlight the need for longitudinal and interventional studies to better understand the role of sleep on developmental outcomes in this population.
Introduction
Sleep is understood to play a key role in the acquisition of language over childhood. Children who get adequate, high-quality sleep tend to have stronger language abilities1,2; and sleep deprivation can hinder a child's ability to focus, process language, and engage in meaningful social interactions. 3 Being born with a cleft lip and palate puts children at risk of multiple difficulties including speech, language, and hearing disorders,4–7 and also sleep disordered breathing.8–10 This paper aims to explore the relationship between sleep and language in children born with congenital cleft lip and palate.
Congenital cleft lip and palate is the most commonly occurring craniofacial birth defect worldwide, with a prevalence of approximately 1 in every 1000 live births. 11 Orofacial clefts result from incomplete fusion of tissue that forms the palate and/or upper lip in utero; they can occur unilaterally or bilaterally and can involve part or all of the soft and hard palate. Speech outcomes in children born with cleft palate +/- lip (CP ± L) are well documented with 60.2% of children achieving speech within the normal range by age 5-years. 4 Persisting speech errors may be attributed to either ongoing structural anomalies or mis-learning as a result of earlier structural anomalies before surgical palate repair. While articulatory speech errors can be fairly well accounted for in this population, there is also evidence to show that children born with CP ± L are at risk of language difficulties such as understanding what is said to them and forming sentences that contain accurate vocabulary and grammatical structures.7,12,13 Language differences between children with CP ± L and those without are seen across receptive and expressive domains. Although these differences tend to fall within a standard deviation of the population mean, 7 they are both statistically and functionally important. Language difficulties can be a contributory risk factor in a child's underachievement in academic and vocational outcomes 14 ; social-emotional development 15 ; and later life outcomes. 16 As such, the language deficit seen in children with CP ± L is an important issue to understand.
The underlying mechanisms which impact language development in children with CP ± L are not fully understood and are likely to involve multiple factors. Two possible contributory factors are, firstly, high incidence of conductive hearing loss in children with CP ± L 6 as a result of structural abnormalities in palatal muscles that contribute to the opening of the eustachian tube 17 ; and secondly, reduced opportunity for babble in children who receive late palate repair.18,19 The current study will explore the hypothesis that sleep quality over the toddler and pre-school years is another potential candidate to play a significant role in the etiology of disordered language in children with CP ± L.
Our understanding of the relationship between language development and sleep over childhood has grown rapidly over the past decade. Experimentally, infants, 20 preschoolers, 21 and children22–24 perform better on tests of new word learning when that learning is followed by a period of sleep, compared to an equivalent time awake. Observationally, duration of nighttime sleep positively predicts concurrent receptive vocabulary in preschoolers, 2 and in infants this measure prospectively predicts receptive vocabulary at school entry.1,25 Clinically, sleep disordered breathing (SDB), which fragments sleep and results in repeated episodes of hypoxia, is associated with weak phonological skill, 26 as well as difficulty processing complex verbal requests in preschoolers 27 and expressive vocabulary in school-aged children. 28 Conversely, children with clinically significant language disorders may show more evidence of SDB compared to their typically developing peers. 29
Children with CP ± L are more likely than their peers to experience SDB, including obstructive sleep apnea, the transient reduction (hypopnea) or cessation (apnea) of airflow as a result of upper respiratory obstruction.8–10,30 Elevated risk for obstructive sleep apnea is apparent in children with CP ± L both before and after palatal repair surgery.31,32 Evidence regarding sleep behavior in children with CP ± L is very limited. One study has investigated a relationship between disrupted sleep/SDB and language outcomes in children with CP ± L. 33 A group of 33 infants with CP ± L underwent polysomnography to assess sleep apnea at a mean age of 2.7 months and was followed up at 3 years of age for neurocognitive assessment. At follow-up children with CP ± L showed lower receptive and, particularly, expressive language on the Bayley Scales of Infant and Toddler Development, Third Edition (BSID-III) compared to a group of 156 controls for whom polysomnography was not available. Language scores for the CP ± L group did not relate to infant polysomnography variables, but the lack of objective sleep data in the control group makes it difficult to draw conclusions about the role of sleep or SDB. The Japan Environment and Children's Study found that children with CP ± L do not sleep any less than peers without CP ± L. 34 This is consistent with findings in studies of SDB in adults as only around half of with SDB experience substantially impacted sleep quantity and quality. 35 Of potential note is that those with poor sleep quality also report higher rates of restless leg, which is also commonly reported in children with cleft palate. 36 The broader picture of sleep in children with CP ± L is far from clear and often associated with other anomalies. Approximately 15-30% of orofacial clefts also have additional diagnoses. There are over 400 conditions and syndromes associated with CP ± L, including 22.q.11 Deletion syndrome and (Pierre) Robin sequence (RS). RS affects approximately 1 in 8300 newborns 37 and is characterized by a small lower jaw (micrognathia), backward placement of the tongue (glossoptosis), and high levels of SDB,9,38,39 which persists through the primary school years. 40 Whilst much is understood about the increased risk of resonance and articulation difficulties in this group, 41 they may also be at risk of increased language difficulties compared to peers with isolated cleft palate. 42 They are therefore a group of particular interest when studying sleep and language.
Summary and Research Questions
Children with CP ± L as a group, have lower than expected language levels. While some explanatory variables have been suggested, this deficit has not yet been fully explained. We hypothesize that one or more sleep variables might be associated with disordered language in this population given their elevated levels of SDB, which has been repeatedly associated with a range of neurocognitive deficits in children. We hypothesize that these issues are likely to be particularly pertinent to children with a cleft involving the palate, and those with Robin Sequence (RS). To begin investigating this issue we turn to the Cleft Collective cohort study, one of the largest cleft lip and palate longitudinal research databases in the world (see Methods for detail).
43
Questions asked of parents/caregivers in Cleft Collective questionnaires were not designed to consider sleep in any detail, however, some questions related to sleep were posed to parents/caregivers when their children were 18 months, 3 years and 5 years of age. Secondary analysis of data from cohort studies can be an important first step when setting out to test hypotheses relating to rare conditions or hard to reach populations. Our aim in this analysis is to establish initial support or refutation of our hypotheses, and to establish whether the ages of children represented by the Cleft Collective data would be suitable to study when collecting primary data specially designed to test the hypotheses proposed here. If poor sleep does contribute to language difficulties in this population, then there are important implications for clinical governance and intervention, leading us to ask:
Do parents of children with cleft lip and palate express concern about sleep behavior?
Does parental concern change over time at ages 18 months, 3 years, and 5 years? Does parental concern differ by cleft phenotype or with additional diagnoses such as a syndrome or Robin Sequence (RS)? Are children with cleft lip and palate getting sufficient hours of sleep in a 24-h period across the three time points?
Does this differ by cleft phenotype or with additional diagnoses such as a syndrome
or Robin Sequence (RS)? Does parent report of sufficient hours of sleep correlate with language skills?
Methods
Ethical approval for the use of secondary data accessed from the Cleft Collective resource was granted by Newcastle University Ethics Committee (Ref: 39000/2023) and approved by the Cleft Collective Project Management Group (project number CC057).
Design
This was an exploratory study using data taken from responses to parent questionnaires as part of the Cleft Collective cohort study at three time points: when children were 18 months of age, 3 years of age and 5 years of age. Data were analysed cross-sectionally.
Data Collection
The Cleft Collective
The Cleft Collective study is a large prospective cohort study of children born with cleft lip and/or palate, investigating causes of cleft, the best treatments and the impact of cleft on those affected and their families. 43 The resource comprises biological samples, speech audio recordings, medical and educational records and parent and child completed questionnaires, completed longitudinally. The resource is available for clinical and academic communities to access and use to address a range of cleft related research questions. More information on the study and how to access the dataset is available at http://www.bristol.ac.uk/cleft-collective/professionals/access. Initial funding for the Cleft Collective was provided by the Scar Free Foundation; additional funding was provided by The Underwood Trust and the Vocational Training Charitable Trust (VTCT). The resource currently holds data on over 12,000 participants from approximately 4200 families, including children with cleft lip and/or palate, their parents (or others with parental responsibility), and their siblings. Questionnaires are sent to families at regular intervals. These are completed by the biological mother and the father or the mother's partner at birth and when the child turns 18 months, 3 years, and 5 years. Questionnaires are also sent beyond 5 years to the parents and the child themselves.
Participants
The sample taken for this study was from parent questionnaires of children at age 18 months, 3 years, and 5 years. This included children with all cleft phenotypes (cleft lip only (CLO), unilateral cleft lip and palate (UCLP), bilateral cleft lip and palate (BCLP), cleft palate only (CPO)) and additional diagnoses such as a known syndrome or RS. The return rate to the Cleft Collective for questionnaires is currently 38% at 18 months, 39% at 3 years and 33% at 5 years. Those with submucous cleft palate were excluded as children born with this phenotype often present late to cleft lip and palate services and so very few are consented to take part in the Cleft Collective study, such that the numbers in this sample (n = 20) were too small for meaningful analysis.
Procedures
The study used maternal responses to the questions with responses from fathers or mother's partners used where there was no maternal response.
Measures
The primary sleep measures were compiled from parent report of concern regarding sleep behavior and reported sufficient hours of sleep over a 24-h period at each time point. Direct questioning of parental concern with sleep was only asked at ages 18 months and 3 years and some questions at these ages related to several behaviors (eg, concern with eating, toileting and sleep); where this was the case positive scores indicating concern were only assigned if parents specifically mentioned sleep in their qualitative answers, otherwise a score of 0 was assigned. Secondary outcomes relating to trouble falling asleep at 18 months and waking in the night for a drink at 3 and 5 years were also considered. The specific questions across the three time points from which all sleep data were gathered are given in Appendix A. Parents’ comments from the option to provide free text to explain their concerns at 18 months and 3 years were also explored to provide qualitative measures regarding experiences with sleep behavior in their children. A measure of “sufficient hours of sleep in a 24-h period” was recorded using the responses to questions 4a or 4b in Appendix A. The questions are taken from the Ages and Stages Questionnaire: Social-Emotional (ASQ:SE). 44 Parents were asked if their child sleeps for at least 10 h in a 24-h period at 18 months, and for at least 8 h in a 24-h period at 3 and 5 years.
Language measures were derived from the answers to six questions at each time point. These included questions which explored receptive language (eg, Without showing him/her, does your child point to the correct picture when you say, “Show me the cat,” or ask, “Where is the dog?”; Without you giving help by pointing or repeating directions, does your child follow three directions that are unrelated to one another?) and expressive language (eg, Does your child say eight or more words in addition to “mama” and “dada”?; Does your child use four and five word sentences?). The questions with regard to language are taken from the Ages and Stages Questionnaire (3rd edition) ASQ-3. 45 Points are assigned to the answers to each of these questions (for example, 10 points for “Yes” a behavior is achieved, 5 points for “Sometimes”, and 0 points for “Not yet”). For full details of the questions asked, see Appendix B. A categorical variable was created by accumulating the points to the answers to questions 1a-f at 18-months, 2a-f at 3-years and 3a-f at 5-years (as laid out in Appendix B). Higher scores indicate more positive outcomes. These accumulated points align with the categories “On schedule” /”Requires monitoring” / “Needs onward referral,” indicating the level of language development.
Confounds
Five potential confounding variables for language outcomes were identified prior to data access, all of which were theoretically driven from existing literature on language outcomes. These included additional syndromic diagnoses, 46 maternal education, 47 type of milk as a baby, 48 birth weight, 49 and exposure to passive smoking. 50
Data Analysis
All quantitative data were analysed using SPSS v29.0.1.0 (IBM, 2023). As an exploratory study, most analyses are descriptive. Frequencies of each sleep measure were calculated at the three time points where possible; for different cleft phenotypes; and for those with additional diagnoses (syndromes and RS). Group differences were explored using non-parametric analyses. Where group differences were observed, effect size was calculated using the equation r = Z/√N, with r = .10 to .29 indicating a small effect, r = .30 to .49 a medium effect and r ≥ .50 a large effect. 51 Tau ordinal correlations of measures of sufficient hours of sleep with language outcome at each of the three time points were calculated. Partial correlations were also conducted to account for the influence of confounding variables. A basic qualitative approach was employed to explore parent-reported experiences with sleep behaviors. Free-text responses from questionnaires were analysed using content analysis, a method that allows for systematic categorization of textual data. Statements were read and re-read to identify recurring themes and patterns. Responses were grouped into descriptive categories based on the nature of the concern (eg, night waking, difficulty settling, co-sleeping, signs of distress, breathing issues). Frequencies of each theme were recorded to provide an overview of common experiences. This approach enabled the identification of sleep-related behaviors that may not have been captured through the structured questionnaire items.
Results
A total of 1990 parents returned questionnaires at all three time points. The final sample included participants with sleep data available for each time point - 1092 questionnaires at 18 months, 972 questionnaires at 3 years and 722 at 5 years. There were responses from parents of children with a range of cleft phenotypes which reflected the wider cleft population. 52 Participant details can be found in Table 1.
Participant Details.
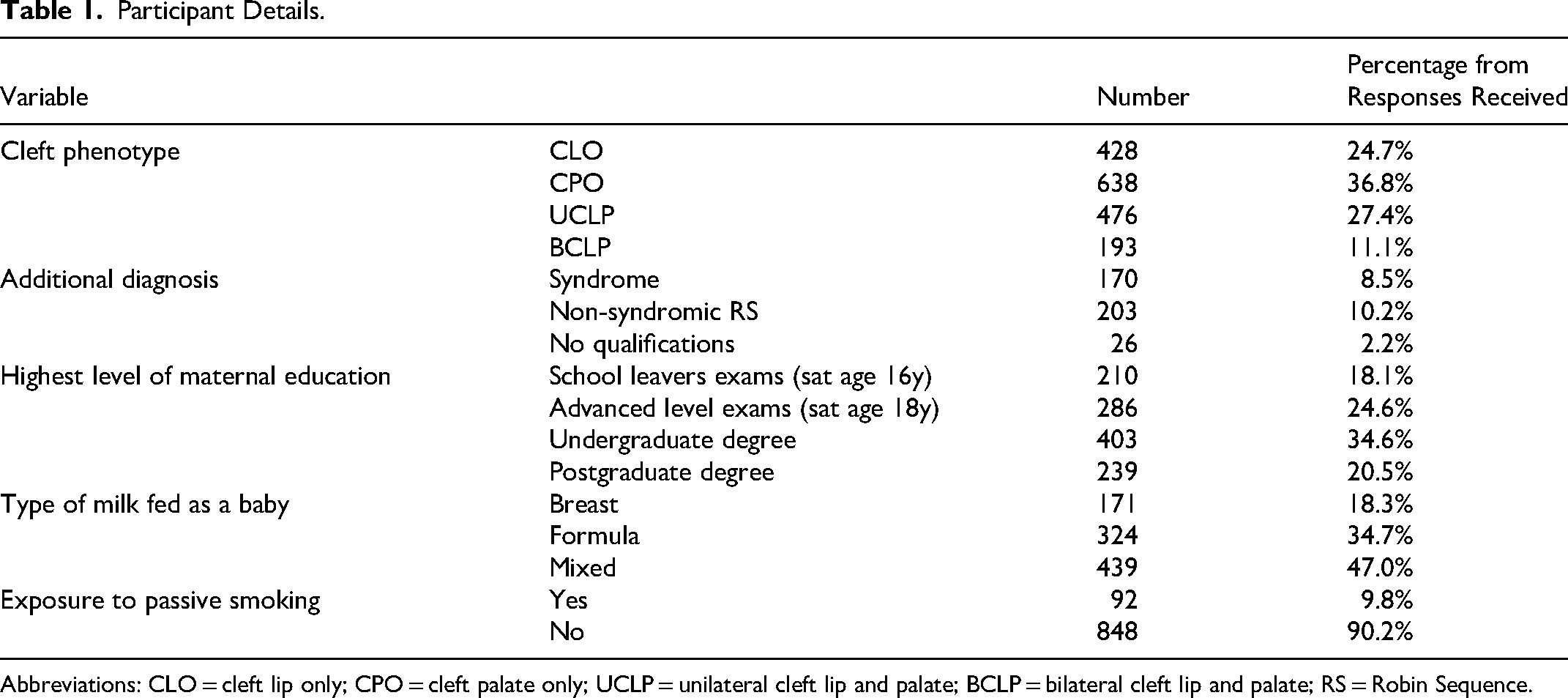
Abbreviations: CLO = cleft lip only; CPO = cleft palate only; UCLP = unilateral cleft lip and palate; BCLP = bilateral cleft lip and palate; RS = Robin Sequence.
Do Parents of Children with Cleft lip and Palate Express Concern About Sleep Behavior?
Levels of parental concern when asked directly were low (Appendix A, questions 1a and 1b). Concern decreased from 18 months (13.0% (n = 134)) to 3 years (7.9% (n = 74)).
Secondary questions about falling asleep at naptime and nighttime at 18 months and getting up to drink in the night at 3 years and 5 years indicated behaviors which might impact quality of sleep. At 18 months, 30.2% (n = 324) of parents reported that their child had difficulty falling asleep most of the time or sometimes. At 3 years 33.5% (n = 323) of parents indicated that their child got up in the night to have a drink; this was unchanged at 34.2% (n = 246) at 5 years.
Content analysis from the qualitative comments in the free text sections of the questionnaires at 18 months and 3 years gave some insight into the issues. Not all parents completed this section (at 18 months n = 48; at 3 years n = 57). However, of those that did, night waking was mentioned by 73% of parents at 18 months (n = 35) and 53% of parents at 3 years (n = 30). Other themes were settling their child to sleep (n = 7, 18 m; n = 6, 3y), co-sleeping (n = 5, 18 m; n = 10, 3y), signs of stress and anxiety when waking in the night (such as crying and arching their back) (n = 5, 18 m; n = 5, 3y) and issues with breathing (n < 5, 18 m; n = 9, 3y).
Differences Across the Cleft Phenotypes
The percentage of parents reporting concern with sleep behavior across the cleft phenotypes is shown in Table 2. Kruskal-Wallis analyses indicated no evidence of significant differences between cleft phenotypes at any age. Post-hoc pairwise comparisons indicated some weak evidence that at 3 years parents with children with CLO were less likely to report concerns than those with CLP. This was corroborated by a Mann Whitney U test comparing CLO to a CLP group (UCLP, BCLP, CPO), showing a small effect of group – U (923) = 84204.000, P = .009, r = .09.
Numbers of Parents Reporting Concerns with Sleep Behavior at 18 Months and 3 Years and Non-parametric Analysis of Group Differences.
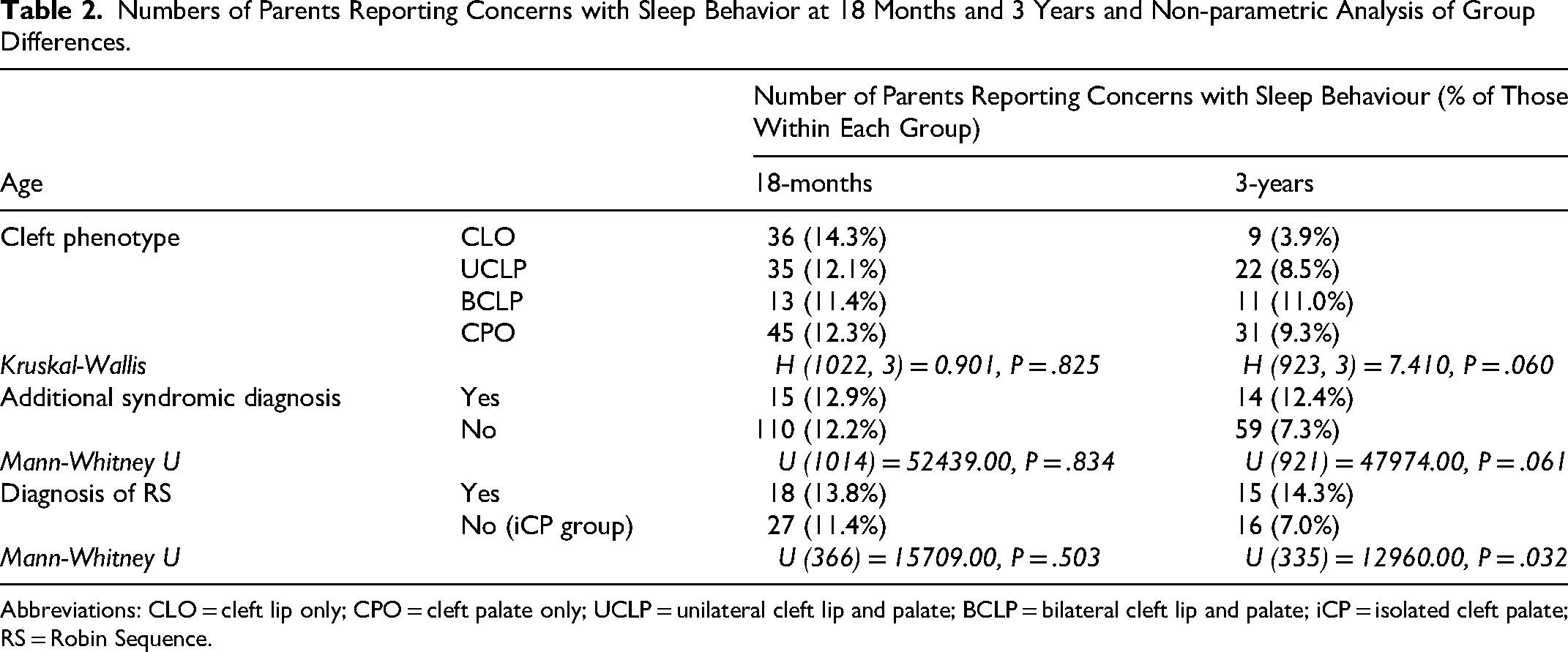
Abbreviations: CLO = cleft lip only; CPO = cleft palate only; UCLP = unilateral cleft lip and palate; BCLP = bilateral cleft lip and palate; iCP = isolated cleft palate; RS = Robin Sequence.
Differences Across Additional Diagnoses
The percentage of parents reporting concern with sleep behavior across those with and without additional syndromic diagnoses, and Robin Sequence (RS) is also shown in Table 2 at 18 months and 3 years. Mann-Whitney U analyses provided evidence of a significant difference between those with RS compared to those with isolated cleft palate (iCP) at 3-years, with a small effect of group (r = .12).
Are Children with Cleft lip and Palate Getting Sufficient Hours of Sleep in a 24-h Period Across the Three Time Points?
Parents in the Cleft Collective study are asked to indicate if their child sleeps a certain number of hours in a 24-h period “Most of the time, Some of the time, or Rarely/Never.” For 18 months this is 10 h over a 24-h period; for 3 and 5years it is 8 h. At all three age points most parents indicated that the children did sleep for these hours “most of the time”; at 18 months this was 88.8% of parents, at 3 years this was 91.8% of parents; and at 5 years this was 90.9% of parents.
Does This Differ by Cleft Phenotype or with Additional Diagnoses Such as a Syndrome or Robin Sequence (RS)?
Figure 1 shows the reports of sufficient hours of sleep across the cleft phenotypes. Those with CLO improved from 18 months to 5 years with more consistent report of sufficient sleep, where those with CPO did not and those with UCLP and BCLP improved up to the age of 3 years and then plateaued. Kruskal-Wallis analysis supported this indicating that there was no evidence of significant group differences between cleft phenotypes at ages 18 months and 3 years, but that there was increasing evidence of some group difference by age 5 years (18 months: H (1069,3) = 2.118, P = .548; 3 years: H (5743) = 5.688, P = .128; 5 years: H (2973) = 7.092, P = .069). After post-hoc pairwise comparisons, the strongest evidence for a group difference was between those with CLO and those with CPO at 5 years (P = .011; adj. P = .063).
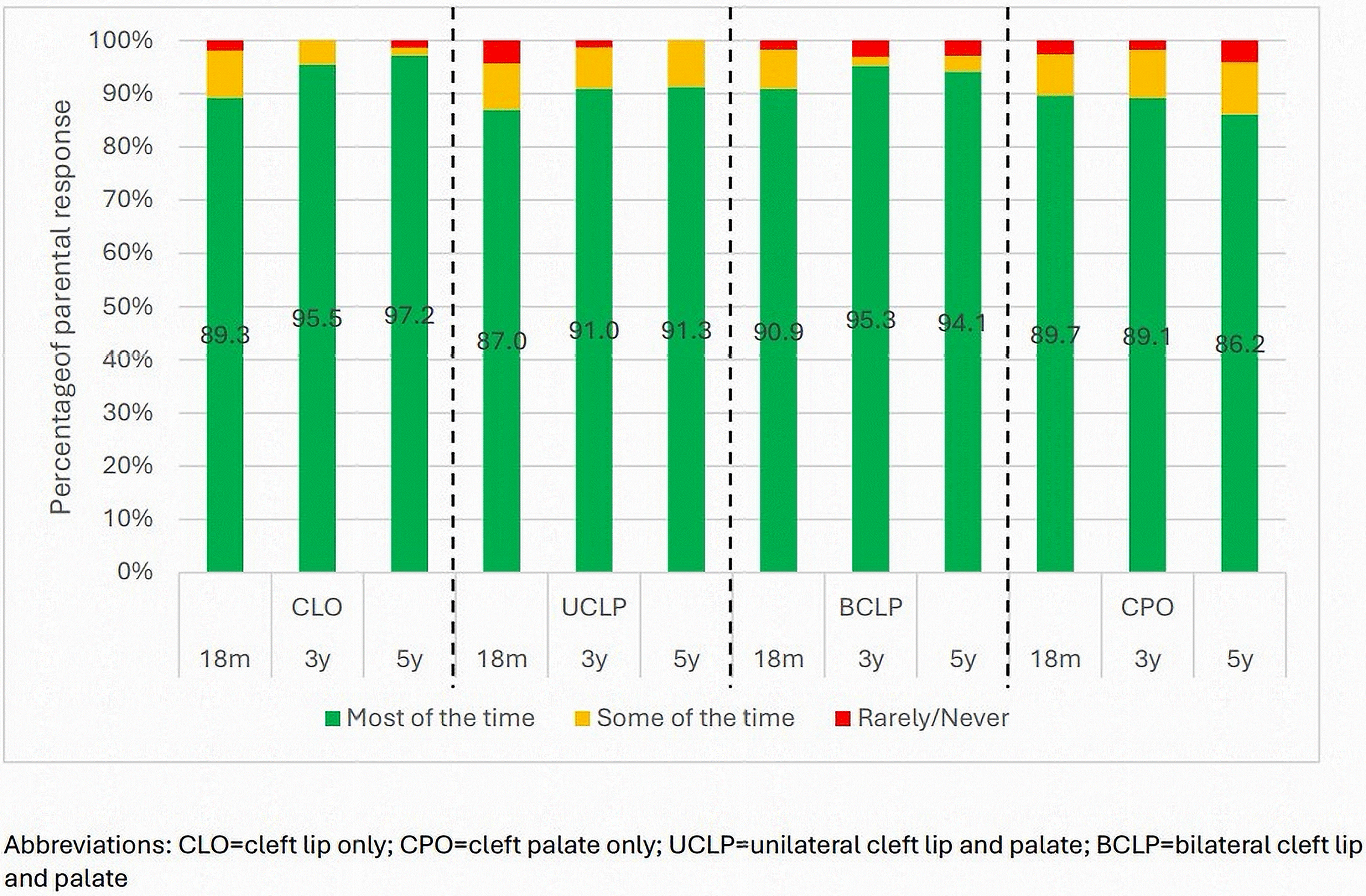
Percentage of parents indicating sufficient hours of sleep over a 24-h period across the three time points and by cleft phenotype.
Figure 2 shows reports of sufficient hours of sleep from parents of children with and without an additional syndromic diagnosis. Mann-Whitney U analysis indicated that there was no evidence of significant group differences at 18 months and 3 years (18 months: U(1060) = 59260.50, P = .636; 3 years: U(574) = 19539.00, P = .763), but that this changed at 5 years, with those with an additional syndrome less likely to indicate that their child slept 8 h in a 24-h period “most of the time” (U (296) = 6209.50, P = .033, r = .12). It also shows that those without an additional syndromic diagnosis improved from 18 months to 5 years with more consistent reports of sufficient sleep, where those with an additional syndromic diagnosis have more varied levels of sleep.
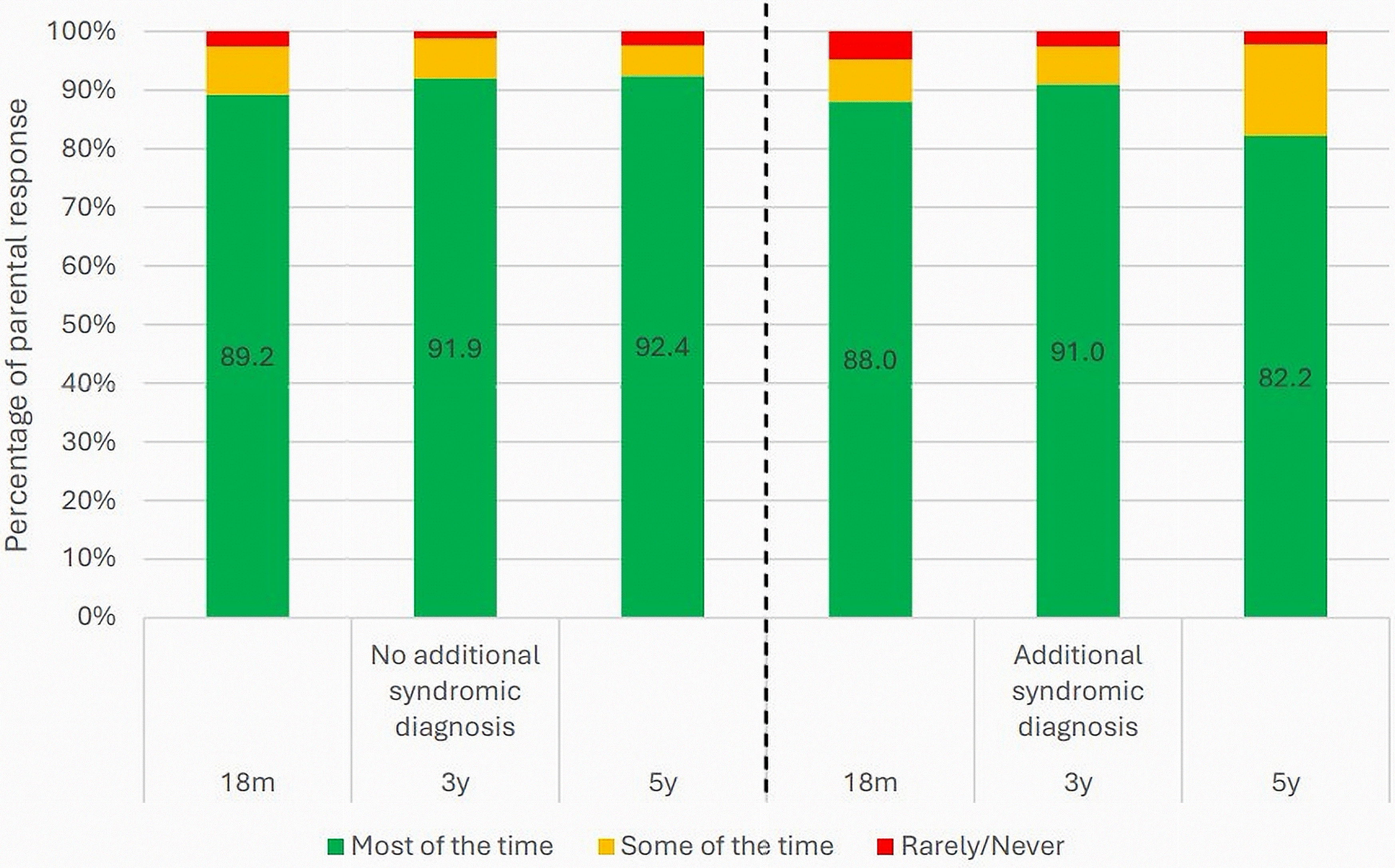
Percentage of parents indicating consistent hours of sleep over a 24-h period across the three time points and by additional syndromic diagnosis.
Figure 3 shows reports of sufficient hours of sleep from parents of children with RS compared with those with iCP. For those with iCP little variability in response was seen over the three time points. For those with RS, parents reported a decrease in consistent hours of sleep after 18 months. Mann-Whitney U analysis indicated that there was no evidence of significant group differences at 18 months (U(388) = 16953.00, P = .742); but that this changed from 3 years (3 years: U(223) = 5772.00, P = .021; 5 years: U(124) = 1914.00, P = .059). At both these time points a small effect of group was observed (r = .15 (3y), r = .17 (5y)).
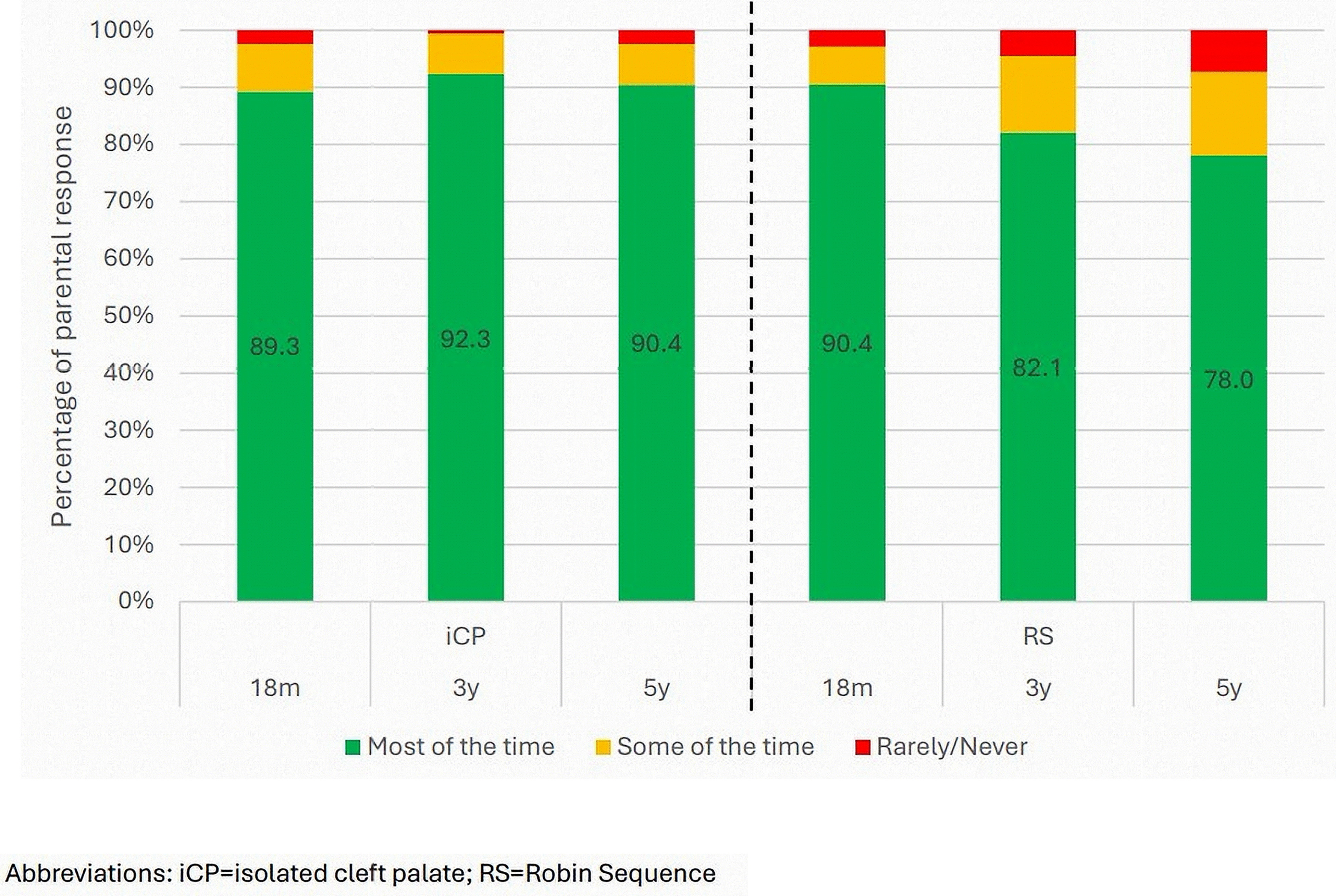
Percentage of parents indicating consistent hours of sleep over a 24-h period across the three time points and by diagnosis of Robin Sequence (RS).
Does Parent Report of Sufficient Hours of Sleep Correlate with Language Skills?
Significant, positive correlations were observed between parental report of sufficient hours of sleep and parent report of language skills (from the derived ASQ variable on communication indicating language is on schedule, requires monitoring or needs onward referral – see Appendix B) at all time points (18 months: τ(998) = .087, P = .004; 3 years: τ(530) = .131, P = .002; 5 years: τ(270) = .445, P < .001). This relationship was strongest at age 5 years where a positive moderate correlation was observed. Partial correlations at age 5 years accounting for the theoretically motivated confounders (additional syndromic diagnoses, maternal education, type of milk as a baby, birth weight, and exposure to passive smoking), showed a continued positive significant correlation between sufficient sleep and language skills (Partial r(167) = .347, P < .001). The presence of an additional syndromic diagnosis was correlated with language difficulties (r(667) = .296, P < .001) as expected, with those who have an additional syndromic diagnosis being more likely to need support for language difficulties. There was a weaker positive significant correlation observed between exposure to passive smoke and language outcomes (r(423) = .148, P = .002). There was evidence of a significant relationship with maternal education and both language (r(423) = −.153, P = .002) and with sleep (r(195) = −.163, P = .022)), whereby the higher the level of maternal education the less likely the parents were to report difficulties with language or sleep.
Discussion
In this paper we sought to explore initial evidence for a relationship between sleep behavior and language development in early childhood as reported by parents of children born with orofacial clefts. Specifically, we looked at levels of parental concern about sleep at 18 months and 3 years and reports of sleeping 8-10 h across a 24-h period from the ages of 18 months to 5 years. For this we used data from the Cleft Collective study. We also ran correlations between reported hours of sleep and language development. We hypothesized that those with a cleft involving the palate and particularly those with Robin Sequence (RS) would experience more disrupted sleep and that there would be a correlation between sleep and language outcomes. All these hypotheses were supported. Below we summarize our findings in relation to previous literature and discuss the possible underlying factors relating to sleep and language before outlining directions for further research.
Parental Concern with Sleep
Parents were asked directly if they had concerns about their child's sleep at 18 months and 3 years. They were also asked questions which related to sleep behavior such as whether their child had difficulty falling asleep or got up in the night. When asked directly, reports of concern were low and decreased over time with only 7.9% of parents reporting ongoing concern at 3 years. This is somewhat lower than anticipated given previous estimates of parental concern about children's sleep in the UK in 0-3-year-olds sit at around 23%. 53
However, questions which might be indicative of disturbed sleep showed that over 30% of parents across all ages studied reported that their child experienced these behaviors at least some of the time. These behaviors included ability to fall asleep and getting up in the night to have a drink. Although parent report of night waking has been shown to underestimate objective data, 54 the rates we observed here were consistent across the ages where other studies have shown a decrease in night waking as children approach age 5 years. 55
Levels of concern did not vary by cleft phenotype at 18 months. By 3 years we observed a higher level of concern in parents of children who had a cleft involving the palate compared to those with cleft lip only. Parents of children who had an additional diagnosis such as a syndrome or RS were also more likely to report concerns with sleep as we would expect from prior research.56–58
Sufficient Sleep in a 24-h Period
The majority of parents (>88%) at all ages reported that their child was getting “sufficient” sleep in a 24-h period. However, we observed some interesting patterns across the different diagnoses. For children with CLO, UCLP and BCLP, parents reported an increase in sufficient sleep from 18 months to 3 years. For those with CPO, reports remained steady with a slight drop at 5 years. This group included children with RS and when we analysed this group separately compared to those with an isolated cleft of the palate (iCP), we observed that it was this particular group whose pattern of sufficient sleep declined across time whilst those with iCP showed a similar pattern to CLO, UCLP and BCLP. RS is of particular interest when studying sleep due to the known airway issues which accompany this disorder, and so it was not surprising to find this pattern.58,59 Similarly, reports of sufficient sleep were erratic in children with additional syndromic diagnoses compared to non-syndromic peers. This is also reported in other studies.56,57,60
The picture for parent-reported nighttime sleep duration in the non-cleft population is quite consistent across studies and across the age range of interest. Between the ages of 18 and 60 months, parental report indicates that children sleep between 10 h and 10.9 h (with SD ranging from 0.4 to 1.3 h).55,61,62 In addition, parent-reported average daytime naps over this age range decrease from 2 h at 18 months to 30 min at 60 months. 55 So for parents in the Cleft Collective study, who were asked how often their child gets 10 h sleep over a 24 h period at 18 months, and 8 h at 3 and 5 years (taken from the ASQ:SE 44 ), answering “sometimes” or “rarely” would indicate that their child has a significant sleep problem. Therefore, the data reported here is likely to indicate that more children are getting “sufficient” sleep than is actually the case.
Relationship Between Sleep and Language
Associations between sleep and language outcomes were observed at all ages with increasing strength across the years. A moderate association remained even after adjusting for confounding variables at age 5 years. These associations have been observed in the non-CP ± L population.2,26–29 To our knowledge there is only one paper prior to this study which has sought to investigate direct links between sleep and language outcomes in children with CP ± L. In 2014 Smith et al 33 reported a correlation between apnea/hypopnea events caused by obstruction, and behavior at 3 years as well as percentage of rapid eye movement sleep in infancy and later cognitive scores at 3 years, but not receptive or expressive language. This study was small, with 33 infants and only 19 with follow-up sleep data, and little detail is given about what the authors mean by behavior or cognitive outcomes. The relevant questions on the BSID-III which was used to measure cognition and those on the quality-of-life questionnaire used to measure behavior include questions about attention skills. Low attention skills are frequently reported in the CP ± L population63–65 and links between attention and language development have been shown in both the non-CP ± L population66,67 and the CP ± L population. 68
We can only speculate about possible mechanisms linking sleep and language in this sample. The reasons for the observed variability in parent-reported sufficient sleep are not clear. This variability could reflect behavioral differences around going to sleep, night waking, or early rising, or it could reflect sleep fragmentation specifically related to sleep disordered breathing (SDB). There are at least three possible mechanistic explanations that we could postulate. The first possibility is that both sufficient sleep and better language are associated with a common factor, or factors which are not measured here. The second explanation is that sleep and language are causally related, with sleep most plausibly being a driving force for either general brain maturation, 69 or for the specific consolidation of newly learned linguistic information.22–24 The third possibility is that language development in childhood is affected by overnight oxygen saturation levels, as supported by the findings that pre-schoolers with SDB show difficulties processing complex verbal requests 27 and school children with SDB have poor expressive vocabulary. 28
Limitations
There are several limitations to using parent report for sleep outcomes. In a recent rapid review of sleep measurement methodologies, 54 six studies using parent sleep diaries were considered and nine studies using parent questionnaires. For children between 3-7 years of age, daily sleep diaries were rated as having good validity for sleep onset, good or moderate for rise time and good for nap time, but poor for sleep onset latency and night waking. The validity of parent questionnaires was generally rated as poor for sleep duration, sleep onset latency and night wakings with one good rating for sleep onset/offset. We must therefore be mindful that parent reported data are likely to over-estimate the amount of nighttime sleep that their children get.
Further limitations of parent-report measures are relevant to this study in particular. Whilst the Cleft Collective questionnaires provide a wealth of data on background and developmental outcomes in children with CP ± L, sleep quantity and quality questions are very limited. One example of a substantial limitation is that parents are not asked the same questions across time points. For example, parents are only asked if they have concerns regarding their child's sleep at 18 months and 3 years, only asked about difficulties falling asleep at 18 months and about waking for a drink at 3 and 5 years. We were therefore unable to directly compare questions across all age points. In addition, some questions were used in our analysis as a proxy for more direct questions, for example the question “Does your child get up in the night for a drink?” was used as a proxy in lieu of a direct question about night waking. Finally, no data were available about daytime napping compared to nighttime sleep. This is significant as studies of sleep in the general population have shown the importance of day/night sleep ratios across development and the consolidation of sleep patterns in the early years. 25
Response rates for questionnaires are always an issue using this methodology. The response rate for the Cleft Collective questionnaires overall is on average between 30-40%. We saw a decline in response rate to the questions used in this analysis over the age points, with parents more likely to respond in detail at 18 months than at 5 years. This had an impact on our data at 5 years which yielded increasingly smaller sample sizes when comparing groups such as RS versus iCP; however, this sample size was still 122 with 38 participants with RS.
Future Research
Findings from this study give food for thought for further research. There are many influences on language development such as genetic factors, environmental factors and cognitive factors.23–25 Sleep is one potential mechanism which links many of these factors.
To advance our understanding of the complex relationship between sleep and language development in young children with orofacial clefts, future research must adopt both observational and interventional approaches. There is a pressing need for empirical data that captures not only the quantity and quality of sleep - including both daytime sleep and SDB - but also how these factors interact with language acquisition over time. Longitudinal studies are valuable in identifying developmental trajectories and causal relationships. Studying change over time is particularly illuminating in relation to children whose bedtime routines and sleep practices may shift significantly following surgical interventions such as palate repair. Understanding how such procedures influence parental and child behaviors around sleep could offer critical insights into optimizing post-surgical outcomes and supporting language development more effectively. This exploratory study has shown that collecting data at these age points provides a good picture of trajectories of sleep behavior and development.
Conclusions
This study examined sleep behaviors in children with cleft lip and palate using data from the Cleft Collective cohort study. While overall parental concern about sleep was not unusually high, a clear and increasingly strong association between sufficient sleep and language development was observed - most notably at age 5 years. This relationship remained significant even after accounting for key confounding factors, suggesting that sleep may play a meaningful role in shaping language outcomes in this population. Children with RS emerged as a particularly vulnerable group. These findings point to RS as a critical subgroup for future research. Longitudinal and interventional studies are now needed to explore the mechanisms linking sleep and language in these populations.
Footnotes
Acknowledgements
This publication involves data derived from independent research funded by The Scar Free Foundation; additional funding was provided by the Underwood Trust and the Vocational Training Charitable Trust (VTCT) (REC approval 13/SW/0064). We are grateful to the families who participated in the study, the UK NHS cleft teams and the Cleft Collective team, who helped facilitate the study. The views expressed in this publication are those of the author(s) and not necessarily those of Scar Free Foundation, Underwood Trust, or the Vocational Training Charitable Trust.
Ethical Statement
Ethical approval for the use of secondary data accessed from the Cleft Collective resource was granted by Newcastle University Ethics Committee (Ref: 39000/2023) and approved by the Cleft Collective Project Management Group (project number CC057).
Author Contribution Statement
Both authors contributed equally to the conception, design, data collection, analysis, interpretation, drafting, and revision of the manuscript. They are jointly responsible for all aspects of the work and have approved the final version for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data underlying this article were provided by The Cleft Collective under project number CC057-SvE following approval from the Cleft Collective Project Management Group. Data are available from the Cleft Collective resource following approval of a project proposal and ethical approval from a research ethics committee for each study. For further information on how you can access data please visit: ![]()
Appendix A.
Questions and their corresponding questionnaire number asked about sleep in the Cleft Collective questionnaires at 18-months, 3-years, and 5-years.
Appendix B.
Questions and their corresponding questionnaire number asked about language in the Cleft Collective questionnaires at 18-months, 3-years, and 5-years.