
Abstract
Objective
To compare long-term esthetic and morphological outcomes of unilateral cleft lip (UCL) repair using the Millard rotation-advancement versus the Tennison-Randall triangular flap technique, testing whether Millard provides superior lip symmetry.
Design
Retrospective cohort study.
Setting
Single tertiary cleft center.
Patients, Participants
Forty adults aged 18-25 were selected from 168 patients treated between 1988 and 1995. Inclusion criteria: complete UCL, primary cheiloplasty, absence of secondary lip revisions, complete frontal photographic documentation, and no syndromic diagnoses. Twenty underwent Millard repair and twenty Tennison-Randall repair.
Interventions
Primary UCL reconstruction performed using either Millard rotation-advancement or Tennison-Randall triangular flap. All operations were carried out by the same senior cleft surgeon under comparable operative conditions.
Main Outcome Measure(s)
Long-term lip symmetry quantified through a Symmetry Index derived from predefined anthropometric landmarks on standardized images. Subjective esthetic satisfaction assessed using the esthetic Units Satisfaction Questionnaire and the Cleft esthetic Rating Scale, completed by patients, the operating surgeon, and a blinded observer.
Results
Millard repair showed significantly greater medial lip width symmetry (p = .014). No significant differences were found for vermilion height, prolabial height, lateral lip width, or lip area. Subjective assessments consistently favored Millard, showing higher satisfaction and fewer negative ratings. Inter-rater reliability across evaluators was high (ICC = 0.82).
Conclusions
Both techniques produced stable long-term outcomes, but Millard yielded superior medial lip symmetry and higher esthetic satisfaction. These findings support its continued clinical preference and highlight the importance of long-term evaluations. Larger prospective studies are needed to confirm these results.
Introduction
Cleft lip and palate (CLP) is a malformation with an incidence of 1 in 700 live births 1 , which is characterized by the presence of an orofacial cleft, due to a lack of fusion of embryological sketches during intrauterine life. 1 Immediately after birth, in children born with CLP, many problems begin to appear, such as nutritional problems and frequent infections of the auditory system. 2 Moreover, when they reach the age of language development, they have limitations in the ability of verbal expression, which can affect learning and socialization too. 2
Another circumstance that concerns this pathology is the defect in dental development and malocclusion that requires orthodontic and sometimes surgical treatment. 3 Due to the previously mentioned causes, this pathology represents a significant public health burden in terms of immediate and long-term medical costs, as well as a significant social impact on patients and their families. 3
These issues suggest the need for patients to require extensive treatment for their functional rehabilitation, as well as social integration by a multidisciplinary team over many years. 3
Within the wide variability of this malformation, it is possible to distinguish two main phenotypes: cleft lip (CL), with or without palate involvement, and isolated cleft palate. This subdivision arises from an embryological and etiological sharing of the two forms, although within each category, it is possible to have unilateral, bilateral, simple, and complex expressions. 4
The optimal treatment of patients affected by lip and palate cleft requires an early esthetic and functional rehabilitation, which today is achieved through several algorithms of procedures, based on multidisciplinary concepts in well-organized centers around the world. Surgical correction is fundamental for the anatomical reconstruction of the nasolabial region: the esthetic aspect is a goal of primary importance, at the same level as the restoration of physiological function, of the above-mentioned structures. 4
A wide range of surgical techniques for the repair of CL has been described over time; the concept that unites these methods is the correct positioning of the orbicularis muscle insertions, the restoration of a normal anatomy of the nasolabial region, nasal reconstruction, and an overall harmony of the face.3,4
Among the numerous techniques described for unilateral CL repair, the Millard rotation-advancement and the Tennison-Randall triangular flap methods have remained the two most widely adopted approaches. They differ substantially in their geometric design and tissue redistribution: the Millard technique emphasizes rotation and advancement to recreate the philtral contour, whereas the Tennison-Randall approach relies on triangular flap interposition to restore lip length and symmetry. This study compares the two historically dominant techniques for unilateral CL repair to provide an evidence-based evaluation of how their distinct surgical concepts influence long-term esthetic and morphological outcomes, addressing the often-overlooked temporal dimension in CL management.
Materials and Methods
A retrospective cohort study was conducted, and ethical review and approval were waived due to its retrospective design and the use of fully anonymized data. All procedures were conducted in accordance with the ethical standards outlined in the Declaration of Helsinki. Patients with unilateral cleft lip (UCL) who underwent surgical treatment at the Plastic and Maxillofacial Department between 1988 and 1995 were reviewed.
A total of 168 patients met the general inclusion criteria for primary cheiloplasty during this period. Of these, 17 patients were excluded because they did not reach an adequate long-term follow-up at the end of facial growth. Furthermore, 16 patients from the Millard group and 40 from the Tennison-Randall group underwent secondary revisions of the labial region. Of those, almost 80% of the patients originally treated with the Tennison-Randall technique were later converted to a Millard-type rotation-advancement repair during revision surgery. In addition, patients were excluded if the cleft involved the alveolar (gengival or bone) component, or if they presented minor or incomplete forms such as Simonart's band. Secondary rhinoplasty was not considered an exclusion criterion. Cleft laterality (right/left) was recorded for all patients but was not considered a discriminant variable in the analysis.
After applying these criteria, 40 patients were collected and divided into two groups based on the surgical technique used:
All procedures were performed by a single senior cleft surgeon under similar operative conditions. Patients with associated craniofacial syndromes, secondary surgeries, or incomplete photographic documentation were excluded.
Surgical outcomes were evaluated at the end of the growth of the facial massif between 18 and 25 years of age through a morphological analysis and a subjective esthetic evaluation.
Morphological Analysis
Postoperative morphological outcomes were retrospectively evaluated in patients aged 18-25 years to assess long-term surgical results following primary cheiloplasty.
Standardized frontal facial photographs were analyzed using digital image software (Photoshop
On each image, a set of predefined anthropometric landmarks was identified on both the cleft and non-cleft sides, based on established craniofacial reference points, including the subunits of the nose and the mouth.
The landmarks selected for the study of the naso-labial area are points that defined the upper lip, the filter, and the base of the columella: (A) center of the base of the columella; (B) right cuspid of the Cupid's Arch; (C) left cuspid of the Cupid's Arch; (D) right labial commissure and (E) left labial commissure. On the imaginary line that crosses the two commissures, there are also: (F) projection of the right cuspid of the Cupid's bow; (G) projection of the left cuspid of the Cupid's bow, and (X) projection of the center of the Cupid's bow (Figure 1).
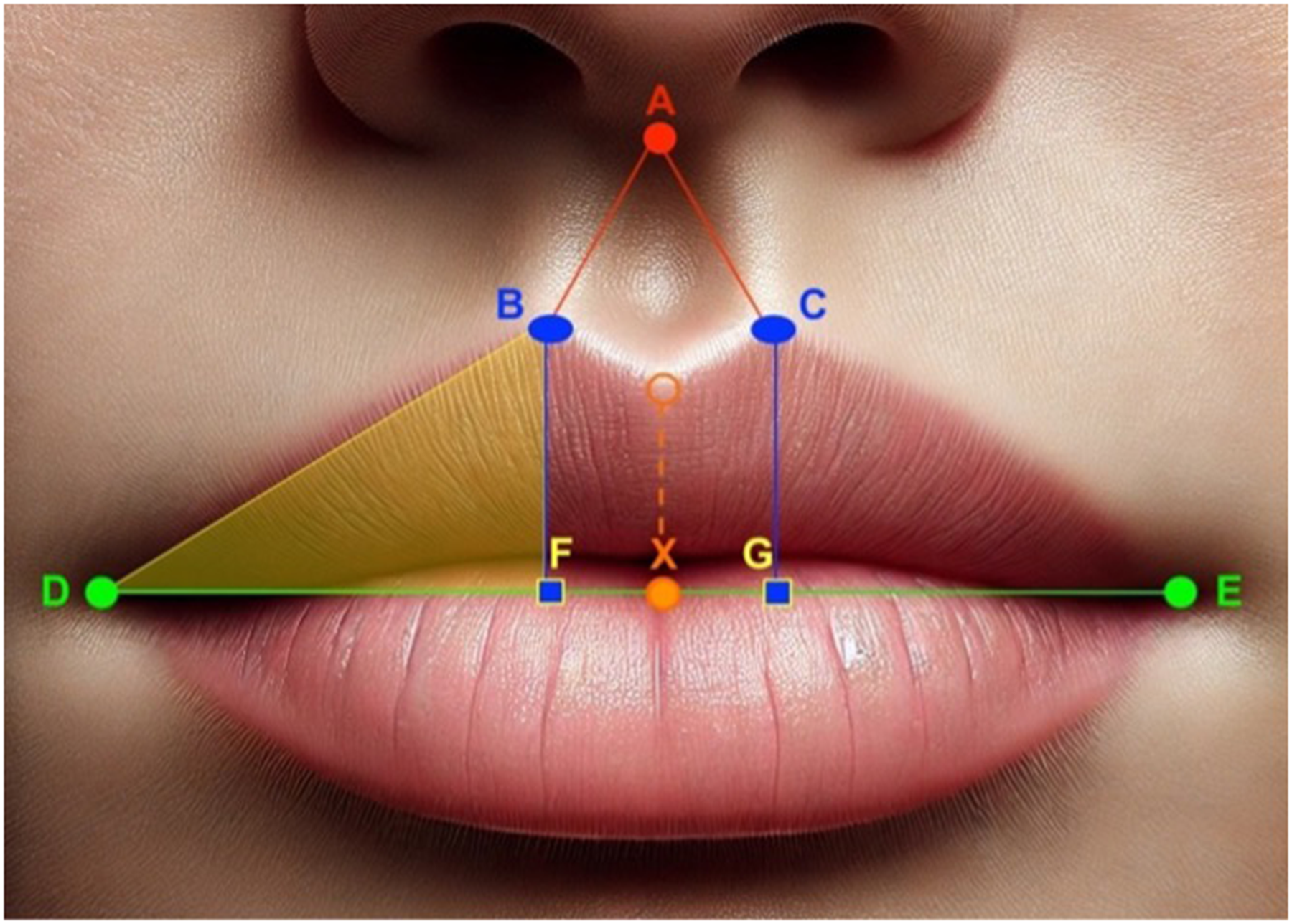
Schematic representation of landmarks of morphological evaluation on digital frontal photographs of adults who underwent cheiloplasty in childhood. (A) center of the base of the columella; (B) right cuspid of the Cupid's arch; (C) left cuspid of the Cupid’s Arch; (D) right labial commissure and (E) left labial commissure; (F) projection of the right cuspid of the Cupid’s bow ; (G) projection of the left cuspid of the Cupid’s bow and (X) projection of the center of the Cupid’s bow.
From these landmarks, linear distances were measured between corresponding anatomical structures of the right and left hemilips.
For each parameter, a Symmetry Index (SI) was calculated to quantify bilateral lip symmetry. The index was defined as the absolute difference between the values measured on the left and right sides, normalized to their mean value and expressed as a percentage, using the following formula:

where L = measurement on the left hemilip; R = measurement on the right hemilip.
This index provides a dimensionless value that allows comparison across patients with different lip sizes. Lower SI values indicate a higher degree of bilateral symmetry and were therefore considered to represent better long-term surgical outcomes from an esthetic and reconstructive standpoint.
The difference that stabilized over time could be horizontal, vertical, or mixed, if both were present: the vertical defect was given by an asymmetry of the prolabium and/or the height of the upper lip, which could be too long or too short, compared to the contralateral one; instead the horizontal defect was given by an asymmetry of the lateral units and/or of the central unit, included in the vermilion subtended by the Cupid's bow.
To quantify the vertical defect, measurements were considered between: AB) center of the columella − right cuspid of the Cupid's Arch; AC) center of the columella − left cuspid of the Cuspid's Arch; BF) height of the vermilion from the right cuspid of the Cupid's Arch and CG) height of the vermilion from the left cuspid of the Cupid's Arch. To quantify the horizontal defect, considered measurements were: FG) width of the central unit (width right cuspid − center of Cupid's bow + left cuspid width − center of the Cupid's bow); DF) right cuspid width − Cupid's bow center; EG) left cuspid width − Cupid's bow center; width of the right side unit and width of the left side unit. Overall, it was also possible to quantify the degree of asymmetry of the surface of the two hemilips, comparing the area of the right side segment with that of the left site. The area was calculated with the mathematical formula of (base × height)/2, where the height was represented by the segment between the cuspid of the Cupid's bow and its projection on the axis between the two commissures, while the base by the width of the lateral segment, previously calculated.
For surface defect, the following measurements were then calculated: DB) height of the right triangle; EC) height of the left triangle; DBF) area of the right lateral segment and ECG) area of the left lateral segment.
Esthetic Analysis
The esthetic results were evaluated using two questionnaires.
Esthetic Units Satisfaction Questionnaire
The first questionnaire was administered only to the patient's criticism. The patient was asked to complete the first questionnaire, which assessed satisfaction with the surgical treatment across several esthetic units: the general appearance of the face, lips, teeth, nose, and speech (Supplementary Material). For each parameter, the grade was indicated with one of the following values: 1 = not satisfied, 2 = satisfied, or 3 = very satisfied. [8].
2. Overall satisfaction questionnaire
The second questionnaire, a simplified four-point version of the Cleft Aesthetic Rating Scale (CARS) was used in this study, 9 and it's critiqued by the patient, the plastic surgeon, and a third blinded observer, a clinician experienced in facial esthetic evaluation and not involved in patient treatment. All evaluators completed the same questionnaire using identical items and rating scales. Standardized instructions were provided according to the evaluator's role. 10 Overall satisfaction with the surgical treatment was assessed by selecting one of the following responses: 1 = very good, 2 = good, 3 = satisfied, 4 = not satisfied.
Results
A total of 40 patients with UCL were included in the study: 20 (50%) underwent cheiloplasty according to the Millard technique and were included in Group 1 (Figure 2), and the other 20 (50%) underwent cheiloplasty according to the Tennison-Randall (Figure 3) technique and were included in Group 2.

Cleft lip repair, pre- and immediate post-operative, according to Millard Technique.

Cleft lip repair, pre- and immediate post-operative, according to Tennison-Randall Technique.
Mean SI and values were calculated for each anatomical parameter to assess postoperative lip symmetry.
Morphological Analysis
Postoperative lip symmetry was assessed in 40 patients using quantitative measurements from standardized frontal photographs. The SI was calculated for each of the five morphological parameters. Before performing statistical comparisons, we calculated descriptive statistics for each SI, including mean, standard deviation, median, minimum, and maximum values. Comparisons were made between patients treated with the Millard technique (n = 20) and those with the Tennison-Randall technique (n = 20) using the Mann-Whitney U test.
For vermilion height, no significant difference was observed between the Millard group (mean ± SD: 11.19% ± 11.17) and the Tennison-Randall group (10.18% ± 8.52) (p = .95). For prolabial height, the Millard group showed slightly lower asymmetry (6.46% ± 6.41) than the Tennison-Randall group (8.47% ± 7.45), though the difference was not statistically significant (p = .48). Regarding lateral lip width, the Tennison-Randall group had a higher SI (15.27% ± 9.51) than the Millard group (10.76% ± 7.91), without statistical significance (p = .15). For medial lip width, a statistically significant difference was found: Millard group showed better symmetry (10.24% ± 8.74) compared to Tennison-Randall (25.83% ± 23.45) (p = .014) (Figure 2). In terms of lip area, the Tennison-Randall group showed greater asymmetry (16.51% ± 13.48) than the Millard group (10.61% ± 9.09), though the difference was not statistically significant (p = .23).
A post-hoc power analysis was conducted to assess the significance of the observed difference in medial lip width (p = .014). Using the observed effect size (Cohen's d = .85 and α = .05), the achieved statistical power was 0.74. Although this indicates moderate sensitivity, the limited sample size suggests caution when interpreting this single significant finding.
Esthetic Analysis
Two separate questionnaires were used to assess esthetic outcomes from the perspective of patients, the operating surgeon, and a third blinded observer.
The Questionnaire 1 shows that patients treated with the Millard technique (Group 1) reported higher rates of being “very satisfied”: Face (35% vs. 5%), Lip (45% vs. 5%), Teeth (65% vs. 10%), Nose (35% vs. 5%), Speech (100% vs. 25%)
Additionally, the proportion of “not satisfied” responses was consistently lower in Group 1.
For questionnaire 2, the percentage of “very good” esthetic judgments was equal or higher for Millard compared to Tennison-Randall across all three observers: Patient (45% vs. 45%), Surgeon (25% vs. 25%), Third blinded observer (45% vs. 25%)
“Unsatisfactory” responses were equal or lower in the Millard group: Patient (0% vs. 5%), Surgeon (10% vs. 10%), Third blinded observer (10% vs. 10%).
The sum of “very good” and “good” responses was slightly in favor of Millard across all raters (Figure 4).
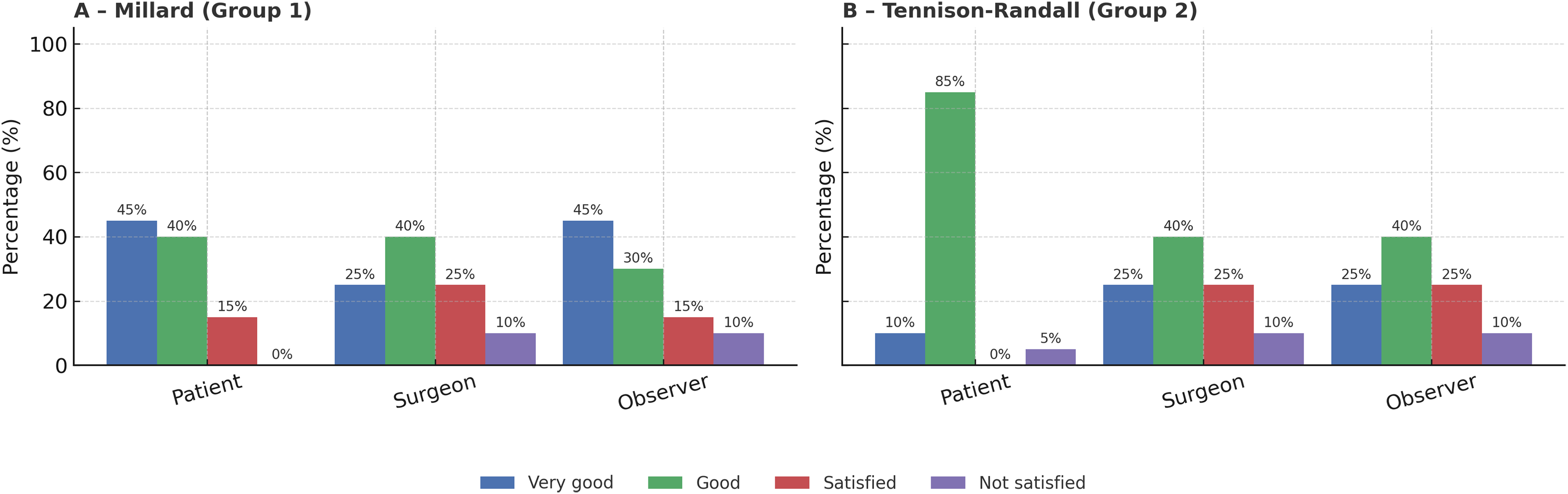
Questionnaire 2 ratings for Millard and Tennison-Randall groups by patients, surgeon, and blinded observer. “Very good” scores were equal or higher for Millard, while “not satisfied” responses were equal or lower. Overall, the combined “very good” + “good” ratings slightly favored the Millard’s technique.
Inter-rater reliability among the three evaluators (patient, surgeon, and blinded observer) was good, with an Intraclass Correlation Coefficient (ICC) of 0.82, confirming consistency in the subjective esthetic assessments.
Discussion
People with a cleft of the lip and/or palate (CL/P) differ from their peers due to their facial appearance, hearing and speech difficulties, and the significant time spent attending appointments and recovering from surgical interventions. These differences may affect life outcomes, including occupation, income, education, relationships, psychosocial health, and lifestyle choices. 11
The primary objective of cleft therapy has evolved from the mere correction of facial deformity to the comprehensive enhancement of the patient's quality of life (QoL). Modern multidisciplinary management aims to achieve satisfactory outcomes across esthetic, functional, and psychosocial domains. 12
Systematic reviews, including those by Queiroz and Mariano, have demonstrated that adults with CL tend to exhibit reduced health-related QoL, particularly in psychosocial and functional dimensions. Nevertheless, some evidence suggests that these individuals may develop adaptive resilience, reporting comparable well-being to non-cleft adults in certain areas.13,14
While the surgical management of CLP has been extensively investigated in pediatric populations, most studies have focused on short- to medium-term outcomes. Comparative analyses, such as those evaluating Pfeifer's wave-line procedure and Randall's technique, have reported no significant esthetic advantage of one method over the other in children.15–20
Conversely, limited data are available on long-term outcomes in adults. Peroz et al. observed that patients treated for unilateral cleft lip and palate (UCLP) generally report lower satisfaction with lip and facial appearance compared with non-cleft controls, although the number of secondary lip revisions does not appear to correlate with greater esthetic satisfaction. 21
More recently, Zhang et al. (2024) compared two techniques for orbicularis oris muscle reconstruction in unilateral incomplete CL, assessing postoperative morphology up to 3 years after surgery. 22 However, long-term data remain scarce.
In our study, we aimed to bridge this gap by analyzing long-term outcomes in 40 adult patients with unilateral CL treated in childhood. We analyzed the postoperative esthetic outcomes of unilateral CL repair using two well-established surgical techniques routinely used in parallel during the study period: Millard rotation-advancement and Tennison-Randall triangular flap.
Through a combined approach that incorporated objective morphometric analysis and subjective esthetic evaluation, we compared the results of the primary treatment at the end of growth of children affected by unilateral CL.
Our findings suggest that the Millard rotation-advancement technique yields significantly better medial lip symmetry and higher subjective satisfaction compared to the Tennison-Randall triangular flap. These results highlight how subtle geometric differences in flap design may influence long-term facial balance and perceived esthetics.
Furthermore, refinements such as the Mohler modification of Millard's method and Fisher's anatomical subunit approach continue to draw upon the same underlying principles of rotation, advancement, and muscular continuity. The present findings thus provide evidence-based context for understanding why the Millard concept remains widely taught and practiced, even as newer variations have emerged.
Our study also emphasizes the importance of integrating quantitative morphometric data with subjective perception. Although Tennison-Randall achieved comparable symmetry in lateral units, the overall esthetic impression favored Millard, likely due to superior Cupid's bow continuity, a more physiologic and linear scar that follows the natural curvature of the philtral ridge, and greater reproducibility of the surgical design across operators.
However, this study has several limitations that should be considered when interpreting the findings. First, its retrospective design limits control over confounding variables, and including only patients without secondary revisions may have favored those with more stable primary results. Nevertheless, case selection was based solely on data completeness and follow-up availability, with no intentional preference for one surgical technique, thus minimizing the risk of selection bias.
Second, the relatively small sample size (n = 40) restricts statistical power and reduces the generalizability of the results. While a post hoc power analysis demonstrated a moderate power (0.74) for the significant difference observed in medial lip width, the potential for a type I error cannot be entirely ruled out. Larger, multicentric studies are therefore needed to validate these findings with stronger statistical confidence.
Finally, the enduring popularity of the Millard technique should be interpreted as a reflection of its reproducibility, versatility, and integration within surgical training, rather than as evidence of absolute superiority. The present results demonstrate specific esthetic advantages associated with Millard's design, yet these should be understood within the broader historical and clinical context of technique evolution and surgeon familiarity.
Overall, these limitations indicate that the present investigation should be interpreted as a long-term observational comparison rather than a definitive hierarchy of surgical approaches. Nevertheless, our findings suggest that both techniques can achieve satisfactory long-term results, while the consistent superiority of the Millard method in medial symmetry, perceived esthetics, and reproducibility may help explain its enduring preference among surgeons. Moreover, subsequent modifications derived from Millard's original design continue to rely on the same fundamental principles of rotation and advancement, further supporting its lasting relevance in CL repair.
Conclusion
This study combined objective morphometric analysis and subjective evaluation to compare long-term esthetic outcomes in patients undergoing primary cheiloplasty with either the Millard or Tennison-Randall technique. While both approaches yielded comparable results across most morphological parameters, the Millard technique demonstrated significantly greater symmetry in the medial lip subunit, a key area for facial harmony. Subjective assessments, particularly those from patients, also tended to favor Millard-based reconstructions. Beyond objective measures, enhanced facial symmetry and esthetic satisfaction are closely related to psychosocial adjustment. Patients who perceive greater facial balance often report improved self-esteem, social confidence, and emotional well-being, underscoring the importance of esthetic harmony in long-term quality-of-life outcomes. 23
From a historical and clinical perspective, it is worth noting that Millard's technique remains the most widely used worldwide, while the Tennison-Randall technique has largely fallen into disuse.
In summary, despite the retrospective design and limited sample size, this study demonstrates that, over more than 2 decades of follow-up, the Millard rotation-advancement technique achieved superior esthetic symmetry and higher satisfaction scores than the Tennison-Randall method.
Our long-term findings support the continued popularity of the Millard technique, which persists not only for historical reasons but because it achieves objectively superior outcomes in facial esthetics and symmetry.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656261422855 - Supplemental material for What We Learnt in Unilateral Cleft Lip Repair Between Millard's and Tennison-Randall's Techniques: Comparison of the Outcomes in Adult Patients
Supplemental material, sj-docx-1-cpc-10.1177_10556656261422855 for What We Learnt in Unilateral Cleft Lip Repair Between Millard's and Tennison-Randall's Techniques: Comparison of the Outcomes in Adult Patients by Angelica Pistoia, Maria Ida Rizzo, Francesca R. Grippaudo, Marta Cajozzo, Francesca Grussu, Francesco Molinaro, Francesca Nascimben and Mario Zama in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656261422855 - Supplemental material for What We Learnt in Unilateral Cleft Lip Repair Between Millard's and Tennison-Randall's Techniques: Comparison of the Outcomes in Adult Patients
Supplemental material, sj-docx-2-cpc-10.1177_10556656261422855 for What We Learnt in Unilateral Cleft Lip Repair Between Millard's and Tennison-Randall's Techniques: Comparison of the Outcomes in Adult Patients by Angelica Pistoia, Maria Ida Rizzo, Francesca R. Grippaudo, Marta Cajozzo, Francesca Grussu, Francesco Molinaro, Francesca Nascimben and Mario Zama in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-3-cpc-10.1177_10556656261422855 - Supplemental material for What We Learnt in Unilateral Cleft Lip Repair Between Millard's and Tennison-Randall's Techniques: Comparison of the Outcomes in Adult Patients
Supplemental material, sj-docx-3-cpc-10.1177_10556656261422855 for What We Learnt in Unilateral Cleft Lip Repair Between Millard's and Tennison-Randall's Techniques: Comparison of the Outcomes in Adult Patients by Angelica Pistoia, Maria Ida Rizzo, Francesca R. Grippaudo, Marta Cajozzo, Francesca Grussu, Francesco Molinaro, Francesca Nascimben and Mario Zama in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgments
We would like to thank all the authors who contributed to the final editing of the manuscript, but also to the Italian Ministry of Health which made this study possible.
Ethical Approval
The parents of all patients included in the article were asked to sign in a written consent in order to use their data for scientifical purpose.
Author Contributions
AP and MIR conceived the idea for this case series. AP drafted the manuscript, reviewed and revised the manuscript and conducted the review of the literature. MIR and FRG coordinated and supervised data collection and critically reviewed the manuscript. MZ and MIR contributed to the diagnostic and therapeutic management of the patients. MIR, FN, FM, FRG, and MZ supervised the final writing of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Generative Artificial Intelligence in Scientific Writing
No Generative Artificial Intelligence was used in writing this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.