
Abstract
Objective
To evaluate the impact of maxillary position on orbitomalar and suborbital projection by comparing patients with and without cleft with normal and retrusive maxilla, and to determine whether projection loss is primarily related to cleft pathology or maxillary retrusion.
Design
Retrospective comparative cephalometric study.
Setting
Single tertiary orthodontic center; records from 2010 to 2015.
Patients
A total of 142 patients (74 with cleft, 68 without cleft) aged 7 to 13 years, meeting defined inclusion criteria. Patients were divided into 4 groups according to cleft status and maxillary AP position determined by SNA: retrusive maxilla with cleft (RCMx, n = 44), normal maxilla with cleft (NCMx, n = 30), retrusive maxilla without cleft (RMx, n = 28), and normal maxilla without cleft (NMx, n = 40).
Interventions
No intervention was performed.
Main Outcome Measures
Linear orbitomalar projection measurements (LOr-VP, IOr-VP, AOr-VP, SbOr1-VP, SbOr2-VP) and maxillary position parameters (SNA, ANS-VP, A-VP). Group comparisons and correlation analyses were performed using non-parametric statistics.
Results
Significant intergroup differences were observed for all orbitomalar and suborbital projection measurements (P < .05). Patients with retrusive maxilla, regardless of cleft status, demonstrated lower orbital and suborbital projection values compared with those with normal maxillary position. Suborbital parameters showed the largest variation between groups. Moderate-to-strong positive correlations were found between maxillary anterior development (SNA, ANS-VP, A-VP) and orbitomalar projection.
Conclusion
Maxillary retrusion, rather than cleft status, appears to be a key determinant of reduced orbitomalar projection and midfacial convexity. In patients with retrusive maxilla, correction of midfacial deficiency may require consideration of infraorbital and zygomatic support in addition to maxillary advancement.
Introduction
Children born with cleft lip and palate (CLP) experience disruptions in the hard and soft tissues of the nasomaxillary skeleton, leading to developmental abnormalities in facial structures due to embryological, intrinsic, and surgery-related factors.1,2 While the most apparent deficiencies are observed in areas adjacent to the cleft, such as the maxilla, nose, and lips2,3 studies have also reported morphological changes in the upper face, malar region, skull base, and clivus.4–6 However, deficiencies in the orbital and zygomatic regions have not been widely studied, despite the nose, the prominence of the zygoma, and the chin being key determinants of facial aesthetics. 7 Projection of the orbitomalar region contributes significantly to midfacial contour and sagittal convexity. Deficiencies in this area are known to flatten the midface profile and may negatively affect both aesthetic outcomes and facial harmony, especially in reconstructive and orthognathic planning.
Maxillary retrusion and orbitomalar morphology represent complex components of midfacial structure that have an inherent 3-dimensional character, particularly evident in soft tissue contour and overall facial convexity. While 3-dimensional imaging techniques may offer more detailed information in this respect, lateral cephalometric analysis has been widely used in the literature to evaluate skeletal relationships of the maxilla and orbitomalar region.8–11 In clinical and research settings, 2-dimensional skeletal measurements continue to provide a practical and reproducible framework for assessing sagittal maxillary position 12 and its association with orbitomalar projection, despite their recognized limitations in fully capturing 3-dimensional morphology. In the present study, cleft-specific cephalometric cut-off values were not defined. Instead, widely accepted normative values that have been consistently used in the literature to evaluate maxillary hypoplasia in cleft populations were employed to allow standardized comparison across groups.
In cases with CLP, the nasomaxillary structures are often positioned retrusively. The effect of this position on the orbitomalar region has been previously investigated by comparing CLP cases with skeletal Class I individuals without cleft. 13 In that study, suborbital projection was significantly reduced in the CLP group, and a positive correlation was observed between the anterior development of the orbitomalar region and the maxilla. 8 However, the degree of maxillary retrusion was not specifically controlled. This represents a common limitation in the existing literature, where comparisons between patients with cleft and those without cleft are often made without stratifying for sagittal maxillary position—potentially obscuring the independent effects of skeletal retrusion on orbitomalar projection.
Although previous work has demonstrated reduced orbitomalar projection in patients with cleft, the independent contribution of maxillary anteroposterior position has not been delineated. To clarify this relationship, the present study evaluated patients with and without cleft while accounting for maxillary anteroposterior position to determine whether midfacial projection loss is primarily driven by cleft-related skeletal disruption or by maxillary retrusion. This approach allows a more precise differentiation of the skeletal components determining anterior midfacial projection and provides a clearer framework for understanding the impact of maxillary position on orbitomalar morphology.
Materials and Methods
Approval was obtained from the local ethics committee of our hospital before the study. Written consent was obtained from the parents of all the patients included in the study. The individuals included in the study (with and without cleft) were divided into 4 groups. Groups were designated according to the anteroposterior position of the maxilla (SNA) and whether they had cleft palate or not. In this classification, an SNA angle less than 78° was considered indicative of maxillary retrusion, while values between 78° and 82° were accepted as normal, based on cephalometric norms reported in the literature.14,15
Retrusive positioned cleft maxilla (RCMx) Normally positioned cleft Maxilla (NCMx), Retrusive positioned maxilla without cleft (RMx) and Normally positioned maxilla without cleft(NMx) groups.
The medical records and cephalometric images of the patients who had undergone orthodontic and orthognathic treatment for unilateral or bilateral complete cleft lip and palate (CLP) in a single center between 2010 and 2015 were analyzed retrospectively. Patients with cleft were consecutive cases treated and followed in the same cleft unit. All cleft patients underwent primary surgical repair performed by the same surgical team using standardized protocols. Patients without cleft were selected from the same center and sourced from the same radiographic archive, and the same inclusion criteria regarding age and availability of pre-treatment lateral cephalograms were applied. The groups were matched by age range and cephalometric imaging protocol to ensure comparability.
Inclusion criteria in the study group were as follows:
Complete unilateral or bilateral CLP, Absence of craniofacial anomalies or syndromes, Completion of CLP repairs within 18 months, Undergoing the same surgical techniques were used for lip and palate repair (modified Millard for the lip, V-Y pushback palatoplasty for unilateral cleft palate, 2 flap palatoplasty for bilateral cleft palate), Absence of pre-surgical orthodontic treatment Being 7 to 13 years old before orthodontic treatment and Having lateral cephalometric X-ray images before alveolar bone grafting.
Inclusion criteria in the group without cleft were as follows:
Absence of craniofacial anomalies or syndromes, Physically healthy and having Class I-Class III maxillomandibular relationship, Being 7 to 13 years old before orthodontic treatment.
Cephalometric Analysis
In all cases, a lateral cephalometric X-ray (PM 2002 CC Proline; Planmeca) was taken after the head was positioned with the Frankfort Horizontal Plane parallel to the ground, the teeth in centric occlusion, and the lips in a relaxed position. The data and images in the X-rays were corrected according to the level of magnification in all cases. All radiographs were taken using a cephalostat to ensure consistent head positioning, and magnification was standardized across cases. Reference points, planes, and angles to be used in measurements on cephalometric x-rays were determined (Figure 1). All tracings and measurements were performed manually. In order to minimize the measurement error, all cephalometric evaluations were made by a single practitioner(to avoid differences between observers), an orthodontist with more than 3 years of experience in cephalometric analysis and craniofacial assessment and repeated 3 times with an interval of 2 weeks. Mean values of the measurements were included in the analyses. Pearson's correlation coefficient was used to examine intraclass variability. The correlation coefficient was above .90 in all reference measurements, confirming no intraclass variability. A total of 5 parameters representing the orbitomalar region were defined as follows: LOr-VP (mm): Distance between the lateral part of the orbital and the vertical plane IOr-VP (mm): Distance between the inferior part of the orbital and the vertical plane AOr-VP (mm): Distance between the anterior segment of the orbital and the vertical plane SbOr1-VP (mm): Distance between suborbital-1 and the vertical plane SbOr2-VP (mm): Distance between suborbital-2 and the vertical plane
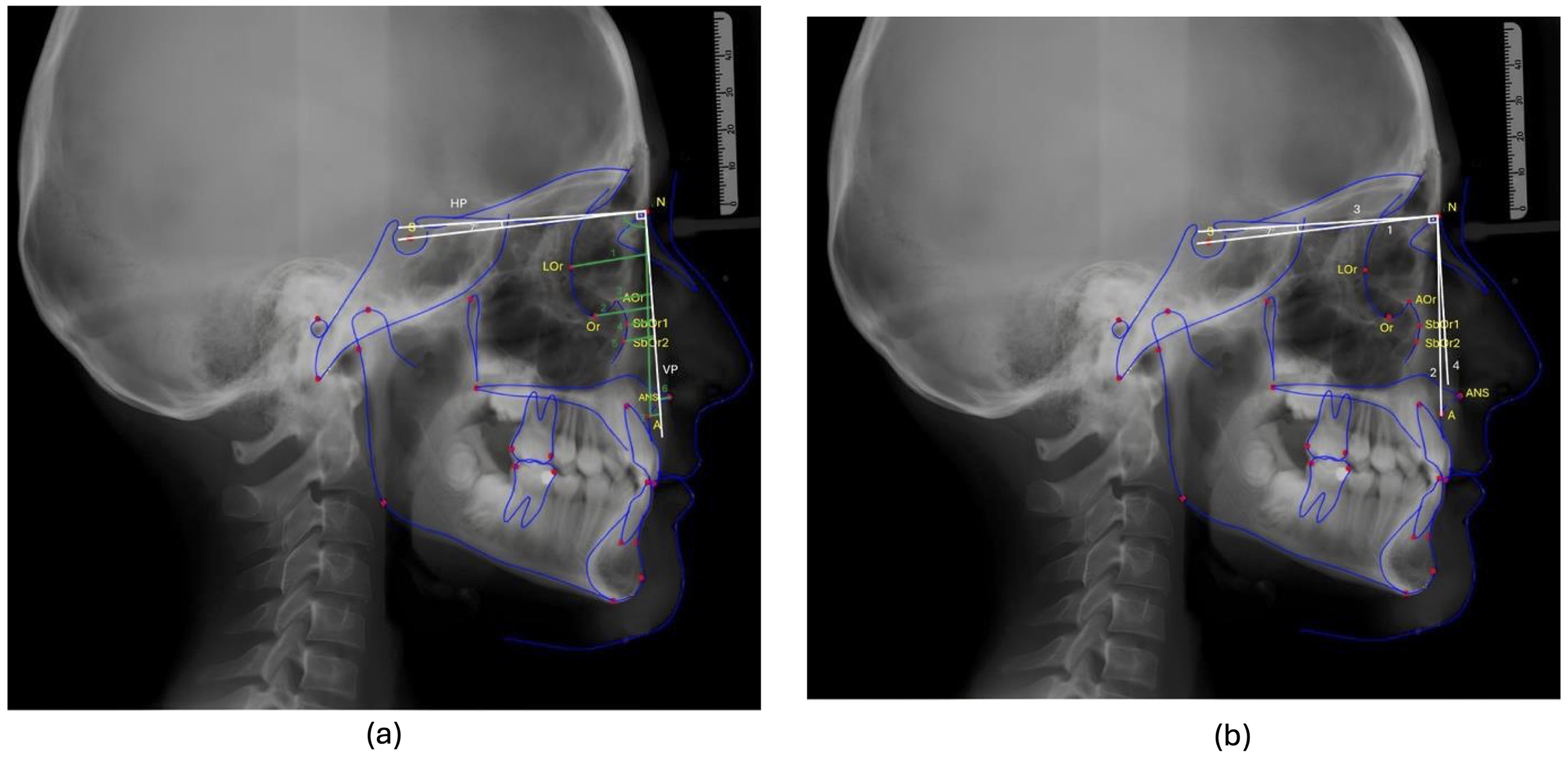
(a) The reference points used in the lateral cephalometric analysis are as follows: S (sella): it is the geometric middle of the sella turcica (sphenoid bone). N (Nasion): It is the most forward point of the frontonasal suture in the midsagittal plane. Or (Orbitale): It is the lowest point of the inferior edge of the orbit. ANS (Anterior Nasal Spine): It is the most extreme point of the bony prominence of the maxilla at the base of the anterior nasal opening. Point A: It is the deepest point of the bony concavity extending from the spina nasalis anterior to the upper incisor in the mid-occlusal plane. (1) SN line: It is the line passing through the S and N points. (2) NA line: It is the line passing through the points N and A. (3) HP: The plane formed from the point N at an angle of 7° to the SN plane. (4) VP (Vertical Plane): It is perpendicular to the horizontal plane descended from the point N. (b) The angle and planes used in the lateral cephalometric analysis are as follows: (1) LOr-VP (mm): It is the distance between the most lateral point of the orbit and the vertical plane. (2) IOr-VP (mm): It is the distance between the most inferior point of the orbit and the vertical plane. (3) AOr-VP (mm): It is the distance between the most anterior point of the orbit and the vertical plane. (4) SbOr1-VP (mm): It is the distance between the suborbital and the most protrusive point of the orbital cavity and the vertical plane. (5) SbOr2-VP (mm): It is the distance between 3 mm inferior of the suborbital-1 point and the vertical plane. (6) ANS-VP (mm) (maxilla anterior-posterior position-1): It is the distance between the ANS point and the vertical plane. (7) A-VP (mm) (maxilla anterior-posterior position-2): It is the distance between point A and the vertical plane. SNA (°): It is the posteroinferior angle formed between the SN line passing through the S and N points and the NA line passing through the N and A points. It gives information about the sagittal position of the apical base of the maxilla relative to the skull base (normal value is 80 ± 2°). Although the 4 groups were unequal in size, the overall sample provided adequate statistical power. Power analysis indicated that the study was sufficiently powered (80%, α = .05) to detect moderate effect sizes across multiple parameters.
Among these, the first 3 parameters (LOr-VP, IOr-VP, and AOr-VP) were used to represent the orbital region, whereas the remaining 2 (SbOr1-VP and SbOr2-VP) represented the suborbital region. The values of these parameters were compared between all groups, and their correlation with other craniofacial parameters was also investigated.
Statistical Analysis
The data obtained in this study were analyzed using the IBM SPSS Statistics software, version 22. The Kolmogorov-Smirnov test was applied to assess the normality of the data distribution. Since the majority of variables did not meet the assumptions of normal distribution, non-parametric tests were employed. Therefore, the Kruskal-Wallis test was used for group comparisons, and Spearman's rank correlation was selected for correlational analysis.
Correlation coefficients were interpreted based on the following thresholds: .00 to .30 as weak, .30 to .70 as moderate, and .70 to 1.00 as strong correlation. 16 The level of statistical significance was set at .05. A P-value less than .05 was considered statistically significant, whereas a P-value greater than .05 indicated a lack of significant difference or association.
Results
Descriptive Statistical Findings
Out of 142 patients included in the study, 74 had unilateral/bilateral cleft lip and palate, while 68 patients were patients without cleft. Among patients with cleft lip and palate, 44 had maxillary retrusion (RCMx), while 30 had a normally developed maxilla (NCMx). In the group without cleft, 28 patients had maxillary retrusion (RMx), and 40 had a normally positioned maxilla (NMx). In the (RCMx) group, %47.7 of the patients were female, and %52.3 were male. In the (NCMx) group, %36.7 of the patients were female, and %63.3 were male. Mean age was 9.90(+-2.24) in the (RCMx) group, 9,742.34) in the (NCMx) group, 10.11(±1.19) in the (RMx) group, and 10.33(±1.41) in the (NMx) group. There was no significant difference between the study groups in terms of age and gender. The gender and age distribution of the cases are shown in Table 1.
Demographic Characteristics of the Groups.
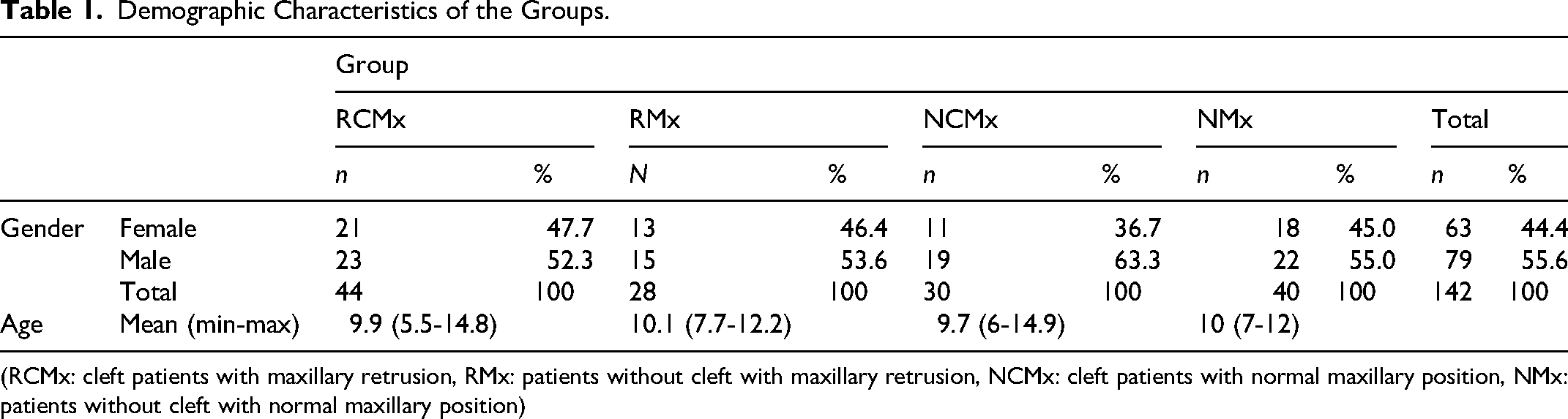
(RCMx: cleft patients with maxillary retrusion, RMx: patients without cleft with maxillary retrusion, NCMx: cleft patients with normal maxillary position, NMx: patients without cleft with normal maxillary position)
Linear Measurement Findings
Table 2 presents the mean and standard deviation (SD) values of orbitomalar and maxillary anteroposterior parameters for each group, along with the corresponding P-values from the Kruskal-Wallis test.
Comparison of Orbitomalar and Maxillary Anteroposterior Parameters Among the 4 Study Groups.
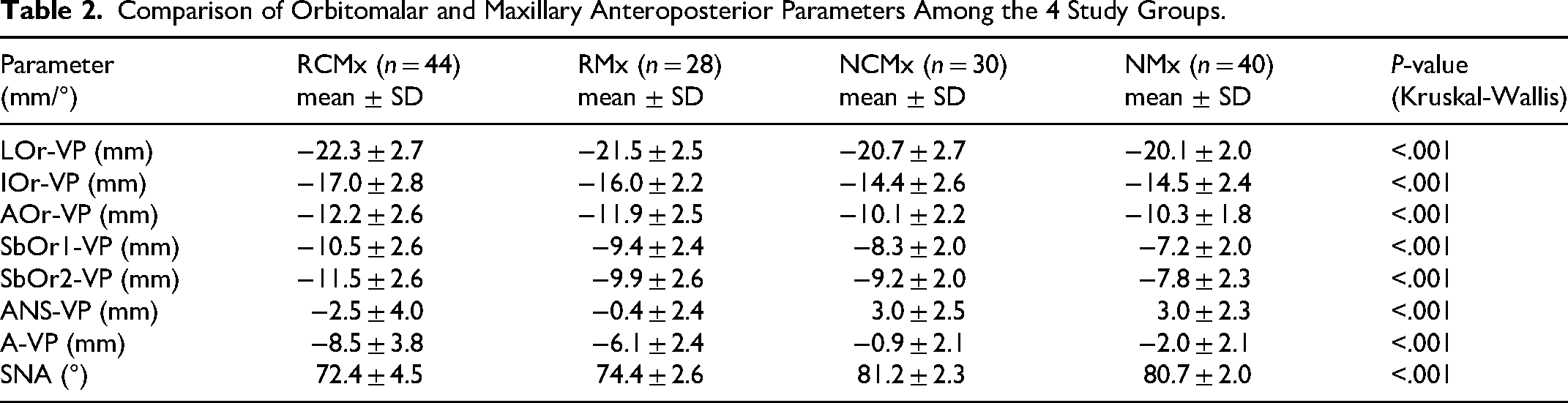
The mean values of the parameters representing the orbitomalar region were evaluated between the groups (Figure 2). Accordingly: LOr-VP (mm) was −22.3 mm in the (RCMx), −21.5 mm in the (RMx), −20.7 mm in the (NCMx), and −20.1 mm in the (NMx) group. IOr-VP (mm) was −17.0 mm in the (RCMx), −16.0 mm in the (RMx), −14.4 mm in the (NCMx), 14.5 mm in the (NMx) group. AOr-VP (mm) was −12.2 mm in the (RCMx), −11.9 mm in the (RMx), −10.1 mm in the (NCMx), and −10.3 mm in the (NMx) group. SbOr1-VP(mm) was −10.5 mm in the (RCMx), −9.4 mm in the (RMx), −8.3 mm in the (NCMx), and −7.2 mm in the (NMx) group. SbOr2-VP (mm) was −11.5 mm in the (RCMx), −9.9 mm in the (RMx), −9.2 mm in the (NCMx), and −7.8 mm in the (NMx) group.
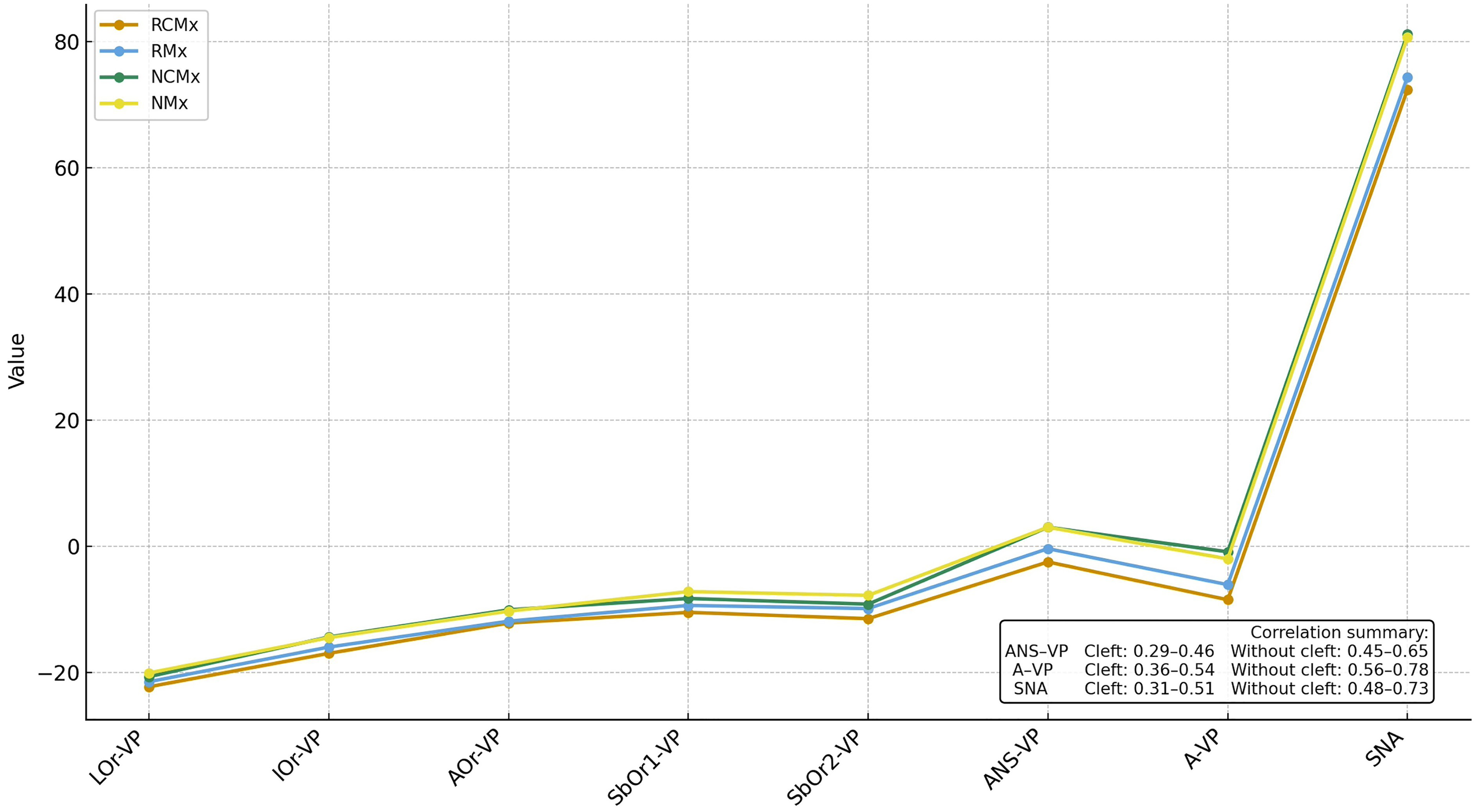
Illustrates the mean values of all orbitomalar and maxillary anteroposterior parameters across the 4 study groups (RCMx, RMx, NCMx, NMx). The graphical comparison highlights the progressive decrease in projection from normally positioned to retrusive maxillae, with and without-cleft groups showing similar trends when maxillary retrusion is present. An inset box summarizes the correlation ranges between orbitomalar parameters and maxillary AP indicators (ANS-VP, A-VP, SNA) for patients with and without cleft.
Comparison of the Parameters of the Orbitomalar Region Between the Groups
Table 2 and Figure 2 present a comparison of orbitomalar region parameters between the study groups. Significant differences were observed in the projection parameters of the lateral, inferior, and anterior orbital points—specifically Lor-VP (mm), IOr-VP (mm), AOr-VP (mm), SbOr1-VP (mm), and SbOr2-VP (mm)—with all showing statistical significance (P < .05).
LOr-VP (mm) values in the RCMx group are significantly lower than those in the (NMx) group.
IOr-VP (mm), AOr-VP (mm), SbOr1-VP (mm), and SbOr2-VP (mm) values in the (RCMx) group are significantly lower than those in the (NCMx) group and (NMx) group.
AOr-VP (mm) values in the (RMx) group are significantly lower than those in the (NCMx) and (NMx) groups.
SbOr1-VP (mm) and SbOr2-VP values in the (RMx) group are significantly lower than those in the (NMx) group.
Detailed descriptive statistics and full pairwise comparisons are provided in Supplementary Table 2.
Correlation between parameters of the orbitomalar region and parameters of maxillary anteroposterior position in patients with and without cleft; correlation analysis between the parameters of the orbitomalar region and the parameters of maxillary anteroposterior position in patients with cleft, with and without maxillary retrusion:
Maxilla anterior posterior position-1 (ANS-VP (mm)) showed a moderate positive correlation with the IOr-VP(mm) (r:0398), AOr-VP(mm) (r:0412), SbOr1-VP(mm) (r:0459), and SbOr2-VP(mm) (r:0456) (P < .05).
Maxilla anterior-posterior position-2 (A-VP (mm)) showed a moderate positive correlation with the Lor-VP(mm) (r:0355), IOr-VP(mm) (r:0476), AOr-VP(mm) (r:0477), SbOr1-VP(mm) (r:0529), and SbOr2-VP(mm) (r:0538) (P < .05).
SNA (°) showed a moderate positive correlation with the Lor-VP(mm) (r:0312), IOr-VP(mm) (r:0,43), AOr-VP(mm) (r:0447), SbOr1-VP(mm) (r:0512), and SbOr2-VP(mm) (r:0514) (P < .05).
Correlation analysis between the parameters of the orbitomalar region and the parameters of maxillary anteroposterior position in individuals without cleft, with and without maxillary retrusion:
Maxilla anterior posterior position-1 (ANS-VP (mm)) showed a moderate positive correlation with the Lor-VP(mm) (r:0454), IOr-VP(mm) (r:0528), AOr-VP(mm) (r:0567), SbOr1-VP(mm) (r:0651), and SbOr2-VP(mm) (r:0636) (P < .05).
Maxilla anterior-posterior position-2) (A-VP (mm)) showed a moderate positive correlation with the Lor-VP(mm) (r:0561), IOr-VP(mm) (r:0646), AOr-VP(mm) (r:0698), and a strong positive correlation with the SbOr1-VP(mm) (r:0781) and SbOr2-VP(mm) (r:0751) (P < .05).
SNA (°) showed a moderate positive correlation with the Lor-VP(mm) (r:0,48), IOr-VP(mm) (r:0545), AOr-VP(mm) (r:0617), SbOr2-VP(mm) (r:0697) and a strong positive correlation with the SbOr1-VP(mm) (r:0727) (P < .05).
Discussion
The aim of this study was to examine how maxillary anteroposterior position relates to orbitomalar and suborbital projection in patients with and without cleft lip and palate. By evaluating both groups according to maxillary position, the study intended to provide a clearer view of whether projection differences are associated with cleft status or with maxillary retrusion itself. The overall findings indicate that maxillary position contributes to midfacial projection, providing additional context for understanding the skeletal factors that may influence orbitomalar morphology in different patient groups.
In this study, the division of patients into 4 groups according to maxillary anteroposterior position (SNA) and cleft presence allowed for a more systematic evaluation of orbitomalar projection differences. This methodological distinction is crucial, as failing to account for maxillary position when comparing cleft patients to controls may lead to misinterpretations of the data. Our findings emphasize that accurate assessment of orbital and suborbital morphology requires a nuanced evaluation of maxillary development, rather than a simple comparison based solely on cleft status. Previous work has demonstrated that suborbital projection is significantly reduced in patients with cleft compared with control subjects; however, no significant differences were observed between unilateral and bilateral cleft subtypes. 13 In that study, lateral, inferior, and anterior orbital parameters were comparable across cleft subgroups, and the associations between orbitomalar projection and maxillomandibular development were consistent irrespective of cleft type. 13 These observations suggest that cleft subtype may have a limited effect on orbitomalar morphology within the context of sagittal maxillary assessment. Accordingly, unilateral and bilateral cleft cases were evaluated as a single cleft group in the present study to allow a clearer interpretation of differences related to maxillary anteroposterior position.
The distribution of age and gender across the study groups showed no significant differences, suggesting that these factors did not introduce bias into the comparisons. Ensuring homogeneity in demographic variables is important when evaluating skeletal characteristics, as age and sex-related growth differences can influence craniofacial morphology. 17 Previous studies have reported that sex-based differences in midfacial development become more pronounced during puberty, particularly due to hormonal influences on bone growth and remodeling. 17 Since the present study focused on patients aged 7 to 13 years, a period before significant pubertal growth acceleration, it is likely that skeletal growth patterns were relatively comparable among participants.
While 3-dimensional assessment techniques—such as CT-based volumetric analysis and surface evaluations of facial convexity—provide a more comprehensive representation of maxillary morphology, lateral cephalometry remains the widely used tool for evaluating sagittal maxillary position in both clinical orthodontics and cleft research due to its accessibility, reproducibility, and long-standing normative database.8–11,18,19 The anterior cranial base completes the majority of its growth within the first years of life and remains relatively stable thereafter, allowing cephalometric planes such as S-N to serve as reliable reference structures for assessing anteroposterior.20–22 Accordingly, angular parameters including SNA continue to be used as standard diagnostic indicators in pre-treatment evaluation of maxillary retrusion, even in cleft populations, where they provide a reproducible method for quantifying maxillary position relative to the cranial base. To our knowledge, no population-specific thresholds defining maxillary retrusion have been established for individuals with cleft; therefore, virtually all cephalometric studies in the cleft literature evaluate maxillary position by referencing normative values derived from individuals without cleft. Numerous investigations have used reductions in SNA relative to these norms to characterize maxillary hypoplasia in cleft cohorts, supporting its continued relevance as a sagittal reference.23–25 While SNA does not capture the full 3-dimensional complexity of midfacial morphology, using this standard reference framework allows the findings of the present investigation to remain comparable with the existing cleft literature while addressing its methodological gap by stratifying patients according to maxillary anteroposterior position. However, it should be acknowledged that 3-dimensional imaging modalities, including surface-based facial convexity analyses and volumetric assessments, have the potential to offer complementary information regarding midfacial contour and projection. Future studies incorporating 3-dimensional evaluation may therefore be valuable to corroborate and further refine the skeletal relationships observed in 2-dimensional cephalometric analyses.
Interpretation of Intergroup Differences
The study groups revealed significant differences in the lateral, inferior, anterior, and suborbital projections (LOr-VP, IOr-VP, AOr-VP, SbOr1-VP, SbOr2-VP). Both patients with cleft and individuals without cleft with maxillary retrusion (RCMx and RMx) showed significantly lower orbitomalar projection values than their normally positioned counterparts, confirming the role of maxillary position in midfacial projection. These findings are consistent with previous research indicating that maxillary retrusion leads to midfacial deficiency, affecting both the infraorbital rim and malar projection6,26,27 and also supported by the displacement theory of facial bone development, which suggests that maxillary hypoplasia can result in secondary changes in adjacent skeletal structures, including the orbitomalar complex.17,28
Among all findings, the most pronounced discrepancies were observed in the suborbital region (SbOr1-VP and SbOr2-VP), where the RCMx group exhibited the most retrusive measurements.
The findings further indicate that the presence of cleft lip and palate does not have a statistically significant impact on the orbital rim area. Similar sagittal projections of the orbital rim have been observed in both unilateral CLP cases and control groups in craniofacial CT-based evaluations, consistent with the present results. 29 A previous investigation comparing the cleft and without-cleft skeletal Class I groups also reported comparable results. 13 Hovewer, a key limitation of that study was the lack of control for maxillary position, which could be a confounding factor. The absence of a statistically significant difference between the cleft and without-cleft groups in the present study indicates that the factor affecting orbitomalar projection is the position of the maxilla rather than cleft status. Supporting this, correlation analyses revealed a positive association between maxillary anterior development and orbital rim projection, emphasizing that maxillary growth plays a primary role in shaping orbital morphology. This is consistent with findings from Posnick et al., 26 who observed flattened cheekbones in patients with skeletal Class III deformities. On the other hand, the present results are different from some earlier studies.29,30 For instance, Zheng et al. 30 compared only UCLP patients with maxillary retrusion to a skeletal Class I control group, potentially overlooking variations in sagittal maxillary development that cannot be captured solely by ANB values. Interestingly, when comparing individuals with normal maxillary position across the cleft and without-cleft groups, we found that although the ANS and A point appeared more anterior in cleft cases, suborbital projection was still less pronounced (Table 2). When the correlation tables for the cleft and without-cleft groups are examined separately, the correlation coefficients are found to be higher in the without-cleft group. This suggests that the loss of anatomical integrity in the premaxilla and lateral maxillary segments, which is frequently observed in CLP patients, may disrupt the pacemaker effect of the nasal septum on midface development.31,32 As a result, this disruption may contribute to sagittal growth retardation in the midface, potentially worsening maxillary retrusion and suborbital projection deficiencies. However, the relatively small difference between the NCMx and NMx groups suggests that when maxillary development is preserved, the structural integrity and the coordination of midfacial growth are maintained, resulting in a stronger coupling between the maxilla and the orbitomalar complex.
Interpretation of Correlation Analysis Results
A key finding of this study is the moderate-high positive correlation between the maxillary anterior-posterior position (ANS-VP and A-VP) and orbitomalar parameters (Lor-VP, IOr-VP, AOr-VP, SbOr1-VP, and SbOr2-VP) across all groups. This suggests that forward maxillary development is associated with a more anteriorly positioned orbitomalar region, confirming the role of maxillary growth in midfacial projection. As mentioned before, this finding aligns with previous research indicating that midfacial hypoplasia, particularly maxillary retrusion, significantly impacts orbitomalar morphology, leading to infraorbital and anterior orbital deficiencies. 33 Among the orbital components, the lateral orbital wall exhibited the weakest correlation with maxillary position, suggesting that this region may be influenced by additional craniofacial factors.
Interestingly, when the correlation table derived solely from cleft patients was compared to that of the group without cleft, the correlation coefficients were found to be stronger in the group without cleft (Table 3). This suggests that in individuals without cleft, maxillary retrusion alone may have a more direct impact on orbitomalar projection. In contrast, in cleft patients, additional factors—such as nasal septal disruption, loss of maxillary integrity, and altered craniofacial growth patterns—may contribute to orbitomalar deficiencies.1,34 The loss of anatomical continuity in the premaxilla and lateral maxillary segments may interfere with the pacemaker effect of the nasal septum on midface development, 32 reduce the reciprocal interactions that support bone graft integration, and alter natural growth patterns, thereby weakening the relationship between maxillary development and orbitomalar projection in CLP patients due to the combined effects of structural discontinuity, septal growth disruption, and growth-modifying surgical interventions.31,32,35
The Table Presents the Correlation Coefficients and Corresponding P-Values for Each variable Across Different Structural Groups, Derived From Patients With and Without Cleft. Correlation Analyses Were Performed Separately for These Groups, and Statistically Significant Results (P < .05) Are Highlighted.

Beyond the direct correlations observed between maxillary position and orbitomalar projection, it is important to consider the biological mechanisms underlying midfacial growth. One such factor is the nasal septum and vomer, which serve as critical regulators of maxillary advancement. The nasal septum exerts a pacemaker effect on maxillary growth, guiding its forward and downward movement during craniofacial development.31,36 The vomer, as the bony extension of the nasal septum, maintains structural continuity with the maxillary and palatal segments, contributing to midfacial stability. 17 In individuals with CLP, disruption of the septo-maxillary complex may weaken this growth stimulation, leading to maxillary retrusion and consequently reduced orbitomalar projection.34,37
This hypothesis aligns with the present findings, where maxillary retrusion was consistently associated with reduced orbitomalar projection across all groups. The pacemaker effect of the nasal septum 32 may explain why even cleft cases with normal maxillary positioning exhibited a less prominent suborbital projection despite A-point being more anteriorly located. The loss of continuity between the nasal septum, vomer, and maxillary segments in CLP cases may contribute to the loss of coordinated midfacial development, particularly in the sagittal plane. This further highlights the need to consider nasal septal integrity as a contributing factor when assessing maxillary growth deficiencies and their impact on orbitomalar morphology.
Limitations
Although lateral cephalometric analysis provides valuable 2-dimensional data on skeletal relationships, it does not fully reflect the 3-dimensional complexity of midfacial morphology. Furthermore, since this study addressed only skeletal measurements, the potential roles of soft tissue dynamics, airway function, and neuromuscular adaptation in orbitomalar projection remain to be explored.
Variations in cranial base flexure can influence angular cephalometric measurements such as SNA by changing the orientation of the maxilla relative to the cranial base. Even though all radiographs in the present study were taken under standardized head positioning, individual differences in cranial base morphology may still affect sagittal measurements. In a previous analysis involving a comparable cleft cohort, no meaningful differences in the N-S-Ba angle were found either between cleft subtypes or between cleft and without-cleft groups. 13 This suggests that cranial base angulation did not vary substantially within that sample. However, this should not be taken to mean that cranial base morphology has no impact, as its influence on SNA-based grouping cannot be entirely ruled out. For this reason, cranial base flexure is acknowledged as a potential source of methodological bias in the interpretation of the present findings.
In addition to these anatomical and methodological limitations, the statistical approach used to assess measurement repeatability also requires clarification. In the present study, intra-operator repeatability was assessed using correlation coefficients. Although high correlation values indicate consistency between repeated measurements, correlation analysis primarily reflects the strength of association rather than absolute agreement. Therefore, this approach may not fully capture systematic measurement differences, and minor intra-operator variability cannot be completely excluded. This methodological aspect should be considered when interpreting the precision of the cephalometric measurements.
In interpreting these findings, it is essential to differentiate statistical significance from clinical significance and from the degree to which patients perceive these differences. While several orbitomalar parameters demonstrated statistically significant variation between groups, such differences may be small in magnitude and may not translate into clinically appreciable changes in midfacial contour. Moreover, patient-perceived midfacial flatness or asymmetry often reflects complex soft-tissue interactions that are not fully captured by skeletal measurements alone. Accordingly, the results should be evaluated not only within a statistical framework but also in relation to their clinical impact and relevance to patient-centered aesthetic outcomes. In clinical practice, each individual must be evaluated on a case-by-case basis; however, the findings of this study reflect statistical averages. These results cannot be directly generalized to every patient, but they can help clinicians focus their attention on specific patterns or areas of potential relevance.
It is also important to consider the biological mechanisms underlying orbital development. The orbits serve as a structural bridge between the face and the cranium, and their development is inherently complex. As the junction between cranial membranous bones and basal enchondral bones, the orbital region is shaped by multiple developmental factors. Since this study emphasizes the connection between maxillary and orbital development, understanding their embryological origins is essential. Almost all skeletal components of the midface, including the maxilla and orbit, originate from neural crest cells derived from the anterior, mid, and hindbrain regions.38,39 Disruptions in the migration or differentiation of these cells during development may result in craniofacial anomalies. In particular, appositional growth and bone deposition in the maxilla—which forms the floor and medial wall of the orbit—play a direct role in shaping orbital morphology.
Taken together, these developmental and morphological findings have important clinical implications. These results highlight the importance of evaluating orbitomalar projection as an integral part of midfacial growth assessment, particularly in individuals with maxillary retrusion. In cleft patients with maxillary hypoplasia, infraorbital retrusion should be carefully considered during treatment planning, as maxillary advancement alone may not be sufficient to restore suborbital contour.29,30 It remains to be clarified whether linear skeletal deficiencies correspond to volumetric deficits in the orbitomalar region and whether soft-tissue adaptations compensate for underlying bony retrusion.
Conclusion
In this study, both cleft and non-cleft individuals with maxillary retrusion demonstrated reduced orbitomalar and suborbital projection, indicating that diminished midfacial projection is closely associated with the anteroposterior position of the maxilla. When the maxillary position was within normal limits, orbitomalar projection remained comparable across cleft and non-cleft groups. These findings suggest that maxillary retrusion, rather than cleft status alone, plays a central role in shaping anterior midfacial projection.
From a clinical standpoint, the results highlight the importance of evaluating maxillary position when planning treatment for midfacial deficiency. In patients with cleft and maxillary retrusion, correction of the maxilla may need to be complemented by additional procedures to enhance infraorbital support, depending on individual skeletal presentation. Future studies using 3-dimensional imaging and volumetric assessment are needed to better define the relationship between maxillary morphology and orbitomalar projection and to validate these findings across broader craniofacial patterns.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656261418522 - Supplemental material for Evaluation of Orbitomalar Region Projection İn Patients With Operated Cleft Lip and Palate Part 2: Effect of Maxillary Position
Supplemental material, sj-docx-1-cpc-10.1177_10556656261418522 for Evaluation of Orbitomalar Region Projection İn Patients With Operated Cleft Lip and Palate Part 2: Effect of Maxillary Position by Gülce Tosun, Alihan Özdemir, Ayşe Gülşen, Mert Doruk, Serhat Şibar and Neslihan Üçüncü in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to all colleagues and collaborators from Gazi University who contributed to this research. OpenAI was used solely for language refinement; all scientific content, analyses, and interpretations remain the responsibility of the authors.
Ethical Approval
This study was approved by the Ethics Committee of Gazi University, Faculty of Dentistry (Approval Code: 2024-1215; Approval Date: July 31, 2024). The research was conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Author Contributions
All authors contributed to the conception and design of the study, data collection, analysis, and interpretation. All authors reviewed and approved the final version of the manuscript before submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author, Dr. Gülce Tosun, upon reasonable request.
Statement on Tracked Changes and Comments
All tracked changes and comments have been removed from the submitted manuscript to ensure full anonymization. No identifying information remains in the document metadata.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.