
Abstract
Objective
To investigate operative experiences and perspectives of surgeons presented with cleft lip (CL) and/or palate (CP) in children with life-limiting and terminal illnesses.
Design
Survey study.
Setting
Electronic.
Patients, Participants
American Cleft Palate Craniofacial Association surgeon members.
Interventions
None.
Main Outcome Measures
Proportion of surgeons who performed cleft lip and/or palate (CL/P) repair, likelihood to operate again, and factors impacting operative decision.
Results
Response rate was 20.5% (121/589) including 113 surgeons treating CL/P across plastic surgery (63.7%), otolaryngology (23.9%), and oral and maxillofacial surgery (12.4%). More completed CL than CP repairs (59.3% vs 21.2%) for patients with example conditions of holoprosencephaly, cardiac abnormalities, trisomy 13, and trisomy 18. Leading CL repair motivations were “parent/caregiver request” (89.6%, 60/67), “appearance” (62.7%, 42/67), and “feeding” (28.4%, 19/67). Leading CP repair motivations were “parent/caregiver request” (66.7%, 16/24), “feeding” (62.5%, 15/24), and “communication” (54.2%, 13/24). Surgeons who had not attempted CL repair described lacking opportunity (34.8%, 16/46) or unfavorable risk–benefit ratios (37.0%, 17/46) as reasons. A greater proportion of those who had not attempted CP repair cited unfavorable risk–benefit ratios (59.6%, 53/89) versus lacking opportunity (21/89, 23.6%). 100% and 95.8% who repaired CL and CP endorsed they would again.
Conclusions
Surgeons more commonly repaired CL than CP in children with life-limiting and terminal illnesses. Nearly all would perform these surgeries again. Respondents who did not repair CP often stated risks outweighed benefits. Studies exploring outcomes of CL/P repair in patients with life limiting and terminal illnesses are scarce. More data are needed to help guide these difficult decisions.
Introduction
The presence of a cleft lip and/or palate (CL/P) is one of the most common congenital differences.1,2 Although the majority of CL/P cases are isolated, approximately 7% to 15% are genetically linked to syndromes and complex diagnoses such as trisomy 13, trisomy 18, and holoprosencephaly.2–5 Long-term prognoses vary both among and within these syndromes.6–10 For patients with severe phenotypes, surgical intervention for CL/P is often overshadowed by life-threatening organ dysfunction, and patients historically do not survive long enough to be considered for CL/P repair.
In patients with such conditions as trisomy 13 and 18, even the decision to perform more critical procedures such as cardiac surgery and tracheostomy can be controversial.11–14 Ethical discussions about whether or not to perform procedures center on challenging topics including the risk of hastening death due to anesthetic complications, unclear benefit given the limited life expectancy, resource allocation to children with more survivable conditions, parental desire to optimize their child's quality of life, and difficulty predicting an individual child's long-term clinical course.11–13,15–18 However, advancements in the management of these syndromes has led to longer life expectancies for select phenotypic subsets.6,7,10–13,15,17 With greater lengths of survival, the decision about whether to perform CL/P repair has become more relevant with several newer studies presenting patients with holoprosencephaly, trisomy 13, and trisomy 18 who survived beyond expectations, eventually undergoing CL/P repair and similar interventions aimed at optimizing quality of life.17,19–21 At the core of arguments both for and against CL/P repair in such patients, surgeons are attempting to maximize patient benefits and to minimize harms while balancing expectations of surrogate decision makers.
While previous studies do exist related to this topic, substantive data to guide the management of these nuanced surgical cases is still rare. The primary objective of this study is to aggregate surgeon perspectives on the management of CL/P in patients with terminal and/or life-limiting illnesses. We hypothesize that cleft lip (CL) and cleft palate (CP) are addressed in a differential manner with a multitude of factors guiding surgeon decision-making. Understanding surgeon perspectives in these situations can help promote ethical treatment decisions.
Methods
Approval of the survey materials and study design was obtained from the Institutional Review Board under IRB #240392 in May 2024 within the authors’ primary institution. The survey instrument included both multiple-choice questions and optional free-text responses. To aid respondents, the survey broadly defined “terminal condition” as a “condition which is not treatable and will likely lead to death” and “life-limiting condition” as a “progressive condition with little prospect of cure, resulting in severe dysfunction or death” with provided diagnosis examples of trisomy 13, trisomy 18, cardiac anomalies, and holoprosencephaly. Subsections of the survey inquired about surgeon demographics, past operative experience with CL/P repair in children who fit said population definitions, reasoning behind operative decisions, surgical timing, and additional consultations. Of note, optional free-text responses were specifically available for the questions asking respondents to list relevant patient diagnoses, to elaborate after any “other” multiple-choice option was selected, to explain “why not” to perform a CL or CP repair, and to offer further general comments if inclined at the end of the form. In turn, for the question regarding diagnoses, surgeons could describe as many diagnoses or as specific of past cases as they wished in the survey, from which answers were later manually categorized by the authors. The survey instrument was prepiloted with 5 American plastic surgeons with various years of experience in practice to hone question design prior to the survey's larger distribution.
Survey responses were collected and managed using REDCap electronic data capture tools hosted at the authors’ institution.22,23 Via REDCap distribution forms, electronic mail invitations to the survey were sent to members of the American Cleft Palate Craniofacial Association (ACPA). Included electronic mail addresses were obtained when publicly available from individuals listed in the ACPA Membership Database who identified with a primary specialty of craniofacial surgery, oral/maxillofacial surgery, otolaryngology, or plastic surgery and who also listed a location in the United States. Contact information and survey responses were anonymized and securely stored in the REDCap database prior to analysis.
The survey was distributed in 30-day intervals over 6 months, with follow-up reminders sent after 15 days to optimize response rates between September 2024 and February 2025. Descriptive data analysis was performed using Microsoft Excel to summarize means and frequencies across variables such as specialty, years of experience, practice setting, operative experience, and various decision-making factors. Free-text responses were extracted further and underwent thematic analysis to identify recurring ethical and clinical justifications for performing or not performing CL/P repairs.
Results
Respondent Demographics
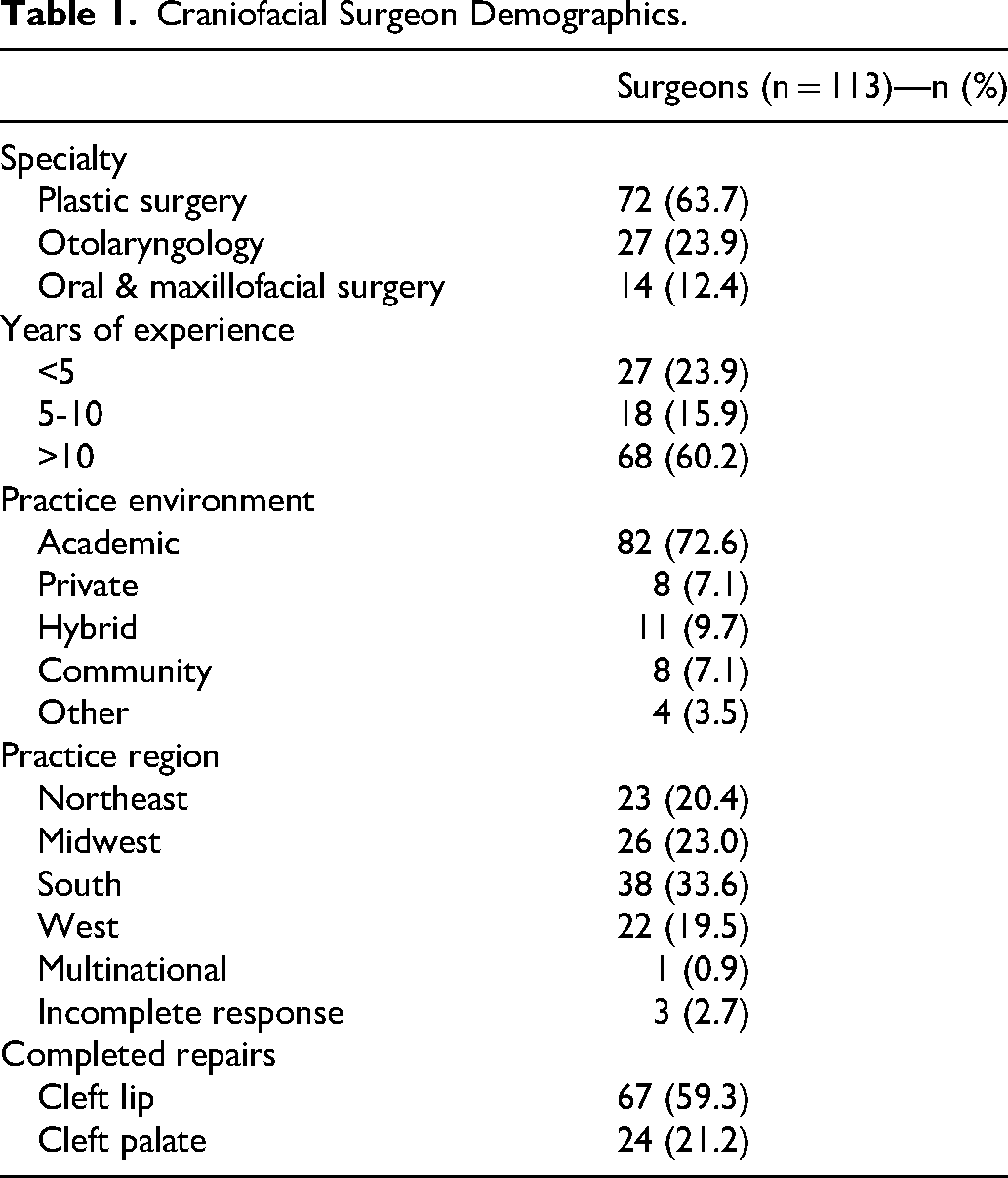
Survey response rate was 20.5% (121/589). Responses included one hundred and thirteen (113/121) surgeons actively treating children with CL/P. Those not actively treating patients with CL/P were excluded from final analysis. Demographic details of the 113 surgeons are presented in Table 1. Respondents were predominantly plastic surgeons (63.7%, 72/113), followed by otolaryngologists (23.9%, 27/113) and oral & maxillofacial surgeons (12.4%, 14/113). Most surgeons (60.2%, 68/113) had been practicing for longer than 10 years and at academic medical centers (72.6%, 82/113). For surgeons who listed their state-specific location within the United States, 19.5% (22/113) practice in the West, 23.0% (26/113) in the Midwest, 20.4% (23/113) in the Northeast, and 33.6% (38/113) in the South. One of the 4 surgeons who did not list a state described their respective practice as “multinational.”
Craniofacial Surgeon Demographics.
Cleft Lip Repair Experience
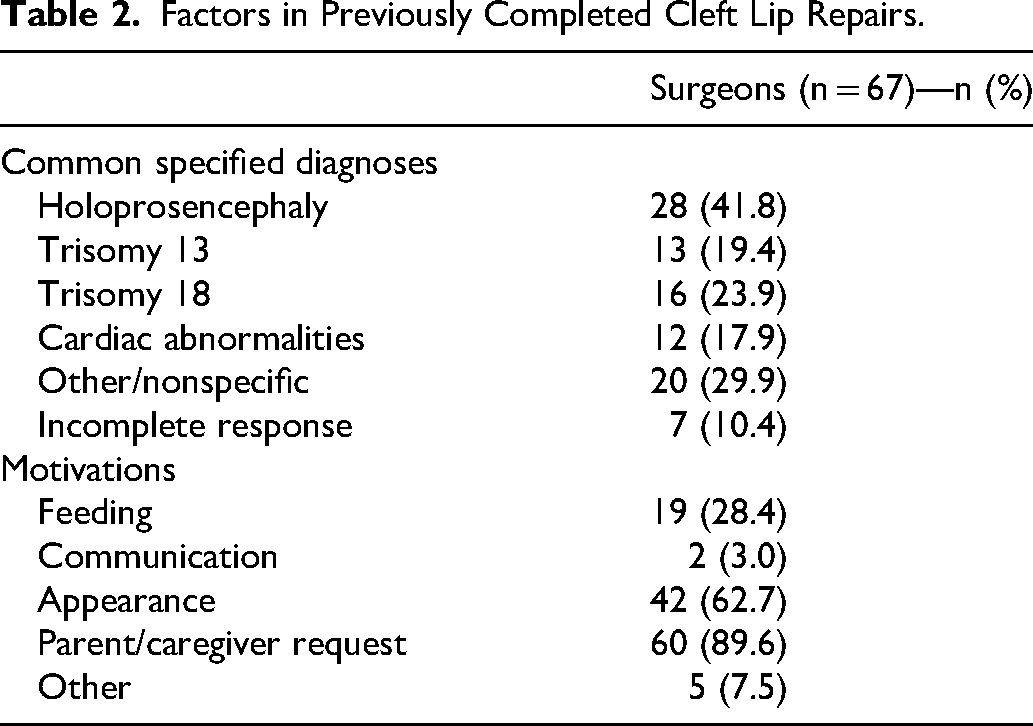
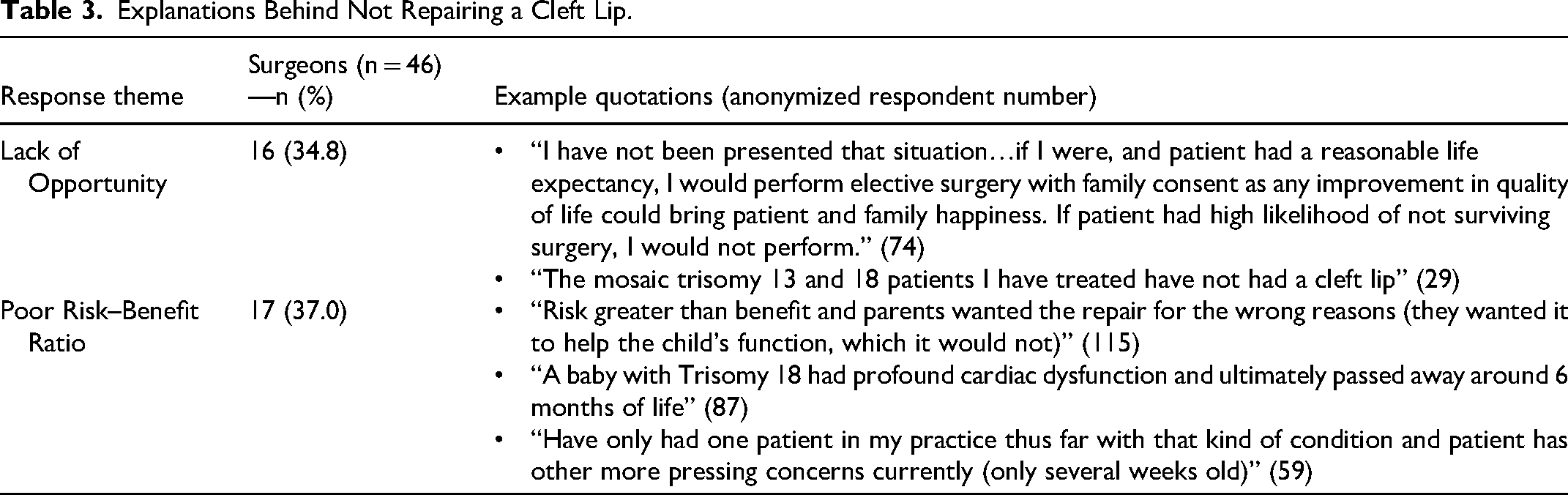
More than half (59.3%, 67/113) of surgeons have repaired a CL in a child with a life-limiting or terminal illness (Table 1). Outlined in Table 2, the most common associated diagnoses were holoprosencephaly (41.8%, 28/67), trisomy 18 (23.9%, 16/67), trisomy 13 (19.4%, 13/67), and cardiac abnormalities (17.9%, 12/67) as calculated by the number of surgeons who listed the specific diagnosis via free-text response. Additional example diagnoses contained within the “other” category included trisomy 21, Smith-Lemli-Opitz syndrome, CHARGE syndrome, Pallister-Killian syndrome, and anencephaly. Popular motivations for CL repair in these patients included “parent/caregiver request” (89.6%, 60/67), “appearance” (62.7%, 42/67), and “feeding” (28.4%, 19/67) (Table 2). All surgeons (100%, 67/67) who had repaired a CL in a child with a life-limiting or terminal illness stated that they would do so again if presented with the same clinical scenario. Of the 40.7% (46/113) of surgeons who had not repaired a CL in this population, 34.8% (16/46) had not been presented with an opportune clinical scenario and 37.0% (17/46) cited a high risk-to-benefit ratio. These data and example free-text responses from these themes are presented in Table 3.
Factors in Previously Completed Cleft Lip Repairs.
Explanations Behind Not Repairing a Cleft Lip.
Within the cohorts who endorsed versus denied performing a CL repair for this patient population, plastic surgeons (74.6%, 50/67 vs 47.8%, 22/46) were more commonly represented than otolaryngologists (20.9%, 14/67 vs 28.3%, 13/46) or oral & maxillofacial surgeons (4.5%, 3/67 vs 23.9%, 11/46) overall and especially so in the CL repair group. A greater proportion of surgeons in the CL repair group also reported practicing greater than 10 years compared to those in the group who had not similarly repaired a CL (65.7%, 44/67 vs 52.2%, 24/46). In contrast, surgeons in practice less than 5 years were more frequently found in the group who had not repaired a CL than in the group who had performed repairs for these patients (37.0%, 17/46 vs 14.9%, 10/67). Regarding practice location, respondents were similarly more likely to be in academic practice compared to other settings both in the group who had repaired a CL and in the group who had not (74.6%, 50/67 vs 69.6%, 32/46).
Cleft Palate Repair Experience
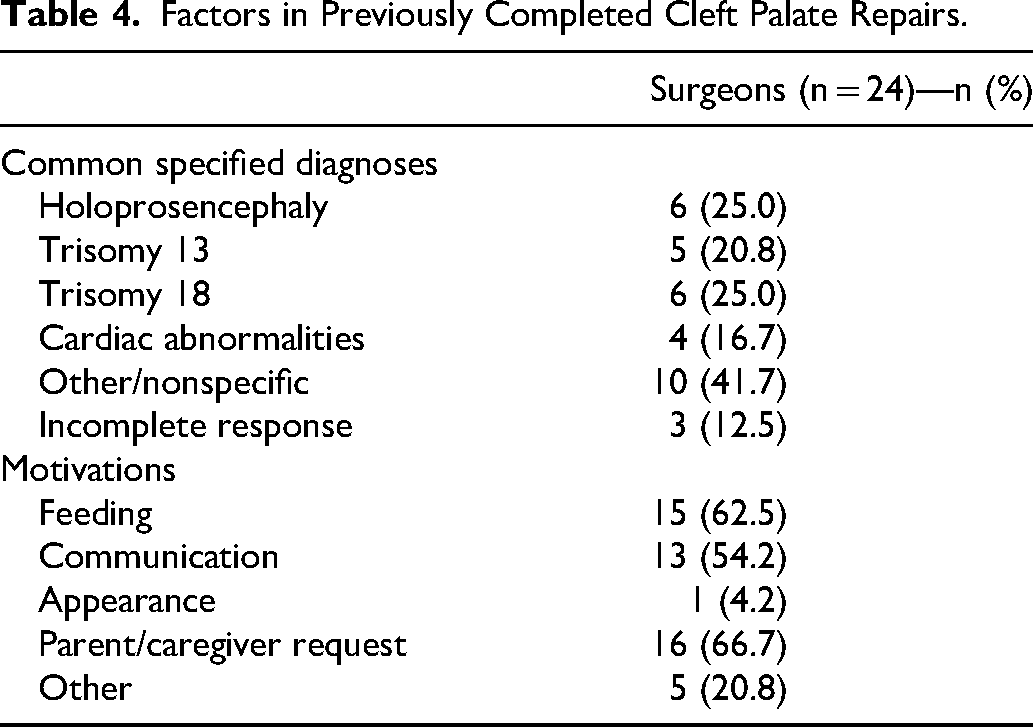
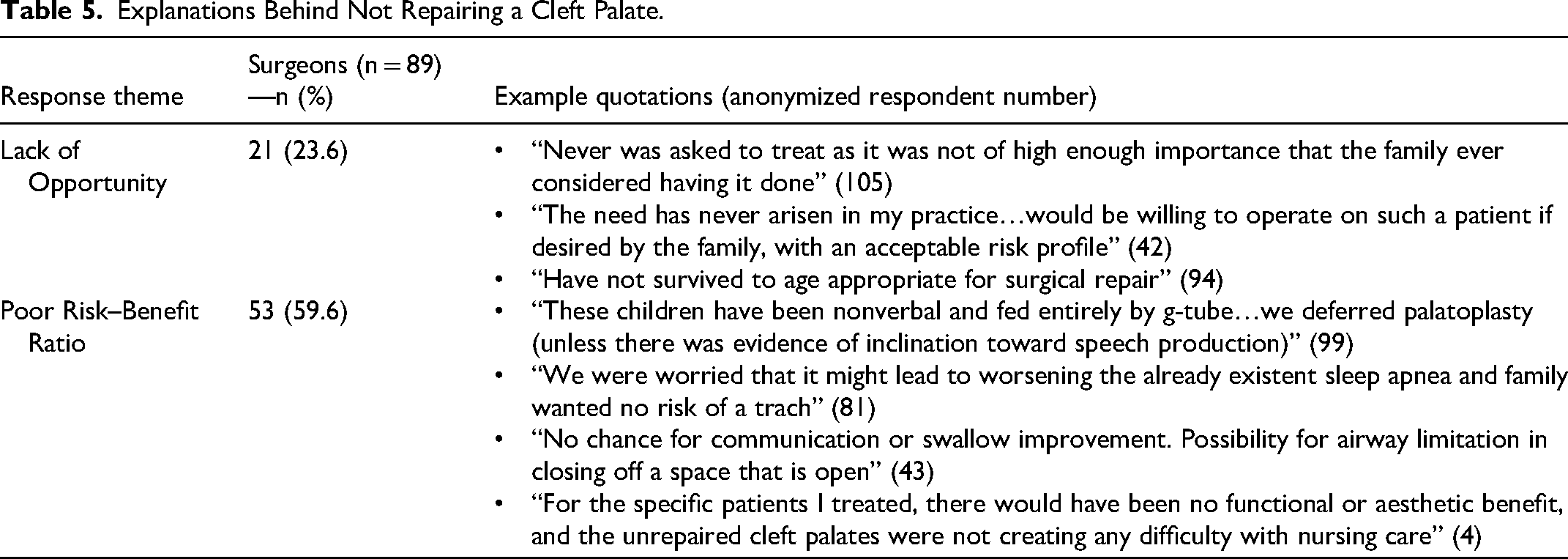
Only 21.2% (24/113) of surgeons had repaired a CP in a child with a life-limiting or terminal illness in the past (Table 1). The most common associated diagnoses were also holoprosencephaly (25%, 6/24), trisomy 18 (25%, 6/24), trisomy 13 (20.8%, 5/24), and cardiac abnormalities (16.7%, 4/24) calculated in the same manner as for CL repairs (Table 4). Example listed diagnoses in the “other” category included trisomy 21, septo-optic dysplasia, Scimitar syndrome, and CHARGE syndrome. Motivations for CP repair in these patients were “parent/caregiver request” (66.7%, 16/24), “feeding” (62.5%, 15/24), and “communication” (54.2%, 13/24). Nearly all surgeons (95.8%, 23/24) who had repaired a CP in a child with life-limiting or terminal illnesses stated that they would do so again if presented with the same clinical scenario, with one surgeon failing to complete said question (Table 4). Of the 78.8% (89/113) of surgeons who had not repaired a CP in this population, most (59.6%, 53/89) cited unfavorable risk-to-benefit ratios related to potential airway decompensation (13.2%, 7/53) as well as minimal speech (39.6%, 21/53) and feeding (28.3%, 15/53) potential. A smaller number of surgeons (23.6%, 21/89) cited a lack of experience or opportunity to make this decision. These data and example free-text responses from the major themes are presented in Table 5.
Factors in Previously Completed Cleft Palate Repairs.
Explanations Behind Not Repairing a Cleft Palate.
As found in CL-related analyses, more surgeons who had and had not repaired a CP in this setting were plastic surgeons (75.0%, 18/24 vs 60.7%, 54/89) than otolaryngologists (25.0% 6/24 vs 23.6%, 21/89) or oral & maxillofacial surgeons (0%, 0/24 vs 15.7%, 14/89). Most of those who endorsed repairing a CP have spent greater than 10 years in practice (66.7%, 16/24), while fewer surgeons with repair experience have practiced less than 5 years (12.5%, 3/24). In the group who had not repaired a CP for such patients, the spread of experience levels was less prominent between those in practice over 10 years (58.4%, 52/89) and less than 5 years (27.0%, 24/89). Academic practice remained the most common practice setting for both surgeons with and without this specific CP repair experience (75.0%, 18/24 vs 71.9%, 64/89).
Impact on Surgical Timing
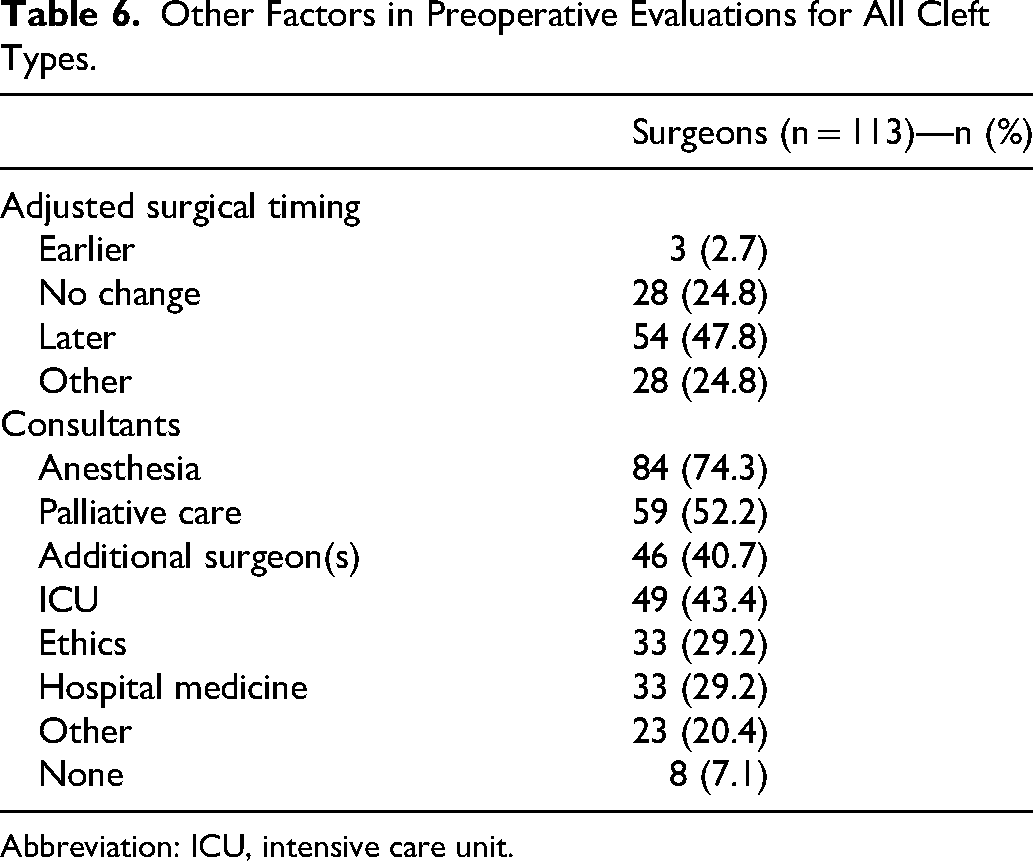
Results related to additional aspects of preoperative planning for all patients including surgical timing are found in Table 6. Approximately half of surgeons (47.8%, 54/113) stated that the presence of a terminal or life-limiting illness would delay their CL/P repair. In contrast, 2.7% (3/113) stated it would hasten time to repair and 24.8% (28/113) stated the diagnosis would not alter their surgical timing. The remaining 24.8% (28/113) responded with free-text answers in the “other” category. Nearly all free-text responses described case-dependent considerations for risks of anesthesia and surgery compared to the potential benefits for the child's function and quality of life (82.1%, 23/28). A smaller fraction also highlighted incorporating specific family goals in decision-making (25.0%, 7/28). Unique quote examples include one respondent describing performing CL repairs “for normalizing of appearance of the infant within the family while alive” and another respondent stating they “would consider earlier [surgical timing] only if parents desired open casket for deceased child and it was for parent wishes.”
Other Factors in Preoperative Evaluations for All Cleft Types.
Abbreviation: ICU, intensive care unit.
Consultations During Patient Evaluation
Nearly all surgeons (92.9%, 105/113) emphasized the importance of consulting other services when faced with the outlined clinical scenario. Consultants included “anesthesia” (74.3%, 84/113), “palliative care” (52.2%, 59/113), “additional surgeon(s)” (40.7%, 46/113), “ICU” (43.4%, 49/113), “ethics” (29.2%, 33/113), and “hospital medicine” (29.2%, 33/113) (Table 6). A subset of surgeons also selected the “other” option with example free-text responses such as “genetics,” “PCP,” “general pediatrics,” “cleft team,” “complex care team,” “cardiology,” and “endocrine.”
Discussion
While the indications for surgical management of CL/P are well defined for otherwise healthy patients, there is a paucity of literature to guide management for those with life-limiting or terminal illness. This study presents the perspectives of 113 cleft surgeons on the management of these medically complex patients. Respondents comprise a diverse group of surgical subspecialists with varying tenures and representing all major regions of the United States. Respondents also operate in a wide variety of practice environments, although an academic setting was documented by the majority (Table 1). The diagnoses most commonly described in both the CL and CP cohorts were holoprosencephaly, trisomy 13, and trisomy 18 (Table 2 and Table 4).
Our study documents that surgeons describe more frequent past experiences with repair of CL than CP in patients with life-limiting or terminal illness, which is consistent with our hypothesis that CL and CP are distinctly treated within this complex population (Table 1). Our results also align with prior evidence that CL repair occurs more often than CP repair in children with trisomy 13 and 18. 19 One plausible explanation for the results is that CL repair is associated with a more minor risk profile than CP repair.24,25 In addition to typically longer anesthetic time, CP repair carries a very real risk of respiratory compromise and oropharyngeal hemorrhage which is compounded by serious medical comorbidities.26,27 As such, CL repair is likely perceived to have a more tolerable risk-to-benefit ratio in comparison to CP repair. Additionally, CL repair is performed earlier in life than CP repair.25,28 Therefore, patients with limited life expectancies may more often be candidates for the earlier procedure versus any later timed operations. Lastly, CL repair instantaneously changes the appearance of a patient, whereas CP repair does not. As such, CL repair may have a significant perceived psychosocial benefit for family and caregivers, even in the postmortem setting. What can encompass pediatric end-of-life care is broad, but multiple studies demonstrate that even for children who die after interventions, the majority of parents do not regret decisions to intervene and do continually seek means of establishing the so-called “normal” parent-child dynamic.17,29
The most frequently listed motivation for both CL and CP repair was parent/caregiver request at 89.6% and 66.7%, respectively. Motivations diverged after this with appearance (62.7%) and feeding (28.4%) subsequently driving CL repairs, while feeding (62.5%) and communication (54.2%) were the next most common drivers for CP repair (Table 2 and Table 4). Nearly all surgeons who performed a CL or CP repair on these patients stated they would do so again if presented with the same scenario. These data affirm that surgeons believe strongly in their decisions to operate. Additionally, parental concerns with the child's appearance is supported by research also indicating that CL repair can play a role in improving parent-child bonding and reducing parental stress levels.30–34 The remaining motivating factors present an ethical conundrum as most patients with holoprosencephaly, trisomy 13, and trisomy 18 will not eat by mouth or develop meaningful speech due to shortened lifespan, developmental delay, and functional instability.4–10 However, recent studies demonstrate some children who survive beyond typical timelines can eventually achieve basic speech and oral intake. One study found that among 64 living children with trisomy 13 or 18 who have survived a year or more, approximately half sometimes used supplemental oxygen and slightly over half had a gastrostomy, including for only intermittent use. Their parents also endorsed 24% to 45% could say “mama” or “papa,” 75% to 87% ate by mouth, and 10% to 39% ate alone with percentages varying by the child's age group. 17 This highlights the nuanced decision that must take place with every patient case and uncertainty in prognostication worth acknowledging for providers and caregivers alike.
In addition to patient factors, surgeon factors may also contribute to the decisions to operate. Respondents in the CL and CP repair groups were more likely to be advanced in their careers than early in practice, while early career surgeons were more likely to be in the groups lacking similar CL or CP repair experience. A combination of factors may contribute to this finding, including that operating for more years intrinsically offers greater case volume among which to encounter rarer diagnoses. More extensive surgical experience may also offer greater confidence in one's operative skills or familiarity with complex ethical dilemmas to be willing to attempt such cases. The prevalence of responses from plastic surgeons in our study compared to otolaryngologists and oral & maxillofacial surgeons is consistent with prior data showing different specialty involvement in caring for children with CL/P, including that plastic surgeons have been responsible historically for the majority of primary CL/P repairs.19,35–39 It is of note that our results by nature of the survey design cannot be interpreted to conclude one specialty is more likely to accept or deny operating in these cases than another. Furthermore, the ACPA and other experts commonly advocate for a multidisciplinary approach to deliver optimal CL/P care which may include multiple surgical specialties at various treatment stages if available and in conjunction with other nonsurgical providers.35,36,40
Among all respondents, most (47.8%) indicated that they would delay their CL/P repair, while smaller fractions stated they would operate earlier (2.7%) or with no change from timing in healthier patients (24.8%) (Table 6). It points to an important area of discussion as some surgeons believe that there is merit in addressing the appearance or functions of the child as early as possible or on a typical schedule to maximize their remaining quality of life. Others, including the majority of surgeons in this study, are more likely to delay any repairs for children with the described medical diagnoses. These conditions complicate the perioperative risk profile, and many surgeons believe delay allows time for growth as well as cardiopulmonary optimization. Beyond clinical variables, family desires are also an important consideration for surgical timing, both in accelerating or delaying repairs, in accordance with previous research. 34
Given the intricacies of the associated diagnoses and the operative procedures themselves, it is not unexpected that almost all surgeons consulted with at least one other clinical team for assistance in clinical decision-making (Table 6). These results align with prior studies of pediatric surgical patients admitted for terminal conditions, including a trend toward greater inclusion of palliative services.41,42 While pediatric palliative care is shown to offer multiple benefits to parent and patient experiences during severe illness, is it is often an underused or incompletely understood resource.29,41–49 When employed appropriately, palliative care may help bridge key gaps in understanding between what is technically possible through medical intervention and what aligns with the caregivers’ specific goals for the patient. Lack of a palliative care consult in pediatric surgery patients has association with greater odds of the patient's death both in the operative room or during attempted resuscitation, implying palliative care may be able to assist surgeons in selecting more goal appropriate care for higher risk children. 41 Ethics consults can serve a similar role to guide “big picture” conversations, but interestingly, ethics teams were less often consulted by respondents of our survey. This may be due to lack of access to or awareness of such services.
This study is subject to limitations inherent to retrospective survey-based research, including response and recall biases. Additionally, the response rate of 20.5% is less than ideal but is similar to some previous surveys of ACPA members. 39 However, given the rarity of similar studies in the published literature and the rarity of the life-limiting diagnoses discussed, we believe even small amounts of additional data can contribute valuable information. Only ACPA member's perspectives were captured in this study, limiting generalizability as many cleft surgeons who are not ACPA members are likely faced with the same challenging clinical scenarios yet are unfortunately not encompassed in the data presented. Future studies may benefit from including surgeon populations beyond ACPA members and in practice outside of the United States to improve response diversity. Completing additional investigations that include perspectives from the caregivers of this patient population may also provide richer, more holistic data to navigate surgical decisions in future cases. Lastly, it is difficult to capture the nuanced and diverse approaches to these patients in a multiple-choice or Likert-style instrument, even with inclusion of optional free-text responses. The design may, therefore, result in oversimplification of the collected surgeon experiences. Further studies should seek to identify the risk profiles of CL/P repair at different time points in patients with life-limiting and terminal illnesses.
Conclusion
The decision to perform CL/P repair in children with limited life expectancy and terminal illnesses is a multifaceted ethical and clinical dilemma. Data are scarce related to the practice patterns and safety of these procedures for such subsets of patients. This study suggests that surgeons have more frequent experience performing CL repairs than CP repairs for the aforementioned patient population, likely due to the risks inherent to CP repair combined with the lower perceived benefits. Parent and caregiver input remains an important driver in clinical decision-making, and surgeons firmly believe in their past decisions to operate. These results also present new insights into the complex ethical and clinical discussions surrounding the care of these patients. Future studies should look to better characterize the perioperative risk profiles of patients and the caregiver perspectives which contribute to choosing CL/P repair in children with terminal and life-limiting illnesses. More detailed investigations may not only serve to educate cleft surgeons generally but they may also provide basis for new clinical tools to guide both clinicians and caregivers navigating the treatment options.
Footnotes
Authors’ Note
Additional Notes: Preliminary data included in this study was previously presented as an oral presentation at the American Cleft Palate Craniofacial Association Annual Meeting in Palm Springs, CA held May 6-10, 2025. Author Lauren E. Sullivan, MD, conducted the original research at Vanderbilt University School of Medicine, but said author is now affiliated with the Department of Plastic Surgery at the University of Kansas Medical Center, Kansas City, KS.
ORCID iDs
Ethical Considerations
The Institutional Review Board of Vanderbilt University approved this survey study featuring participant anonymization and secure data storage in the REDCap database under IRB #240392 (approved 5/15/2024).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data are available upon request of the corresponding author and is presently stored securely in a REDCap database.