
Abstract
Craniofacial microsomia (CFM) presents with variable underdevelopment of craniofacial structures. The clinical severity varies widely and may lead to airway compromise and feeding difficulties in neonates. Herein, we describe a rare case of unilateral CFM with a severe Tessier number 7 cleft, complete mandibular agenesis, ear deformities, and extensive intraoral adhesions. Particularly, adhesions between the tongue and oral mucosa induced a deficiency of reconstructable soft tissue, making the release of the adhesion challenging and complicating the timing of surgical intervention. The patient required tracheostomy for respiratory distress and was fed via a nasogastric tube due to severe Tessier number 7 cleft, which caused significant difficulty with oral feeding. Considering the need for oral feeding and the anatomical challenges, surgical intervention was performed on day 70. The procedure involved removal of intraoral adhesions, separation of the oral cavity from the external face to restore functional integrity, and reconstruction of the oral commissure. This allowed initiation of oral feeding and facilitated aesthetic improvement without complications. This case illustrates a severe form of CFM and highlights the importance of timely, growth-adapted interventions to restore essential functions.
Introduction
Craniofacial microsomia (CFM) is a congenital anomaly involving underdevelopment or absence of facial structures derived from the first and second pharyngeal arches. 1 With an incidence ranging from 1 in 3000 to 1 in 5000 live births, it is recognized as the second most prevalent congenital facial anomaly after cleft lip and palate. 2 Although its pathogenesis remains incompletely understood, the proposed mechanisms include vascular disruption, abnormal migration of cranial neural crest cells, and damage to the Meckel's cartilage. 3
CFM presents with a wide range of craniofacial findings, most often involving hypoplasia of the mandible, ear, and orbit. 4 Mandibular anomalies have long been recognized as a hallmark of CFM, with severities ranging from mild hypoplasia to complete agenesis. Auricular malformations frequently accompany mandibular defects, ranging from preauricular skin tags to complete aural atresia. 5 Additional findings include facial nerve palsy, 6 soft tissue hypoplasia, and extracraniofacial anomalies involving the spine, heart, and kidneys. 7
Beyond the well-documented anomalies, several distinct clinical features have also been investigated. In a retrospective review of 198 patients with hemifacial microsomia, 23% were found to have concomitant lateral cleft, also known as Tessier number 7 cleft, which significantly correlated with orbital and mandibular deformities. 8 Furthermore, Chen et al. reported that tongue dysmorphologies were identified in 4.8% of patients with CFM. 9 However, despite the range of features reported, no cases to date have described the coexistence of multiple severe anomalies in a single patient. Notably, these include extensive intraoral adhesions—features not previously documented in the context of CFM.
We report a rare case of CFM characterized by mandibular agenesis and a severe lateral facial cleft, along with extensive intraoral adhesions and agenesis of the ossicles and external auditory canal (EAC). This case exemplifies a severe manifestation of CFM, in which a Tessier number 7 cleft coexists with extensive skeletal and soft tissue anomalies, highlighting the phenotypic breadth of the disorder and underscoring the importance of individualized surgical planning.
Case Report
A male infant was born at 37 weeks and 5 days of gestation via cesarean section, weighing 3190 g and measuring 51 cm in length. Prenatal ultrasonography and fetal magnetic resonance imaging suggested micrognathia, but the lateral facial cleft was not clearly detected. The neonate exhibited poor initial crying and activity, requiring positive-pressure ventilation followed by endotracheal intubation. No known family history of congenital anomalies or other relevant medical conditions was present. A postnatal physical examination revealed a left-sided lateral facial cleft and mandibular hypoplasia. The patient was subsequently referred to the Department of Plastic and Reconstructive Surgery for further evaluation.
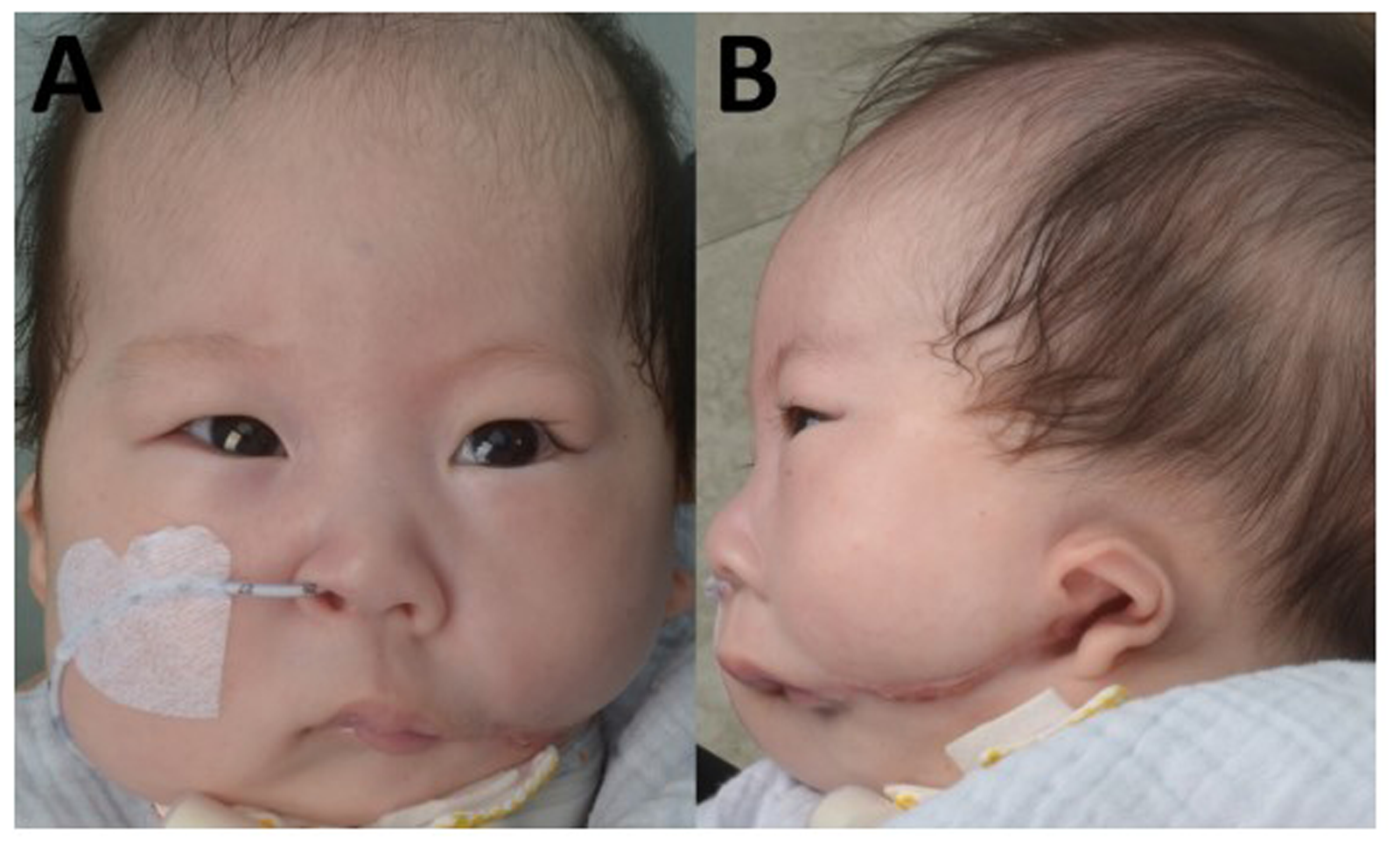
Upon initial evaluation, the patient exhibited features consistent with unilateral CFM, accompanied by a lateral facial cleft extending to the preauricular region (Figure 1A). Multiple intraoral adhesions were observed primarily involving the palate, tongue, and buccal mucosa. The left side of the palate was fused to the upper buccal mucosa, resulting in obliteration of the gingivobuccal sulcus, and the right side was adhered to the tongue and upper buccal mucosa. In addition, the left side of the tongue was severely adherent to the adjacent lower buccal mucosa (Figure 1B). Moreover, a soft-tissue mass protruding from the lateral aspect of the lower lip was observed.
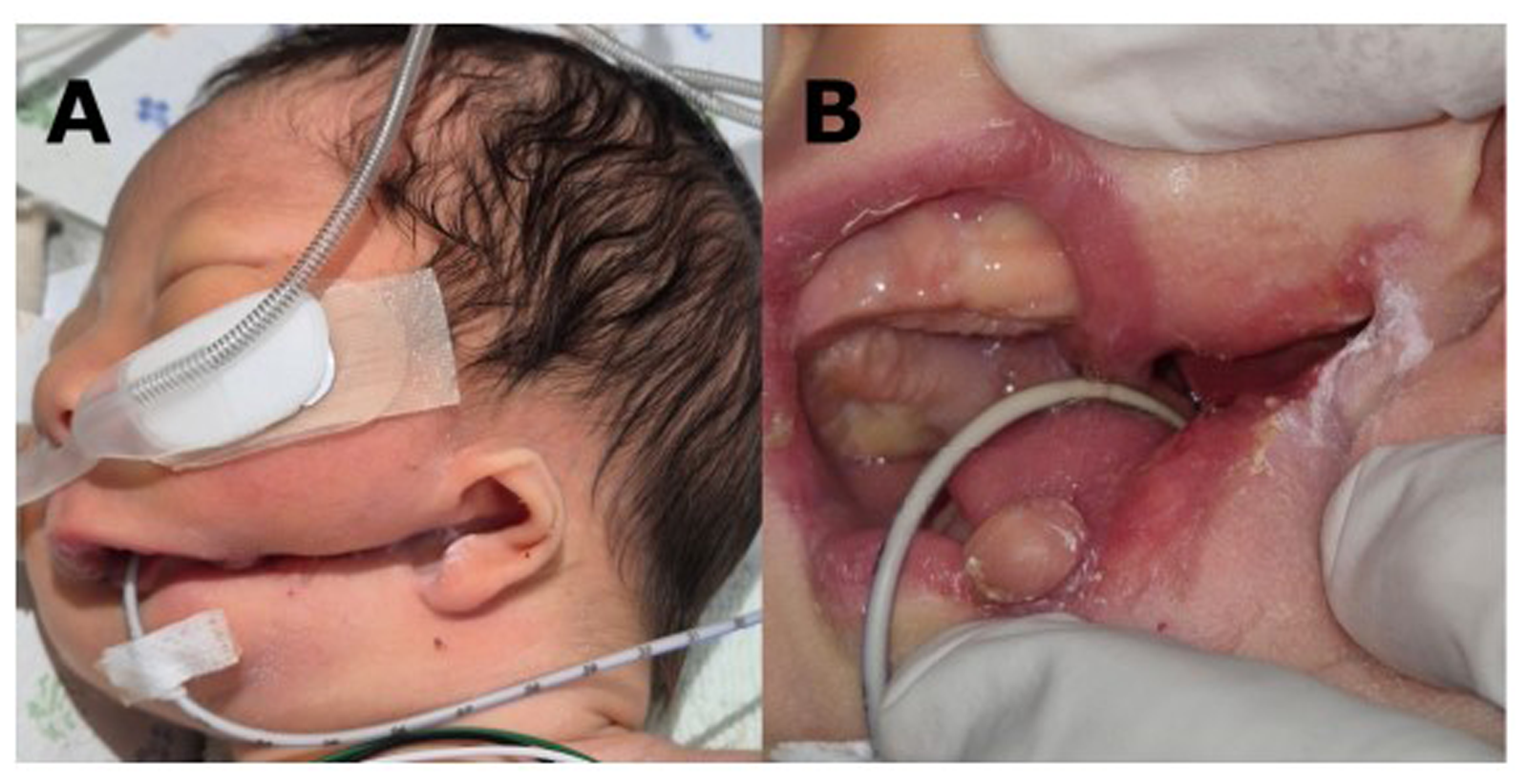
Photograph Taken on Initial Evaluation. (A) Left-sided Craniofacial Microsomia is Noted, With a Lateral Facial Cleft Extending Toward the Preauricular Region. (B) Multiple Intraoral Adhesions are Observed, Along With a Soft Tissue Mass Protruding From the Lateral Aspect of the Lower Lip.
Three-dimensional facial computed tomography (CT) revealed agenesis of the left mandibular body, ramus, and condyle, with only minimal remnants, and the absence of the tympanic segment of the left temporal bone (Figure 2). The zygomaticomaxillary complex exhibited mild hypoplasia, with a reduced orbital size on the cleft side. The left EAC and ossicles were absent, consistent with complete aural atresia, whereas the inner ear structures remained intact (Figure 3).
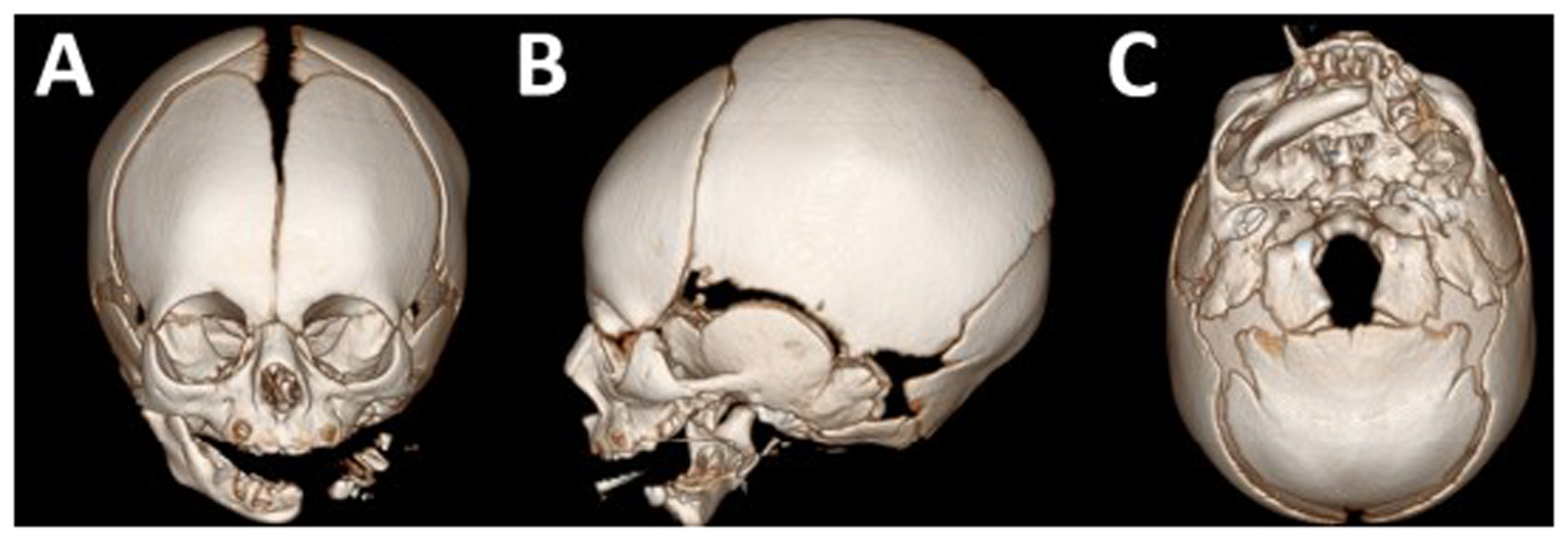
3D Facial Computed Tomography Scan Showing Mandibular Agenesis Leaving Small Remnant of Mandible as Well as the Absence of the Tympanic Segment of the Left Temporal Bone and Hypolplasia of Zygomaticomaxillary Complex. (A) Anteroposterior View. (B) Left Lateral View. (C) Submental View.
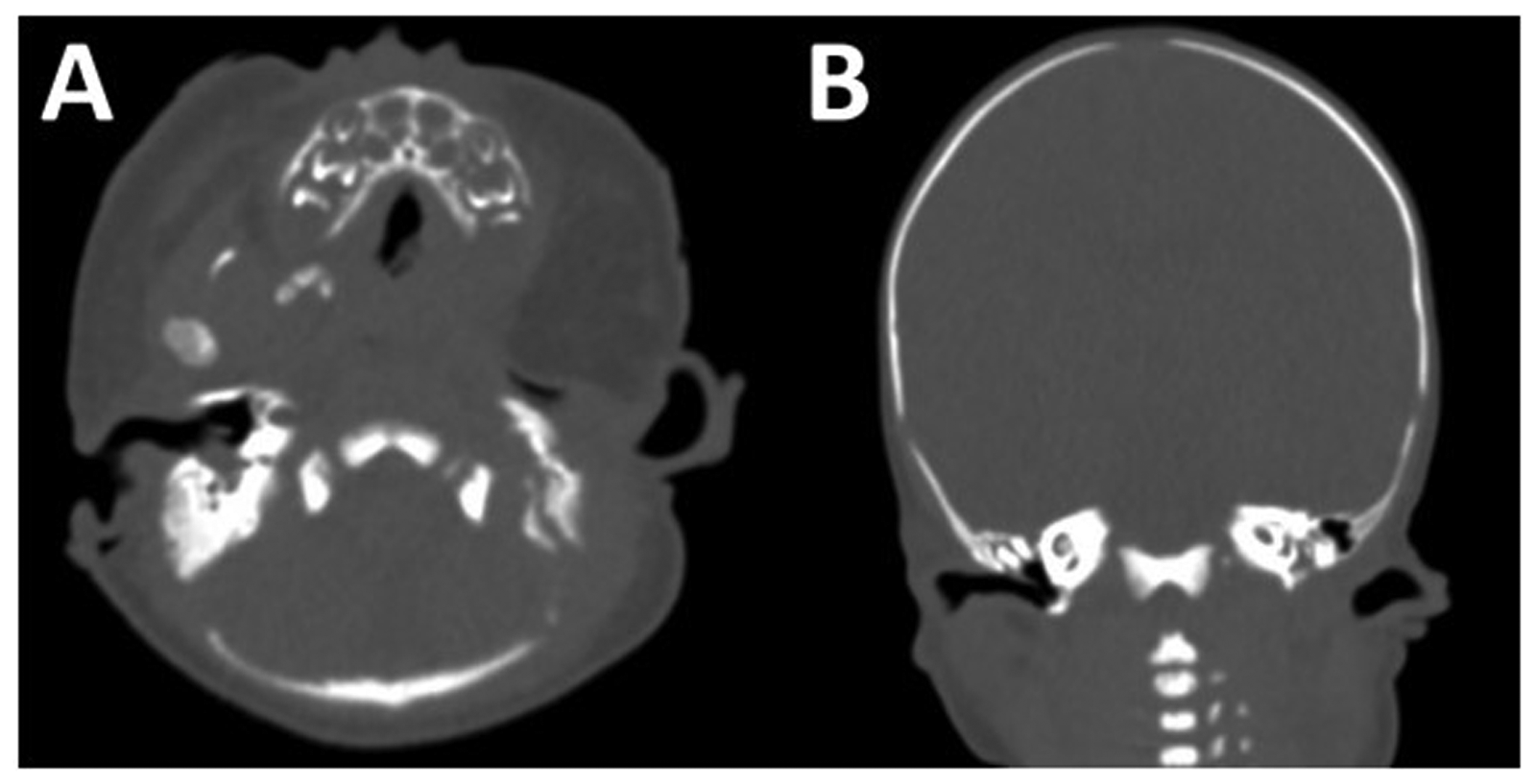
Facial Computed Tomography Scan Showing Complete Aural Atresia With Absence of the External Auditory Canal and Ossicles, While the Inner Ear Structures Remained Intact. (A) Axial View. (B) Coronal View.
Clinical evaluation revealed partial peripheral facial weakness on the cleft side, as evidenced by incomplete eye closure on the left side during crying and sleep. Additionally, the nasolabial folds and forehead creases on the cleft side were less prominent than those on the non-cleft side. Newborn hearing screening demonstrated normal function in the right ear, whereas responses in the left ear were minimal to absent, warranting further audiologic evaluation.
Brain CT revealed no intracranial abnormalities, and spinal radiography showed no vertebral anomalies. Karyotyping did not reveal any chromosomal abnormalities. The extremities were unremarkable, and no other syndromic features were observed.
Normal oral feeding was not feasible because of the lateral facial cleft. Nasogastric tube feeding was initiated and the patient maintained normal growth. Although extubation and a trial of room air were attempted, feeding-related respiratory distress led to reintubation on day 14, and subsequent tracheostomy on day 55.
Surgical Procedure
Surgical intervention was performed on day 70, considering the need for oral feeding and degree of growth. The preoperative appearance is shown in Figure 4A. As noted in the initial evaluation, the adhesions were severe and a tooth was embedded in the mandibular remnant (Figure 4B). The protruding mandibular remnant and the associated tooth on the left lower lip were excised. Subsequently, the fused area between the left side of the soft palate and upper buccal mucosa was released, and the gingivobuccal sulcus was reconstructed using techniques such as Z-plasty (Figure 4C). On the noncleft side, adhesions involving the palate, upper buccal mucosa, and tongue were present (Figure 4D), which were released as extensively as possible and the intraoral space was maximized (Figure 4E).
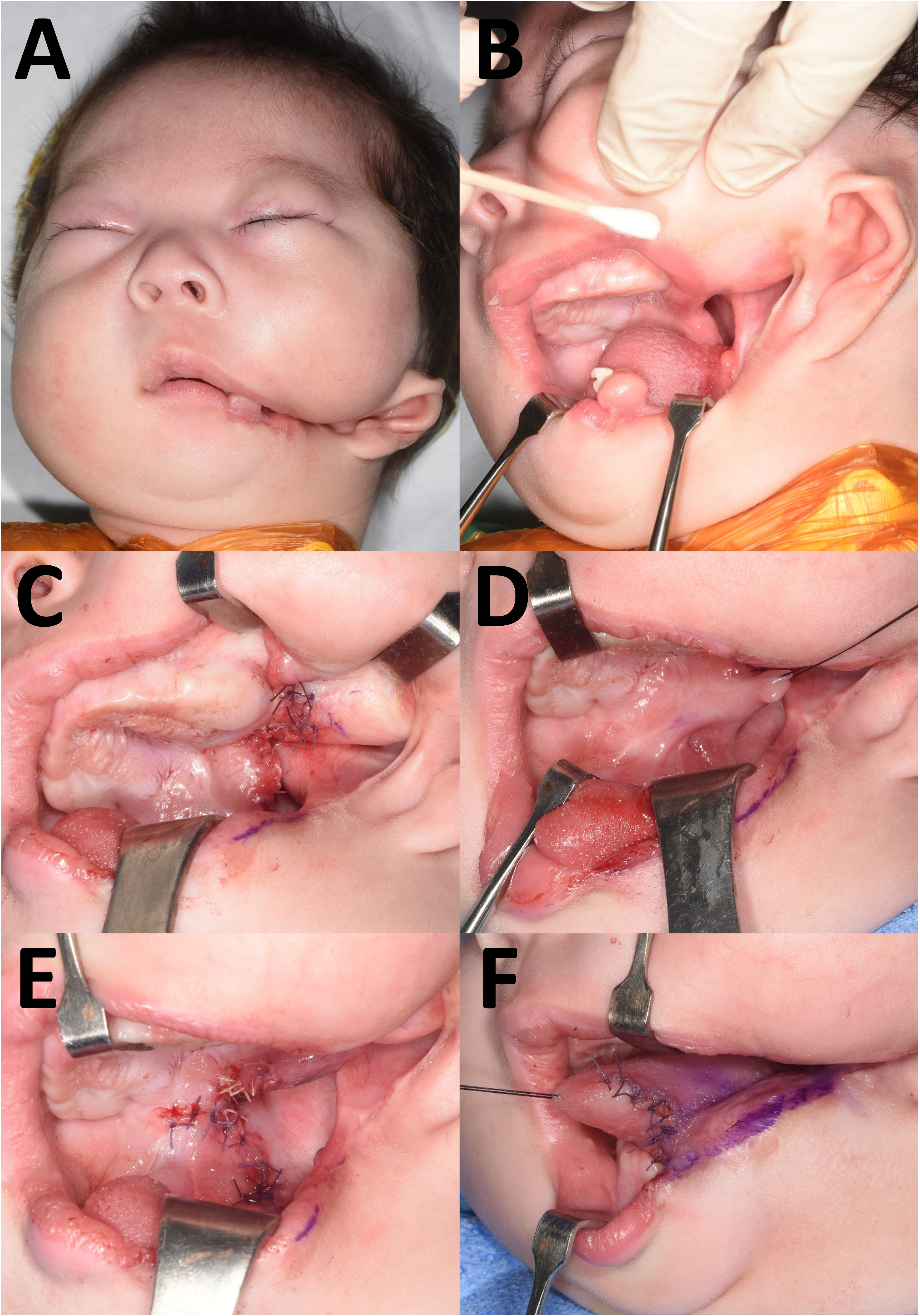
Intraoperative Findings and Surgical Procedures on Day 70. (A) Preoperative Photograph. (B) Mandibular Remnant With an Embedded Tooth on the Left Lower Lip. (C) Release of the Left Soft Palate–Buccal Mucosa Adhesion and Sulcus Reconstruction With Z-plasty on the Cleft Side. (D) Adhesions Involving the Right Palate, Buccal Mucosa, and Tongue on the Noncleft Side. (E) Extensive Release and Z-plasty Performed. (F) Partial Release of Tongue Adhesion on the Cleft Side, Limited Due to the Risk of Mucosal Necrosis.
On the cleft side, extensive adhesion between the tongue and lower buccal mucosa, along with a wide lateral cleft, posed significant challenges for achieving adequate mucosal coverage after release. Given the limited availability of soft tissue, simultaneous complete release of the tongue adhesion and reconstruction of the lateral cleft was anticipated to result in mucosal necrosis. Therefore, only the anterior portion of the tongue adhesion was partially released, and the tongue contour was reconstructed accordingly (Figure 4F).
The left oral commissure was marked for symmetry using the position of the right oral commissure as a reference. An incision was made along the mucocutaneous junction of the lateral cleft. After separately dissecting the mucosa and skin and identifying the orbicularis oris muscle, very few muscles remained in the lower lip. The mucosa was trimmed and sutured to establish an internal lining, and the muscle was approximated end-to-end to the extent possible. The deep tissues were sutured after wide dissection of the mucosa and skin, and the left oral commissure was reconstructed with reference to the contralateral commissure. The skin was closed in a straight-line fashion, and Z-plasty was placed at the nasolabial fold.
After surgery, the oral cavity and external face were successfully separated, allowing the patient to initiate normal oral feeding. The feeding volume gradually increased and eventually approached almost normal levels. At the 3-month follow-up, the patient showed a markedly improved facial appearance compared with the preoperative state (Figure 5).
Postoperative Photograph Taken at 3 Months After Surgery, Demonstrating Separation of the Oral Cavity From the External Face as Well as Significant Improvement in Facial Appearance. (A) Frontal View (B) Lateral View.
Additional surgery is planned for the following year to release the residual adhesion between the tongue and lower buccal mucosa, accompanied by scar revision on the left cheek. Subsequent procedures, including mandibular and auricular reconstruction, will be considered in accordance with the patient's facial growth and development.
Discussion
CFM is a clinical term for a condition encompassing a wide range of craniofacial anomalies with syndromic features. Heterogeneous clinical presentations frequently complicate the establishment of a definitive diagnosis. Cousley and Calvert proposed diagnostic criteria based on the presence of ipsilateral mandibular and ear defects, or asymmetry involving the mandible or ear. 10 Treacher Collins syndrome and severe orbitofacial clefts may be mistaken for bilateral CFM because of overlapping features. 11 Goldenhar syndrome, traditionally distinguished from CFM, presents with similar phenotypes, including epibulbar dermoid and vertebral anomalies. While recent perspectives suggest that Goldenhar syndrome should no longer be considered a distinct entity given its shared clinical and developmental spectrum, 12 it remains crucial to assess for the presence of additional anomalies.
The patient had an extensive lateral facial cleft accompanied by multiple anomalies, most notably mandibular agenesis, in the absence of findings indicative of a syndromic condition. The lateral cleft extended to the preauricular region, and agenesis of several skeletal components of the lower face was observed. The EAC was completely absent. Instead, the lateral facial cleft extended abnormally toward the temporomandibular joint (TMJ), resulting in a cavity resembling a blind-ending pouch. In addition, this case was unique in that it exhibited extensive intraoral adhesions. Considering the constellation of findings, the patient was defined as having unilateral CFM with a severe Tessier number 7 cleft phenotype.
The Orbit, Mandible, Ear, Nerve, Soft tissue (OMENS) classification system provides a standardized framework to describe the severity and extent of craniofacial anomalies in patients with CFM.13,14 According to the OMENS classification, the patients were categorized as O1, M3, E2, N1, and S2, indicating mild orbital hypoplasia, absence of the mandibular ramus and TMJ, microtia with aural atresia, upper facial nerve injury, and moderate soft tissue deficiency, respectively. This classification reflects the severity of mandibular and auricular deficiencies, as well as the complexity of the associated soft tissue anomalies, all of which significantly influence surgical planning.
Tracheostomy is often required in neonates with respiratory distress, particularly when extubation is infeasible. Although the need for tracheostomy has decreased in recent years with the introduction of mandibular distraction osteogenesis, it remains necessary for patients with severe mandibular deformities. Feeding difficulties occur in up to 83% of the patients with CFM, highlighting the importance of timely airway and nutritional management during early infancy. 15 The most widely accepted consensus for determining the timing of surgery is to separate the oral cavity and external face as early as possible in order to initiate oral feeding. 16 The goals of surgery are to restore function, create an oral commissure on the cleft side as symmetrically as possible, and achieve aesthetically satisfactory outcome. 17
In the present case, the patient developed respiratory distress shortly after birth, necessitating intubation. Although extubation was attempted several days later, feeding-related respiratory distress necessitated reintubation, ultimately leading to tracheostomy. Because of the extensive adhesions between the tongue and lower buccal mucosa, it was anticipated that allowing time for growth would increase the amount of reconstructable soft tissue and potentially reduce the number of surgical interventions. Moreover, aggressive surgical approaches at an early stage may cause mucosal necrosis.
After consultation with the pediatric team, surgery was performed on day 70. During the procedure, adhesions were released, and the affected structures were reconstructed to restore anatomy as closely as possible to the normal configuration. However, as anticipated, complete separation of the tongue from the buccal mucosa was not achieved because of the limited availability of soft tissue. Although Z-plasty is typically performed on both the mucosal and cutaneous sides when correcting lateral facial clefts, it was not feasible on the mucosal side in this case. Nevertheless, the oral commissure was reconstructed to achieve symmetry and the oral cavity and external face were effectively separated to facilitate normal oral feeding.
This case highlights the complexity of managing severe craniofacial clefts involving skeletal and soft-tissue deficiencies. This emphasizes the value of a growth-oriented, individualized approach and demonstrates that functional and aesthetic improvements can be achieved through carefully timed, staged interventions, even in the presence of profound anatomical limitations.
Conclusion
This report presents a rare case of unilateral CFM with severe lateral facial cleft and multiple structural anomalies. Early surgical intervention enabled oral feeding and facilitated functional recovery, while future staged procedures are planned to address residual tongue adhesions. Long-term follow-up is warranted to monitor facial growth and nerve function, and further reconstruction may be required as the patient matures.
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board of Pusan National University Hospital (IRB No. 2508-007-154). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent to Participate
The patients provided written informed consent for participation in this study.
Consent for Publication
The patients provided written informed consent for publication and use of the images.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
No datasets were generated or analyzed during the current study.