
Abstract
Objective
To compare speech outcomes in 4 groups of 5-year-olds with cleft of the hard and soft palate: with Robin sequence without additional conditions (RS−), with Robin sequence with additional conditions (RS+), without Robin sequence with additional conditions (CP+), and without Robin sequence without additional conditions (CP−).
Design
Registry-based cohort study.
Setting
Regional public care university hospitals in Sweden.
Participants
A total of 433 children with cleft of the hard and soft palate: 72 with RS−, 28 with RS+, 61 with CP+, and 272 with CP−.
Interventions
Primary cleft palate repair in 1 or 2 stages.
Main outcome measures
Dichotomized outcomes of percentage of consonants correct, percentage of nonoral speech errors, and velopharyngeal competence. Logistic regression was used for statistical analysis.
Results
Children with RS+ had significantly lower odds of age-appropriate consonant production (OR 0.17, 95% CI 0.08-0.40), no nonoral speech errors (OR 0.17, 95% CI 0.07-0.39), and velopharyngeal competence (OR 0.24, 95% CI 0.10-0.56) than those with CP−. Significantly lower odds of age-appropriate consonant production were found for children with RS− (OR 0.50, 95% CI 0.29-0.88) and CP+ (OR 0.45, 95% CI 0.24-0.84) than children with CP−.
Conclusions
Both Robin sequence and additional conditions were associated with decreased odds of age-appropriate consonant production at 5 years of age. For children with RS+, the odds were further reduced, and they also had decreased odds of no nonoral speech errors and of velopharyngeal competence. The results can form the basis for informing parents and planning intervention.
Introduction
Cleft palate may affect several structures and functions to varying degrees, such as eating, ear function, hearing, speech, facial growth, teeth, and occlusion, depending on the extent of the cleft. The cleft is surgically closed to provide the best possible conditions for normal development. 1 Although additional conditions, such as syndromes, other malformations, and intellectual disabilities, may affect speech and language development, 2 children with cleft palate and additional conditions are often excluded from larger studies. 3
Robin sequence is an additional condition that sometimes occurs together with a cleft of the palate. It includes micrognathia resulting in glossoptosis and upper airway obstruction. 4 An often wide, U-shaped cleft palate has been reported in over 70% of cases of Robin sequence.5,6 A larger cleft width and upper airway obstruction can result in challenging palatal surgery for children with Robin sequence, which may lead to delayed surgery.7,8 Delayed closure of the palate, in turn, may hamper speech development. 9 Thus, it is important to increase knowledge about speech outcomes in this group of children.
Prevalence of Cleft Palate and Additional Conditions
The estimated global prevalence of cleft lip and/or palate is 1.7 per 1000 live births, but varies geographically and in different ethnic groups. 10 In Sweden, between 2000 and 2020, the birth prevalence of cleft lip and/or palate was 1.5 per 1000 births and of cleft palate without cleft lip, 0.6 per 1000 births. 11 The prevalence of additional conditions in children with cleft palate without cleft lip has varied in European studies, between 34% and 52%.12–14 The reported global prevalence of Robin sequence was 9.5 per 100,000 live births in a systematic review and meta-analysis. 4 Robin sequence is pathogenically heterogeneous and may also occur together with other additional conditions. 15 For example, in a study by Karempelis et al., 65 out of 234 patients with cleft palate and Robin sequence also had a diagnosed syndrome. 15 Among these patients, 29 syndromes were identified, with Stickler's syndrome being the most common. Other syndromes were less frequent and occurred in only 1 to 3 individuals. 15 It should be taken into account that the reported prevalence of additional conditions in children with cleft palate is affected by different methodologies and the availability of resources and techniques used to assess genetic and medical conditions, both globally and over time. 16
Speech in Children With Cleft Palate
There is a lack of agreement about which methods of palatal surgery produce the best speech results in children born with cleft palate. 1 Methods vary in surgical technique, 1 timing, 3 and whether the palate is closed in 1 or 2 stages. 17 Despite complete closure of the palate, incompetent velopharyngeal function may persist postoperatively, resulting in speech symptoms, such as hypernasality, nasal emissions, velopharyngeal friction sounds, and weak and nasalized consonants. 3 In some cases, incompetent velopharyngeal function leads to compensatory changes of articulatory place and/or manner for certain consonants. 18 In the large randomized controlled trial Timing of Primary Surgery for Cleft Palate (TOPS), including 461 children with nonsyndromic cleft palate without cleft lip from Europe and South America, speech was compared after palatal surgery at 6 and 12 months of age. 3 Twelve percent of all children in the TOPS trial, regardless of timing of palatal surgery, were reported to have incompetent velopharyngeal function at 5 years of age. However, some of them had been treated with secondary surgery to improve speech. 3 Regarding methodology for cleft palate speech assessment, it has been recommended that several blinded listeners trained in cleft palate speech assessment should be used, and that intra- and interrater reliability of speech assessments should be reported to enable interpretation of the validity of speech results.19,20 Without reports on reliability, it is difficult to determine the validity of the results. Speech assessment should be based on audio or audio-video recordings with standardized speech material.19,20
Speech in Children With Robin Sequence
Children with Robin sequence are sometimes included21,22 and sometimes excluded 3 from studies on cleft palate speech. In 2015, Wan et al. 23 stated that there was a lack of high-quality and long-term outcomes for this patient group. One reason for excluding participants with Robin sequence could be that the aim is to have groups of participants that are homogeneous.
A review of 19 articles by Sullivan et al. 8 reported the occurrence of incompetent velopharyngeal function and secondary speech surgery after cleft palate repair in children with nonsyndromic Robin sequence. Furthermore, 5 out of 8 studies comparing the occurrence of incompetent velopharyngeal function between children with cleft palate with and without Robin sequence reported no significant differences between groups. However, several studies used 1 rater only, reports on the reliability of speech assessments were uncommon, and not all studies described the methods used for speech assessment. This makes it difficult to determine the validity of the results. According to the review, 8 6 out of 9 studies comparing rates of secondary speech surgery between groups with and without Robin sequence found no significant differences. This contradicts findings in a systematic review and meta-analysis, where strong evidence for higher rates of secondary surgery was reported in children with cleft palate and Robin sequence compared to children with cleft palate and no Robin sequence. 24
In the above-mentioned review by Sullivan, 8 3 studies with more robust methodology were included.25–27 Naros et al. 25 assessed speech in a total of 44 5- to 6-year-olds with cleft palate: 22 with Robin sequence and 22 without Robin sequence, all without other additional conditions. No significant differences in speech outcomes were found between groups. 25 Butterworth et al., 26 assessed speech in larger groups of 5-year-olds with oral clefts, 281 with and 1345 without Robin sequence. Children with diagnosed syndromes that could affect speech were excluded. Participants with cleft palate and Robin sequence were less likely to meet all 3 speech outcome standards than those without Robin sequence, but not when adjusted for sex and cleft extent. 26 Finally, Hardwicke et al. assessed speech in 5-year-olds with cleft palate: 24 with Robin sequence (including 3 children with syndromic Robin sequence) and 24 without. 27 They reported significantly poorer results in terms of nasality and more cleft speech characteristics in the group with Robin sequence compared to the group without Robin sequence. 27
Another study, using consensus listening, by Schwaiger et al., 28 was not included in the review by Sullivan et al. 8 They compared speech in 51 5-year-olds with cleft palate with Robin sequence (of which 8 had a diagnosed syndrome) with 128 children with nonsyndromic cleft palate without Robin sequence. 28 The group with Robin sequence had significantly more cleft speech characteristics. 28
To summarize, the results from previous studies on speech in children with Robin sequence are partly contradictory, which may to some extent be due to different inclusion and exclusion criteria as well as different methods for speech assessment. There is a need for more studies with robust methodology and a high number of participants to increase knowledge on speech outcomes in children with cleft palate and Robin sequence.
The Swedish Cleft Lip and Palate (CLP) Registry
The national Swedish CLP registry aims to promote quality control, research, and improvement of treatment. 29 It also enables investigation of speech in an entire national cohort of children with cleft palate with and without Robin sequence. The coverage and reporting degree of the registry is above 90%. 29 Various procedures for primary palatal surgery that differ in timing, staging, and technique are used at different Swedish CLP centers. 9 The cleft palate is usually closed in 1 stage, at between 9 and 15 months of age, or in 2 stages, with soft palate closure at about 6 months and hard palate closure at about 2 years of age. For more detailed information on primary palatal surgery in Swedish-born children, see Klintö et al. 9 In cases of suspected need for secondary surgery, velopharyngeal function is investigated with videofluoroscopy and/or nasoendoscopy before secondary palatal surgery is decided to be performed. Procedures for secondary surgery are re-repair of the palate, pharyngeal flap, buccal flap, and plastic surgery of the pharynx (eg, sphincter pharyngoplasty). For information on the incidence of surgical treatment of incompetent velopharyngeal function in Swedish children with cleft palate, see Schaar Johansson et al. 30
The Swedish CLP registry includes information on speech outcome reported by speech-language pathologists at ages 18 months and 5, 10, 16, and 19 years. 29 Data on diagnosed Robin sequence, syndromes, and/or additional malformations are registered at birth and updated continuously, and data on surgical intervention are registered continuously. Speech variables related to velopharyngeal function and consonant production are included. 29 The reliability of speech data in the CLP registry has been examined in several previous studies. Both the percentage of consonants correct (PCC) and the related quality indicator age-appropriate consonant production at 5 years have been found to be reliable. 31 Furthermore, data on the percentage of nonoral speech errors and the overall perceived velopharyngeal competence (VPC, ie, the impression of hypernasality, audible nasal air leakage, and weak articulation), and the related binary quality indicators, have been found to be reliable at 5 years of age. 32 For further information on the reliability of speech data in the Swedish CLP registry, see Klintö et al. 31 and Brunnegård et al. 32
Objective
The main objective of this registry-based study was to investigate speech outcomes at 5 years of age in a complete cohort of children with cleft of the hard and soft palate with and without Robin sequence. Speech outcomes of 4 groups of children were compared: with Robin sequence without additional conditions (RS−), with Robin sequence with additional conditions (RS+), without Robin sequence with additional conditions (CP+), and without Robin sequence without additional conditions (CP−). We also aimed to investigate differences in age at primary palatal surgery and occurrence of secondary palatal and/or velopharyngeal surgery and speech-language therapy up to 5 years of age between the subgroups.
Methods
The Ethics Review Authority in Sweden approved the study (reference no. 2020-00227). The consultation group for quality registries, care databases, and preparation approved data disclosure (reference no. 163-24).
Participants
A total of 545 children born with a cleft of the hard and soft palate in Sweden from 2009 to 2018 had been registered in the Swedish CLP registry (Appendix 1). Only 8 children with a cleft of the soft palate had a registered Robin sequence; thus, children with a cleft of the soft palate were not included. Participants who were deceased (n = 11), had emigrated from Sweden (n = 6), or had no primary palatal repair registered (n = 18) were excluded. This resulted in 510 children. Of those, an additional 24 were excluded since they did not attend their 5-year speech follow-up, 5 due to registrations outside the timespan (5 years of age ± 6 months), 37 due to absence of judgable speech, and 11 due to lack of speech registration for unknown reasons. The speech data for the remaining 433 children were used for analysis (Appendix 1). Reasons for missing speech data could be difficulties in participating in the follow-up at the CLP center due to additional conditions or lack of accessible speech.
Data in the Swedish CLP Registry
Coverage Degree
All 6 Swedish CLP centers are connected to the Swedish CLP registry. The coverage degree for children in the registry born with any type of oral cleft in Sweden from 2009 to 2018 was 94.3%, when comparing data on cleft diagnosis (ICD-10 33 ) from the Central patient registry, managed by the Swedish National Board of Health and Welfare, with data from the CLP registry.
Background Characteristics
Data on Robin sequence (yes/no), syndrome (yes/no), additional malformations (yes/no), and intellectual disability (yes/no) were available from the CLP registry. Detailed information on types of additional conditions was previously included in the CLP registry but has been removed as it was found to be unreliable; therefore, this information was not available for the present study. Furthermore, no information on socioeconomic status, ethnicity, or nonverbal IQ was available in the registry. Data on hearing status and diagnosed language impairment were available in the CLP registry but were considered unreliable due to insufficient reporting degrees; we therefore did not include those variables in our analyses.
Characteristics of the study sample are presented in Table 1. Of the included children, 62.8% had CP−, 16.6% had a RS−, 6.5% had a RS+, and 14.1% had CP+. As seen in Table 1, a larger proportion of participants in the CP− group were female (62.9%) than male (37.1%). In the other subgroups, biological sex was more evenly distributed.
Distribution of Biological Sex, Age at Primary Soft Palatal Surgery, and Age at Complete Primary Palatal Repair.
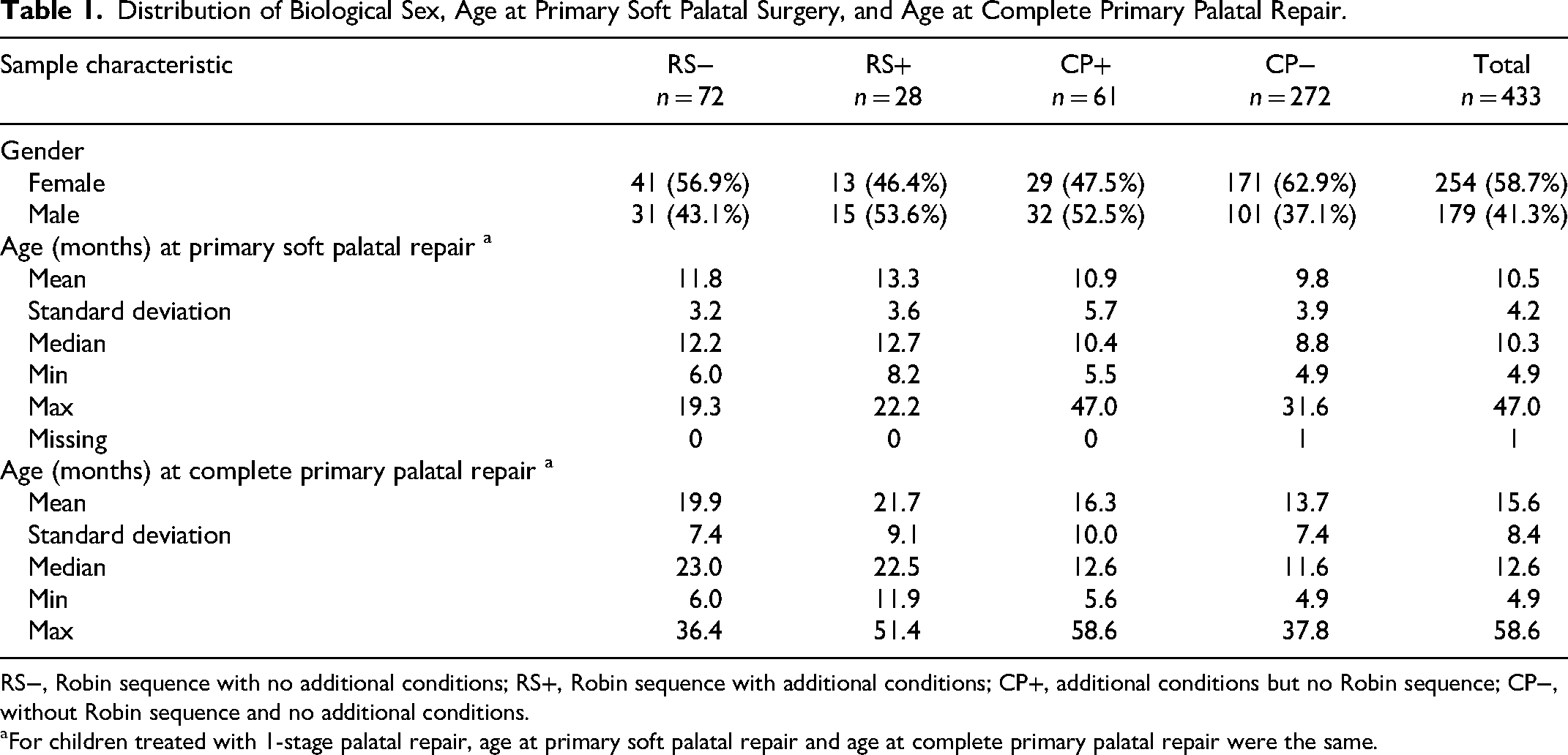
RS−, Robin sequence with no additional conditions; RS+, Robin sequence with additional conditions; CP+, additional conditions but no Robin sequence; CP−, without Robin sequence and no additional conditions.
For children treated with 1-stage palatal repair, age at primary soft palatal repair and age at complete primary palatal repair were the same.
To examine the risk of selection bias, group characteristics were compared between the 433 included children and the 77 children excluded due to no registered speech data, as presented in Appendix 2. We found that compared to the included group, in the excluded group the proportion of children with CP− was considerably smaller (31.2% vs. 62.8%) and the proportion with CP+, considerably larger (49.4% vs. 14.1%, Appendix 2).
Surgery Registrations
During the study period, 2 of the centers performed primary palatal surgery in 1 stage, and 1 transitioned from 1-stage surgery to 2-stage surgery. One center performed 1-stage surgery on children with cleft of the soft palate and cleft of the hard and soft palate, and 2-stage surgery on clefts including the lip and alveolus. Two centers performed 2-stage surgery.
Data on primary palatal surgery and secondary palatal and/or velopharyngeal surgery were recorded and coded according to the Swedish National Board of Health and Welfare's classification of health interventions. 34 The reporting degree of cleft-related surgeries, performed until 2022 for all children born from 2009 to 2022 in the Swedish CLP registry, was 94.4%, when comparing the number of cleft-related surgical intervention codes in the registry for each individual with the number of surgical intervention codes for each individual in the Central patient registry.
Speech Registrations
Speech data in the CLP registry were based on perceptual assessment of standardized audio recordings at 5 years of age ± 6 months, by speech-language pathologists at Sweden's 6 CLP centers. 2 or 3 speech-language pathologists specialized in cleft palate speech are affiliated to each CLP center. The speech-language pathologists who elicited and recorded the child's speech also performed speech analysis and recorded speech data.
Speech was assessed according to the procedure described in The Swedish Articulation and Nasality Test (SVANTE), including single word naming, sentence repetition, and continuous speech. 35 Of the 433 children who participated in the single word naming task, the majority (51.5%) were assessed with the original SVANTE single word naming test (59 words). In 40% of the cases, the SVANTE minimum standard set (30 words), included in the original SVANTE single word naming test, 35 was used, and in 8.5% of the cases, the word test in the randomized controlled trial TOPS (36 words). 3 All 3 tests were designed according to the same principles to analyze cleft speech characteristics. 36
Articulation variables were based on phonetic transcriptions of the single word naming task in the word tests according to the International Phonetic Alphabet 37 for 1 target consonant in each single word. PCC was calculated by dividing the number of correct consonants with the total number of elicited consonants. 35 If the target consonant was changed to another phoneme, it was scored as incorrect. The percentage of nonoral speech errors (ie, glottal and pharyngeal articulation, and active nasal fricatives) was calculated by dividing the number of incorrectly produced consonants with the total number of elicited consonants. Based on all available speech material, VPC was rated on the 3-point scale VPC-R, with scale values “competent/sufficient,” “marginally incompetent/insufficient,” and “incompetent/insufficient.” 35
Speech-Language Therapy
In connection with the speech assessment, the speech-language pathologists recorded whether the child had received speech-language therapy at their local clinic before age 5 years or not. Information on the number of speech-language therapy visits was available, but we considered the data to be unreliable due to a high proportion of missing values. Thus, this data was not included in the analysis. Information on the type of intervention is not recorded in the CLP registry.
Outcome Measures
Speech
Three binary outcome measures were derived from the perceptually assessed speech variables:
Age-appropriate consonant production, defined as at least 86% correct consonants, corresponding to 2 standard deviations below the mean of normal data in 5-year-olds without cleft palate
35
(yes/no). No nonoral speech errors, defined as a maximum of 5% nonoral errors, to have a margin of errors (yes/no). Velopharyngeal competence, defined as competent or marginally incompetent velopharyngeal function (yes/no).
Primary Palatal Surgery
Since some participants had been treated with 1-stage closure of the palate, and others with 2-stage closure, 2 variables regarding age at surgery were created:
Age at primary soft palatal repair Age at complete primary palatal repair
For children treated with 1-stage palatal repair, age at primary soft palatal repair and age at complete primary palatal repair were the same.
Secondary Intervention
For secondary surgery and speech-language therapy, 2 binary variables were created:
Secondary palatal and/or velopharyngeal surgery before 5 years of age (yes/no) Speech-language therapy before age 5 years (yes/no)
Statistical Analysis
Based on registrations of additional conditions in the CLP registry, participants were categorized into 4 subgroups: RS−, RS+, CP+, and CP−. Assumptions for logistic regression were evaluated and found to be acceptable, including the absence of multicollinearity and adequate sample size per cell. The association of subgroup membership to each of the 3 outcome variables was analyzed using logistic regression. Biological sex may influence consonant production in 5-year-olds with oral clefts, 9 but not velopharyngeal competence. 30 Thus, for the outcomes of age-appropriate consonant production and no nonoral speech errors, we used both an unadjusted model and a model adjusted for biological sex. Since Robin sequence often contributes to later primary palatal surgery, we decided against including age at primary surgery in the regression analyses. However, differences among subgroups in registered age at primary soft palatal repair and age at complete primary palatal repair were assessed with the Kruskal-Wallis test and a pair-wise analysis. Post hoc analysis with Dunn's test with Bonferroni correction of P-values was performed in cases of significant differences. To compare the occurrence of secondary palatal and/or velopharyngeal surgery and speech-language therapy before age 5 years between the groups, Fisher's exact test was used. Significance levels were set to P < 0.05 (2-tailed), and statistical analysis was performed using IBM SPSS Statistics version 28.0.1.1.
Results
Age at Primary Palatal Repair
Ages at primary soft palatal repair and complete primary palatal repair in the different subgroups are presented in Table 1. There were significant differences between subgroups in terms of age at primary soft palatal repair (H[3] 46.064; P < 0.001) and age at complete primary palatal repair (H[3] 60.416; P < 0.001). The group with RS− had undergone primary soft palatal repair at a significantly later age than the group with CP− (Tables 1 and 2). The group with RS+ had undergone primary soft palatal palate repair at a significantly later age than both groups without Robin sequence. Furthermore, the 2 groups with Robin sequence had complete primary palatal repair at a significantly later age than the 2 groups without Robin sequence. No other significant differences were seen regarding age at primary palatal repair (Tables 1 and 2).
Differences in Age at Surgery When Analyzed Pairwise (Dunn's Test).
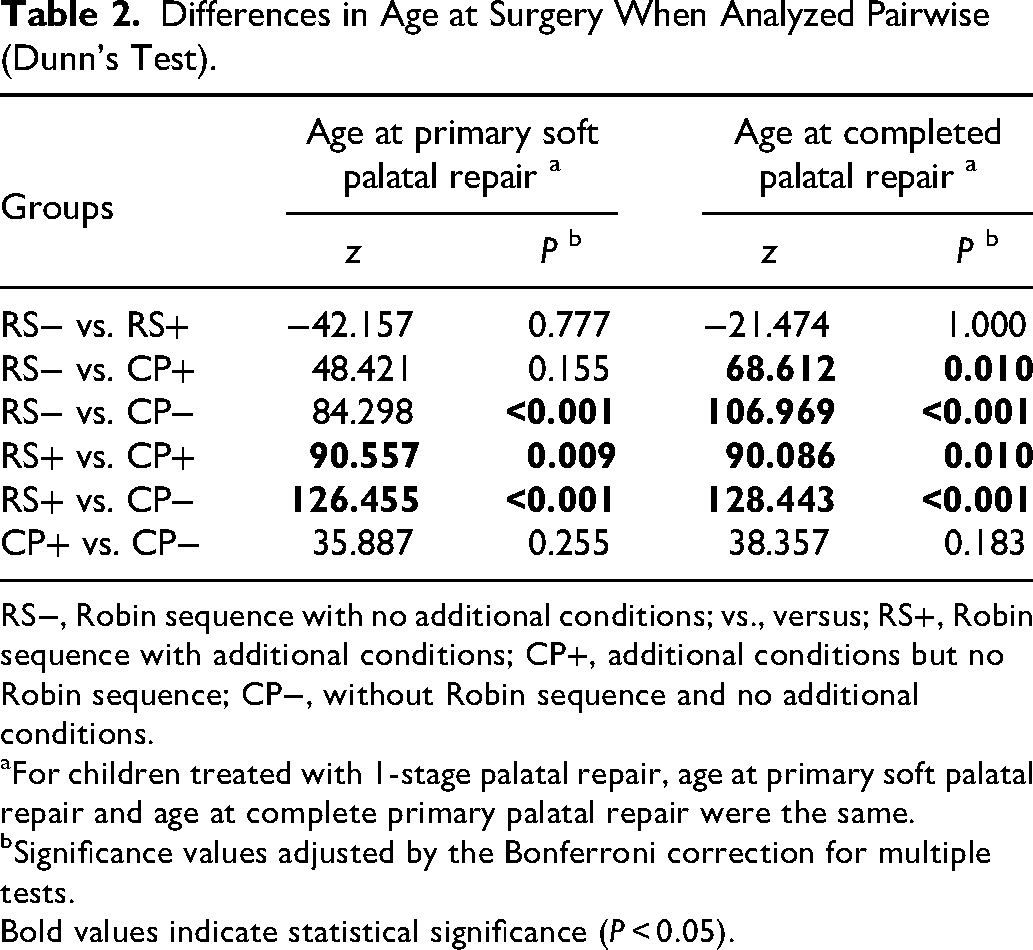
RS−, Robin sequence with no additional conditions; vs., versus; RS+, Robin sequence with additional conditions; CP+, additional conditions but no Robin sequence; CP−, without Robin sequence and no additional conditions.
For children treated with 1-stage palatal repair, age at primary soft palatal repair and age at complete primary palatal repair were the same.
Significance values adjusted by the Bonferroni correction for multiple tests.
Bold values indicate statistical significance (P < 0.05).
Occurrence of Secondary Palatal and/or Velopharyngeal Surgery
In the total group of 433 children, 9.7% had been treated with secondary palatal and/or velopharyngeal surgery before the age of 5 years (Table 3). The incidence was the lowest in the group with CP− and the highest in the group with RS+; however, no significant differences were seen (Table 3).
Proportions With a History of Secondary Palatal and/or Velopharyngeal Surgery and Speech-Language Therapy Before 5 Years in Different Subgroups Compared to the Group With Cleft Palate Only (Fisher's Exact Test).
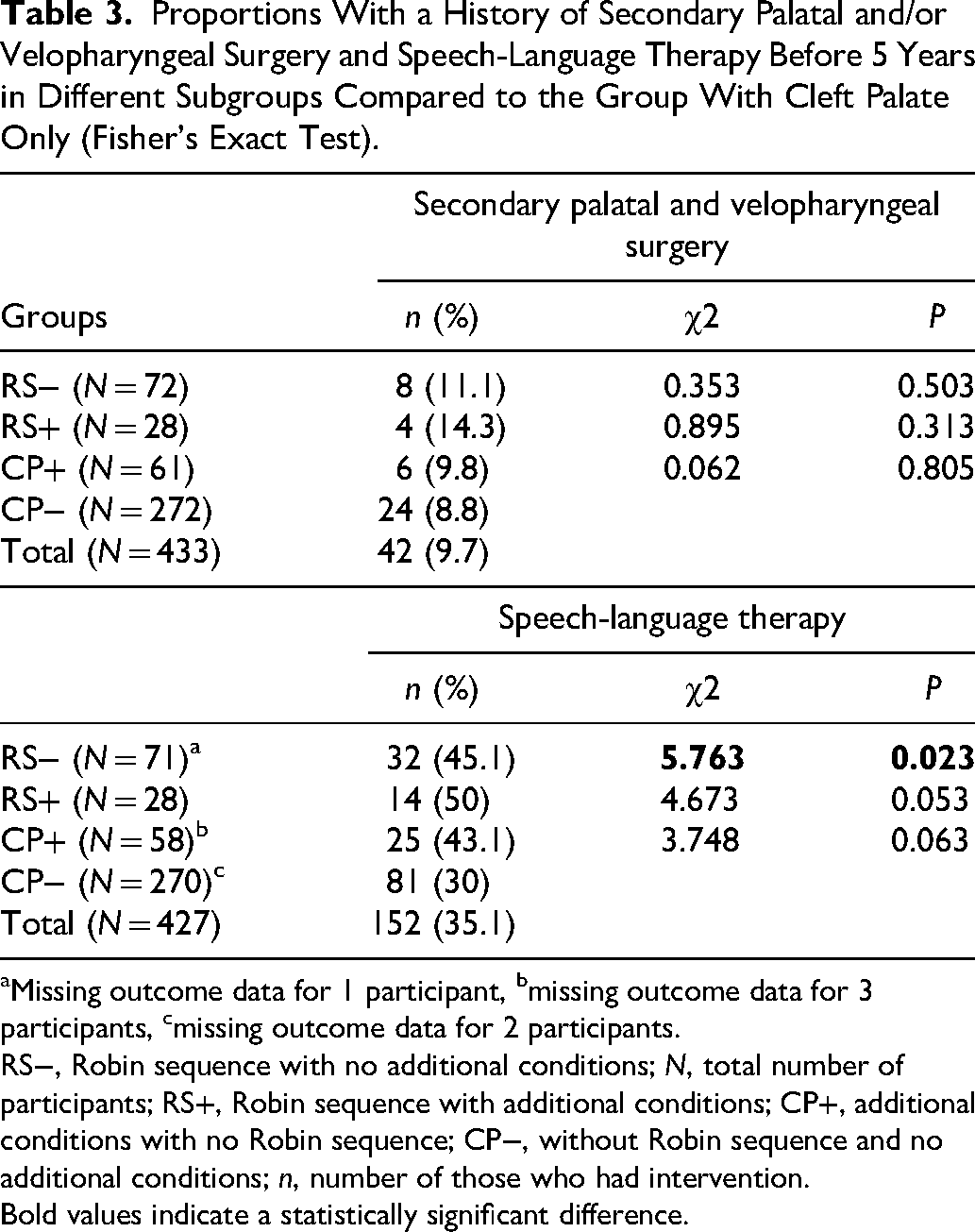
Missing outcome data for 1 participant, bmissing outcome data for 3 participants, cmissing outcome data for 2 participants.
RS−, Robin sequence with no additional conditions; N, total number of participants; RS+, Robin sequence with additional conditions; CP+, additional conditions with no Robin sequence; CP−, without Robin sequence and no additional conditions; n, number of those who had intervention.
Bold values indicate a statistically significant difference.
Occurrence of Speech-Language Therapy
The occurrence of speech-language therapy before 5 years of age is presented in Table 3. In some cases, there were missing data: 1 participant (1.4%) with RS−, 3 participants (4.9%) with CP+, and 2 participants (0.7%) with CP−. A significantly higher proportion of children with RS− (45.1%) had received speech-language therapy compared to the group with CP− (30%). Higher proportions of children who had received speech-language therapy were also seen in the groups with RS+ (50%) and with CP+ (43.1%); however, those differences were not statistically significant (Table 3).
Age-Appropriate Consonant Production
Results of logistic regression analysis modeling the odds of age-appropriate consonant production are presented in Table 4. There were missing outcome data for 2 participants (2.8%) with RS−, 1 participant (3.6%) with RS+, 8 participants (13.1%) with CP+, and 9 participants (3.3%) with CP−. Compared to participants with CP−, unadjusted odds for age-appropriate consonant production were 83% lower for those with RS+ (odds ratio (OR) = 0.17, 95% confidence interval (CI) = 0.08-0.40), 55% lower for those with CP+ (OR = 0.45, 95% CI = 0.24-0.84), and 50% lower for those with RS− (OR = 0.50, 95% CI = 0.29-0.88). When the model was adjusted for sex, the odds ratios increased marginally (Table 4).
Results of Logistic Regression Analysis Modeling the Association of Robin Sequence and/or Other Additional Conditions to Odds of Age-Appropriate Articulation at 5 Years of Age. The Adjusted Model Was Adjusted for Biological Sex.
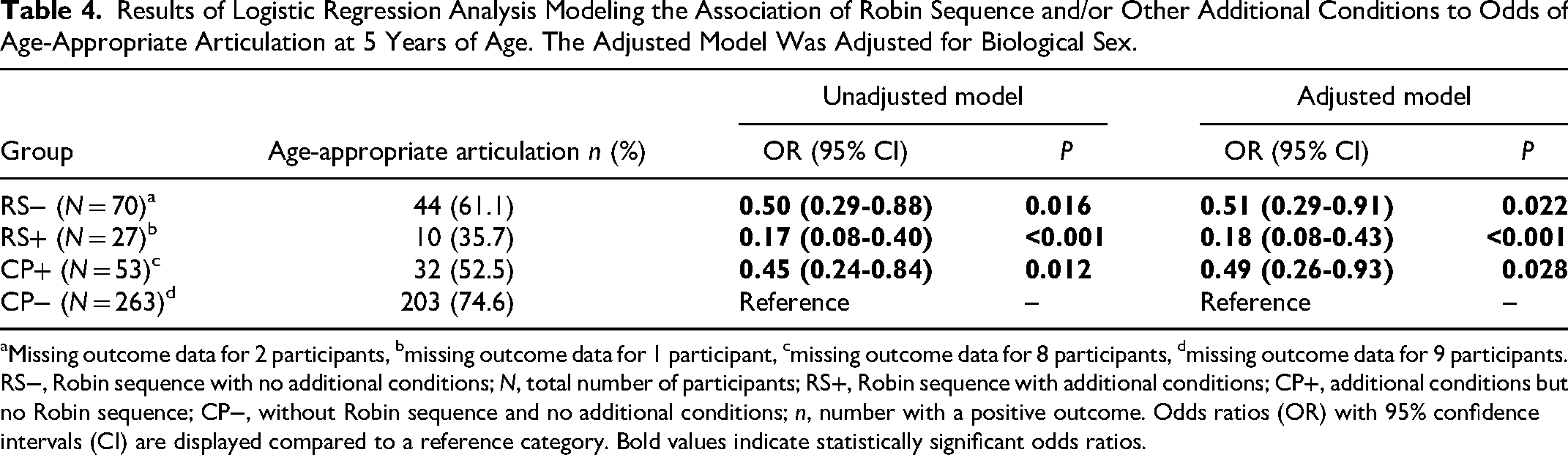
Missing outcome data for 2 participants, bmissing outcome data for 1 participant, cmissing outcome data for 8 participants, dmissing outcome data for 9 participants.
RS−, Robin sequence with no additional conditions; N, total number of participants; RS+, Robin sequence with additional conditions; CP+, additional conditions but no Robin sequence; CP−, without Robin sequence and no additional conditions; n, number with a positive outcome. Odds ratios (OR) with 95% confidence intervals (CI) are displayed compared to a reference category. Bold values indicate statistically significant odds ratios.
No Nonoral Speech Errors
Results of logistic regression analysis modeling the odds of no nonoral speech errors are presented in Table 5. There were missing outcome data for 2 participants (2.8%) with RS−, 1 participant (3.6%) with RS+, 8 participants (13.1%) with CP+, and 8 participants (2.9%) with CP−. Unadjusted odds for no nonoral speech errors were 83% lower for participants with RS+ (OR = 0.17, 95% CI = 0.07-0.39) compared to those with CP−. When the model was adjusted for sex, the odds ratio increased marginally. No other significant differences in odds ratios were found (Table 5).
Results of Logistic Regression Analysis Modeling the Association of Robin Sequence and/or Other Additional Conditions to Odds of No Nonoral Speech Errors at 5 Years of Age. The Adjusted Model Was Adjusted for Biological Sex.
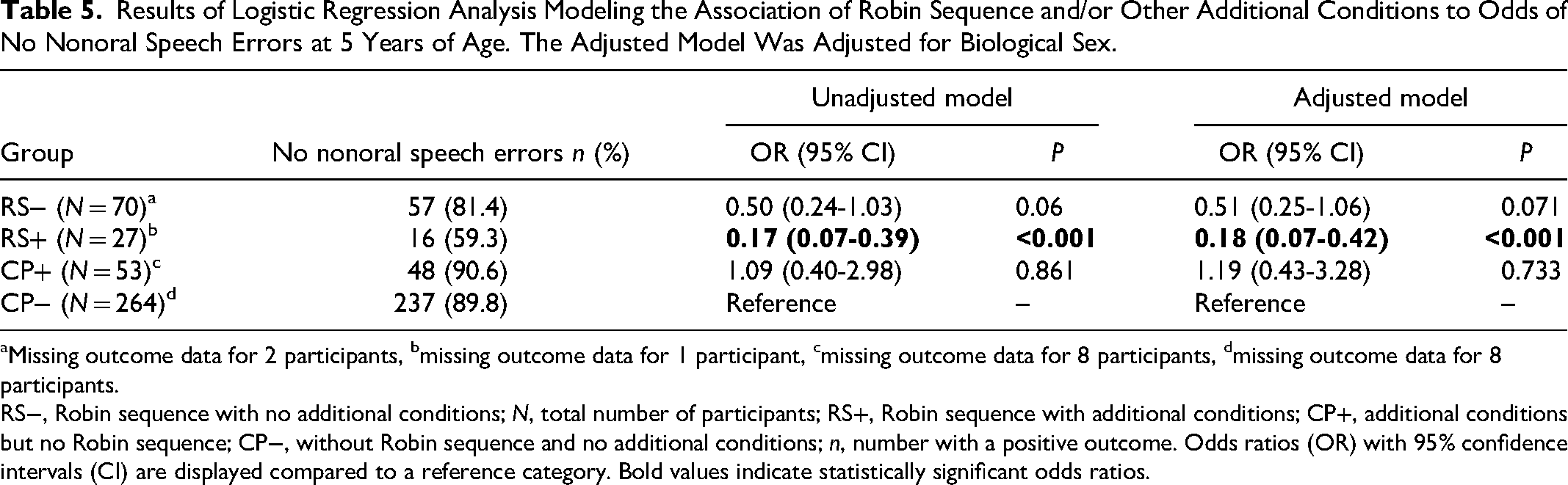
Missing outcome data for 2 participants, bmissing outcome data for 1 participant, cmissing outcome data for 8 participants, dmissing outcome data for 8 participants.
RS−, Robin sequence with no additional conditions; N, total number of participants; RS+, Robin sequence with additional conditions; CP+, additional conditions but no Robin sequence; CP−, without Robin sequence and no additional conditions; n, number with a positive outcome. Odds ratios (OR) with 95% confidence intervals (CI) are displayed compared to a reference category. Bold values indicate statistically significant odds ratios.
Velopharyngeal Competence
Results of logistic regression analysis modeling the odds of velopharyngeal competence are presented in Table 6. There were missing outcome data for 1 participant (3.6%) with RS+, 2 participants (3.3%) with CP+, and 1 participant (0,4%) with CP−. Odds of velopharyngeal competence were 76% lower for participants with RS+ (OR = 0.24, 95% CI = 0.10-0.56) compared to those with CP−. No other significant differences in odds ratios were found (Table 6).
Results of Logistic Regression Analysis Modeling the Association of Robin Sequence and/or Other Additional Conditions to Odds of Velopharyngeal Competence (VPC) at 5 Years of Age.
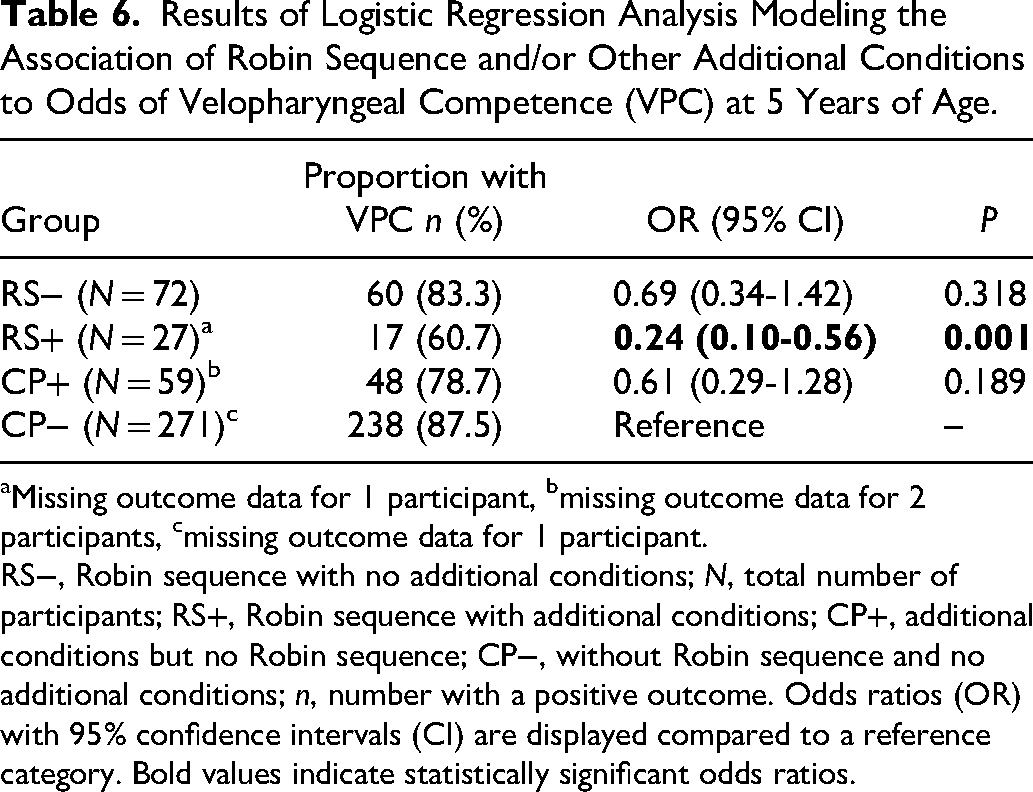
Missing outcome data for 1 participant, bmissing outcome data for 2 participants, cmissing outcome data for 1 participant.
RS−, Robin sequence with no additional conditions; N, total number of participants; RS+, Robin sequence with additional conditions; CP+, additional conditions but no Robin sequence; CP−, without Robin sequence and no additional conditions; n, number with a positive outcome. Odds ratios (OR) with 95% confidence intervals (CI) are displayed compared to a reference category. Bold values indicate statistically significant odds ratios.
Discussion
In this registry-based study, we compared speech outcomes of 5-year-olds with cleft of the hard and soft palate with RS−, with RS+, with CP+, and CP−.
Results Compared to Previous Studies
Compared to participants with CP−, the presence of Robin sequence or additional conditions decreased the odds of age-appropriate consonant production at 5 years of age by 50% to 55%. Participants with RS+ had 83% lower odds of age-appropriate consonant production than participants with CP−. Furthermore, the odds of no nonoral speech errors were 83% lower, and the odds of velopharyngeal competence were 76% lower, for participants with RS+ compared to participants with CP−. No significant differences in odds of no nonoral speech errors and velopharyngeal competence were found between groups with RS− and CP−.
The decreased odds of age-appropriate consonant production in participants with RS− compared to participants with CP− found here contradict results reported in 2 earlier studies.25,26 Naros et al. found no significant differences in articulation and hypernasality between 5- and 6-year-olds with cleft palate with and without Robin sequence; however, they included a lower number of participants (in total 44) 25 than the present study. Butterworth et al. found children with cleft palate and Robin sequence to be less likely to have good articulation and no structurally related speech difficulties or history of speech surgery than those without Robin sequence, but not when adjusted for sex and cleft extent. 26 In the studies by Naros et al. 25 and Butterworth et al., 26 children with known syndromes that could possibly affect speech were excluded. It should be taken into account that Butterworth et al. 26 included children with cleft of the soft palate, which were excluded in the present study due to the low number of children with cleft of the soft palate with Robin sequence. An alternative to excluding them would have been to include them in the larger group with cleft of the hard and soft palate. We decided not to do so, as we have previously found differences in speech outcomes between children with cleft of the soft palate and cleft of the hard and soft palate. 9
The decreased odds of age-appropriate consonant production in children with RS+ are in line with the findings by Hardwicke et al. 27 and Schwaiger et al., 28 who also included cases with diagnosed syndromes and found significantly more cleft speech characteristics in 5-year-olds with cleft palate and Robin sequence than in peers with non-syndromic cleft palate without Robin sequence. It is possible that some variables which could not be controlled for in the present study, that may have a negative effect on articulation, such as, hearing impairment and low nonverbal IQ were more common in the subgroups with additional conditions than those without.
Robin sequence or additional conditions alone did not decrease the odds of velopharyngeal competence, while the combination of Robin sequence and additional conditions did. The results are not fully comparable with those in previous studies, as other inclusion criteria and groupings have been used.2,27,38 Persson et al. found a higher frequency of speech symptoms related to velopharyngeal function in children with cleft palate with additional malformations and/or syndromes, including Robin sequence, than those without. 2 Hardwicke et al. found a higher prevalence of hypernasality in the group with Robin sequence, including cases with syndromes. 27 Butterworth et al. found reduced odds of no cleft speech characteristics and symptoms of incompetent velopharyngeal function in children with 2 or more congenital differences without diagnosed syndromes. 38
In the CP− group, 87.5% had competent velopharyngeal function, which means that 12.5% had incompetent velopharyngeal function. This is equivalent to the results in the TOPS trial, where 12% were reported to have incompetent velopharyngeal function at 5 years of age. 3 In the TOPS trial, the composite score VPC-Sum was used, based on single word speech material and combining hypernasality ratings and frequency of passive velopharyngeal symptoms and nonoral speech errors. 3 In the present study, the binary variable used for velopharyngeal competence was based on the VPC-R scale. Moreover, in the TOPS trial, only nonsyndromic children with cleft palate who were medically fit for cleft palate surgery at 6 months of age were included, leading to a more selected sample than the sample studied here. Furthermore, parents of 299 children declined participation in the TOPS trial, and only speech recordings of 461 out of 558 (82.6%) included children were analyzed, while the reporting degree for speech was over 90% in the present study. Genetic testing is not obligatory in the Swedish CLP registry, as it was in the TOPS trial, 3 and it should also be taken into account that syndromes and additional conditions are underreported in the CLP registry. 39 To summarize, methodological differences mean that the results are not fully comparable.
Primary Palatal Surgery
Primary palatal surgery completed at a later age may be disadvantageous for speech outcomes at 5 years of age. 9 The larger cleft width, common in Robin sequence,7,8 makes palatal surgery more challenging, 8 and may delay the timing of the surgery. Other reasons for delayed primary palatal repair include other ongoing medical interventions precluding safe surgery, and known airway obstruction, where cleft palate repair may increase the obstruction. 7 As expected, participants with Robin sequence had primary soft palatal repair and complete palatal repair at a significantly later age than participants with CP−. This may have contributed to poorer speech results at 5 years of age in participants with Robin sequence than without. 8
Secondary Palatal and Velopharyngeal Surgery
In an earlier study, we found that primary palatal surgery at a later age may be associated with increased risk of secondary palatal and velopharyngeal surgery. 30 In the present study, although the participants with Robin sequence had primary palatal surgery at a later age than those with CP−, we found no significant differences between groups regarding the occurrence of secondary palatal and/or velopharyngeal surgery. These results were unexpected, since previous studies have shown significantly higher rates of secondary speech surgery in children with cleft palate with Robin sequence than without.24,28 On the other hand, in the present study, children with RS− did not have significantly lower odds of achieving competent/marginally incompetent velopharyngeal function than peers with CP−. It therefore seems likely that there was no greater need for secondary surgery in this subgroup compared to the group with CP−. Children with RS+ had decreased odds of achieving competent/marginally incompetent velopharyngeal function than peers with CP−, and this subgroup had the highest proportion of children who had undergone secondary surgery before 5 years of age, although the differences were not statistically significant. It should be taken into account that in the present study, registry data at 5 years of age were investigated, and some children might have undergone secondary palatal and/or velopharyngeal surgery at a later age.
Speech-Language Therapy
Participants with RS− had received speech-language therapy to a significantly higher degree than children with CP−. Compared to the group with CP−, higher proportions in the group with RS+ and the group with CP+ had received speech-language therapy; however, the differences were not significant. It cannot be ruled out that the differences would have been significant if the subgroups had been larger. Other interesting aspects of speech-language therapy in subgroups, such as, extent and type of therapy 40 cannot be determined from a multicenter registry study, since it is not possible to achieve sufficient reliability on such detailed data.
Methodological Issues and Limitations
This study was based on prospectively collected registry data, including the whole cohort of children born with cleft of the hard and soft palate in Sweden from 2009 to 2018. The use of registry data made it possible to study speech in larger groups than would otherwise have been possible. We chose to exclude children with cleft of the soft palate from the study, since the cohort included only 8 children with cleft of the soft palate with Robin sequence. Thus, if participants with a cleft of the soft palate had been included, some subgroups would have been too small to analyze. The coverage degree and reporting degree for surgeries and speech in the Swedish CLP registry are above 90%, 29 which is high compared to, for example, the randomized controlled trial TOPS. 3 Of the 77 excluded children with cleft of the hard and soft palate in the present study, the majority (n = 42) had additional conditions other than Robin sequence, and likely not enough speech to participate in speech assessment. This might have biased the results toward better average outcomes in the included cohort, and should be considered when generalizing findings.
Reliability of speech data in the Swedish CLP registry at 5 years of age, and the binary outcomes based on speech data used in the present study, has been investigated in 2 studies and considered good.31,32 Nevertheless, when interpreting the results, one should be aware of certain limitations of the study, such as the use of 3 different word tests to collect the speech data. This is somewhat compensated by the fact that all word tests were designed according to the same principles, to capture cleft palate speech errors, 36 minimizing the effects of the differences between the tests on speech results.
An advantage of using binary variables as speech outcomes is that the outcomes are robust and have good reliability.31,32 They are also clinically relevant, as the cut-offs have been set at levels where intervention should be initiated if the results are not positive. For example, children who are judged to have incompetent (rather than marginally incompetent or competent) velopharyngeal function should be offered visualizing examination of velopharyngeal function in order to decide if secondary surgery is required. 32 This cut point is therefore clinically relevant. Children who do not have a positive result on the outcome age-appropriate consonant production, where the cut-off corresponds to 2 standard deviations below the mean in normal data, 35 should be offered speech therapy. Similarly, children who do not have a positive result on the outcome no nonoral speech errors should be offered speech therapy, as nonoral speech errors are abnormal processes not seen in typically developing Swedish-speaking children. The disadvantage of the binary indicators is that they are rough, meaning that detailed information on speech may be missed.
Although variations in factors such as nonverbal IQ, type of speech-language therapy offered, 40 cleft width, 41 skill of involved surgeons, 42 and socioeconomic status 26 could potentially influence speech outcomes, those variables are not reported in the CLP registry and could therefore not be adjusted for in the analysis. Moreover, although included in the CLP registry, data on hearing status and number of speech-language therapy visits, which may also impact speech development,40,43 is often missing from registrations and therefore not sufficiently reliable to include in research studies. Hearing is often tested at local hospitals on separate occasions rather than in conjunction with the follow-ups at the CLP centers. Similarly, as Sweden is a geographically large country, speech-language therapy is usually carried out at local hospitals rather than at the CLP centers. In connection with the follow-ups at the CLP centers, the speech-language pathologists at each center aim to collect data on speech-language therapy from the local speech-language pathologists, but this information can be difficult to access. Registrations, therefore, usually include information on whether the children have received speech-language therapy or not, but not always to what extent and never of what type. With increasingly detailed variables comes increasing difficulty in achieving high reliability; this has been taken into careful consideration when deciding which variables to include in the Swedish CLP registry. To summarize, several possible confounding variables could not be controlled for in the present study.
In line with previous studies,2,38 our findings indicate that additional conditions have a negative impact on speech outcomes. It is likely that the independent variable, additional conditions in this study included both conditions with a high and low impact on speech. The measure PCC includes both speech problems typical of cleft palate and incompetent velopharyngeal function, and speech errors unrelated to cleft palate and incompetent velopharyngeal function. A lower PCC score is therefore not always an indication of speech problems related to cleft palate/ incompetent velopharyngeal function. The lack of detailed information on types of additional conditions in the registry data made the analysis of the impact of specific diagnoses on speech based on this dataset impossible. Another fact that needs to be considered when interpreting the results is that it can be assumed that additional conditions, especially those detected at a later age, are underreported in the CLP registry. 39 In a previous study at 1 Swedish CLP center, it was found that the prevalence of additional diagnoses was 14.4 percentage points higher in medical records than in the CLP registry. 39
Conclusions
The presence of the Robin sequence or additional conditions in children with cleft of the hard and soft palate decreased the odds of age-appropriate consonant production at 5 years of age. The lowest odds for age-appropriate consonant production were found in the group with RS+. This group also had lower odds of having no nonoral speech errors and velopharyngeal competence than those with CP−. These findings underscore the need for targeted follow-up and early speech-language intervention, particularly for children with RS+. The results can form the basis for informing parents of children born with cleft palate and Robin sequence regarding prognosis for speech outcomes at 5 years of age, and when planning intervention and follow-up for children born with Robin sequence.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656251387538 - Supplemental material for Speech Outcomes in 5-Year-Olds Born With Cleft Palate With and Without Robin Sequence—A Swedish Registry Study
Supplemental material, sj-docx-1-cpc-10.1177_10556656251387538 for Speech Outcomes in 5-Year-Olds Born With Cleft Palate With and Without Robin Sequence—A Swedish Registry Study by Kristina Klintö, Malin Schaar Johansson, Karin Brunnegård and Magnus Becker in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656251387538 - Supplemental material for Speech Outcomes in 5-Year-Olds Born With Cleft Palate With and Without Robin Sequence—A Swedish Registry Study
Supplemental material, sj-docx-2-cpc-10.1177_10556656251387538 for Speech Outcomes in 5-Year-Olds Born With Cleft Palate With and Without Robin Sequence—A Swedish Registry Study by Kristina Klintö, Malin Schaar Johansson, Karin Brunnegård and Magnus Becker in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgments
The authors are grateful to all CLP team members who have contributed data to the CLP registry.
Ethical Approval and Informed Consent
This study was approved by the Ethics Review Authority in Sweden (reference no. 2020-00227). Data disclosure was approved by the Consultation Group for Quality Registries, Care Databases, and Preparation in Region Skåne (reference no. 163-24). The Ethics Review Authority of Sweden waived the requirement for informed consent because of the retrospective nature of the study. The procedure for information and consent followed the legal guidelines for participation in national quality registries in Sweden.
Funding
This study was funded by The Sven Jerring Foundation, Maggie Stephen's Foundation, The Foundation in Memory of Consul Thure Carlsson, and The Promobilia Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available because of ethical restrictions but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.