
Abstract
Objective
The German system of care for patients with cleft lip and/or palate (CL/P) is fragmented. An argument against centralization is that the higher burden of travel for patients in remote and rural areas would reduce appointment adherence and subsequent care outcomes. Our objective was to test the association of travel burden and adherence and outline potential benefits of centralized cleft care.
Design
Follow-up appointments June 2005 to August 2020 were retrospectively analyzed for patients with CL/P in a large German tertiary care center. Distance to care center and travel time by car/public transportation were calculated using Google Maps. Demographic characteristics included population density, degree of urbanization, and average disposable income per capita of the municipality of origin. Multiple regression models including flexible spatial function learning assessed associations with follow-up appointment adherence.
Results
Patients (n = 1140) had 9447 scheduled appointments with a 48.2% attendance rate. Distance to the clinic (M = 85.19 ± 75.12 km, range 0.45–536), travel time (M = 71.18 ± 48.5 min, range 2–330), population density (725.32 ± 807.82 inhabitants/km², range 14–4861), and lower average income (20,993.38 ± 1220.72 Euro, range 14,521–32,348.83) were not associated with appointment attendance. Patients from more rural areas were slightly more likely to attend check-ups (p = 0.027, 95% CI [0.016, 0.212]).
Conclusion
The burden of travel to the clinic was not associated with attending follow-up appointments for patients with CL/P. These findings challenge a common assumption about attendance and warrant further multi-center studies to inform policy decisions for restructuring cleft care in Germany.
Introduction
In 1992, the authors of the Eurocleft study realized that – while different clinical procedures might all lead to acceptable results – standardization, centralization, and therapy through high volume operators are directly correlated with good outcomes. They reasoned that the future of the specialty lies with larger centers that permit intercenter surgical audits. 1 In the United Kingdom, these results, combined with the results of a multicenter study commissioned by the UK health ministers and supervised by the Clinical Standards Advisory Group, 2 triggered the reorganization of care provision for patients with cleft lip and/or palate (CL/P). Operating sites were reduced from 57 clinics to 11 specialist clinical networks and the number of surgeons responsible for primary surgery was significantly reduced. 3 Multidisciplinary care is coordinated within a unified framework by the National Health Service (NHS), that provides universal health care. Services are funded through taxation and free at the point of use. However, waiting times for certain services and delays in non-urgent surgeries can occasionally occur due to resource constraints in the public system. 4 Some 15 years later, a national evaluation of changes in clinical outcomes and patient satisfaction, known as the Cleft Care UK study, was conducted. 3 While some areas, like audiological outcome and prevalence of dental caries, showed little to no improvement, 5 the overall assessment was very favorable. Improved outcomes were observed in facial appearance and dentoalveolar relationships, 6 perceptual speech outcomes 7 and children's self-confidence. 8 Similar efforts to limit the number of specialized multidisciplinary cleft teams were undertaken in the Netherlands, 9 Hungary, Slovak Republic, and Poland 10 inspired by the example of the UK and the Scandinavian countries, that traditionally rely on centralized healthcare.
In comparison, care provision in the United States is regionalized, with specialized cleft teams concentrated in major medical centers. The level of service varies significantly between states and even between individual hospitals or clinics, leading to disparities in treatment quality. 11 The U.S. health care system operates primarily on a private insurance model integrating various public programs, such as Medicaid and Medicare. This fragmented structure has ambiguous effects for patients with CL/P. Access to specialized care mostly depends on insurance coverage, which varies significantly based on socioeconomic factors, geographical location, and whether patients are insured through private plans or public programs.11–14 The cost of surgery, ongoing speech therapy, orthodontics, and psychological care can result in significant financial barriers for families.15–17 On the other hand, assuming that the necessary access is granted, highly qualified specialized care teams, particularly in academic medical centers and cleft-craniofacial centers, provide advanced primary and follow-up care.
In Germany, the health care system is a hybrid of statutory health insurance (SHI) and private health insurance, with the majority of the population covered under SHI. This system provides near-universal coverage and guarantees access to high-quality care, 18 including for those with CL/P. However, care is delivered through a decentralized network of specialized centers, each with varying levels of expertise and resources and working according to their own organizational approach. While small centers might achieve positive outcomes for their patients, it has been argued repeatedly that their small numbers render it difficult to statistically prove the quality of their therapeutic concept.1,19 In contrast, regional university hospitals and certified craniofacial units offer highly specialized cleft care with larger patient populations. Currently, no national registry of cleft centers exists and there is no system of center accreditation. Germany does not have a central cleft organization equivalent to the American Cleft Palate-Craniofacial Association (ACPA), although working groups such as the German interdisciplinary working group for cleft lip and palate/craniofacial anomalies (Arbeitskreis LKG, AK-LKG) 20 strive to foster interdisciplinary collaboration.
Examining different healthcare systems and care structures helps to identify each systems’ benefits and disadvantages influencing patient outcomes through different mechanisms of coverage, cost, and organization. In the context of healthcare reforms, these insights could be used to ensure that available resources are allocated as sensibly and effectively as possible to achieve optimal treatment outcomes for all patients.
In Germany, the so-called hospital reform bill passed the responsible legislative institutions in autumn 2024 and implementation will proceed in stages through 2026. The reform aims at enhancing efficiency, quality, and financial sustainability within the healthcare system. Central to the reform is a shift from volume-based to needs-based hospital financing, introducing fixed base payments to reduce financial incentives for high case volumes. Hospitals will be categorized into three levels—basic, regular, and maximum care—based on the scope and complexity of services provided. This system is meant to safeguard and improve the quality of treatment, defining quality criteria for specialist clinics, that correspond to their range of services. 21 The ministry argues that for planned surgeries, better treatment outcomes outweigh longer travel times. Examples include significantly improved survival rates for cancer patients primarily treated in certified centers and significantly lower numbers of revision surgeries in the case of orthopedic total joint replacements. The same benefits should apply to the primary surgery and ongoing follow-up care of patients who are born with a CL/P.
A frequently cited concern about centralizing care is that the significantly higher time and financial cost of longer journeys might lead to socially disadvantaged families in particular being unable or unwilling to attend appointments.12,14,22–25 This, in turn, could lead to a significant deterioration in care and clinical outcomes, especially in vulnerable patient groups.
The aim of this study was to evaluate the correlation between the distance from patients’ homes to our care center and the corresponding travel time with the frequency of attending scheduled follow-up appointments. We hypothesized that the frequency of appointments kept would decline with increased distance and travel effort. Additionally, evaluated factors included demographic characteristics such as income structure, public transport accessibility, and degree of urbanization of the place of residence. The degree of urbanization was included as a variable since local access to social and healthcare institutions might influence mobility behavior and willingness to travel longer distances.
Methods
In the present study, patients were treated at a tertiary care center and specialized center for cleft care in Germany. The retrospective analysis was approved by the ethical review committee of the Medical Faculty, Leipzig University, Germany (IRB Board Number 00001750). Medical reports of all patients who were seen at the clinic's consultation hour for cleft patients between June 2005 and August 2020 were matched with their place of residence indicated and included in the assessment.
Patients after primary reconstruction are scheduled at least once a year for follow-up through age 18 in the weekly interdisciplinary consultation hour in order to identify problems during growth and arrange for timely interventions. During the appointment, the maxillofacial surgeon, orthodontist, and speech therapist carry out examinations and recommend treatment if necessary. An otorhinolaryngology or pediatric audiology specialist is consulted if required. Other specialties can be called upon for specific questions. After each consultation, a follow-up appointment is scheduled. For data analysis, we tracked whether patients kept their scheduled annual appointments. The number of possible visits was based on the date of the first presentation and the age at this point. For example, 8 annual visits would be expected for all patients who were 10 years old in 2005, while only 1 annual visit was expected during the study period for patients who had primary surgery in 2019. Adherence was thus defined as the proportion of possible appointments attended.
Additionally, patients with suspected diagnosis of submucous cleft and patients with CL/P in need of medical advice or further medical care can present for consultation. The latter group, defined as patients referred with a specific concern (ie, exclusion of submucous cleft, planning of prosthetic rehabilitation in adult patients), was excluded from the analysis.
For the remaining subjects, data concerning their journey to the outpatient clinic was collected. Google Maps (Google 2025, maps.google.de) was used to calculate the distance by car in kilometers, entering the home address and the clinic address. The estimated travel time by car (minimum, maximum, best estimate) for a Friday morning arrival (as consultation hours take place at this time) was also calculated. In addition, public transportation connections and estimated travel time were determined.
Starting from postal codes, we used data from the Federal Statistical Office to determine the population density and the degree of urbanization of the municipality of origin. 26 The population density was recorded in inhabitants per square kilometer; the degree of urbanization is indicated by the Federal Statistical Office in three levels (1 = densely populated, 2 = medium population density, 3 = sparsely populated). Population density was included as a variable alongside degree of urbanization as it provides a finer-grained, more continuous measure that captures variation within urban and rural areas. This way, it helps differentiate between sparsely and moderately populated urban and rural areas and clarifies the effect of the degree of urbanization, which is useful as an indicator of accessibility of public facilities and services, in particular specialized healthcare. The official regional key provided by the Federal Statistical Office was used to identify and assign the disposable income per capita (in Euro) of the corresponding territorial unit from a dataset made available by the Institute of Economic and Social Sciences. 27
Data Analysis
We used the R package Bayesian Regression Models with the programming language Stan (brms) 28 to run multilevel binomial regressions modeling the probability that patients would attend follow-ups in any given year as a function of the four predictor variables. A binomial likelihood is appropriate for aggregated binary data with a certain number of attendances in a fixed number of years, automatically accounting for different numbers of available years across individuals.
To capture complex and potentially non-linear effects of residential distance to the care center as well as travel times, we used a Gaussian process (gp) as a flexible tool for function learning (implemented through the gp() function in brms). The urbanity index was included as an ordered categorical predictor (via the monotonic predictor mo() function), while both population density and average income were z-standardized before analysis and entered as linear predictors. Finally, to account for the nested data structure and potential heterogeneity among individuals, we included individual ID as a random effect. We used the default priors of the brms package. Visual inspection of traceplots and rank histograms suggested good model convergence and no other pathological chain behaviors, with convergence confirmed by the Gelman-Rubin criterion R^hat ≤ 1.01. All inferences are based on several hundred effective samples from the posterior. To validate the results of our Bayesian model, we repeated the analysis using frequentist methods and fitted simpler models with all variables entered as linear predictors in the R package linear mixed-effects models using Eigen and S4 (lme4). 29 A significance level of 0.05 was assumed for all frequentist analyses.
Results
Data of 1182 patients were examined. Patients with missing records were excluded (n = 4). Thirty-eight cases presented on referral. In 28 cases, a submucosal cleft palate could be excluded clinically, in 4 cases, specialized prosthetic restoration was initiated, in 6 cases other specific problems were solved in a single setting. All cases were excluded from further analysis. Subsequently, the statistical evaluation included data of 1140 patients. Female participants accounted for 43.2% (n = 493) of the sample, while 56.8% (n = 647) were male. The average age was 7.41 years (± 8.49) at the beginning of the study period and 15.58 (± 10.61) years at the end of the period. The largest group of patients was those with unilateral or bilateral cleft lip and palate (CLP), with 492 patients (43.16%). Next were patients with cleft palate only (CP), with 377 patients (33.07%), followed by patients with cleft lip only (CL), with 271 patients (23.77%). In total, 48.24% of 9447 scheduled appointments were kept; this corresponds to one to eleven appointments per capita.
The mean distance between the home address and the outpatient department was 85.19 km (± 75.12). The average of the estimated journey time by car was 71.18 min (± 48.5). Average journey time by public transportation was 113.55 min (± 75.13). In 77 cases, Google Maps was not able to identify means of public transportation for the journey, these individuals were excluded only for the respective analysis.
The mean population density was 725.32 ± 807.82 inhabitants per square kilometer. There was a fairly even distribution across patients with 354 families in densely populated areas (degree of urbanization = 1), 456 in areas of medium population density (degree of urbanization = 2) and 368 came from sparsely populated areas (degree of urbanization = 3). Average annual income was 20993.38 Euro (± 1220.72).
Figure 1 visualizes the data and plots the Bayesian model results including 95% credible intervals (see Table 1 for p-values of the frequentist analysis). The large map on the left shows the average proportion of attended follow-ups for all individuals from a given postal-code area (larger proportions are indicated by darker dots), while the inlet plot zooms in on the region surrounding the care center (“UKL” in the map) and additionally visualizes how many individuals came from each area. From visual inspection alone, it becomes evident that patients from the immediate vicinity of the care center do not attend follow-up appointments more reliably. And indeed, the Bayesian function-learning results in Fig. 1 reveal that there is no general decrease in attendance for individuals living further away from the tertiary care center, which is also supported by the frequentist model (p = 0.567, Table 1). Looking at Google Maps’ calculated travel time by car or public transport as alternative distance measures (Figure 2) again reveals no association with the likelihood of keeping appointments (travel time by car: p = 0.909, travel time by public transport: p = 0.0724). In the frequentist model, there is a small statistically significant (p = 0.027) association for the degree of urbanization: Patients from more sparsely populated areas were slightly more likely to present for follow-up examination. Accounting for the urbanity index, the population density itself (ie, inhabitants per square kilometer) does not show this effect. Lastly, the average income per capita (in Euro) shows a relatively uncertain (yet, in frequentist model, statistically significant) downward trend: the higher the average income in an area, the lower the probability of attendance tended to be. Note that this effect is driven by a few outliers from wealthy residential areas far away from the care center who were relatively unlikely to attend follow-ups. Specifically, the ten individuals from the highest-income regions all travelled more than 350 km and attended only 12.19% of appointments.
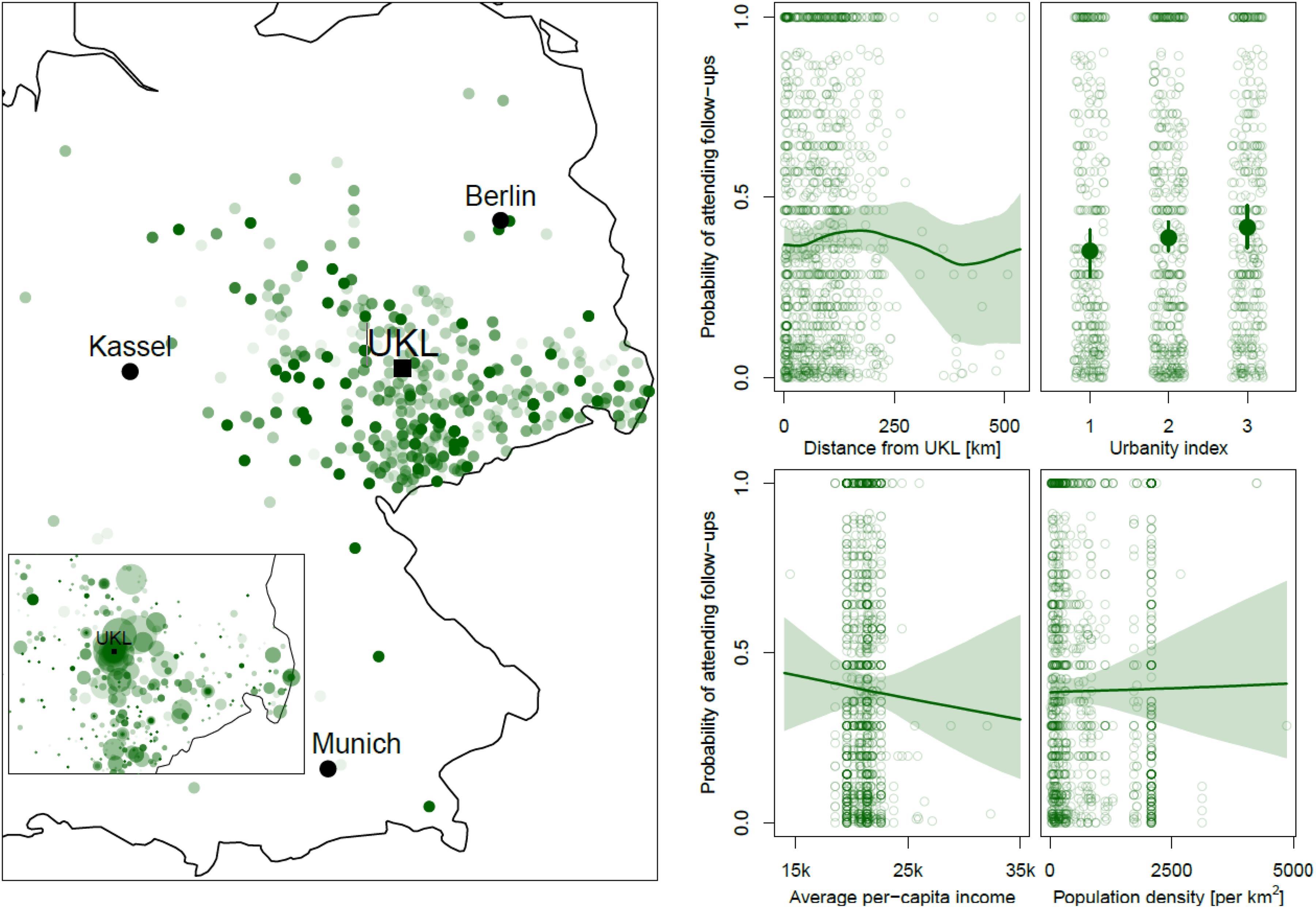
On the Left, Patients’ Place of Origin is Shown Geospatially; The Strength of the Color Indicates the Likelihood of Attending Follow-up Visits (the Darker the Shade, the Higher the Probability of Attendance). In the Inlet, the Size of the Dots Represents the Number of Patients from that Region. The Plots on the Right-Hand Side Show the Association Between the Probability of Attending Follow-up Appointments and Each of the Variables Shown on the X-axis Including 95% Credible Intervals. UKL: University Cleft Center at Leipzig University Hospital (Universitätsklinikum Leipzig, Germany).
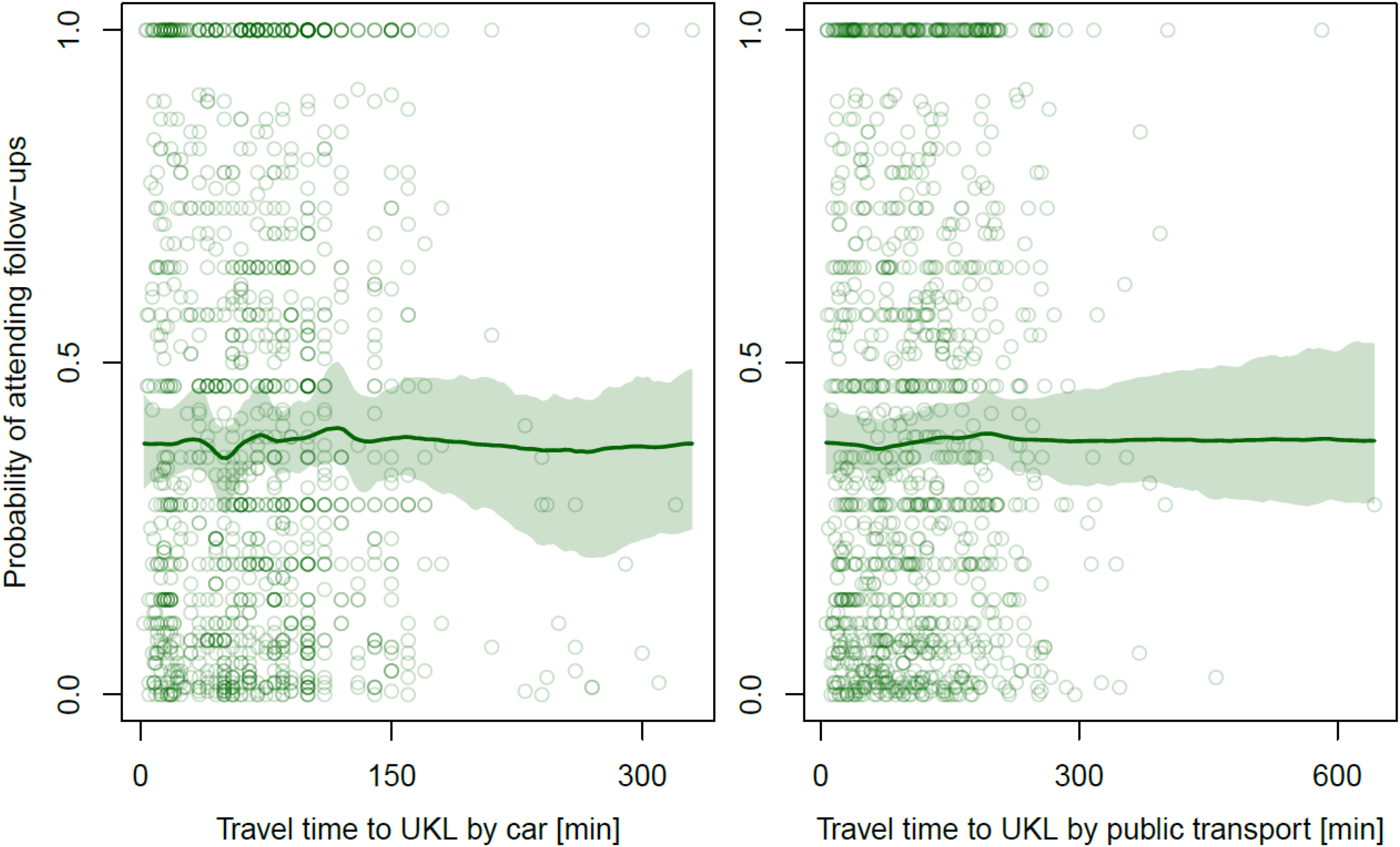
Association Between the Travel Time by Car or Public Transport and the Probability of Attending Follow-up Appointments Including 95% Credible Intervals. UKL: University Cleft Center at Leipzig University Hospital (Universitätsklinikum Leipzig, Germany).
Associations Between Residential Distance to the Care Center and Demographic Characteristics and the Probability to Attend Follow-up Appointments from a Multilevel Multiple Regression Model. The Level of Significance Was Accepted at p < 0.05, Statistically Significant Numbers Were Marked with an Asterisk.

Discussion
The objective of this paper was to determine if burden of travel for patients in remote and rural areas reduces the adherence to follow-up appointments. In our sample of 1140 patients with CL/P, we did not find a correlation between distance to care center and probability of attending scheduled follow-up appointments (p = 0.578, 95% CI = [-0.033, 0.060]). Patients from a municipality with a low degree of urbanization were more likely to attend appointments (p = 0.027, 95% CI = [0.016, 0.212]). These relationships are important when organizing care of patients with CL/P, especially when it comes to the question of whether healthcare should be centralized.
Distance to Care Center
It seemed likely that the adherence to follow-up appointments would be strongly correlated with the time and expense of traveling to an outpatient clinic, as previous general studies in samples without CL/P predominantly showed an effect of distance decay. 25 However, no statistically significant association was observed within the study sample between increasing distance travelled and the proportion of attendance of scheduled appointments. Although distance to healthcare facilities is generally recognized as a barrier to access, the concept of access is versatile and integrates the dimension of acceptability. 30 Beyond mere travel distance, factors such as the availability of public transport, having access to a vehicle and a driver's license, health status, age, and current employment influence mobility behavior to access medical care in rural areas.31–33 Distance as a barrier to the utilization of health care services might be viewed as relative to patients’ resources and perceived necessity of treatment, among other factors. 32 Additionally, patients from more rural regions seem to show a significantly higher tolerance for longer travel distances. 33 Residents of sparsely-settled areas are prepared to accept significantly higher maximum travel times than residents from urban areas that experience very good within-town access. 33 This might explain the significantly higher probability of patients from more rural areas (lower level of urbanization) to keep follow-up appointments in our study group.
Evaluating samples of patients with CL/P, several studies assessing loss to follow-up equally found no effect of travel distance or time,34–37 while one study in Pennsylvania reported driving distance was associated with attrition of patients during longitudinal follow-up. 38 In a survey in North Carolina, around 48% of respondents traveled more than one hour to receive cleft care, but approximately 67% noted that they did not perceive the travel as problematic. 39 Also in the Cleft Care UK Study (CCUK), the concern of extended travel time and perceived higher obstacles to attend appointments after centralized reorganization did not present as a barrier to care. 8 On the contrary, patient experience and satisfaction with medical care seemed to improve in a centralized organization of cleft care.8,40
The burden of travel to the clinic does not seem to be associated with attending follow-up appointments. Improved quality of care perceived by patients may even increase adherence rates.
Socioeconomic Status
Socioeconomic status is a source of possible inequality, impacting adherence to recommended follow-up appointments. Socioeconomic status and income level have been shown to increase loss to follow-up in pediatric populations in Western countries41–45 and in patients with CL/P in particular.34,35,38,46 Notably, most of these studies are set in the United States, where the insurance status is heavily dependent on the income level. 47 Therefore, it is unlikely that this correlation can be directly applied to a German sample. Estimated per capita income had no effect on adherence to follow-up appointments in our sample and there are other studies that similarly did not find an effect of income level.38,48 While in our analysis the effect of income was significant in the frequentist model and showed a slight negative association between income and attendance rates, this effect was driven by outliers and not reliable in the more robust Bayesian model. Families with higher income may be more likely to choose larger cleft centers for treatment and accept the longer journey.39,49 Appointments that parents do not consider necessary (in general one of the main reasons for failed attendance48,50) may not be attended due to the high effort involved.
Attendance Rate
The overall low attendance rate of 48.24% that we found in our sample is similar to low attendance rates reported in international literature. In a U.S. multidisciplinary cleft center, 62% of patients were lost to follow-up before reaching graduation (age ∼15), and 25% were lost before age 8. 48 Another recent analysis found an 11% decrease per year in the odds of attending annual follow-up for patients with syndromes, compared to a 4% decrease in children without syndromes. 36 While not a focus of the study, there were 74 patients with CL/P in the context of a syndrome and their attendance rate was equally lower in this group (39.47% for patients with a syndrome versus 49.57% in the group with isolated CL/P). In patients treated by a non-governmental organization in El Salvador, 33.7% of patients with cleft lip and 49.7% of patients with cleft palate/cleft lip or cleft palate returned for follow-up at least once, with a yearly attrition rate of 27%. 37 In a separate study of speech evaluations, 66.9% attended initial assessments and only 50.6% adhered to follow-up visits. 51
Low follow-up rates might be due to a variety of factors. Apart from socioeconomic factors described above, patients name a low perceived necessity, poor organization, and personal issues as reasons for not attending. 48 An additional psychological burden of attending visits might lead to patient and caregiver fatigue and lower attendance rates. 36
Centralization of Healthcare
In the context of healthcare, centralization describes the concentration of specialized therapy in highly qualified centers that meet high standards of care. Basic health care and emergency care are excluded from this coverage and should be universally guaranteed. There are several advantages to this centralized treatment of rare and complex diseases, which are partly interdependent and mutually reinforcing. First, the concentration of rare or complex cases at specialized centers helps to ensure that in-depth experiences and sufficient expertise can be gained by professionals as well as benefiting medical education.52,53 Second, physicians specializing in particular diseases or therapies leads to higher-quality care and better outcomes. Patients gain access to physicians with specific expertise in their condition, minimizing variation in quality of care.53–56 Third, in specialized centers, a multidisciplinary approach can be implemented more easily, fostering collaboration among experts from various fields. Support services, such as social work, mental health care, and nutrition counselling can be provided for patients undergoing specialized therapy and contribute to improved outcomes.53,57 Fourth, by pooling financial resources, expertise, and infrastructure in larger centers, healthcare systems can reduce duplication of services, lower costs, and thus work more effectively. 58 A pooled larger funding base might also provide access to state-of-the-art technology and equipment at centralized care institutions that smaller facilities might not be able to afford. This allows for more advanced diagnostic tools, treatments, and surgical procedures that might not otherwise be available. Additionally, allocating human and financial resources for research projects is more feasible. Fifth, high-quality scientific collaborations between similarly structured centers are facilitated that share higher case loads, well-organized documentation, and structured treatment protocols. Patients can benefit from innovative treatments derived from ongoing research. 53 Finally, specialized centers tend to implement better systems for follow-up care after the initial therapy/surgery and can involve different disciplines. Depending on the condition, this is essential to improve long-term health outcomes. 59
While all these aspects are relevant to the quality of care, patients with CL/P in particular benefit from treatment by high-volume surgeons, experienced multidisciplinary teams, and systematic follow-up care during the whole period of craniofacial growth. Conversely, fragmented systems without standardized protocols can result in poorer long-term outcomes for certain patient groups,10,60–62 and there may be a social component to this. In the United States it was demonstrated that patients with CL/P from higher-income households, of White race, and from urban communities are significantly more likely to be treated by high-volume surgeons at high-volume hospitals, whereas patients from underserved areas travel significantly farther and are treated at low-volume hospitals. 49 This disparity highlights the need for evidence-based quality standards and minimum patient thresholds to ensure equitable access to high-quality care.
Strengths and Limitations
The comparatively large number of patients included in a 15-year period leads to a relatively high reliability of the observed associations. The catchment area of the tertiary care center including densely populated urban core areas and large rural territories are well suited to explore effects of potential centralization. However, the retrospective design of the study inherently entails several limitations. As data were collected retrospectively, detailed information on family income and educational background was not available. Instead, average disposable income in the region served as a proxy, which should be interpreted with caution as it may introduce bias. Moreover, the data included pertained to one cleft center only, so that we cannot be sure if patients may have undergone further treatment at other surrounding centers without our knowledge. Additionally, specifics to the clinic organization (as for example the timing of consultation hours and the organization of follow-up appointments) might affect generalizability. We could also only analyze data from patients that actually visited our center; therefore, it is possible that other, unobserved, variables influencing parents’ decision to consult our specialists in the first place also influenced their later attendance to follow-ups, potentially weakening causal interpretations. As only four months of the study time period occurred during the COVID pandemic and impacted all patients equally, it should not significantly influence the results except for a potentially minimal reduction in attendance. Finally, it should be noted that the road networks and connections to the public transport network were subject to changes during the 15-year study period and may have distorted some of the travel times provided by Google Maps.
Conclusions
The distance to the outpatient clinic, travel time by car or public transportation, and population density of the residential area were not associated with the adherence to follow-up appointments in a large German sample of patients with CL/P. Families from rural areas were more likely to keep appointments. These findings mitigate the concern of travel burden when centralizing specialized care and warrant further multi-center studies to guide policy decisions regarding the restructuring of cleft care in Germany.
Footnotes
Ethics Approval and Informed Consent Statement
This study received ethical approval from the local ethical review committee of Medical Faculty, Leipzig University, Germany (IRB Board Number 00001750, 12-15-2020). This is an IRB-approved retrospective study, all patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties.
Author Contributions Statement
Conceptualization A.K.S, D.D., E.G. and A.M.F.; methodology A.K.S, D.D., B.L., F.F. and A.M.F.; software D.D.; validation D.D.; formal analysis D.D. and A.K.S.; investigation A.K.S.; data curation A.K.S., E.G.; writing—original draft preparation, A.K.S. and D.D.; writing—review and editing, all. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.