
Abstract
Many areas of health research increasingly involve end users of research (typically patients and their families/caregivers) in study design, management, and dissemination. Beyond recruiting patients as research participants, the shift is towards engaging patients, parents and caregivers as active partners on the research team, who are recognised and valued as ‘experts-by-experience’ (EbyE). Currently, involving EbyE is not routine in global craniofacial research. This paper highlights the value of EbyE involvement, addresses how to incorporate EbyE at all stages of research and discusses key considerations in facilitating positive experiences for EbyE.
Background
Experts by experience (EbyE) offer valuable perspectives that can only come from living with a condition(s). By incorporating people with lived experience into research, projects benefit from early identification of potential facilitators and barriers. In addition to offering practical improvements to increase accessibility, EbyE involvement provides robust representation.
In recent years, as healthcare has evolved away from paternalism to adopting practices underpinned by patient-centred care, patients are increasingly recognised as partners in their care. 1 Subsequently, patients have increasingly become involved in medical and other research as EbyE, a progression generally acknowledged to result in more informed, accessible, and relevant research. 2 Research involvement differs to research participation where people complete a survey, questionnaire or participate in a clinical trial, interview, or focus group. Research involvement occurs when EbyE are active partners in the design, management and dissemination of research, for example on a project steering group alongside research team members.
Routine inclusion of people with cleft lip and/or palate (cleft) and their parents/caregivers in study design and management is relatively new to the field of craniofacial research. Practices from fields such as dementia care, 3 diabetes, 4 and mental health 5 could augment EbyE engagement in craniofacial research. The wealth of learning, resources, experience, and practices in other fields are excellent examples for craniofacial researchers to utilise and develop further, and removes the need to start afresh.
In the UK, engaging EbyE as experts throughout a study is a requirement for many funders, including the National Institute for Health and Care Research (NIHR). 6 Similarly, the U.S. Patient-Centred Outcomes Research Institute (PCORI) involves patients and other stakeholders in research prioritisation and expects funding applicants to engage patients from research inception to dissemination. 7 The U.S. National Institute of Dental and Craniofacial Research (NIDCR) grants now often include Patient Advisory Boards (PABs). 8 The Canadian Institutes of Health Research (CIHR) facilitates and funds a Strategy for Patient-Oriented Research (SPOR) in which patients are central to health and research discussions to action change in research processes alongside policy and practice. 9 These international funder examples highlight the essential contribution that EbyEs offer in the assessment and commissioning of research funding. EbyE involvement supports research credibility and accessibility, and helps to ensure funding is allocated according to EbyE need and relevance. In turn, this can lead to policy and practice changes.
The benefits of incorporating lived experience perspectives within research have been demonstrated for some time. For example, Aotearoa (New Zealand) requires any planned research that will impact the indigenous Māori population to consult with Māori iwi (tribes) early in design stages to ensure the study upholds Māori values and beliefs, and includes Māori as stakeholders above and beyond research participation. Incorporating Māori lived experience perspectives into research has benefitted Māori health and broader outcomes, has positively impacted legislative policy, and has facilitated more effective interaction between Māori and health providers.10–12
Similarly, the U.S. based Rare Disease Advisory Councils, 13 supported by the National Organization for Rare Disorders, were created by patients, caregivers, families and providers and gives those affected by rare diseases a stronger voice in 27 state governments. Councils highlight and address barriers that hinder people with rare conditions receiving the treatment and care they need. Notably, three states signed RDAC legislation into law in 2023.
This article highlights the different ways to involve EbyE in research and includes the many benefits of involvement alongside guidance on navigating the facilitators and barriers associated with their involvement. The article hopes to offer a starting point for those new to involving EbyE in research and a helpful refresher to those already doing so. Although outside the scope of this article, it is important to acknowledge there are other beneficial opportunities for EbyE and clinician collaboration, e.g., in shared decision-making, service design, and delivery.
Working with Experts-by-Experience in Craniofacial Research
Research suggests some inconsistency between clinicians, patients, parent/caregiver, and researchers’ treatment priorities. 14 Such incongruences could lead to wasted funding and gaps in understanding patient preferences and treatment satisfaction. To address this, a UK based initiative, the James Lind Alliance Priority Setting Partnerships (PSP), 15 aims to involve patients, carers, and clinicians in co-developing treatment research priorities. A PSP brings together clinicians, patients and carers to identify and prioritise health and care uncertainties which research could address. 15
One PSP prioritised the remaining unanswered questions from people with cleft, their parents/carers, and healthcare professionals. The differing research priorities between stakeholders were stark: patients prioritised causes of cleft; parents concentrated on infancy and childhood concerns such as breastfeeding, reflux, and speech and psychological outcomes; and healthcare professionals were most focussed on treatment outcomes/processes/development.16,17 Through further discussion the alliance partners reached consensus on a ‘top 10’ research priorities for UK cleft care. 18
Without reaching consensus, future research may expend stakeholder time and funding on futile avenues of research; multiple, differing perspectives could add more time and disharmony to research since researchers would need to focus on numerous topics or concentrated research ideas. This would ultimately be impractical, costly, and not conducive to the researching of key issues as identified using a collaborative, consensual approach.
Involving Experts-by-Experience Throughout the Research Cycle
Engagement with EbyE team members should continue beyond establishing research topics and questions. Some funders encourage researchers to work with a Public Co-applicant (EbyE) who brings personal insights to grant application development. Additional involvement of EbyE can ensure methods, data collection, and dissemination strategies are appropriate for participants. Lay language research summaries can also be assessed by EbyE to ensure clarity. Figure 1 shows the different ways that EbyE can be involved throughout the research cycle.
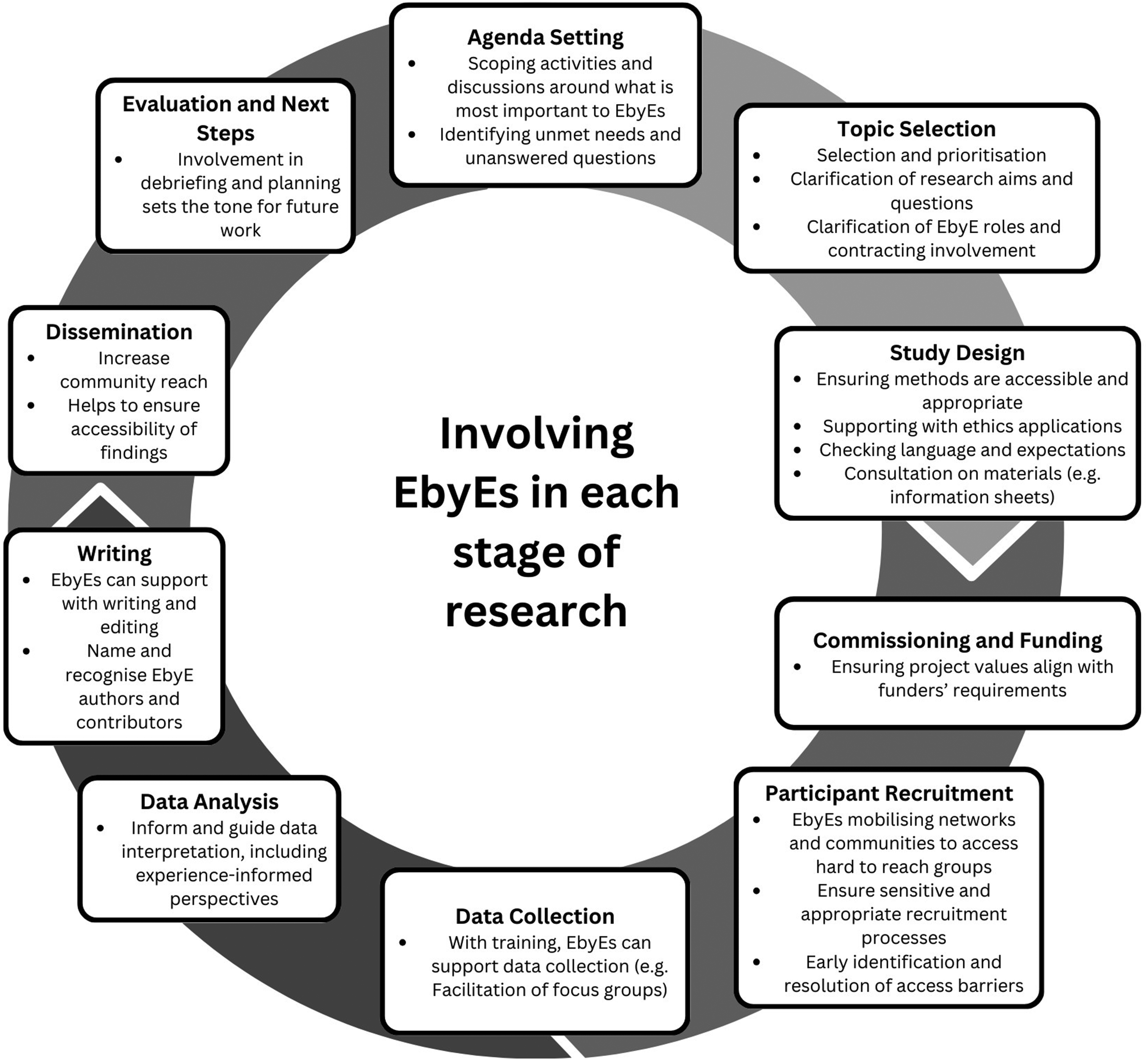
Experts by experience and the research cycle.
EbyE are invested in the success of research and bring knowledge only EbyE hold. For example, working with EbyE on craniofacial research may identify issues with proposed catering, venue accessibility, or interview topics – a topic that may seem benign could inadvertently cause distress. EbyE will likely have suggestions for interview and/or questionnaire item wording and, given their personal expertise, may suggest topics previously overlooked. Further, EbyE can advise on the likelihood of people participating in research projects, and may have insight into effective recruitment strategies. Given appropriate training and support, EbyE can assist with data collection, analysis, reports, and conference presentations. 19 They can support research dissemination via their networks in non-traditional formats that ultimately widen the research's reach. 20 Involving EbyE throughout the research can foster working relationships 21 and helps alleviate power imbalances by creating space for EbyE to be involved in all stages of a project. 22 Barriers to EbyE engagement in research remain, but can be redressed through simple changes.
Navigating Common Barriers to Expert-by-Experience Involvement
Firstly, limited understanding of how to meaningfully engage EbyE risks tokenism rather than the needed move towards shared decision-making. 23 Understanding the principles of meaningful engagement takes time but a wealth of resources are available to support learning in this area. Improving researchers’ and clinicians’ knowledge and skills is recommended via a blend of real-world and interactive learning 24 including resources such as e-learning modules and online handbooks.25,26
When engaging EbyEs in research, specific considerations include reassuring EbyE that care/treatment will not be affected by contribution to the research activities, clarification whether EbyE might know professionals or other participants involved, and making clear if researchers are part of the EbyE care team (current or past). Finally, if EbyE disagree with researchers on a project detail, would the EbyE be side-lined from future research and other opportunities? 27
Managing expectations is fundamental; EbyE should be made aware that research can take years to plan and be funded and is frequently time-consuming and slow. If people are not briefed appropriately, their interest and enthusiasm could be lost. If there is a hiatus in the project, keeping people informed is essential to avoid unintentionally creating a sense of abandonment. It is helpful for EbyE to have a single point of contact for questions or concerns, and to keep them informed and engaged - regular check-ins and updates are particularly useful in this regard. 28
Facilitating Expert-by-Experience Involvement in Research
Informing and Training the EbyE
EbyE should be fully briefed about required commitment and tasks (negotiated per individual skills and experience) and what training and support is available. Additionally, it should be identified early who will deliver training and who will offer support to the EbyE. Support could include recognising the emotional labour felt when involved in research or ensuring safe spaces to share experiences and knowledge. 5 Allowing adequate time and opportunity to build trust, rapport, and understanding is essential to encourage productive working relationships.19,20 In line with ensuring safe spaces to share experiences, it is important to provide EbyE with information on where to locate psychological services or support groups. Opportunities for debriefing during, and after completion of research projects, particularly for those less familiar with working in research, is an additional support measure. 29 This could address any potential distress and further promote trust, rapport, and understanding between researchers, clinicians, and EbyE.
It is acknowledged there is no one-size-fits-all solution, and will depend on the existing relationship between the researcher/clinician and the EbyE. For example, if a researcher/clinician is regularly working with an EbyE, and there is a strong rapport, it would be odd to distribute a list of resources rather than simply asking, “How are you doing?”
Recognising the Contributions of EbyE
EbyE should be active partners in research, which requires recognition of preconceptions. A common belief in healthcare is that clinicians (and by extension, researchers) hold most of the knowledge and power. Discussing ways to level power within the team could offer creative solutions, like asking the EbyE to set agendas or co-chairing meetings (see PARTNERS2 Collective for further examples 5 ). Valuing EbyE expertise can be demonstrated by acknowledging their time and contributions, offering payment, and/or covering associated costs including conference attendance fees, travel, and accommodation.26,30 Demonstrating flexibility to fit in with EbyE's work and education schedules also demonstrates that their time and input is valued – e.g., by offering opportunities to collaborate during an evening or a weekend if preferred by collaborators. 5 Where practical, EbyE should be supported to have opportunities for co-authorship (eg, in journal articles) to strengthen EbyE focus in research dissemination. Discussions concerning expectations of authorship should occur in the early stages of the research cycle to avoid unpleasant surprises, and should include consideration of any support and skill development that may be needed. 31
Finally, following the conclusion of research, a courtesy to strengthen the relationship and value EbyE contributions would be to let the EbyE know if and how their feedback impacted the research. 32
Accessibility
Challenges in reaching EbyE whose voices are seldom heard in research are well-known. 33 People from marginalised and minority groups are typically under-represented in research participation and involvement meaning that key perspectives are not included. Reasons for this are far ranging and often historic, and include mistrust (of researchers), communication challenges, dismissal of cultural concerns, 34 technological barriers, mobility, cognitive, communication difficulties, 35 and legacy of poor research practices, and structural injustices. 36 Inevitably, these issues can hinder collaboration with EbyE, particularly if they are unaware of these opportunities or lack exposure to research institutions or settings. Researchers have an ethical responsibility, and in many jurisdictions a legal one, to actively adopt inclusive research practices to redress this imbalance. 37 For example, careful thought should be given regarding where to recruit EbyE. Going to where people are and/or reaching out to community leaders can be constructive as can managing people's expectations, and eliciting people's access requirements. 38 Inviting people to contribute in a way that suits them as well as focussing on developing a community of relationships is key to building trust and rapport. Using clear and straightforward language is also essential to break down barriers.38,39
Conclusion
There is need to engage EbyE throughout cleft and craniofacial research, not simply as research participants but as active partners in the pursuit of greater understanding. Tangibly utilising EbyE throughout all stages of a study enables research to be patient-centred and holistic in its approach. Using EbyE expertise to review study design, surveys, and interview materials can identify potential issues early, shed light on areas which may otherwise be overlooked, and assist with participant recruitment. Common challenges associated with working with EbyE include concern around any impact research involvement may have on their treatment and professional relationships, however with open communication, these concerns can be well managed. Based on the growing evidence across fields, the authors encourage craniofacial researchers and clinicians alike to work with EbyE as colleagues. EbyE, clinicians, and researchers all have valuable knowledge each can share for the benefit of current and future cleft care, resulting in research teams that are greater than the sum of their parts. Finally, by including EbyE, research teams are responsive to the community's own desire to be represented in research that affects them as exemplified by the rallying cry ‘nothing about us without us’. 40
Footnotes
Acknowledgements
The authors would like to thank Samantha Kingsbury for her objective feedback and suggestions for editing the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.