
Abstract
Objective:
Assess the Health-Related Quality of Life in children and adolescents with non-syndromic craniosynostosis and compare it with participants without craniosynostosis.
Design:
Non-experimental, cross-sectional design.
Setting:
The assessment was done remotely and the instrument was sent via chat or email.
Patients/ Participants:
Participants (ages 8–17) with non-syndromic craniosynostosis (n = 27) and without craniosynostosis (n = 26).
Main Outcome Measure(s):
We used an adapted version for the Mexican population of the Health-Related Quality of Life Questionnaire for Children and Adolescents -KIDSCREEN-52.
Results:
All scores were in the average clinical range and both groups scored similarly in all domains except those with craniosynostosis were significantly lower in the Social Support and Peers domain (rpb = 0.48).
Conclusions:
Children and adolescents with non-syndromic craniosynostosis reported similar Health-Related Quality of Life as the control group, except for the Social Support domain, which should be investigated in future studies.
Keywords
Introduction
Health-Related Quality of Life (HRQoL) is defined as an individual's subjective perception of the impact of health status including disease and treatment, on physical, psychological and social functioning. 1 Since children with health conditions have a higher risk for psychosocial difficulties compared to their peers, researchers should assess the impact in their HRQoL to understand long-term sequelae. 2
There has been an increasing interest in assessing HRQoL in populations with craniofacial conditions because of their long-term implications and treatment needs; nevertheless, few reports mention the impact on HRQoL for patients with craniosynostosis. Studies have reported mixed outcomes in children with non-syndromic craniosynostosis, for example, lower HRQoL than controls, especially in school functioning, 3 while in contrast, another study reported average HRQoL. 4 Normal HRQoL has also been reported in untreated sagittal synostosis, except for lower positive emotional functioning. 5 In another study, authors did not find differences in the HRQoL in adolescents with non-syndromic craniosynostosis compared to the average population. 6 Regarding adults with this condition, there is a report of superior quality of life in comparison with the normative population 7 where no correlations were found with demographic or condition related variables (eg, number of interventions) and the authors proposed this could be due to a greater resilience in this group caused by their condition during childhood. In contrast, in another study with adults with craniosynostosis reported high levels of unemployment, greater likelihood of being single and childless, poor body image and more pressure to conform to societal appearance ideals. 8
In order to address the mixed results of the studies assessing the HRQoL and a lack of information about individuals with craniosynostosis in Mexico, the aim of this study was to assess the HRQoL in Mexican children and adolescents with non-syndromic craniosynostosis who completed craniofacial surgery in comparison to controls without craniosynostosis.
Methods
Participants were surgically treated at the Pediatric Neurosurgery Department of the General Hospital Gaudencio González Garza in Mexico City. Contact information from the participants with craniosynostosis was pulled from a database of parents that expressed interest in being contacted when research projects were available. The participants of the study included children and adolescents between 8–17 years old previously treated for non-syndromic craniosynostosis. Their parents or guardians were informed about the study via phone call and if they agreed to participate, the parents or guardians and the child signed an informed consent. A structured interview was completed with parents through a video call to obtain sociodemographic and clinical information about the participants. The HRQoL questionnaire was sent via email or chat for the participant to answer. The study was approved by the Facultad de Estudios Superiores Iztacala Ethics Committee (Approval CE/FESI/042021/1391) and conducted according to the Declaration of Helsinki. The control group was recruited from different school centers and through snowball sampling. Participants were assessed depending on their age, education, and if their parents had similar academic background as the parents of the patients with craniosynostosis.
Inclusion and Exclusion Criteria
The diagnosis of non-syndromic craniosynostosis was established by a pediatric neurosurgeon who confirmed the diagnosis through a computed tomographic scan. The participants in the craniosynostosis group underwent cranial vault remodeling surgery. Children with sagittal, unicoronal, lambdoid, metopic and multisutural craniosynostosis were excluded if they had had more than one surgical procedure, other medical, psychological or neurological conditions or failed to complete the questionnaire. Children in the control group were excluded from the study if they had a medical, psychological or neurological condition or failed to complete the questionnaire. No medical, psychological or neurological disorders were reported during the interview with parents or guardians.
Instruments
The HRQoL Questionnaire for Children and Adolescents -KIDSCREEN-52 9 is designed to address generic HRQoL in healthy and chronically ill children and adolescents. This instrument aims to identify children at risk in terms of their subjective health. We used the adapted and validated version of the KIDSCREEN-52 for the Mexican population, 10 which is considered the extended version and is recommended when more detailed insight is needed into how the HRQoL of children varies in different dimensions. 11 The 52 items based on recall of the past week assess 10 domains: Physical Well-being, Psychological Well-being, Moods and Emotions, Self-Perception, Autonomy, Parent Relation and Home Life, Financial Resources, Social Support and Peers, School Environment and Social Acceptance (Bullying). The items have a 5-point Likert scale response with higher scores indicating higher wellbeing. Raw scores are converted to T-scores and scores based on Mexican norms had a mean range of 42–57 and a standard deviation range of 6.6–10.6. 10
Data Analysis
The demographics and the domains assessed by the KIDSCREEN-52 were compared with a Mann-Whitney U test. Effect sizes (rpb) were calculated and were considered: 0.10–0.29 small, 0.30–0.49 moderate and >0.50 large. A Holm-Bonferroni correction was used to address the multiple comparisons with a < 0.005 adjusted p value.
Results
A total of 60 participants were approached, from which 53 returned the questionnaire. Data was collected from April 2021 to June 2023. Table 1 shows the groups’ characteristics. Both groups had similar sociodemographic characteristics and showed similar scores in almost all the domains assessed by the KIDSCREEN-52, except for the Social Support and Peers domain (p < 0.005) with a moderate effect size (Table 2), with the craniosynostosis group having the lower score. The proportion of participants in the control group scoring lower than one standard deviation below the mean in the Social Support and Peers domain was 7.7% (2 participants) while 29.6% was the proportion in the craniosynostosis group (8 participants).
Sociodemographic Characteristics of the Sample.
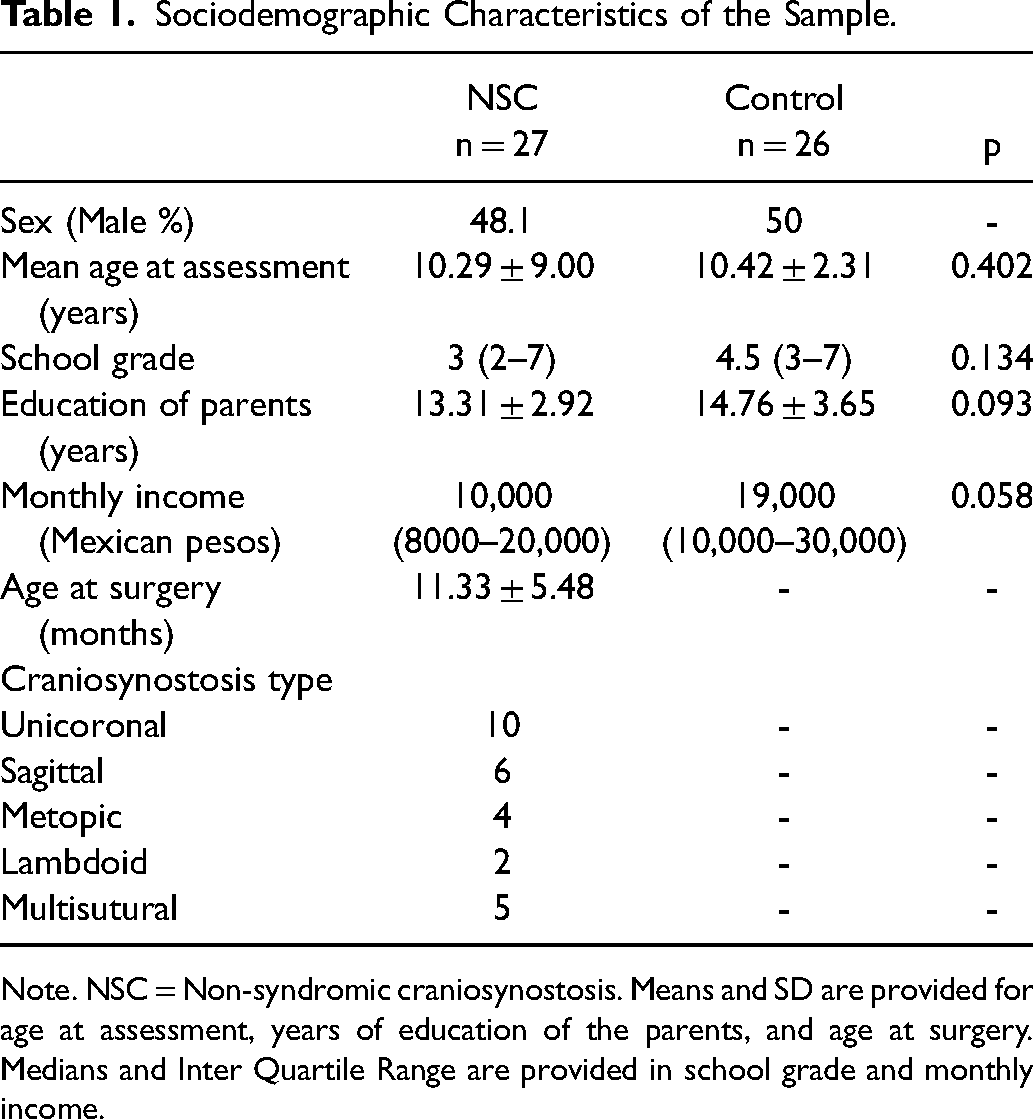
Note. NSC = Non-syndromic craniosynostosis. Means and SD are provided for age at assessment, years of education of the parents, and age at surgery. Medians and Inter Quartile Range are provided in school grade and monthly income.
Comparison Between Non-Syndromic Craniosynostosis and Control Groups in the KIDSCREEN-52 Domains.
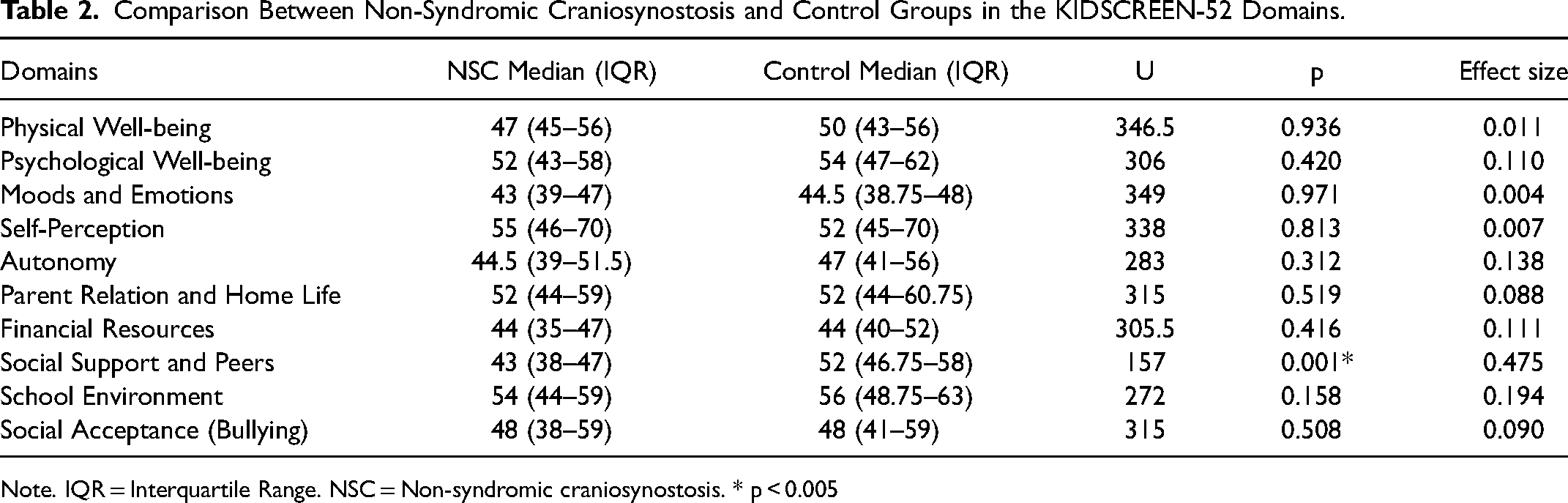
Note. IQR = Interquartile Range. NSC = Non-syndromic craniosynostosis. * p < 0.005
Discussion
This study aimed to assess HRQoL in children and adolescents with non-syndromic craniosynostosis and compare it with a control group without craniosynostosis. Both groups showed similar HRQoL in all the domains except for the Social Support and Peers domain. We found that the median scores were in the average clinical range in all the domains assessed by the questionnaire. The Social Support and Peers domain assesses the relationships with other children, the quality of interaction between their peers and the ability to form and maintain friendships. Specifically, we found that from six questions in this domain, three differed between groups (1. Have you spent time with your friends? 2. Have you had fun with your friends? 3. Have you been able to talk to your friends about everything?). It may be that participants with craniosynostosis have more difficulty engaging in social relationships with peers, as has been reported in adults with the condition 8 or that the group with craniosynostosis experienced more difficulties in HRQoL during COVID-19 confinement than peers as reports of different pediatric health conditions.12,13 Follow up studies should be carried out in Mexico without the social restrictions that were in place during part of the period of data collection to clarify this study's results.
We did not find differences in the domains that can be affected by a craniofacial condition such as self-perception or social acceptance, indicating that the children who responded the questionnaire were satisfied with their body image, had good self-esteem and did not feel bullied. Moreover, they did not show low scores in the School Environment domain that can be affected by the cognitive difficulties reported in this condition,14,15 showing reasonable school adjustment from the children's perspective.
The results we found are in line with previous reports in children with non-syndromic craniosynostosis, Kljajić study found that HRQoL was average and no difference was found in comparison with a normative sample; moreover, they found no impact from the craniosynostosis type and the type of surgical procedure. 4 Furthermore, an HRQoL within the normal range was found in almost all the measures in Boltshauser's study assessing children with sagittal craniosynostosis without surgery, except for the positive emotions area, which means they felt less joyful, happy and confident. 5
Although previous reports from other countries have found risks of low HRQoL in different domains (school functioning 3 and positive emotions 5 ), HRQoL should be investigated in children with different social, cultural and economic backgrounds as those findings might not be replicated in other countries. This study used an adapted and validated instrument in the Mexican population that can detect low HRQoL. 10 Within this sample, the average HRQoL may reflect that they have coping strategies and resilience that allow them to perceive a good physical, psychological, cognitive and emotional adjustment as other authors have reported.5,7 These results can be useful for clinicians that provide care to children with craniosynostosis to understand the long-term implications in HRQoL.
The main limitations of this study include the small sample size across a wide age range and the lack of capacity to compare the differences between the types of craniosynostosis. The addition of parental perspectives should be assessed, as in previous research3,4 to better describe associations with their children; however, the KIDSCREEN-52 has not been adapted and validated in the Mexican population for parents. A longitudinal follow-up should be performed to learn if the results maintain or change into adulthood.
In conclusion, Mexican children and adolescents with non-syndromic craniosynostosis reported similar HRQoL as their peers except for the Social Support and Peers domain, which should be further investigated.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.