
Abstract
Objectives
1. To assess the skeletal class occlusion and lateral cephalometry in children with isolated cleft palates (non-Robin sequence) and 2. to identify associations between these findings and pre-palatoplasty cleft palate measurements.
Study design
Retrospective cohort study.
Setting
North American Institutional Tertiary Paediatric Center.
Patients
Our cleft database was reviewed, and patients were included if they had an isolated cleft palate without a Robin Sequence diagnosis, had a Furlow palatoplasty and had available per operative cleft palate measurements and available lateral cephalogram between 6 and 8 years old. Thirty-two patients matched to inclusion criteria.
Intervention
Furlow's Palatoplasty.
Main Outcome and Measures
Cleft size at palatoplasty, cephalometric measurements and skeletal occlusal classes were analysed. ANOVA was used to test the association between cephalometric measurements and occlusal classes. Results are presented as means with a 95% confidence interval. The association between cleft measurements and cephalometric parameters was tested with Spearman Correlation (rs).
Results
The skeletal occlusal outcome at 7 years old for this series of patients was: Class I: 19%; Class II: 59% and Class III: 22%. No single cleft measurement at palatoplasty was predictive of the skeletal occlusal outcome. A larger hard palate cleft was associated with a shorter antero-posterior maxilla.
Conclusions
The skeletal occlusal class outcomes were similar to those found in a previous study in the literature. The occlusal prognosis appears to be better than in patients with Robin Sequence or with an associated cleft lip. No preoperative measurement was found to be associated with the occlusal outcome.
Introduction
Cleft lip and palate malformations are among the most common craniofacial anomalies in newborns. 1 Children with clefts are prone to impaired maxillary growth 2 with secondary abnormal skeletal occlusion. Patients with cleft present a higher rate of class III malocclusion than non-cleft patients with orthodontic need. 3 The hypothesis regarding suboptimal maxillary or mandibular growth includes anatomical and cleft characteristics, in association to physical and surgical strain.4,5 Wide clefts are associated with an impaired maxillary growth.6–9 However, most studies analyzing cleft size and occlusal outcomes were done on cleft lip and palate cohorts. Studies on patients with isolated cleft palates are sparse. Reiser et al. did not find any association between cleft palate size and crossbite scores in an isolated cleft palate subgroup analysis. 10 Seo et al. observed more class III malocclusions in patients with isolated cleft palates compared to the normal population. 9
Patients born with Robin sequence (RS) are characterized by mandibular micrognathia, glossoptosis and cleft palate, all of which could influence the future occlusal outcome. In a previous study, we have analyzed cleft palate characteristics and occlusal outcomes in a cohort of patients with RS. 11 RS patients presented a class II malocclusion in 59% of cases and bimaxillary hypoplasia with class III malocclusion (41%). A correlation was found between a wide cleft at palatoplasty and mandibular retrusion at 7 years old. To our knowledge, these outcomes have not been assessed in a non-RS population with an isolated cleft palate. On average, the non-RS patients have a shorter and narrower hard palate cleft than patients with RS. 12 This could lead to different occlusal outcomes in non-RS patients. The objectives of our study are (1) to assess the growth of the maxilla, the mandible, and the skeletal occlusal outcome among patients without RS at age 7 and (2) to identify associations between pre-operative anatomic cleft palate measurements and malocclusion dental class, and cephalometric measurements. Our null hypothesis is that there is no association between cleft measurements and malocclusion in non-RS patients, whereas the alternative hypothesis is that an association does exist.
Method
Study Design and Patient Population
The database of patients with cleft lip and palate at the Centre Hospitalier de l’Université Laval was retrospectively reviewed. Inclusion criteria were: (1) patients born with a cleft palate not associated with a cleft lip or RS; (2) patients operated on with Furlow palatoplasty in our tertiary centre between 9 and 11 months; (3) available demographics and per operative cleft palate measurements and (4) available lateral cephalometric analysis between 6 and 8 years old. All palatoplasty cases were done by the same surgeon (J.E.L.) and were followed by the same orthodontist (A.B.) who was blinded of the cleft measurements. The retrospective study was conducted in accordance with the principles outlined in the World Medical Association Declaration of Helsinki. 13 No board of ethics approval was obtained since this study was done with a database without any contact with the patients. This database was used for other of our studies.12,14,15
Assessed Clinical Parameters
Medical records were reviewed for demographic and medical data. Cleft palate measurements (in millimetres) were done with an ophthalmologic caliper and a ruler at the start of the palatoplasty procedure following the insertion of a Dingman retractor (Figure 1). 12 A digitized lateral cephalogram was done before orthodontic treatment between 6 and 8 years old. A lateral cephalometric analysis with Quick Ceph Studio software 5.2.1 (Quick Ceph Systems, San Diego, California; Figure 2) was done twice within a two-month interval by the same orthodontist, who was unaware of the initial cleft palate measurements. The dental occlusion class was recorded according to the Angle classification of malocclusion. 16 All cephalometric measurements were compared with the reference values of the regional population (province of Quebec, Canada) 17 to reduce the effect of different ages at cephalogram. Unless otherwise specified, all data are presented as relative values, for which 1.0 corresponds to the exact value found in the reference population for the same age group.
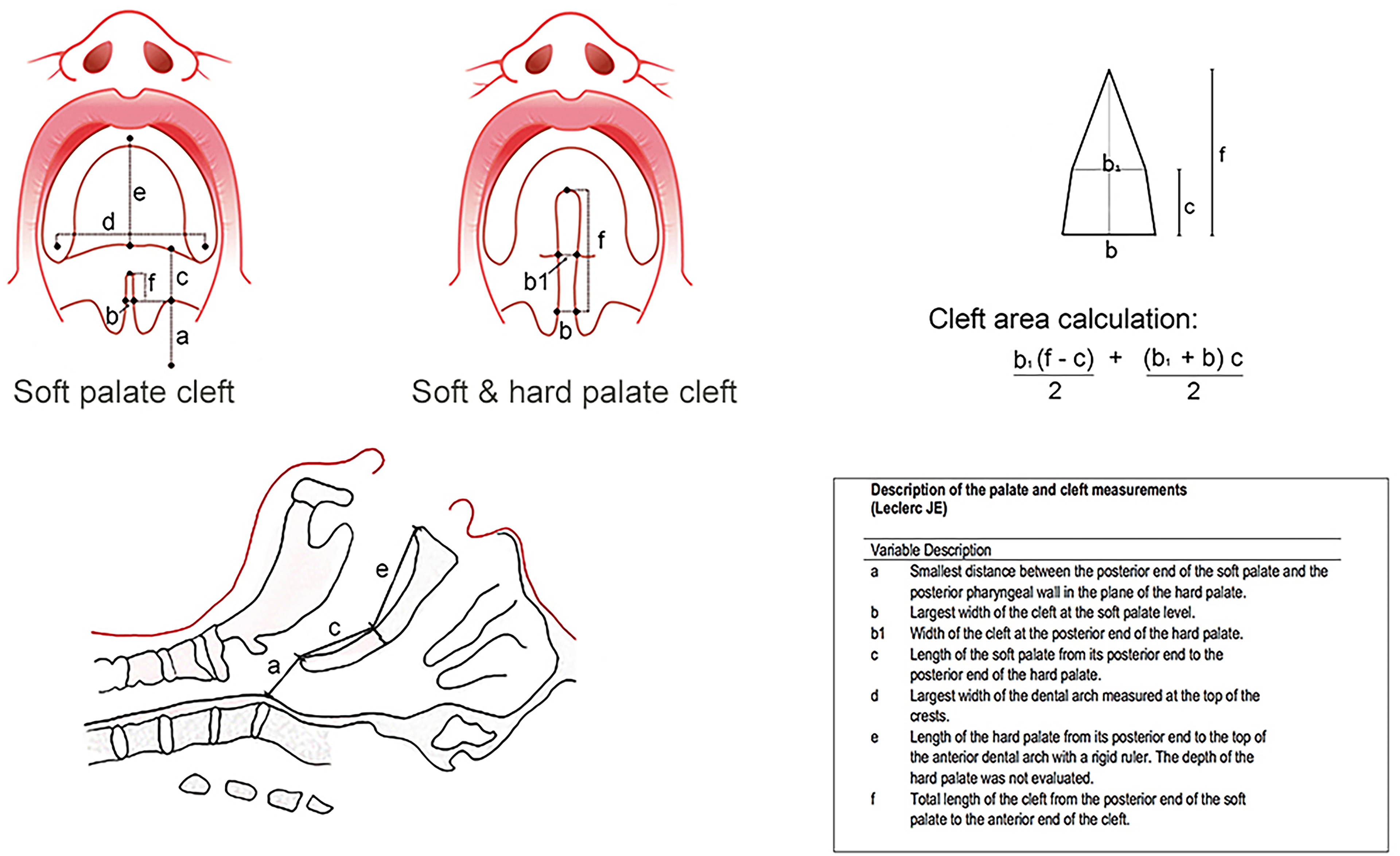
Cleft and palate measurements.
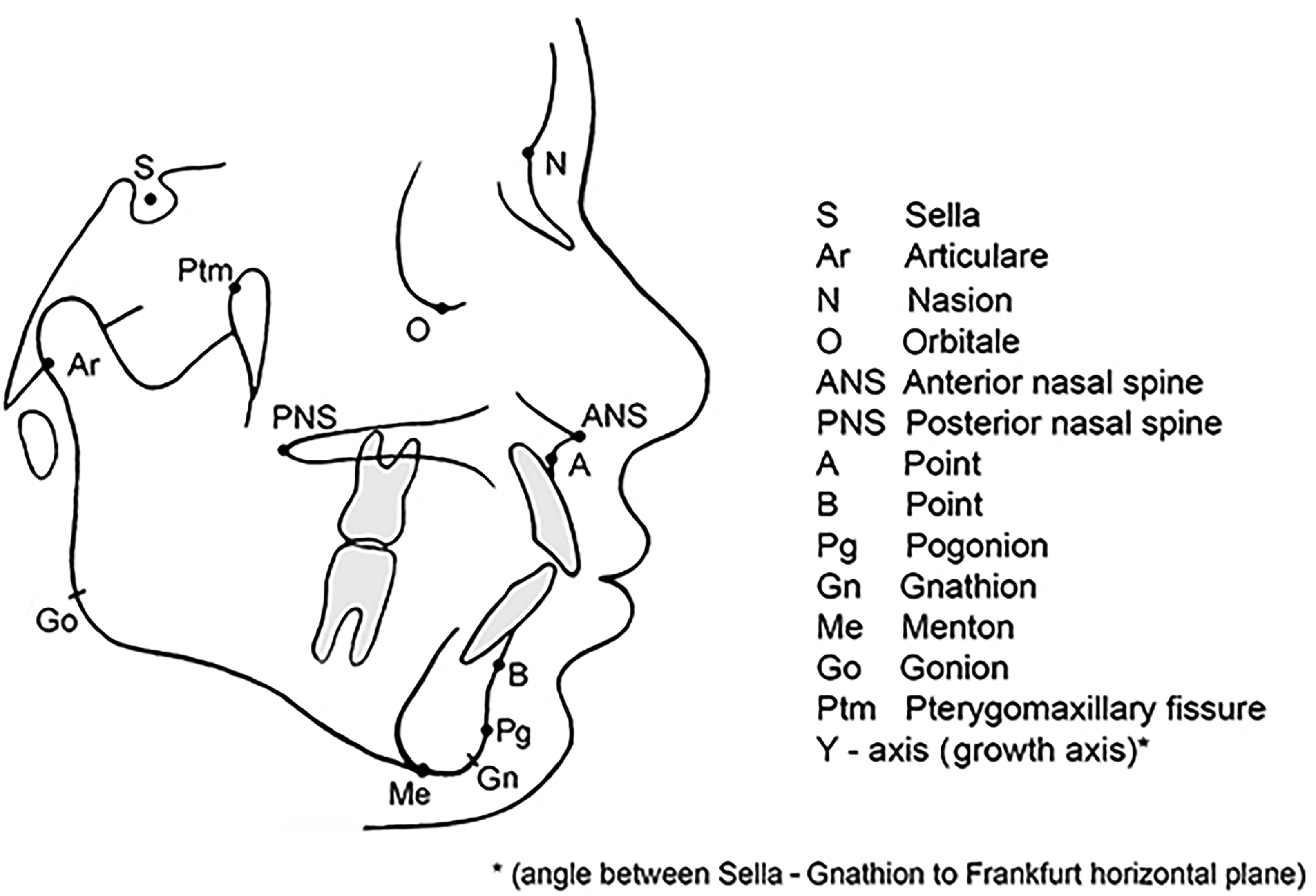
Lateral cephalometric landmarks.
Statistical Analysis
To compare occlusal class groups, the Pearson Khi-2 test was used for categorical parameters, while one-way ANOVA F-test was used for continuous variables, which are presented as mean with a 95% confidence interval. Bonferroni correction was applied for multiple comparisons. Spearman's correlation coefficients were obtained and transposed to a heat map to calculate associations between cleft measurements and cephalometric parameters. The delayed duplicated cephalometric measurements by the same reader allowed intra-observer consistency analyses. Interclass correlation coefficients (ICC) were calculated to measure intra-observer consistency cephalometric measurements. ICC (1.1) was obtained with a one-way random effects, absolute agreement, single rater/measurement. 18 A coefficient of 75% and over was considered good or excellent. 19 Statistical analyses were done with SAS 9.4 (SAS Institute Inc, Cary, North Carolina).
Results
Population
Between 2009 and 2015, forty-three patients underwent a Furlow palatoplasty by the same surgeon in our centre. Among them, thirty-two were included in our study. Eleven patients were excluded. No cleft measurements were available in one patient. Absence of cephalogram was seen in ten patients, as seven patients did not reach the age of six yet, two patients were lost during the follow-up and one patient had physical and intellectual limitation preventing appropriate imaging. Mean age and weight at surgery were 10.3 months (SD = 0.5 months) and 8.8 kg (SD = 1.3 kg), respectively. Mean age at cephalometry was 7.5 years old (SD = 0.6 year). Female patients represented 63% of our sample. In 66% of patients, the cleft extended into the hard palate. At about 7 years old, 6 patients (19%) presented a normal skeletal occlusal class (class I), 19 patients (59%) had a class II and 7 patients (22%) had a class III. No association was found between weight at surgery (p = .99), sex (p = .60) or hard palate involvement (p = .60) and the occlusal class.
Cleft Characteristics
All cleft measurements were obtained from the 32 patients, except for the f length, which was missing for one patient (Figure 3). No significant difference was present between the occlusal classes at a 5% significance level.
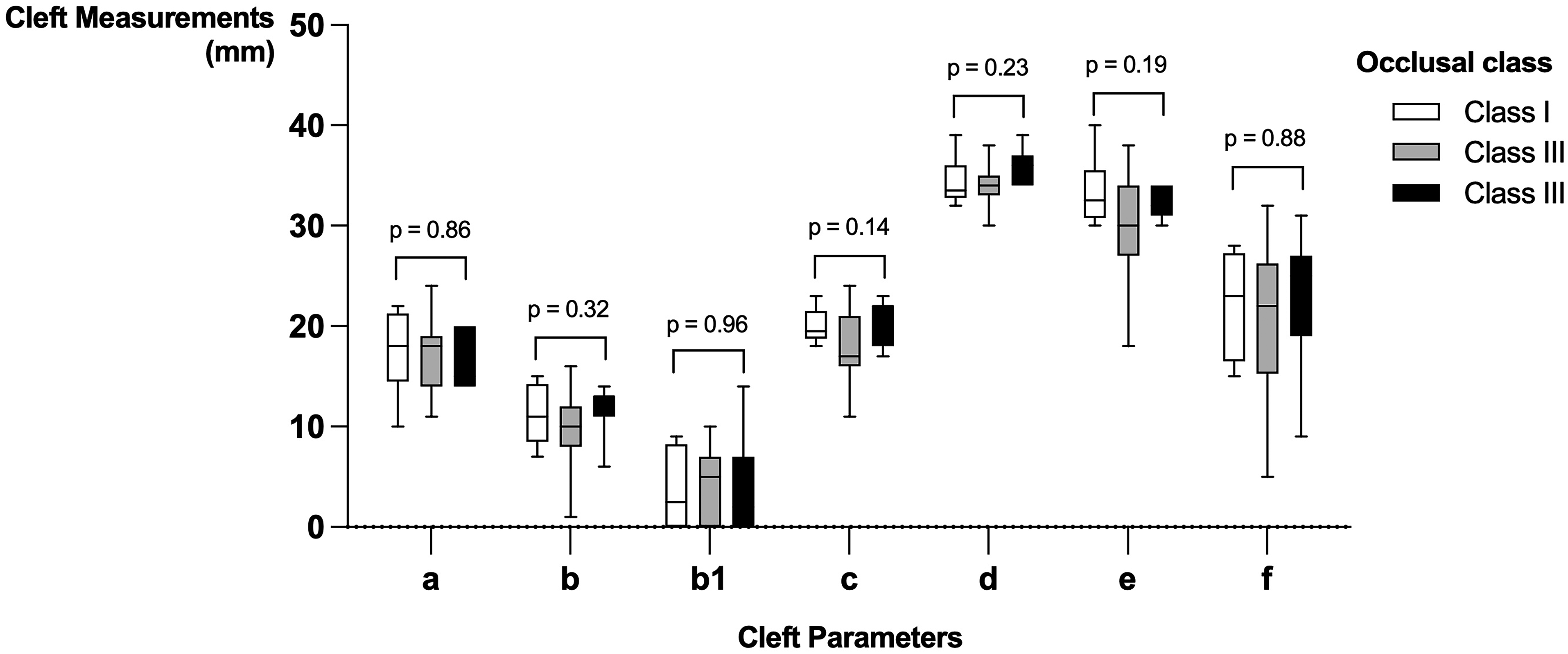
Palate and cleft measurements for each occlusal class. There is no statistically significant difference between the classes at a 5% significance level.
Cephalometric Data
Intra-observer reproducibility analyses are presented in Table 1. All interclass correlation coefficients were over 75%, which confirms a good measure reliability with repeated delayed cephalogram analyse by the same reader, except for gonial angle (Ar-Go-Me), vertical height of the superior maxilla (Is-ANS), vertical length of the middle third of the face (N-ANS), length of the mandible (Go-Pg) and length of the ascending ramus (Ar-Go). Significant intra-observer variability for these parameters leads to poor reliability of these four measurements and consequently, no relevant conclusion can be drawn from these parameters.
Intraobserver Consistency Analysis of Cephalometric Parameters.
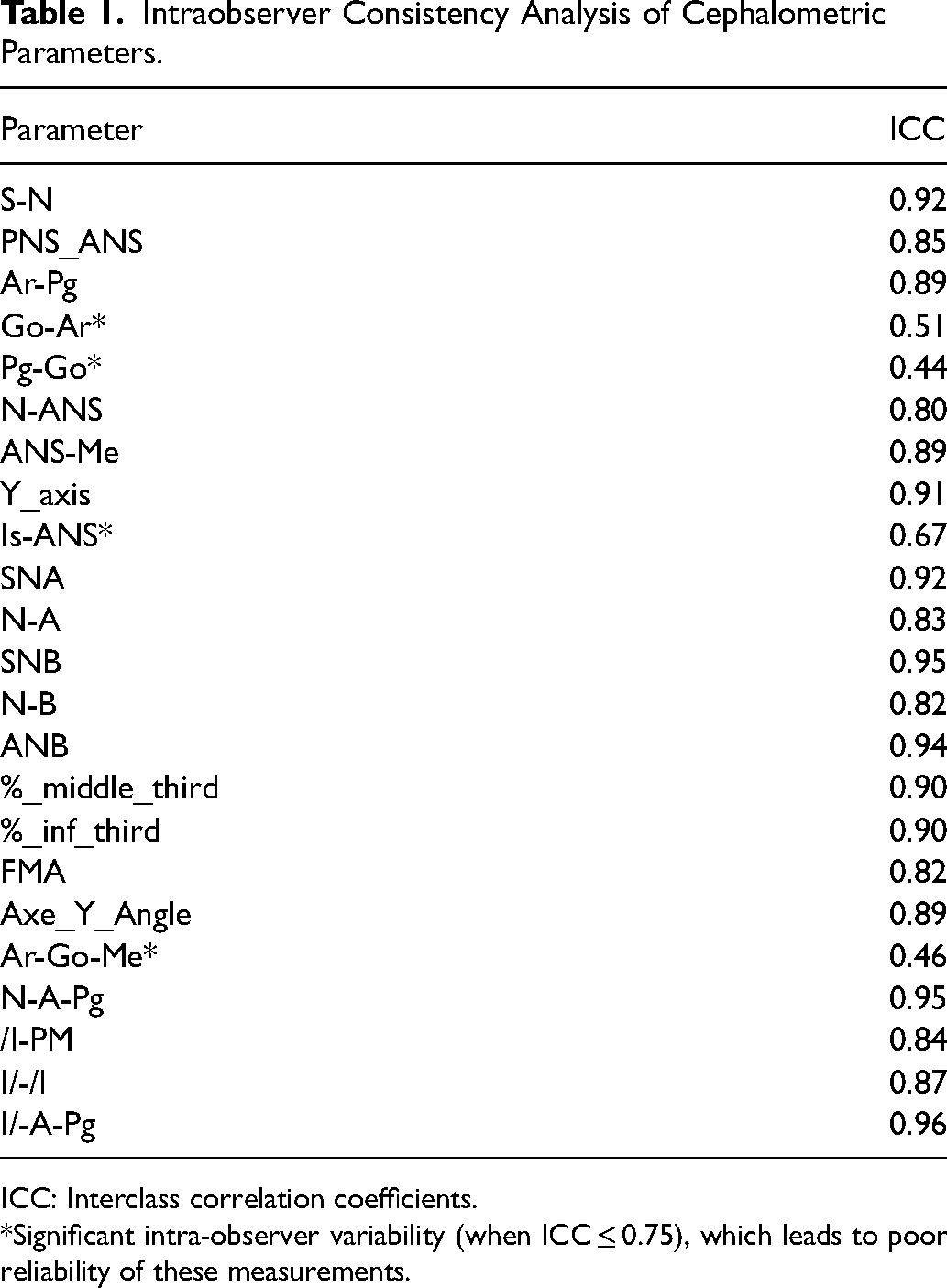
ICC: Interclass correlation coefficients.
*Significant intra-observer variability (when ICC ≤ 0.75), which leads to poor reliability of these measurements.
Cephalometric measurements are presented in Table 2. Many parameters significantly differed from the reference population values. The length of the cranial base (SN), antero-posterior length of the maxilla (ANS-PNS), diagonal length of the mandible (Ar-Pg) and angle of the Y-axis were all smaller than the reference population. However, no difference was seen between the skeletal occlusal classes in these values. Maxilla and mandible positions were similar to the reference population values in class I patients. These values differed significantly from the reference population in cases with malocclusion, especially with class II. Maxilla (SNA) and mandible (SNB) positions in relation to skull base were smaller in classes II and III. In addition, N-A and N-B measurements were more negative in class II, which is represented as a higher positive ratio, in comparison with the reference population values. This represents maxillary and mandibular antero-posterior positions relatively to skull base and indicates a more retrusive maxilla and mandible in class II patients. Only the N-B measurement differed significantly between the occlusal classes. Class II patients had a significantly decreased antero-posterior mandibular growth compared to class III patients (p = .04, with Bonferroni correction for multiple comparisons).
Cephalometric Measurement Ratio Between Occlusion Classes and in Comparison to Reference Population.
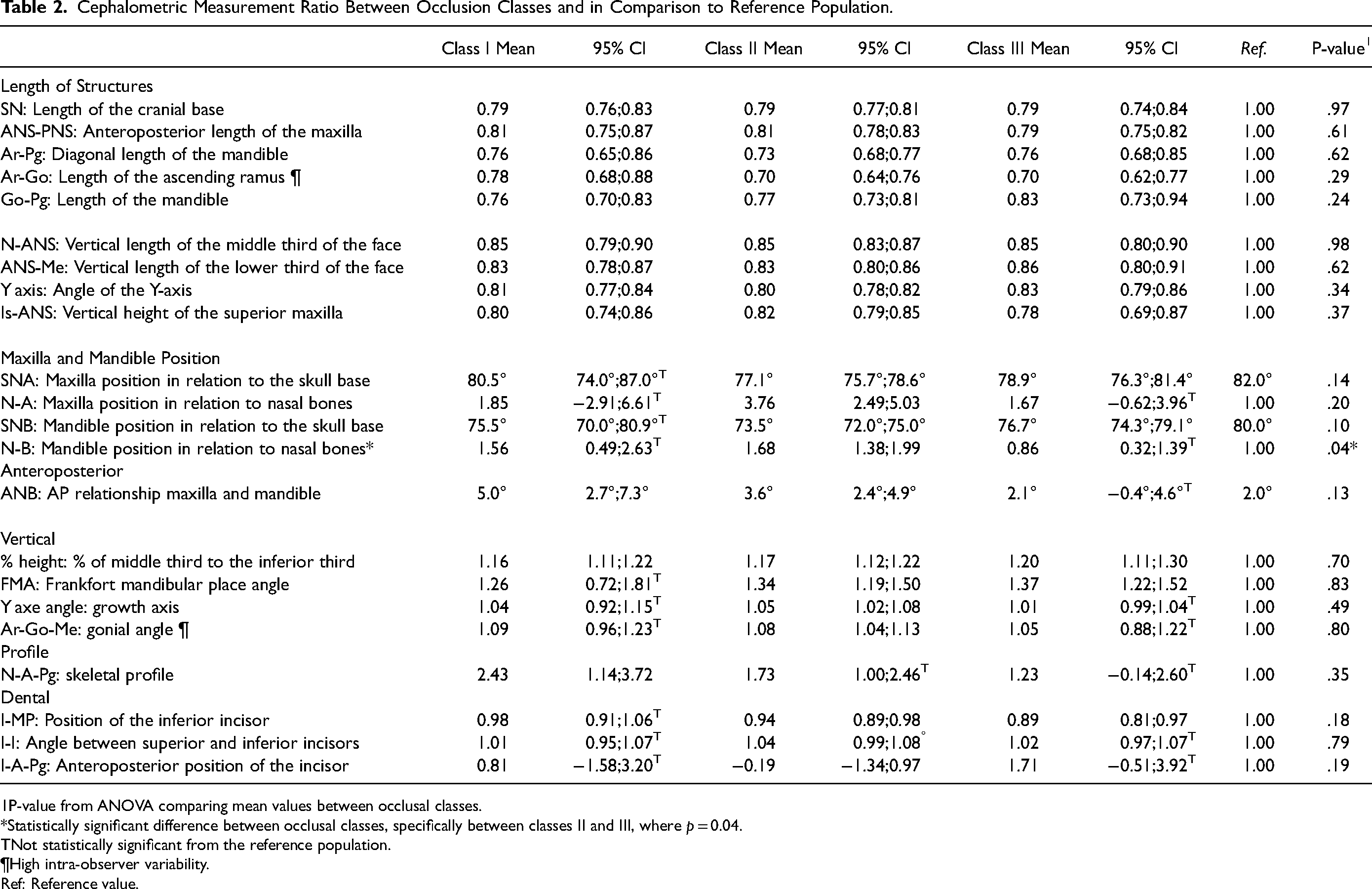
P-value from ANOVA comparing mean values between occlusal classes.
*Statistically significant difference between occlusal classes, specifically between classes II and III, where p = 0.04.
Not statistically significant from the reference population.
¶High intra-observer variability.
Ref: Reference value.
Association Between Cleft Measurements and Cephalometric Parameters
A heatmap of Spearman's correlation coefficients was designed (Figure 4). A larger cleft at the posterior end of the hard palate (b1) was significantly associated with a smaller antero-posterior maxillary length (PNS-ANS) (p ≤ .05). A longer soft palate (c) was significantly associated with a retrusive mandible (ANB) (p ≤ .05).
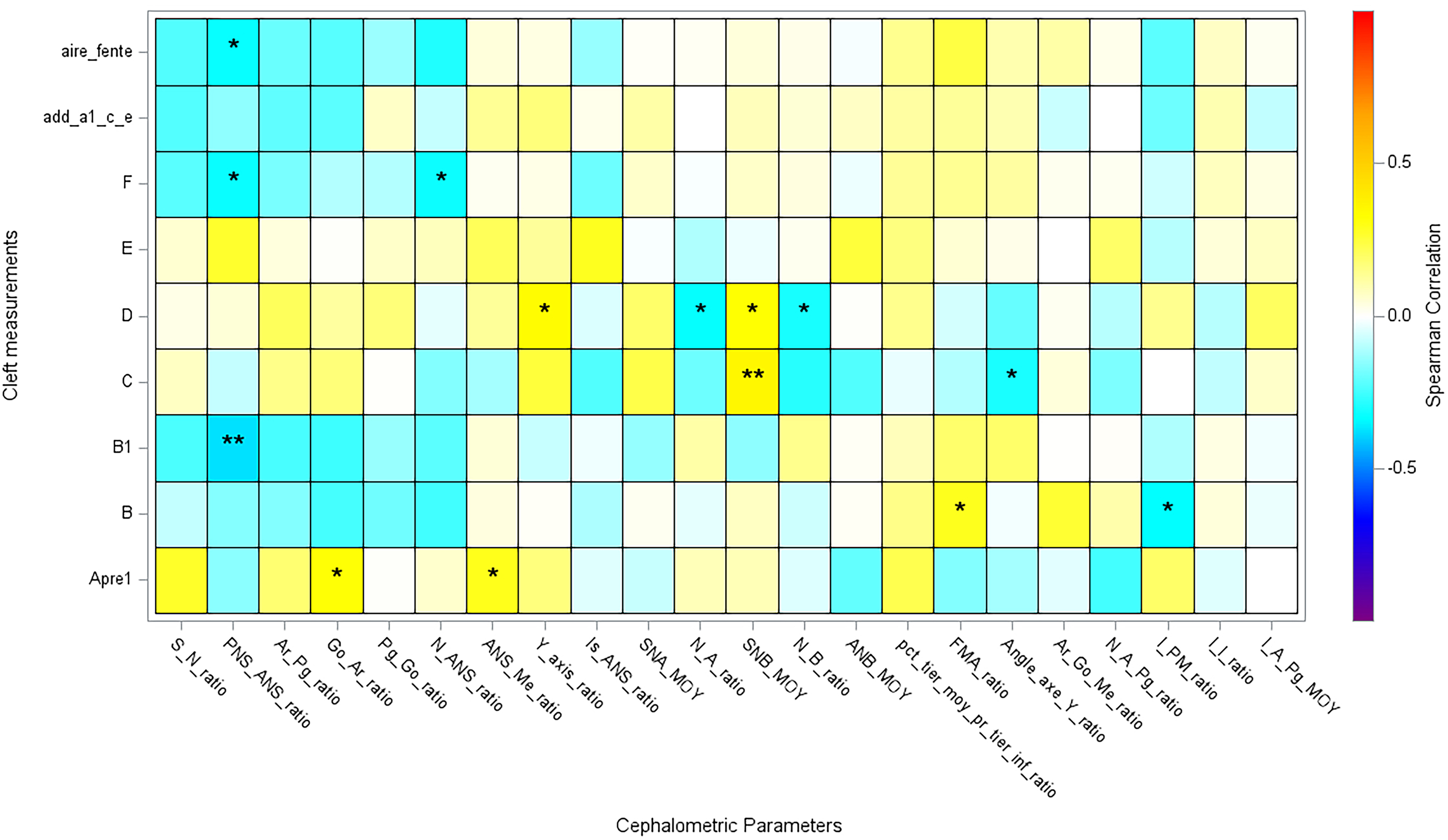
Heat map of Spearman's correlation coefficients. *.05 < p ≤ .10 **.01 < p ≤ .05.
Discussion
Occlusal Outcome in Patients with Isolated Cleft Palates
In our cohort, patients with an isolated cleft palate without RS presented a normal skeletal occlusion class in 19% of cases. Fifty-nine percent had a class II occlusion and twenty-two percent, a class III. A Swedish retrospective study on isolated cleft palate showed similar results, with 68% of class II and 27% of class III malocclusions at 6 years old. 20 A Korean study showed a higher class III prevalence, with a 5.5-odd ratio of having class III malocclusion in patients with an isolated cleft palate compared to the normal population. 21 In our cohort of patients without lip involvement, one finding was similar to the findings of a previous study on patients with unilateral cleft lip and palate 2 : impaired antero-posterior maxillary growth as shown by a smaller SNA and a higher ANB. Moreover, smaller SNA and SNB were found in classes II and III, which could be explained by a decreased maxillary and mandibular horizontal growth.
We did not find any association between cleft measurements and skeletal occlusal outcome. However, a larger hard palate cleft was associated with a shorter antero-posterior maxilla. A significantly longer distance between nasion and mandible was found in patients with a class II occlusion, which suggests noticeable vertical growth. Previous studies have shown an association between the size of cleft lip / palate and maxillary growth, 6 whereas others did not.22,23 Literature is scant about the size of an isolated cleft palate in relationship with maxillary and mandibular position and dimensions. The impact of a cleft lip repair on maxillary growth makes comparisons of cleft lip and palate and isolated cleft palate outcome difficult. 23 An earlier study found no association between cleft palate size and crossbite score, but only horizontal skeletal occlusion was analyzed. 10 This is consistent with our study.
Comparison With RS Patients
The design of our previous study on patients with RS was identical to this one except for the palatoplasty technique (Furlow for non-RS vs. Von Langenbeck with intra velar veloplasty for RS). In our RS study, 59% of patients had a class II malocclusion, 41% a class III, and no patient had a normal class I. This contrasts with patients without RS, but with an isolated cleft palate (iCP) who presented a normal skeletal occlusal class in almost 20% of cases (p = .0486, with Pearson Khi-2 test). 11 Patients with an iCP are likely to have a better occlusal outcome than patients with RS. The relationship between cleft size and skeletal occlusal outcome or cephalometric parameters also differs in the 2 groups. We have previously shown that a smaller distance between soft palate and posterior pharyngeal wall (A) and a smaller distance from dental arch and pharyngeal wall (A + C + E) were associated with the occurrence of a class III malocclusion in patients with RS, 11 which was not found in the present study. With our results, we conclude that there is no association between cleft measurements and malocclusion in non-RS patients and we do accept our null hypothesis. Because the values of the initial cleft measurements are less extreme in the latter group, a larger cohort may be needed to reach statistical significance.
Limitations
The first and most important limitation of this study is the small size of the cohort, which reduces power. Our team has previously shown that patients with iCP have a shorter and narrower hard palate cleft in non-RS vs. RS patients. 12 Less severe changes in non-RS patients would, again, lessen study power. We only analyzed anteroposterior skeletal occlusion class. Horizontal growth and crossbite were not measured. The mandible still grows after age 7 so the outcome may still be different. The influence of other mouth or pharyngeal surgery such as velopharyngoplasty was not analyzed because of the small size of the cohort. No genetic background or parental skeletal evaluation was performed. Finally, there was heterogeneity in a few intra-observer correlation coefficients in cephalogram assessment. However, none of the affected parameters came out with a significant difference between classes. In our comparisons with the previous study on patients with RS, the palatoplasty surgical technique was not the same.
Conclusions
The skeletal occlusal outcome at 7 years old for this series of patients with an isolated cleft palate was: 19% of Class I, 59% of Class II and 22% of Class III. No single cleft measurement at palatopasty was predictive of the skeletal occlusal outcome in these patients. A larger hard palate cleft was associated with a shorter antero-posterior maxilla. In comparison with the results of our previous study on patients with Robin sequence, patients with iCP had a better overall occlusal outcome.
Footnotes
Data Availability Statement
Raw data can be shared by the corresponding author upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article